MEDICAL CONNECTIONS | CONEXIUNI MEDICALE®
EDITOR IN CHIEF
ASSISTANT EDITORS
Rumelia Koren
Vasile Blaga (electronic version)
ASSISTANT EDITOR IN CHIEF
Ottó Andó (print version)
Călin Bumbuluţ
Cristian Sever Oană (editorialist)
EDITOR (Methodology of the Scientific Research)
Tudor Stăncioiu (Dental Medicine)
Tudor Cătălin Drugan
EDITORIAL BOARD
Adalbert Bauer (SCM Satu Mare, România)
Liliana Lup (Synevo Satu Mare, România)
Nicolae Bidilean (Emergency County Hospital,
Gavriel Kesler (Israel)
Satu Mare, România)
Ladislau Kiss (Emergency County Hospital,
Melinda Boros (Bucureşti, România)
Satu Mare, România)
Gheorghe Borcean (Caransebeş Hospital, România)
Sorina Mihalca Man (Emergency County Hospital,
Ioan Brândeu (Emergency County Hospital,
Satu Mare, România)
Satu Mare, România)
Gad Neumann (Hasharon Hospital, Tel Aviv, Israel)
Constantin Cârstea (CMI Braşov, România)
Alina Negru (SCM Satu Mare, România)
Manole Cojocaru (Titu Maiorescu University,
Lea Rath-Wolfson (Hasharon Hospital, Tel Aviv, Israel)
Bucureşti, România)
Viorel Rădulescu (CMI Olt, România)
Raluca Monica Comăneanu (Titu Maiorescu University,
Marius Dinu Roatiş (Emergency County Hospital,
Bucureşti, România)
Satu Mare, România)
Corina Cornean-Santa (Emergency County Hospital,
Cristian Bogdan Rusu (Emergency County Hospital,
Satu Mare, România)
Satu Mare, România)
Bogdan Feciche (Emergency County Hospital,
Dana Shvero Kesler (Hadassa University, Jerusalem, Israel)
Satu Mare, România)
Gheorghe Trip (Emergency County Hospital,
Gyula Grosz (SCM West Satu Mare, România)
Satu Mare, România)
Carlos Gruzman (Hasharon Hospital, Tel Aviv, Israel)
Karoly Zilahi (SCM Praxis, Bixad, România)
Orsolya Horber (SCM Praxis Bixad, România)
Aliza Zeidman (Hasharon Hospital, Tel Aviv, Israel)
EDITOR
ASSOCIATED EDITOR
College of Physicians Satu Mare
Satu Mare Association of Family Physicians
Satu Mare, 23 Eroilor Revoluţiei Pl.
Affiliated with National Society of Family Medicine/
General Medicine
email: colmedsm@gmail.com
Satu Mare, UK 30 Bobocului St.
PARTNERSHIP
EXTERNAL PARTNERSHIP
Titu Maiorescu University, Bucharest
Vasile Goldiş
Hasharon Hospital,
Faculty of Medicine and Dental Medicine
Western University of Arad
Rabin Medical Center
67A Gheorghe Petraşcu St.
94 Revolutiei Blvd., Arad, Romania
Affiliated with Sackler School of Medicine,
Petah Tikva 49372, Israel
EDITORIAL OFFICE
23 Eroilor Revoluţiei Pl., 440055, Satu Mare, Romania, Tel/Fax: 0040261-710456, 0040361-408164
ISSN online 2068 - 8369
ISSN 1843 - 9306
Journal included in Te Schedule of Medical Publications of CMR, 10 credits CMR for subscribers
Indexed in Index Copernicus®, CNCS B+ Category, Code 944
Medical Connections/Conexiuni Medicale® is a trademark of College of Physicians Satu Mare and Satu Mare Association of Family Physicians
Printed at TIPOOFFSET, Fabricii st, No. 93-103, Cluj Napoca, Tel.: 0040264-456071, Fax: 0040264-595711
SCIENTIFIC AND PEER REVIEW BOARD | COLECTIV ŞTIINŢIFIC ŞI DE RECENZIE
Acad. Prof. Univ. as. Dr. Virgil Enătescu
Prof. Univ. Dr. Tuvia Hadar
(Emergency County Hospital, Satu Mare,
(Beilinson Hospital, Rabin Medical Center, Sackler
Romania)
Faculty of Medicine, Tel Aviv University, Israel)
Acad. Prof. Univ. Dr. Doina Onicescu
Prof. Univ. Dr. Gheorghe Manole
(Titu Maiorescu University, Faculty of Medicine
(Titu Maiorescu University, Faculty of Medicine
and Dental Medicine, Bucharest, Romania)
and Dental Medicine, Bucharest, Romania)
Acad. Senior Scientific Researcher Dr. Sorin Riga
Prof. Univ. Dr. Dorel Augustin Manu
(Prof. Dr. Al. Obregia Clinic Hospital of Psychiatry,
(Titu Maiorescu University, Faculty of Medicine
Bucharest, Romania)
and Dental Medicine, Bucharest, Romania)
Acad. Senior Scientific Researcher Dr. Dan Riga
Prof. Univ. Dr. Dan Mănăstireanu
(Prof. Dr. Al. Obregia Clinic Hospital of Psychiatry,
(Titu Maiorescu University, Faculty of Medicine
Bucharest, Romania)
and Dental Medicine, Bucharest, Romania)
Prof. Univ. Dr. Rumelia Koren
Prof. Univ. Dr. Elena Moldoveanu
(Hasharon Hospital, Rabin Medical Center, Sackler
(Titu Maiorescu University, Faculty of Medicine
School of Medicine, Tel Aviv University, Israel)
and Dental Medicine, Bucharest, Romania)
Prof. Univ. Dr. Mircea Cinteză
Prof. Univ. Dr. Adriana Stănilă
(Carol Davila University of Medicine and
(Victor Papilian Faculty of Medicine, Sibiu,
Pharmacy, Bucharest, Romania)
Romania)
Prof. Univ. Dr. Vasile Astărăstoae
Prof. Univ. Dr. Maria Lidia Nica Udangiu
(Gr. T. Popa University of Medicine and Pharmacy,
(Titu Maiorescu University, Faculty of Medicine
Iaşi, Romania)
and Dental Medicine, Bucharest, Romania)
Prof. Univ. Dr. Petru Armeanu
Prof. Univ. Dr. Dan Florin Ungureanu
(Titu Maiorescu University, Faculty of Medicine
(Titu Maiorescu University, Faculty of Medicine
and Dental Medicine, Bucharest, Romania)
and Dental Medicine, Bucharest, Romania)
Prof. Univ. Dr. Ilie Constantin
Conf. Univ. Dr. Tudor Cătălin Drugan
(Victor Babeş University, Faculty of Medicine,
(Iuliu Haţieganu University, Faculty of Medicine,
Timişoara, Romania)
Cluj Napoca, Romania)
Prof. Univ. Dr. Gheorghe Ionel Comşa
Conf. Univ. Dr. Ghinescu Minerva
(Ovidius University, Constanţa, Romania)
(Titu Maiorescu University, Bucureşti, România)
Prof. Univ. Dr. Constantin Dumitru
Conf. Univ. Dr. Mircea Sorin Sabău
(Titu Maiorescu University, Faculty of Medicine
(University of Medicine and Pharmacy Târgu
and Dental Medicine, Bucharest, Romania)
Mureş, Romania)
Prof. Univ. Dr. Rivka Gal
Ş. L. Dr. Anca Ciurea
(Hasharon Hospital, Rabin Medical Center, Sackler
(Iuliu Haţieganu University, Faculty of Medicine,
School of Medicine, Tel Aviv University, Israel)
Cluj Napoca, Romania)
Prof. Univ. Dr. Doina Lucia Ghergic
Ş.L. Dr. Virgil Radu Enătescu
(Titu Maiorescu University, Faculty of Medicine
(Eduard Pamfil Universitary Clinic of Psychiatry,
and Dental Medicine, Bucharest, Romania)
Timişoara, Romania)
Te Medical Connections/Conexiuni Medicale® is indexed in Journals Master List of Index Copernicus®
CNCS B+ Category, Code 944
© Copyright Medical Connections/Conexiuni Medicale, Satu Mare, 2016
No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form or by any
means without prior permission in writing of Medical Connections/Conexiuni Medicale®. Permission is not
however required to copy abstracts of papers or of articles on condition that a full reference to the source is
shown. Correspondence regarding permission to reprint all or part of any article published in this journal
should be addressed to the Editor, e-mail: colmedsm@gmail.com
MEDICAL CONNECTIONS | CONEXIUNI MEDICALE®
EDITOR ŞEF
EDITORI ADJUNCŢI
Rumelia Koren
Vasile Blaga (versiunea electronică)
EDITOR ŞEF ADJUNCT
Ottó Andó (versiunea tipărită)
Călin Bumbuluţ
Cristian Sever Oană (editorialist)
EDITOR (metodologia cercetării științifice)
Tudor Stăncioiu (Medicina Dentară)
Tudor Cătălin Drugan
COMITET EDITORIAL
Adalbert Bauer (SCM West Satu Mare, România)
Liliana Lup (Synevo Satu Mare, România)
Nicolae Bidilean (Spital Judeţean de Urgenţă,
Gavriel Kesler (Israel)
Satu Mare, România)
Ladislau Kiss (Spital Judeţean de Urgenţă,
Melinda Boros (Bucureşti, România)
Satu Mare, România)
Gheorghe Borcean (Spital Municipal Caransebeş,
Sorina Mihalca Man (Spital Judeţean de Urgenţă,
România)
Satu Mare, România)
Ioan (Brândeu Spital Judeţean de Urgenţă,
Gad Neumann (Spital Hasharon, Tel Aviv, Israel)
Satu Mare, România)
Alina Negru (SCM Satu Mare, România)
Constantin Cârstea (CMI Braşov, România)
Lea Rath-Wolfson (Spital Hasharon, Tel Aviv, Israel)
Manole Cojocaru (Universitatea Titu Maiorescu,
Viorel Rădulescu (CMI Olt, România)
Bucureşti, România)
Marius Dinu Roatiş (Spital Judeţean de Urgenţă,
Raluca Monica Comăneanu (Universitatea Titu Maiorescu,
Satu Mare, România)
Bucureşti, România)
Cristian Bogdan Rusu (Spital Judeţean de Urgenţă,
Corina Cornean-Santa (Spital Judeţean de Urgenţă,
Satu Mare, România)
Satu Mare, România)
Dana Shvero Kesler (Universitatea Hadassa,
Bogdan Feciche (Spital Judeţean de Urgenţă,
Ierusalim, Israel)
Satu Mare, România)
Gheorghe Trip (Spital Judeţean de Urgenţă,
Gyula Grosz (SCM West Satu Mare, România)
Satu Mare, România)
Carlos Gruzman (Hasharon Hospital, Tel Aviv, Israel)
Karoly Zilahi (SCM Praxis, Bixad, România)
Orsolya Horber (SCM Praxis Bixad, România)
Aliza Zeidman (Spital Hasharon, Tel Aviv, Israel)
EDITOR
EDITOR ASOCIAT
Colegiul Medicilor Satu Mare
Asociaţia Medicilor de Familie Satu Mare
Satu Mare, P-ţa Eroilor Revoluţiei nr.23
Afiliată la Societatea Naţională de Medicina Familiei/
Medicină Generală
email: colmedsm@gmail.com
Satu Mare, str. Bobocului UK 30
PARTENER
PARTENER EXTERN
Universitatea Titu Maiorescu Bucureşti
Universitatea de Vest Vasile Goldiş
Hasharon Hospital, Rabin Medical Center
Facultatea de Medicină şi Medicină Dentară
din Arad
Afiliat la Sackler School of Medicine,
str. Gheorghe Petraşcu 67A
94 Revoluţiei Blvd., Arad, România
Universitatea Tel Aviv
7 Keren Kayemet St.,
Petah Tikva 49372, Israel
REDACŢIA
P-ţa Eroilor Revoluţiei nr 23, 440055, Satu Mare, Romania, Tel/Fax: 0261-710456, 0361-408164
ISSN online 2068 - 8369
ISSN 1843 - 9306
Revistă inclusă în Nomenclatorul Publicaţiilor Medicale ale CMR, 10 credite CMR pentru abonaţi
Indexare în Index Copernicus®, CNCS categoria B+, cod 944
Medical Connections/Conexiuni Medicale® este marcă înregistrată a Colegiului Medicilor Satu Mare şi a Asociaţiei Medicilor de Familie Satu Mare
Tipărit la TIPOOFFSET, str. Fabricii, Nr. 93-103, Cluj Napoca, Tel.: 0040264-456071, Fax: 0040264-595711
Contents
Editorial
Overview of Options for the Recognition of Family Medicine / General Medicine as a European
Medical Specialty
7
Original Articles
Te Socio-Demographic Characteristics Associated with the Increased Likelihood of Subsequent
Schizophrenia
Virgil Radu Enatescu, Minodora Manea, Radu Stefan Romosan, Ana Maria Draghici,
Valentin Alexandru Pinzaru, Cristina Ana Bredicean, Ion Papava
11
Correlation Between Excessive Weight Loss and Quality of Life Improvements 12 Months after
Laparoscopic Sleeve Gastrectomy
Viorel Dejeu, Dănuț-Aurel Dejeu, Paula Dejeu, Aurel Babeș
21
General Review
Treatment of Primary Osteoporosis
Cristina Căpățînă, Cătălina Poiană
29
Te Ovarian Cancer Under the Histories Magnifying Glass, Terapy Possibilities Over the Time.
An Overview
Ionuț Marcel Cobec
37
Cerebral Intraventricular Hemorrhage. A Gestational Pathological Event - Review
Zamfir-Radu Ionescu, Georgiana-Cristina Ionescu
41
Transperitoneal vs. Retroperitoneal Laparoscopic Nephrectomy for Renal Cell Carcinoma:
a General Review
Cristian Bogdan Rusu, Bogdan Ovidiu Feciche, Lilian Gorbatai, Tiberiu Botezan, Bogdan Bumbuluț,
Andrei Bumbuluț, Rumelia Koren
45
Treatment with Human Milk for Adults Conditions
Mihaela N. Niță
49
Guidance for Authors
53
Cuprins
Editorial
Privire de ansamblu asupra opțiunilor de recunoaștere a Medicinei de Familie/Medicinei Generale
ca specialitate medicală europeană
57
Articole originale
Caracteristici socio-demografice asociate cu probabilitatea crescută a unui diagnostic ulterior
de schizofrenie
Virgil Radu Enatescu, Minodora Manea, Radu Stefan Romosan, Ana Maria Draghici,
Valentin Alexandru Pinzaru, Cristina Ana Bredicean, Ion Papava
61
Corelație între scăderea greutății excesive și îmbunătățirea calității vieții la 12 luni
după gastrectomia verticală laparoscopică
Viorel Dejeu, Dănuț-Aurel Dejeu, Paula Dejeu, Aurel Babeș
71
Revistă generală
Tratamentul osteoporozei primare
Cristina Căpățînă, Cătălina Poiană
79
Cancerul ovarian sub lupa istoriei; modalități terapeutice de-a lungul timpului.
O revistă generală
Ionuț Marcel Cobec
87
Hemoragia cerebrală intraventriculară. Un eveniment patologic intragestațional
Zamfir-Radu Ionescu, Georgiana-Cristina Ionescu
91
Nefrectomia transperitoneală vs retroperitoneală pentru carcinomul renal.
O revistă generală
Cristian Bogdan Rusu, Bogdan Ovidiu Feciche, Lilian Gorbatai, Tiberiu Botezan, Bogdan Bumbuluț,
Andrei Bumbuluț, Rumelia Koren
95
Tratamentul cu lapte uman al afecțiunilor adulților
Mihaela N. Niță
99
Standarde de redactare
103
Colegiul Medicilor
Satu Mare
Colegiul Medicilor Satu Mare este o persoană juridică autonomă, neguvernamentală,
apolitică şi fără scop patrimonial. Este într-o largă accepţiune o organizaţie profesională
liberală şi reuneşte peste 626 de medici.
Colegiul Medicilor Satu Mare crede că poate reuşi urmând trei principii: să vorbească doar
când are ceva important de spus, să nu critice până când nu are soluţii şi să nu propună decât
soluţii rezultate din sfatul colectiv. Forţa Colegiului Medicilor constă în prezentarea în faţa
societăţii ca o voce autentică, permanent validată, a tuturor membrilor săi.
Satu Mare College of Physicians is an autonomous legal entity, non-governamental, apolitical
and non-profit. In a widley acception it is a liberal professional organization and brings
together over 626 doctors.
Satu Mare College of Physicians believes it can succeed by following three principles: to
speak only when he has something important to say, to make no critics until he has solutions
and to propose only solutions resulted from a of collective advice. Te force of Physicians
College consist in showing in front of the society an authentic voice, always validated, from
all its members.
Eroilor Revoluţiei Pl. no.23, 440055 Satu Mare, Romania.
Tel./Fax: +40-261-710456, +40-361-408164, e-mail: colmedsm@gmail.com
EDITORIAL
OVERVIEW OF OPTIONS FOR THE RECOGNITION OF FAMILY
MEDICINE / GENERAL MEDICINE AS A EUROPEAN MEDICAL
SPECIALTY
Călin Bumbuluț
Assistant Editor-in-Chief, Vice-President of UEMO
Glossary:
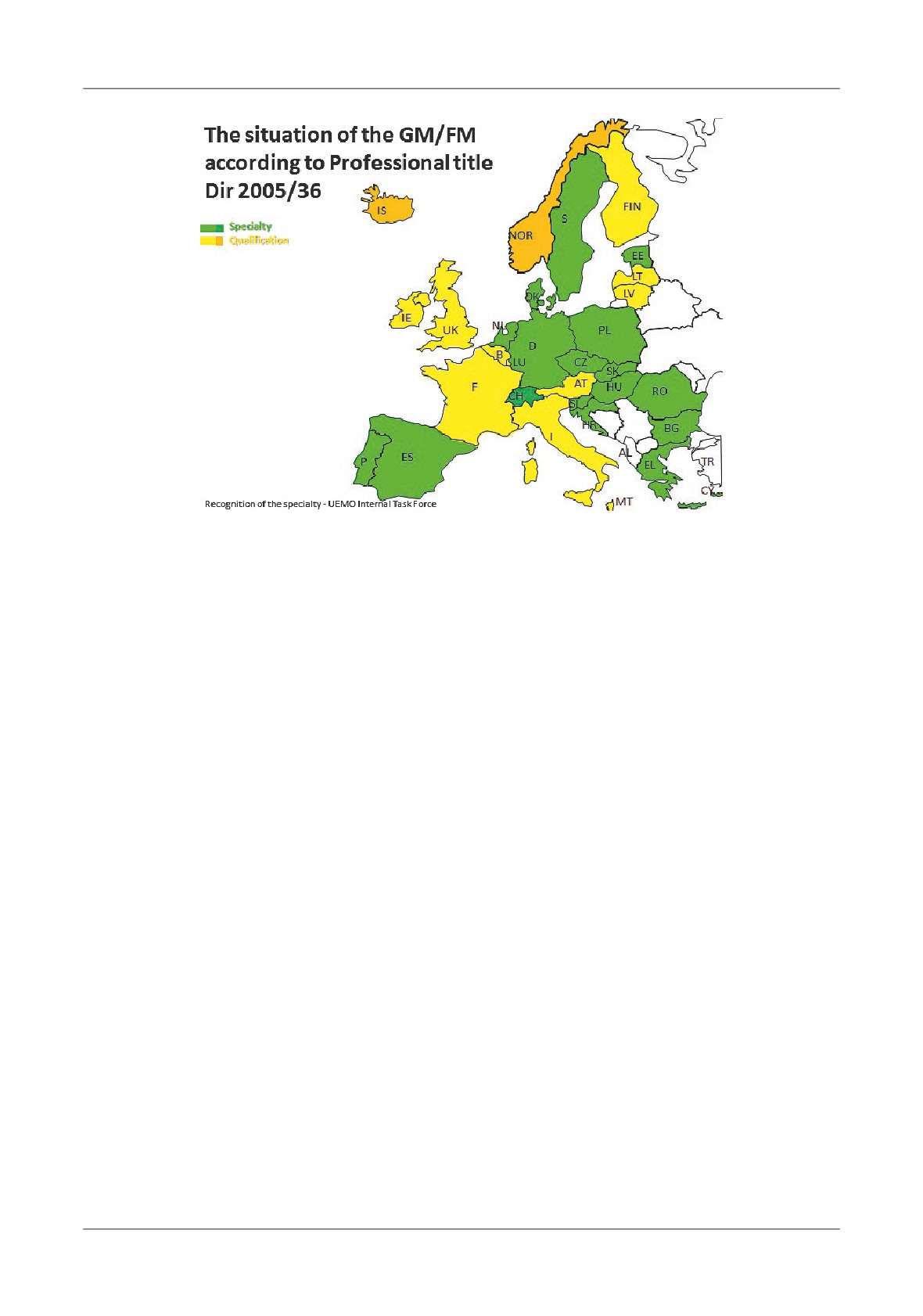
The actual situation
Te European Union of General Practitioners/
Te EU legislation (Directive 2005/36 and 2013/55)
Family Physicians (Union Européenne des Médecins
aims at ensuring the recognition of qualifications in
Omnipraticiens/Médecins de Famille - UEMO) was
order to facilitate the free movement of professionals and
founded in 1967, quickly grew to encompass organisations
in the case of doctors to set up minimum requirements
from all the current Member States of the European Union
for getting an automatic recognition.
as well as from the countries of the European Free Trade
Te regulating laws of the profession at the
Association and other European countries. Since
1992,
European level are: Directive 2005/36/CE and Directive
UEMO has official, non-governmental, consultative status
2013/55/CE.
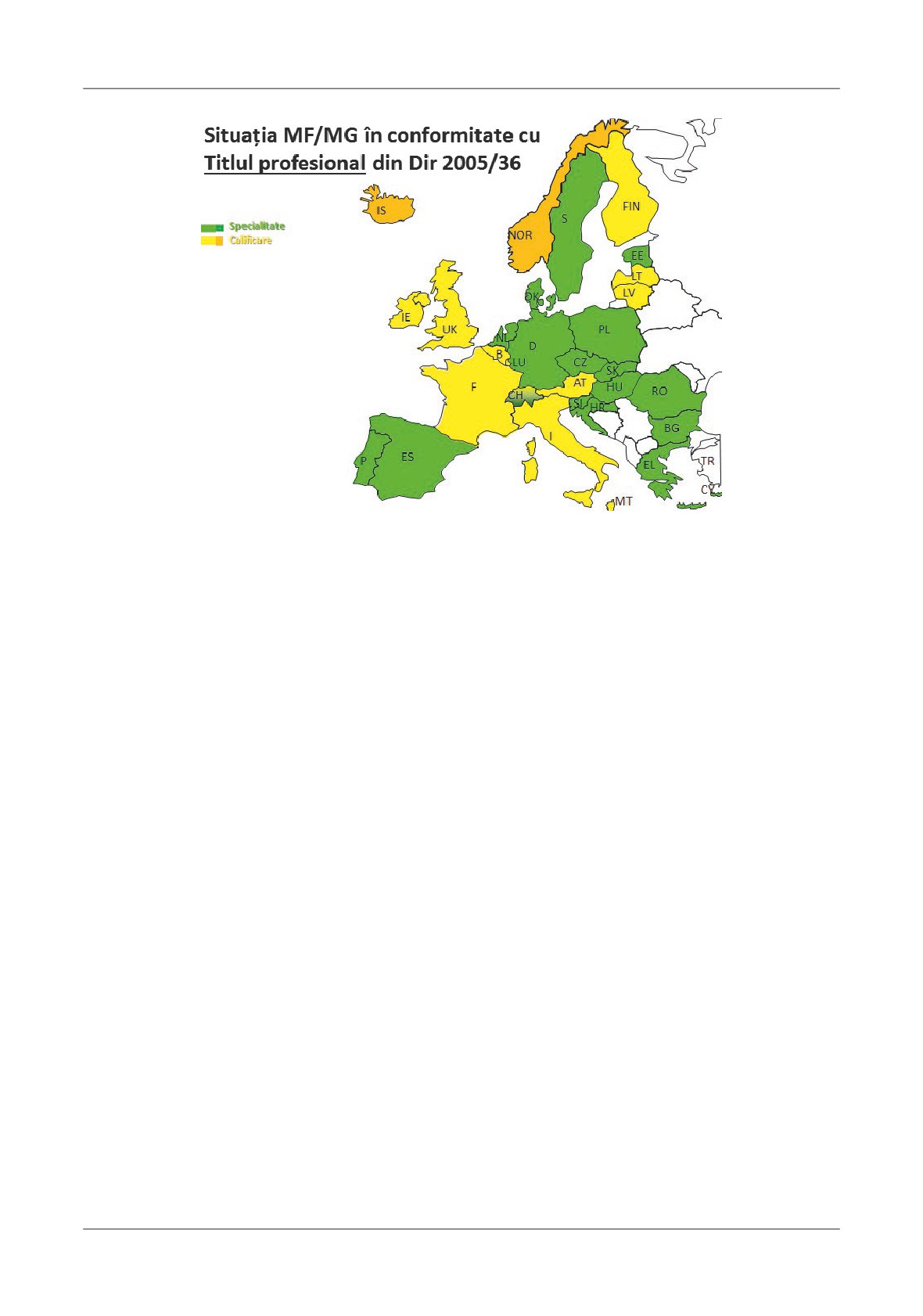
Currently, from 28 countries, 17 (more than 1/2,
ENMCA is an acronim for European Network of
over
2/5) are recognizing the specialty of FM/GM.
Medical Competent Authorities. Te Network brings
From May 2016, there are two more countries with
together European Competent Authorities responsible for
internal recognition, as the Netherlands notified the
the recognition of medical qualifications, in line with the
EC, the Evidence of formal qualifications are “Certificate
Directive 2005/36/EC on the recognition of professional
of enrollment on a specialist register of general
practitioners; Diploma of medicine specialist”, and also
Competent Authorities are the regulatory bodies
Sweden changed in
“Proof of specialist in general
with obligations placed upon them by the revised Mutual
medicine”.
Recognition of Professional Qualifications Directive
At least 24 countries are applying specific training
2005/36/EC (PQD), and they control access to regulated
programs for FM/GM.
professions, professional and vocational titles and
“(…) the minimum training duration in Annex V
professional activities which require specific qualifications.
was established during the last revision of the Directive
National Authority provides information on the
in 2003, (…) the majority of member states fall within
recognition of professional qualifications in every EU country
a range of four to six years of specialist training for all
and guide professionals through the administrative formalities.
qualifications listed in the Annex. Te findings of the
Group of Coordinators for the recognition of
survey also highlight that some member states allow for
professional qualifications, with the mission to establish
specialist training to be considerably shorter.
cooperation between Member States’ authorities and the
Te minimum training duration defined in Annex
Commission on questions relating to the recognition of
V seems to be determined according to the shortest
professional qualifications.
national point of reference. Minimum harmonization,
Annex V - list of liable qualifications to automatic
i.e. using the lowest common denominator of training
recognition from the Directive 2005/36/EC. Contain the
years as point of reference as practiced in Annex V does
Evidence of formal qualifications, Professional title and
not contribute to the mutual trust required for the
Reference date
system of automatic recognition. If competent
IMI - Te Internal Market Information system is an
authorities cannot verify the specific content of specialist
IT-based information network that links up national,
training, they at least want to be sure that the duration
regional and local authorities across borders.
of training allows for an adequate degree of specialization;
Overview of Options for the Recognition of Family Medicine / General Medicine as a European Medical Specialty
7
Editorial
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
we ask for a minimum duration that reflects more than
2. Recognition through automatic mechanism as
the lowest common denominator. We call for the
specialty not as qualification.
Commission to consider this insufficiency in its future
3. Preventing the interference of political and
work on the Directive in order to make automatic
administrative authorities in the regulation of the
recognition compatible with patient safety needs.”
Family Medicine (i.e. the intention of some governments
(ENMCA position paper on minimum training duration
to replace generalist practitioner physicians with nurses)
in Annex V, April 2016)
4. Equality with other specialties for the access to
Tere are four types (until now) of regulating of the
training and CME, for the accreditation of the events,
General Medicine in the European Union and affiliated
the right to be elected and to vote in representative
countries:
national medical organizations and for the representation
- recognition of the specialty of General Medicine/
in Europe.
Family Medicine at national level and notifying of this
5. Tere are specialties recognized only in some
to the CE with the nomination in Annex 5.1.4
countries, but they are benefiting from the introduction in
- recognition as special qualification of General
the Directive
36, Annex 5.1.3 such Neuropsychiatry,
Medicine/Family Medicine at national level and
which has national recognition just in 10 EU countries, or
notifying of this to the EC with the nomination in
Radiology in 11 Eu countries, Accident and emergency
Annex 5.1.4.
medicine in 7, Biological hematology in 4, Dermatology
- recognition of the specialty of General Medicine/
only in 3 (!) (at least in 2005, as is notified in Directive 36).
Family Medicine at national level in specific national law
6. Keeping of the 28, 29 and 30 Articles in the
but notified to the EC as qualification in Annex 5.1.4.
2005/36 Directive regarding the general frame of
- unification with another specialty nominated in
qualification in General Medicine, is required for
Annex 5.1.3, under a new nomination (i.e. - Internal
situations where the physician hasn`t obtained the
General Medicine in Switzerland).
specialty but only the qualification title.
Te pros and cons for recognition of the Family
7. Concerns about the increasing of the expenditure
Medicine as specialty
for GP`s payment is irrelevant insofar as Family
Tis is a check list about the opportunities and the
Medicine benefit in all countries of a separate budgetary
benefits (or not) of recognition as specialty.
allocation (Te main concern is the supposed belief of
Te pros:
the politicians about the increasing of funding of the
1. Te perspective of an European curriculum /
GPs as consequence of the recognition as specialists).
European training programs for General Medicine,
8. Te trend for all the specialties in Europe is to
taking into account the nowadays variety of these, both
regulate the training content and the European
in duration and in content.
examination; we cannot stand apart from this process;
8
Bumbuluț
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
Editorial
the development of the Charter of Training (similar to
Possible scenarios:
other specialty) for our specialty is a necessity.
- coexisting of two regimes at national levels in 17
9. Te force of the generalist practitioners will
EU countries, meaning maintaining the status quo.
increase if the arguments will be discussed on an equal
- the changing of the current Directive through
level with other specialties, in front of political and
several steps: deletion of the Article 28, the inclusion in
administrative authorities.
Annex 5.1.3, deletion of the Annex 5.1.4, inclusion in
Te cons:
Article 25 of the training requirements in GM. We must
1. Te risk to lose our individuality in the ocean of
recognize, it’s the less plausible from political point of
specialties (more than 50) (though “union in diversity”
view because is needed that European Parliament to
is the motto of the EU).
vote all this, and it is not a desirable one for this
2. If not all countries have the specialty, it will create
moment, because there are countries from those
a complex system for the migration of doctors in EU.
seventeen with large number of GP’s without recognition
3. Not to lose the simple system for free movement
of the specialty from different reasons. Our interest is to
of doctors and automatic recognition.
maintain the Articles 28, 29 and 30. Moreover, the
4. Te danger of being “assimilated” in the interests
Directive deals with all regulated professions and not
of other specialties in dealing with authorities.
only doctors so engaging in a full legislative process for
5. Risk of realizing that “some are more equal than
one profession is unrealistic. Tis would have to be
others”.
considered if/when the Directive will be revised.
6. Te possibility that a generalist could be elected
- the progress with Directive 2013/55 regarding
in a representative national or international medical
Annex V notification (list of liable qualifications to
organization can be a benefit, but also a loss when you
automatic recognition) through changing procedures
have to fight not only for the interest of your specialty.
and introducing
“delegated act”. In Article
26, the
7. Maintaining the acquired rights from the Article
second paragraph is replaced by the following: “… the
30 and nothing more.
Commission shall be empowered to adopt delegated acts in
8. Which duration should have the specific
accordance with Article 57c concerning the inclusion in
training? What should be its content? Should it keep its
point 5.1.3 of Annex V of new medical specialties common
specificity? (Article 28).
to at least two-fifths of the Member States”.
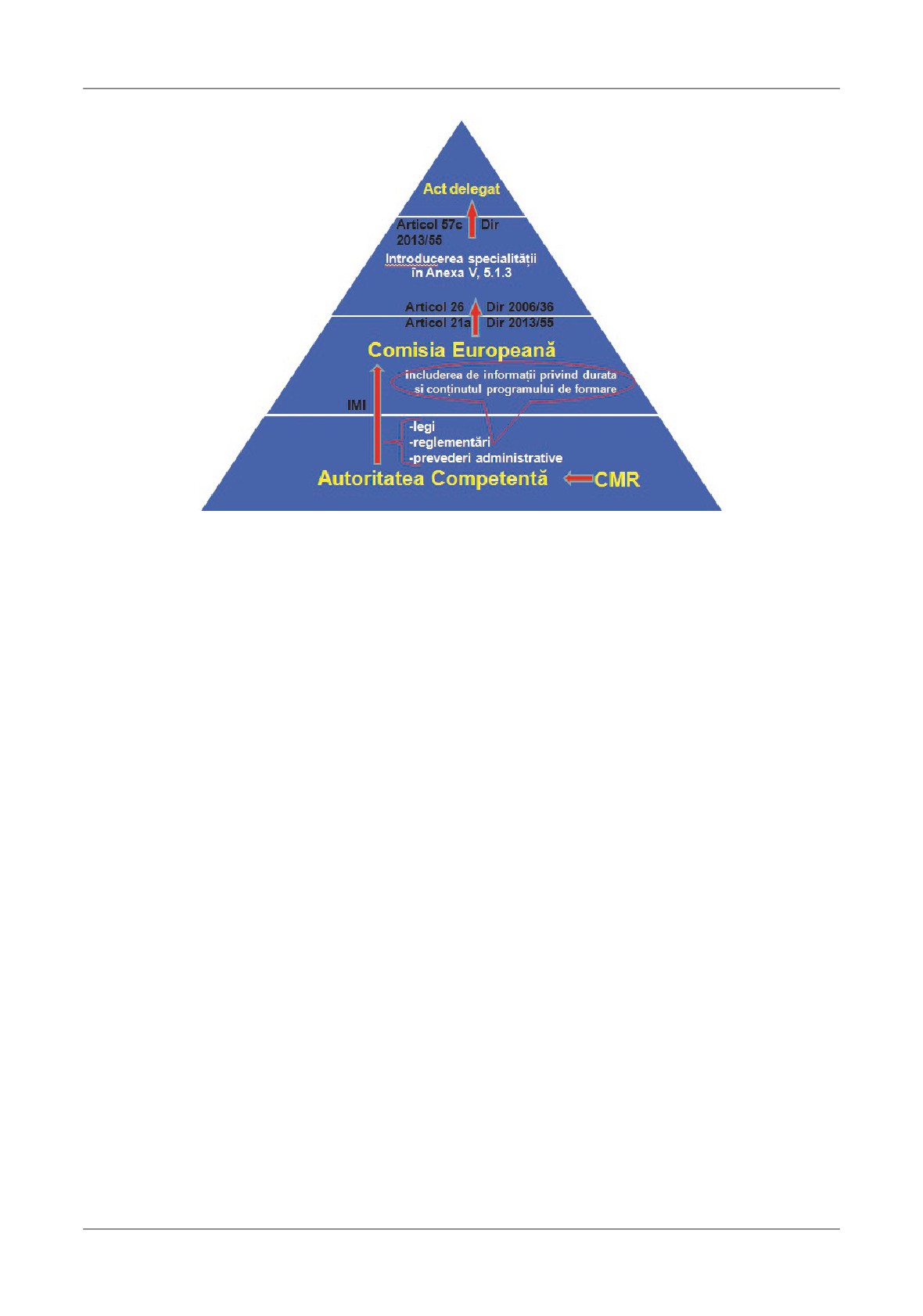
Path for European recognition
Te ideal path: request from the Competent
Te question for us is whether our specialty is “one
Authority via IMI to the European Commission,
among others”, or if we will choose a totally separate
presenting the laws, regulations and administrative
way. Is needed more integration with other specialties,
provisions adopted in the matter of issuing the title of
or more specificity?
qualifications as a specialist in Family Medicine,
9
Overview of Options for the Recognition of Family Medicine / General Medicine as a European Medical Specialty
Editorial
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
including information on the duration and content of
highly qualified and vocationally trained medical
training programs, in order to adopt delegated act under
graduates.
Dir. 2013/55, Article 57c by the European Commission,
After successful completion of their medical degree they
for introducing of the specialty of General Medicine/
have a period of hospital based training which is combined
Family Medicine in Annex V, 5.1.3 under Article 26 of
with specialist training for general practice involving a
the Dir 2005/36 revised by Dir 2013/55, and Article
period of supervised work within a GP training practice.
21a, the condition that the new specialty to be adopted
Tere are Chairs of General Practice/Family Medicine
in at least 2/5 of the EU states being satisfied.
in universities and most European countries recognize the
Te last developments - the UEMO Statement on
specialty of General Practice/Family Medicine.
Recognition of General Practitioners/Family Doctors
UEMO calls upon those countries that do not yet have
as Specialists, adopted in unanimity by the General
recognition of the Specialty to examine their own systems so
Assembly of UEMO, at Porto, in 11 of June 2016:
as to promote and achieve the recognition of GPs/FDs as
“UEMO, as an organisation of European General
Specialists in the field of General Practice/Family Medicine
Practitioners/Family Doctors, demands the recognition of
within one year.
General Practitioners as Specialists.
Furthermore UEMO pledges itself to pursue this goal
General Practice is the robust basis of any cost-
through the European Commission and the forthcoming
effective Health System and General Practitioners are
Directive in 2017 (Annex V, 5.1.3 and 5.1.4)”.
10
Bumbuluț
ORIGINAL ARTICLE
THE SOCIO-DEMOGRAPHIC CHARACTERISTICS ASSOCIATED WITH
THE INCREASED LIKELIHOOD OF SUBSEQUENT SCHIZOPHRENIA
Virgil Radu Enatescu1, Minodora Manea2, Radu Stefan Romosan1, Ana Maria Draghici3,
Valentin Alexandru Pinzaru1, Cristina Ana Bredicean1, Ion Papava1
1Department of Psychiatry, “Victor Babeș” University of Medicine and Pharmacy, Timișoara, 2Department of Medical
Psychology, “Iuliu Hațieganu” University of Medicine and Pharmacy Cluj Napoca and 3“Eduard Pamfil” Psychiatric
Clinic, Timișoara, România
Address for correspondence:
Virgil-Radu Enatescu
Department of Psychiatry, “Victor Babeș” University of Medicine and Pharmacy, Timișoara, România,
Timișoara, 21 Iancu Vacarescu St, PO 300182
Tel: +40 723374896, Fax: +40 356711617
Email: enatescu.virgil@umft.ro
Received: 09.05.2016
Accepted: 28.05.2016
Med Con June 2016 Vol 11, No 2, 11-20
Abstract
were associated with the increased likelihood for the
subsequent evolution towards schizophrenia diagnosis.
Introduction: Schizophrenia is the most disabling
Conclusions: Te identification of an initial socio-
psychiatric disorder whose clinical and functional
demographic profile associated with a high likelihood of
prognostic, at least in part, is contingent on the
subsequent evolution towards schizophrenia diagnosis
promptitude of treatment initiation. Establishing
should increase the accuracy in making a diagnosis of
diagnosis of schizophrenia is usuallydelayed at the first
schizophrenia, even from the first episode of psychosis.
episode of psychosis, which can impede a proper case
Keywords: first episode of psychosis, schizophrenia,
management.
socio-demographic characteristics
Te main objective of the research was to identify
the baseline socio-demographic characteristics at the
Introduction
first episode of psychosis associated with an increased
likelihood of evolution towards a diagnosis of
Psychosis is an extremely complex concept whose
schizophrenia following subsequent episodes.
meaning can vary from that of a singular clinical
Material and methods: Data from medical records
symptom to a comprehensive syndrome that consists of
of
100 patients that were admitted to the “Eduard
a well-delineated cluster of symptoms and ultimately
Pamfil” Psychiatric Clinic in Timișoara for two
could be considered as a psychiatric disorder distinctively
consecutive and distinct episodes of psychosis, were
named by psychiatric nosology.
analysed. Te first hospitalization overlapped with the
Over the last decades, psychiatric research has
first episode of psychosis.
unequivocally revealed, through several clinical and
Results: Binary logistic regression revealed that the
population studies, that the early identification and
mean age (OR=0.90, 95%CI 0.85-0.95), professional
detection of the first episode of psychosis could be crucial
status (OR=3.75, 95%CI 1.10-12.74) and the quality
to the subsequent evolution of this kind of major
of social support
(OR=3.47,
95%CI 1.11-10.82),
psychiatric disorder [1]. Moreover, diagnostic accuracy is
existing at the onset of the first episode of psychosis,
a frequent challenge in psychiatric clinical practice,
The Socio-Demographic Characteristics Associated with the Increased Likelihood of Subsequent Schizophrenia
11
ORIGINAL ARTICLE
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
especially when the patient is facing the onset of a first
psychosis, the first of which being considered as the first
psychotic episode. Regarding this issue, previous research
episode of psychosis.
has revealed that diagnostic stability, especially in the
Te inclusion criteria were as follows: the age of
first years of a psychiatric disorder with psychotic features
studied patients, which was between 18 and 65 years at
and severity, is relatively low, while frequent diagnostic
the time of the first psychiatric hospitalization; the
changes occur during future psychotic episodes [2,3].
presence of at least two consecutive psychiatric admissions
Research also shows a constant tendency to underdiagnose
in our clinic for two distinct episodes of psychosis, with
schizophrenia at the first episode [4]. Tis can be due to
both of them being assignable to one of the ICD-10
limited information obtained transversally at the first
schizophrenia spectrum disorders; the existence of a
episode, or it maybe because of the high stigma associated
distinct clinical remission period between the two
with this diagnostic label [5,6].
episodes of at least six months [13] but no more than two
Te correct identification and diagnosis of
years; the lack of any other comorbid psychiatric
schizophrenia, starting with the first episode, could
condition that could interfere with the interpretation of
improve the therapeutic strategy for the patient through
results; and finally, complete data in the selected patients
more effective case management, more active involvement
medical records. Hence, the following psychiatric
of the patient’s family and the establishment of a more
diagnoses assigned to schizophrenia spectrum disorders,
complex recovery plan, which takes into consideration
according to ICD-10, were taken into account: acute and
not only clinical remission but, most importantly,
transient psychotic disorders of any type; schizophrenia
attaining functional remission and recovery [7].
of any type; persistent delusional disorder of any type;
So far, the purpose of numerous researches has been
and, schizoaffective disorders of any type. Organic
the identification of biological, clinical and neuro-
psychosis and schizophrenia-like psychosis induced by
imagistic markers that can have a significant impact on
substance use or by a general medical condition were
diagnostic accuracy in schizophrenia starting from the
excluded, asthey were considered irrelevant for the
first episode, resulting in increased diagnostic validity
objective of our current research. In the current study,
[8-10].
there were no eligible patients with a diagnosis of
Given the general consensus regarding the notably
schizotypal disorder or induced delusional disorder.
negative outcome of the delayed diagnosis of
Out of 147 eligible patients, we excluded 33 of
schizophrenia, we consider the identification of those
them because they presented with a diagnosis other than
socio-demographic characteristics that could better
a psychotic disorder from the schizophrenia spectrum at
integrate the premorbid patient profile in those who are
the second admission (e.g., a diagnosis of an affective
at increased risk for schizophrenia to be of great value
episode with psychotic features), while we were unable
for clinical practice, even from the first psychotic
to obtain relevant information for our research for
episode, in order to improve the accuracy of psychiatric
another 14 patients. Finally, the total number of research
diagnosis in a timely manner.
patients was 100.
Te current study aimed to identify those baseline
Te study was conducted according to the
socio-demographic featuresof the first episode of
Declaration of Helsinki, the European Guidelines on
psychosis corresponding to one of the International
Good Clinical Practice and the requirements of relevant
Statistical Classification of Diseases and Related Health
national and regional authorities and ethics committees.
Problems
10th Revision
(ICD-10) schizophrenia
Methods
spectrum disorders [11,12], which are associated with
All socio-demographic data were collected and
an increased likelihood of a subsequent evolution
processed in the same standardized manner in an
towards an ICD-10 schizophrenia diagnosis at the
electronic file. Te following baseline socio-demographic
second episode of psychosis in the same patient.
variables associated with the first episode of psychosis
were taken into consideration: age at the onset of
Material and Methods
psychosis, gender, educational level, professional status,
marital status, residency and the quality of social support.
Participants and study design
All of these variables were uniformly collected as specific
A retrospective longitudinal study was carried out
items in full concordance with our medical records. In
on medical data records belonging to 100 patients, who
our research, the professional status of retired patients
were admitted twice to the Eduard Pamfil Psychiatric
was the result of medical reasons different from psychiatric
Clinic in Timișoara, between January 2010 and January
disorders; we couldnot find any link between those
2015, for two distinct and consecutive episodes of
medical conditions and the first episode of psychosis
12
Enatescu et al
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
ORIGINAL ARTICLE
(e.g., cardiovascular diseases). Whenever it was necessary,
relation to the psychiatric diagnosis established
supplementary data were gathered from psychiatrists
at the second episode of psychosis
involved in the treatment of selected inpatients and also
Te baseline socio-demographic features ofthe
from other attached clinical documents.
studied sample recorded at the first episode of
Data analysis
psychosisare presented in Table I, depending on the
SPSS version 17 for Windows was used to analyse
psychiatric diagnoses established at the second psychiatric
data. Te chi-squared test was used to compare
admission for a consecutive episode of psychosis.
frequencies of categorical variables, while the two-tailed
Regarding the mean age at the onset of the first
parametric t-test for independent samples was used to
episode of psychosis for the entire studied sample,
compare the means of continuous variables. Non-
depending on the diagnoses established at the second
parametric rank tests (the Mann-Whitney U-test and
episode of psychosis, we found significant differences as
the Kruskal-Wallis H test) were used to analyse ordinal
follows: the diagnosis of schizoaffective disorder had the
variables. In this sense, due to the abnormal distribution
lowest mean age at onset in comparison to the patients
of the variable represented by age at the first episode of
with persistent delusional disorders
(Kruskal-Wallis
psychosis, we chose non-parametric rank tests in order
Test; H=35.796, p<0.001). Te patients with a diagnosis
to analyse the differences between the distinct psychiatric
of schizophrenia had a slightly higher mean age at onset
diagnostic subgroups. Spearman rho correlations were
than patients with schizoaffective disorders, while the
determined in the case of ordinal dependent variables,
patients with a stable diagnosis of acute and transient
while Pearson correlation was used for continuous
psychotic disorders at both episodes had intermediary
variables. Te marginal homogeneity test was used to
mean age onset. Moreover, depending on gender
assess the stability of psychiatric diagnoses at the second
distribution at the second episode of psychosis, when we
episode of psychosis in comparison with the first episode.
compared the mean age onset of first episode psychosis
In order to evaluate the potential value of the
in schizophrenia, male patients had a lower mean age at
baseline socio-demographic factors in predicting an
onset than female patients, although it was not
increased likelihood of subsequent schizophrenia
statistically significant
(Mann-Whitney U Test;
diagnosisat the second episode of psychosis (treated as a
U=119.000, Z=-1.363, p=0.181).
binary dependent variable with 1 meaning presence of
Gender distribution of the four subsamples,
schizophrenia and
0 meaning the absence of
according to diagnoses at the second episode of
schizophrenia; hence, the presence of another
psychosis, showed interesting results. In the case of
schizophrenia spectrum diagnosis), we performed a
patients with schizophrenia as well as acute and transient
binary logistic regression with the ENTER method,
psychotic disorder, gender distribution wasequal or
with alpha set at 0.05. In the statistical process model,
almost equal for these two diagnoses. Differently, for
the residency was excluded because it was considered as
patients presenting with persistent delusional disorders
being less relevant for the proposed objectives.
and schizoaffective disorders, there was female
In order to facilitate statistical analysis, some
predominance. Tese differences did not reach statistical
independent variables were regrouped into two main
significance (X2=5.257, p=0.154).
categories: professional status was reorganized into with
Residency, whether urban or rural, presented a
an occupation (including employed and students at the
slightly different distribution depending on diagnoses at
first episode of psychosis) and withoutan occupation
the second episode of psychosis. Te distribution based
(including unemployed and retired for various reasons);
on residency showed that patients with schizophrenia
marital status was restructuredinto two groups, with a
and schizoaffective disorder resided in urban and rural
partner (married and in a relationship) and without a
areas alike, with the urban percentage being slightly
partner (single or divorced and not in a relationship);
higher. Meanwhile, patients with persistent delusional
and lastly, social support was reorganized as with
disorders and acute and transient psychotic disorders
satisfactory social support and with unsatisfactory social
resided mostly in urban settings but without statistical
support (those lacking social supportwere grouped with
significance (X2=3.839, p=0.279).
those with inadequatesupport).
If graduating at least from high school is considered
as having received a higher level of education, we
Results
observed that those who were diagnosed with
schizophrenia at the second episode of psychosis had the
Baseline socio-demographic characteristics
lowest percentage in comparison with those who were
associated with the first episode of psychosis in
diagnosed with acute and transient psychotic disorders,
13
The Socio-Demographic Characteristics Associated with the Increased Likelihood of Subsequent Schizophrenia
ORIGINAL ARTICLE
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
Table I. Te baseline socio-demographic features of the studied sample depending on the psychiatric diagnoses
established at the second episode of psychosis
Baseline socio-demographic
Schizophrenia of
Acute and
Persistent
Schizoaffective
parameters associated with the
any type
transient psychotic
delusional
disorders of any
first episode of psychosis
(n=36)
disorders of any
disorders of any
type (n=7)
type (n=21)
type (n=36)
Average age at the onset (years)
31.8
(9.914)
35.4
(11.097)
48.8
(10.901)
29.4
(7.323)
Gender distribution
Female
18 (50.0%)
12 (57.1%)
27 (75.0%)
5 (71.4%)
Male
18 (50.0%)
9 (42.9%)
9 (25.0%)
2 (28.6%)
Residency distribution
Urban area
21 (58.3%)
17 (81.0%)
26 (72.2%)
4 (57.1%)
Rural area
15 (41.7%)
4 (19.0%)
10 (27.8%)
3 (42.9%)
Educational level
Gymnasium
20 (55.6%)
8 (38.1%)
19 (52.8%)
3 (42.9%)
High school
13 (36.1%)
8 (38.1%)
11 (30.6%)
2 (28.6%)
University
3 (8.3%)
5 (23.8%)
6 (16.7%)
2 (28.6%)
Professional status
Unemployed
26 (72.2%)
13 (61.9%)
16 (44.4%)
4 (57.1%)
Employed
1 (2.8%)
6 (28.6%)
11 (30.6%)
3 (42.9%)
Student
4 (11.1%)
0 (0.0%)
0 (0.0%)
0 (0.0%)
Retired
5 (13.9%)
2 (9.5%)
9 (25.0%)
0 (0.0%)
Marital status
Married / cohabiting
9 (25.0%)
5 (23.8%)
21 (58.3%)
2 (28.6%)
Celibate
27 (75.0%)
16 (76.2%)
15 (41.7%)
5 (71.4%)
Widow
0 (0.0%)
0 (0.0%)
0 (0.0%)
0 (0.0%)
Te quality of social support
Lack of social support
5 (13.9%)
1 (4.8%)
2 (5.6%)
2 (28.6%)
Unsatisfactory socialsupport
14 (38.9%)
9 (42.9%)
8 (22.2%)
0 (0.0%)
Satisfactory social support
17 (47.2%)
11 (52.4%)
26 (72.2%)
5 (71.4%)
Te presence of smoking in the
year preceding FEPa
15 (41.7%)
9 (42.9%)
11 (30.6%)
4 (57.1%)
Te presence of alcohol use in the
12 (33.3%)
7 (33.3%)
12 (33.3%)
5 (71.4%)
year preceding FEPa
Age is indicated as a mean (SD)
aFEP - first episode psychosis
persistent delusional disorders
and schizoaffective
frequently favourable, meaning married or in a stable
disorders. Te differences in educational levels did not
relationship, for patients who were diagnosed with
differ statistically depending on psychiatric diagnoses at
persistent delusional disorders in comparison with those
the second episode of psychosis (Kruskal-Wallis Test;
who had schizophrenia at the second episode of
H=2.808, p=0.422).
psychosis. For patients with acute and transient
When we compared the cumulative percentage of
psychotic disorders and schizoaffective disorders, the
patients who were unemployed and retired, thereby
results were quite similar to those for schizophrenic
having an unsatisfactory professional status, we observed
patients. Te differences in marital status revealed by
that this percentage was higher for patients presenting
our research were statistically significant between
with schizophrenia in comparison with patients from
psychiatric diagnoses (X2=11.033, p=0.012).
the other diagnostic categories with statistical significant
If we consider satisfaction with social support, the
differences between psychiatric diagnoses that were
patients who evolved towards schizophrenia at the
taken into consideration in our research (X2=22.521,
second episode of psychosis had the lowest percentage
p=0.007).
for this quality of support starting from the onset of the
Regarding marital status, our results showed that
disorder, compared to patients with acute and transient
marital status at the first psychotic episode was more
psychotic disorders, persistent delusional disorders and
14
Enatescu et al
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
ORIGINAL ARTICLE
Table II. Binomial logistic regression predicting likelihood of subsequent schizophrenia
based on socio-demographic parameters associated with the first episode of psychosis
Socio-demographic parameters
B
SE
Wald
df
p
Odds
95% CI for Odds
associated with the first episode
Ratio
Ratios
of psychosis
Lower Upper
Age at onset
-0.101
0.027
13.753
1
0.000
0.904
0.858
0.954
Gender
0.532
0.562
0.896
1
0.344
1.702
0.566
5.123
Education level
-0.463
0.350
1.752
1
0.186
0.629
0.317
1.249
Professional status at the onset of
1.322
0.624
4.495
1
0.034
3.752
1.105
12.741
psychosis (without occupation)
Marital status at the onset of psychosis
-0.957
0.735
1.699
1
0.192
0.384
0.091
1.620
(without a partner)
Social support prior to psychosis
1.244
0.580
4.598
1
0.032
3.471
1.113
10.823
(unsatisfactory)
Constant
3.179
1.619
3.855
1
0.050
24.028
Note: Gender refers to males compared to females
schizoaffective disorders. However, statistical significance
patients with unsatisfactory social support at the first
for these differences was not reached
(X2=11.238,
episode of psychosis had the likelihood to evolve towards
p=0.081).
a schizophrenia diagnosis at the latter episode increase
Interestingly, patients with a diagnosis of
by three and a half times in comparison with their
schizoaffective disorder at the second episode self-
counterparts (OR=3.47, 95%CI 1.11-10.82).
reported smoking more often in the year preceding the
onset of their first psychotic episode than patients with
ICD-10 diagnosis distribution and short-term
other diagnoses, but this result did not reach statistical
diagnoses’ stability at the second episode of
significance (X2=1.041, p=0.307).
psychosis in comparison with the first episode
Likewise, alcohol use in the year preceding the onset
of psychosis
of psychosis was significantly more frequently self-
Psychiatric diagnoses’ distribution at the first
reported by schizoaffective patients compared with the
episode of psychosis and the stability of these diagnoses
frequency of alcohol consumption reported by all the
at the second episode presented a very dynamic
rest of the sample (X2=4.101, p=0.043).
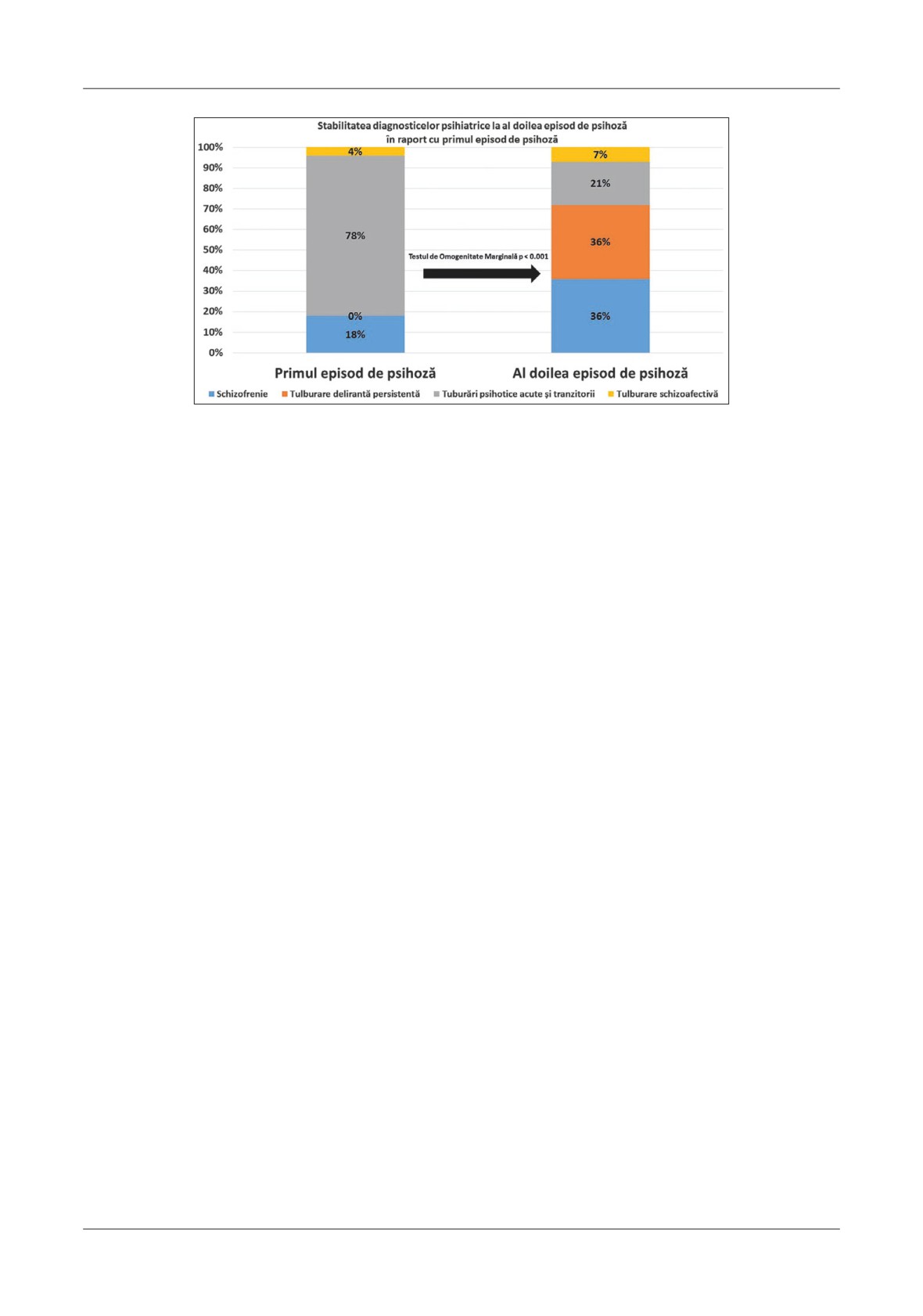
evolution pattern (Figure1).
It has been revealed that there was an obvious
Baseline socio-demographic parameters of first
restraint shown by psychiatrists in diagnosing
episode of psychosis associated with an increased
schizophrenia (18%) at the first episode of psychosis,
likelihood for a schizophrenia diagnosis at the
with most of them preferring instead the diagnosis of an
second episode of psychosis
acute and transient psychotic disorder of any type
With regard to the predictive value of baseline
(78%). Expectedly, regarding the first episode of
socio-demographic variables at the first episode of
psychosis, a diagnosis of persistent delusional disorder
psychosis, which are associated with an increased
was extremely rare (in our study, there was no case),
likelihood to evolve towards schizophrenia diagnosis at
immediately followed by schizoaffective disorder (4%).
the subsequent episode of psychosis, we found our
Even though schizophrenia and schizoaffective disorders
results tobevery interesting and meaningful (Table II).
were most likely underdiagnosed at the first episode of
Tus, binary logistic regression revealed that an
psychosis, these two diagnoses remained stable at the
older age at the onset of the first episode of psychosis
second episode of psychosis (a consistency rate of 100%
was associated with a decreased likelihood of evolution
for both diagnoses). In order to analyse the diagnostic
towards schizophrenia at second episode psychosis
stability for the entire studied sample between the two
(OR=0.90,
95%CI
0.85-0.95). An unfavourable
consecutive episodes of psychosis, we performed the
professional status (such as unemployment) at the first
marginal homogeneity test, which revealed a significant
episode of psychosis was associated with almost four
difference
(p<0.001) from first episode diagnoses
times more increase in the likelihood of a schizophrenia
compared to their distribution in the latter. Tis
diagnosis at second episode psychosis
(OR=3.75,
significant difference is conspicuously due to the high
95%CI 1.10-12.74). An interesting finding is that
instability of the diagnosis of an acute and transient
15
The Socio-Demographic Characteristics Associated with the Increased Likelihood of Subsequent Schizophrenia
ORIGINAL ARTICLE
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
Figure 1. Te stability of psychiatric diagnoses between
the first and second episode of psychosis
psychotic disorder, whose frequency lowered
first episode of psychosis, preferring instead to diagnose
dramatically (more than 50%) at the second episode of
it as an acute psychotic disorder, even if we are talking
psychosis.
about diagnoses such as acute and transient psychotic
disorder with schizophrenia or schizophrenia-like
Discussion
symptoms. We raise the issue that, starting with the first
episode of psychosis, the excessive diagnosis of acute
Despite the relative short time between the two
psychotic disorder, instead of schizophrenia, may raise
episodes that were taken into consideration, our research
more disadvantages in patient and family management,
has revealed consistent diagnosis instability. Te lack of
as well as the long-term therapeutic strategy. On the one
psychiatric diagnostic stability between the first and
hand, one study has revealed the important clinical
second episode of psychosis is due to the instability of
features that differentiate between these two psychiatric
the diagnosis of acute and transient disorders, which
disorders. Tus, in the case of schizophrenia, the long-
usually evolve towards other diagnostic categories,
term prognosis of the disorder is undoubtedly worse
mostly schizophrenia. Tis mirrors the results of other
than that for patients with acute and transient psychoses
international studies, raising the question of how well
[18]. On the other hand, from the ethical perspective,
this acute psychiatric diagnosis is defined and whether it
we have to note that, according to our nationwide
is partly a transitional diagnosis, being ultimately
health policy, the therapeutic protocols are much more
changed with a diagnosis of schizophrenia or other
restrictive with regard to the atypical antipsychotics
major psychiatric disorders of psychotic nature [14-17].
including their long acting injectable forms of
Based on the continuous medical care that our mental
administration, which are not allowed to be prescribed
health system provides, we have to mention that, in our
for other types of schizophrenia spectrum disorders
research,
98% of patients were treated during both
rather than for schizophrenia itself.
hospital admissions by the same psychiatrist and, in
Most studies show that schizoaffective disorder is
only
2% of cases they were treated by different
less frequent than schizophrenia (less than half ) [19,20];
psychiatrists. Tus, we are not able to assign this result
but, in our study, the odds ratio was 1:5, which indicates
on an inter-rater lack of confidence. We have to raise the
either underdiagnosed schizoaffective disorder at the
question of the accuracy of information obtained by the
first episode in our hospital, or as a direct consequence
psychiatrist at the first episode of psychosis, in regard to
of the study design and sample selection based on
the onset of observable psychotic symptoms. Te time
restrictive inclusion criteria.
criterion of one month is absolutely crucial for both
Te study revealed an interesting evolution
aforementioned diagnoses.
regarding persistent delusional disorders between the
Regarding our cultural background, we have to ask
two psychotic episodes. If this diagnosis was practically
ourselves whether the stigma associated with
absent at the first episode of psychosis, it almost matched
schizophrenia contributed to the restraint shown by the
schizophrenia in frequency at the second episode,
psychiatrist in referring to this diagnosis label from the
making it a preferred diagnosis or even an over-
16
Enatescu et al
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
ORIGINAL ARTICLE
diagnosed disorder at our clinic [21,22]. Te diagnostic
Regarding marital status, our finding that patients
preference of persistent delusional disorder over
with persistent delusional disorder have a more favourable
schizophrenia could also be caused by fewer stigmas in
marital status in comparison to the other three psychotic
our culture associated with this diagnosis. Another
disorders is reflected in other studies [29]. It becomes
reason for this may be that, in the diagnostic process at
obvious that patients with schizophrenia, acute and
the second episode of psychosis, the decision by the
transient psychosis and schizoaffective disorders have a
treating psychiatrist was influenced by the misbelief that
worse premorbid functionality when compared to
schizophrenia can only appear at a younger age, in turn
patients with persistent delusional disorders. Tis can be
disregarding the bizarre nature of the patient’s delusions
attributed in part to the younger age of onset for patients
and the constant presence of hallucinations. Tis could
with these diagnoses compared to persistent delusional
explain the overdiagnosis of persistent delusional
disorder, when it would have been too early for the
disorder over schizophrenia in our context.
patients to have a family [26].
Mean ages of the onset of our patients differed
Similar to other research, a worse professional status
significantly in regard to the psychiatric diagnoses at the
is associated with schizophrenia at the second psychotic
second episode of psychosis; these differences are in line
episode, followed by patients with acute psychosis and
with similar studies and epidemiology research [23-26].
schizoaffective patients. Patients with persistent
Of these, schizoaffective patients had the lowest mean
delusional disorder had better premorbid functionality
age at onset, but not significantly different from those
regarding the professional area [26,27,29]. Tis should
with schizophrenia. Other studies also confirm that
raise an alarm regarding the necessity of a more complex
patients with persistent delusional disorders had the
therapeutic approach, especially for patients with
highest onset mean age, which is statistically different
schizophrenia spectrum disorders. In support of
from the other diagnoses in our research [23,25]. Te
pharmacological treatment, we need to make more use
mean ages of onset in our research were similar to other
of cognitive and vocational rehabilitation in order to
studies [24,27], even though there were studies showing
achieve better recovery results [37,38].
significantly lower mean ages of onset [26]. Tis can be
Te quality of social support was frequently
partly explained by the time gap between detection and
unsatisfactory for schizophrenia patients, which shows
the duration of untreated psychosis, the only exceptions
that this particular diagnosis involves high levels of both
being patients with acute and transient psychosis where
cognitive and social impairment that affect the patient
the time criterion of one month is crucial for the
starting with several years before onset [34,39]. Tis
diagnostic process [28]. One study has shown a delay of
result reconfirms the necessity of psychosocial
3.5±4.3 years from onset to the first psychiatric hospital
interventions, especially in schizophrenic patients,
admission for patients with persistent delusional
which is in line with recent studies and could result in
disorder [29].
improving social cognition [40]. Furthermore, the lack
Gender distribution in our sample was similar to
of social and family support for schizophrenia patients
other studies showing that schizophrenia has an almost
outlines the genetic penetrance of this disorder in the
equal female/male odds ratio, with a slight preference
case of first degree relatives [41].
for males and a higher presence amongst females for the
In the current research, smoking and alcohol
other diagnoses [26,29-31].
consumption haveshown no statistically significant
Te educational level of patients who evolved
differences for schizophrenic patients compared to the
towards schizophrenia outlines the poor level of
other three diagnostic categories, which is comparable
premorbid adjustment of patients with this diagnosis,
to a previous study
[33]. However, from all the
compared to the other studied diagnoses [32,33]. On
schizophrenia spectrum disorders studied, schizoaffective
the one hand, the poor academic performance of
patients more frequently reported the premorbid use of
schizophrenia patients indicates that a cognitive
alcohol and tobacco. Tese particular behaviours may
impairment indeed exists and often precedes the onset
be related to the hedonic component of the disorder.
of the disorderby a number of years [34,35]. On the
Lastly, the research evidenced that, from all baseline
other hand, cognitive impairment measured by poor
socio-demographic variables associated with the first
academic performance represents an important clinical
episode of psychosis, younger age of onset, unsatisfying
guideline for differentiating schizophrenia from
professional status and poorer social support at the onset
persistent delusional disorder. When faced with a
could have a predictive value for a future schizophrenia
patient with cognitive impairment, a diagnosis of
diagnosis. Irrespective of the diagnoses at the first
schizophrenia becomes more valid [29,36].
episode of psychosis, these three socio-demographic
17
The Socio-Demographic Characteristics Associated with the Increased Likelihood of Subsequent Schizophrenia
ORIGINAL ARTICLE
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
factors together indicate a significantly higher likelihood
11.
World Health Organization.
1992. ICD-10
that a patient might evolve towards a schizophrenia
classifications of mental and behavioural disorder:
diagnosis at the subsequent episode of psychosis [33].
Clinical descriptions and diagnostic guidelines. Geneva:
Moreover, they might better integrate the socio-
World Health Organization.
demographic premorbid profile of those individuals
12.
Ritsner MS, Gottesman II. 2011. Te schizophrenia
who are at an increased risk of developing schizophrenia,
construct after 100 years of challenges. In: Handbook of
once the first episode of psychosis has occurred.
Schizophrenia Spectrum Disorders. Ritsner MS, editor.
Conflicts of Interest
Vol 1. Heidelberg, Germany: Springer, pp 1-44.
Te authors do not have any conflict of interest to
13.
Andreasen NC, Carpenter WT Jr, Kane JM, Lasser
report regarding this study.
RA, Marder SR, Weinberger DR. Remission in
Schizophrenia: Proposed Criteria and Rationale for
Consensus. Am J Psychiatry. 2005;162:441-9.
References
14.
Aadamsoo K, Saluveer E, Küünarpuu H, Vasar V,
Maron E. Diagnostic stability over 2 years in patients
1.
McGorry PD. Early intervention in psychosis: obvious,
with acute and transient psychotic disorders. Nord J
effective, overdue. J NervMent Dis. 2015;203(5):310-
Psychiatry. 2011;65(6):381-8.
318.
15.
Farooq S. Is acute and transient psychotic disorder
2.
Schwartz JE, Fenning S, Tanenberg-Karant M, et al.
(ATPD) mini schizophrenia? Te evidence from
Congruence of diagnoses 2 years after a first admission
phenomenology and epidemiology. PsychiatrDanub.
diagnosis of psychosis. Arch Gen Psychiatry.
2012;24(Suppl 3):S311-5.
2000;57:593-600.
16.
Castagnini A, Foldager L, Bertelsen A. Long-term
3.
Subramaniam M, Pek E, Verma S, Chan YH, Chong
stability of acute and transient psychotic disorders. Aust
SA. Diagnostic stability 2 years after treatment initiation
N Z J Psychiatry. 2013;47(1):59-64.
in the early psychosis intervention programme in
17.
Queirazza F, Semple DM, Lawrie SM. Transition to
Singapore. Aust N Z J Psychiatry. 2007;41(6):495-500.
schizophrenia in acute and transient psychotic disorders.
4.
Veen ND, Selten JP, Schols D, et al. Diagnostic
Br J Psychiatry. 2014;204:299-305.
stability in a Dutch psychosis incidence cohort. Br
18.
Pillmann F, MarnerosA. Longitudinal follow-up in
Journal Psychiatry. 2004;185:460-4.
acute and transient psychotic disorders and schizophrenia.
5.
Pini S, de Queiroz V, Dell’Osso L, et al. Cross-sectional
Br J Psychiatry. 2005;187:286-7.
similarities and differences between schizophrenia,
19.
Perala J, Suvisaari J, Saarni SI, et al. Lifetime prevalence
schizoaffective disorder and mania or mixed mania with
of psychotic and bipolar I disorders in a general
mood-incongruent psychotic features. Eur Psychiatry.
population. Arch Gen Psychiatry. 2007;64:19-28.
2004;19(1):8-14.
20.
Olfson M, Marcus SC, Wan GJ. Treatment patterns
6.
Wood L, Birtel M, Alsawy S, Pyle M, Morrison A.
for schizoaffective disorder and schizophrenia among
Public perceptions of stigma towards people with
Medicaid patients. Psychiatr Serv. 2009;60:210-6.
schizophrenia, depression, and anxiety. Psychiatry Res.
21.
Crowe R R. & Roy MA. 2008. Delusional disorders. In Te
2014;220(1-2):604-8.
Medical Basis of Psychiatry. S. H. Fatemi& P. J. Clayton
7.
Henry LP, Amminger GP, Harris MG, et al.Te
(Eds.) New York, USA: Humana Press, pp 125-31.
EPPIC follow-up study of first-episode psychosis: longer-
22.
SoykaM, Zingg C, BaumgärtnerG. Prevalence of
term clinical and functional outcome 7 years after index
delusional disorder among psychiatric inpatients: data
admission. J Clin Psychiatry. 2010;71(6):716-28.
from the German hospital register. Neuropsychiatry.
8.
Burton CZ, Vella L, Harvey PD, Patterson TL,
2011;4:319-23.
Heaton RK, Twamley EW. Factor structure of the
23.
Marneros A, Pillmann F, Wustmann T. Delusional
MATRICS Consensus Cognitive Battery (MCCB) in
disorders--are they simply paranoid schizophrenia?
schizophrenia. Schizophr Res 2013;146(1-3):244-8.
Schizophr Bull. 2012;38(3):561-8.
9.
Chung Y, Cannon TD.Brain imaging during the
24.
Castagnini A, FoldagerL. Variations in incidence and
transition from psychosis prodrome to schizophrenia. J
age of onset of acute and transient psychotic disorders. Soc
NervMent Dis. 2015;203(5):336-41.
Psychiatry PsychiatrEpidemiol. 2013;48(12):1917-22.
10.
Xu K, Schadt EE, Pollard KS, Roussos P, Dudley JT.
25.
Pagel T, Baldessarini RJ, Franklin J, BaethgeC.
Genomic and network patterns of schizophrenia genetic
Characteristics of patients diagnosed with schizoaffective
variation in human evolutionary accelerated regions.
disorder compared with schizophrenia and bipolar
MolBiolEvol. 2015;32(5):1148-60.
disorder. Bipolar Disord. 2013;15(3):229-39.
18
Enatescu et al
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
ORIGINAL ARTICLE
26.
Mancuso SG, Morgan VA, Mitchell PB, Berk M,
deficits
in schizophrenia. J Clin Psychiatry.
Young A, Castle DJ. A comparison of schizophrenia,
2014;75Suppl 2:25-9.
schizoaffective disorder, and bipolar disorder: Results
35.
Cuesta MJ, Sánchez-Torres AM, Cabrera B, et al.
from the Second Australian national psychosis survey. J
Premorbid adjustment and clinical correlates of cognitive
Affect Disord. 2014;30;172C:30-7.
impairment in first-episode psychosis. Te PEPsCog
27.
Pillmann F, Wustmann T, Marneros A. Acute and
Study. Schizophr Res. 2015;164(1-3):65-73.
transient psychotic disorders versus persistent
36.
Mehta UM, Tirthalli J, Subbakrishna DK,
delusional disorders: a comparative longitudinal
Gangadhar BN, Eack SM, Keshavan MS. Social and
study. Psychiatry ClinNeurosci. 2012;66(1):44-52.
neuro-cognition as distinct cognitive factors in
28.
Marshall M, Lewis S, Lockwood A, Drake R, Jones P,
schizophrenia: a systematic review. Schizophr Res.
CroudaceT. Association between duration of untreated
2013;148(1-3):3-11.
psychosis and outcome in cohorts of first-episode patients: a
37.
Choi KH, Fiszdon JM, Bell MD. Beyond cognition: a
systematic review. Arch Gen Psychiatry. 2005;62(9):975-83.
longitudinal investigation of the role of motivation
29.
Wustmann T, Pillmann F, Friedemann J, Piro J,
during a vocational rehabilitation program. J NervMent
Schmeil A, Marneros A. Te clinical and
Dis. 2013;201(3):173-8.
sociodemographic profile of persistent delusional disorder.
38.
Medalia A, Opler LA, Saperstein AM. Integrating
Psychopathol. 2012;45(3):200-2.
psychopharmacology and cognitive remediation to treat
30.
Castagnini A, Berrios GE. Acute and transient psychotic
cognitive dysfunction in the psychotic disorders. CNS
disorders
(ICD-10 F23): a review from a European
Spectr. 2014;19(2):115-20.
perspective. Eur Arch Psychiatry ClinNeurosci.
39.
Michaels TM, Horan WP, Ginger EJ, Martinovich Z,
2009;259(8):433-43.
Pinkham AE, Smith MJ. Cognitive empathy contributes
31.
DeRosse P, Burdick KE, Lencz T, Siris SG, Malhotra
to poor social functioning in schizophrenia: Evidence
AK. Empirical support for DSM-IV schizoaffective
from a new self-report measure of cognitive and affective
disorder: clinical and cognitive validators from a large
empathy. Psychiatry Res. 2014;220(3):803-10.
patient sample. PLoS One. 2013;8(5):e63734.
40.
Lindenmayer JP, McGurk SR, Khan A, et al.
32.
Levine SZ, Rabinowitz J. A population-based
Improving social cognition in schizophrenia: a pilot
examination of the role of years of education, age of
intervention combining computerized social cognition
onset, and sex on the course of schizophrenia. Psychiatry
training with cognitive remediation. Schizophr Bull.
Res. 2009;168(1):11-7.
2013;39(3):507-17.
33.
Ramirez N, Arranz B, Salavert J, et al. Predictors of
41.
Walder DJ, Faraone SV, Glatt SJ, Tsuang MT,
schizophrenia in patients with a first episode of psychosis.
Seidman LJ. Genetic liability, prenatal health, stress and
Psychiatry Res. 2010;175(1-2):11-4.
family environment: risk factors in the Harvard
34.
Nuechterlein KH, Ventura J, Subotnik KL,
Adolescent Family High Risk for schizophrenia study.
BartzokisG. Te early longitudinal course of cognitive
Schizophr Res. 2014;157(1-3):142-8.
19
The Socio-Demographic Characteristics Associated with the Increased Likelihood of Subsequent Schizophrenia
ISSN 1843-9306
Revista „Medical Connections/Conexiuni Medicale” are o vizibilitate naţională şi internaţională
prin indexarea în Journals Master List a bazei de date internaţionale Index Copernicus®, începând
cu numerele din anul 2009, precum şi datorită includerii în cadrul schimburilor cu Universitatea
Titu Maiorescu, Bucureşti, Facultatea de Medicină şi Medicină Dentară, Sackler School of
Medicine afliată la Universitatea Tel Aviv, Hasharon Hospital, Centrul Medical Rabin din Israel
şi Universitatea de Vest Vasile Goldiş, Arad.
Te journal “Medical Connections/Conexiuni Medicale” has a national and international
(ISSN e-serials 2068-8369), and due to the fact that the journal is included in an exchange
program between national and international universities such as Titu Maiorescu University,
Bucharest, Faculty of Medicine ans Dental Medicine, and Hasharon Hospital, Rabin Medical
Center Affiliated with Sackler School of Medicine, Tel Aviv University, and Vasile Goldiş Western
University of Arad, Romania. Te “Medical Connections/Conexiuni Medicale” is indexed in
Journals Master List of Index Copernicus®, isues since 2009
ORIGINAL ARTICLE
CORRELATION BETWEEN EXCESSIVE WEIGHT LOSS AND QUALITY
OF LIFE IMPROVEMENTS 12 MONTHS AFTER LAPAROSCOPIC
SLEEVE GASTRECTOMY
Viorel Dejeu1,3, Dănuț-Aurel Dejeu1,3, Paula Dejeu2, Aurel Babeș3
11st Surgical Clinic, 2Laboratory Service, Bihor County Emergency Clinical Hospital, affiliated to 3Faculty of Medicine
and Pharmacy, Oradea University, Oradea, Romania
Address for correspondence:
Viorel Dejeu
P-ta Nucetului, 22, Bl. BC4, Ap. 111
Oradea, Romania
E-mail: viodejeu@yahoo.com
Received: 02.02.2016
Accepted: 28.06.2016
Med Con June 2016 Vol 11, No 2, 21-28
Abstract
surgery is not proportionally reflected in improvement
of the QoL.
Background and aims: Bariatric surgery offers the
Keywords: laparoscopic sleeve gastrectomy, morbid
best treatment to realize long-term sufficient weight loss
obesity, quality of life, excessive weight loss,
in morbidly obese patients. Negative effect of obesity on
comorbidities
the quality of life (QoL) is increasingly often mentioned.
Te main objective of this study is to investigate the
Introduction
weight changes and the impact of laparoscopic sleeve
gastrectomy on quality of life in
1 year after the
Obesity became a global health issue in the last
procedure. Te relation between the excessive weight
decades. It has implications in the costs of health care
loss
(EWL) and the improvement in the QoL
and diminishes the quality of life. Obesity in his own
questionnaires was also assessed.
represent o psychosocial problem, but it is also
Material and Methods:
185 morbidly obese
accompanied with a rapid increase in health risks [1].
patients were evaluated before laparoscopic sleeve
Te continuous increase in a number of obese people
gastrectomy and 12 months after surgery. Te evaluation
is accompanied by an increase in a number of obesity-
included anthropometric measurements, SF-36 and
related diseases, including type
2 diabetes mellitus,
Moorehead-Ardelt Quality of Life Questionnaire II
hypertension, lipid disorders, or ischemic heart
(MA-QoLQ).
diseases [2].
Results: Te mean excessive weight loss percentage
Morbid obesity is defined as having a body mass
was 59.6%. All domains of SF-36 and also MA-QoLQ
index (BMI)≥40 or BMI≥35kg/m2 combined with at
showed significant improvement in 1 year (p<0.0001).
least one comorbid condition, such as type 2 diabetes
Any correlation between the extent of EWL and
mellitus
(T2DM), hypertension, dyslipidemia, or
differences between the total score of QoL questionnaires
obstructive sleep apnea.
couldn’t be demonstrated (rho=-0.0134, p=0.8563).
In 1946, the World Health Organization in its
Conclusions: Surgical treatment results in a
constitution defined health as a state of complete
significant improvement in the quality of life. Te extent
physical, mental, and social well-being and not merely
of body weight loss achieved by a patient following the
the absence of disease or infirmity. Terefore, the
Correlation between Excessive Weight Loss and Quality of Life Improvements 12 Months after Laparoscopic
21
Sleeve Gastrectomy
ORIGINAL ARTICLE
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
modern concept of health also covers the quality of life,
selected from the patients admitted in the 1st Surgery
and a sense of health is one of its basic determinants.
Clinic of Bihor County Emergency Clinical Hospital,
According to many authors, a sense of health is, actually,
Oradea, Romania and Medlife-Genesys Clinic, Arad,
a fundamental condition determining a good quality of
Romania for laparoscopic sleeve gastrectomy in the
life. Amongst numerous complications related to obesity
period January 2011-December 2015.
and overweight, apart from somatic diseases affecting
Te approval of the Ethical Committee for both
function of individual organs and systems, their negative
hospitals was obtained for the study design. Informed
effect on the quality of life is increasingly mentioned.
consent was signed by every patient being an essential
Practitioners are confronted with various options
criterion in entering the study.
for weight loss but only bariatric surgery offers the best
Te inclusion criteria for this study were: BMI
treatment to realize long-term sufficient weight loss in
exceeding 40kg/m2 or - BMI exceeding 35kg/m2, when
morbidly obese patients [3,4]. Besides weight loss, it
diagnosed with obesity related diseases, including type 2
also has profound effects on obesity-related
diabetes, hypertension, lipid disorders, or obstructive
comorbidities, such as T2DM, hypertension and
sleep apnea for more than 3 years and age between 18-
obstructive sleep apnea [5,6].
65 years.
Laparoscopic Roux-en-Y gastric bypass (LRYGB)
Te exclusion criteria were: patients with psychiatric
represents the golden standard in bariatric surgery and is
and/or psychological disorders, symptomatic gastro-
the most frequently used surgical procedure all over the
esophageal reflux disease, prior bariatric surgery, prior
world [7,8]. Tere are some clear advantages that make
major abdominal surgery and inability of reading or
LRYGB the favorite bariatric procedure: fully reversible,
understanding the questionnaires.
the best long term results documented in many clinical
Using the above described selection criteria we
studies. Laparoscopic sleeve gastrectomy
(LSG)
selected 237 patients. From these, 205 patients signed
represents a newer bariatric procedure; it was started as
the informed consent to participate in the study. At the
the first stage intervention of the duodenal switch (DS)
follow-up only
187 patients presented and
185
in morbidly obese patients to permit a safer treatment
completed the questionnaires for QoL assessment.
modality in terms of anesthetic and surgical risks. Te
Te patients qualified for surgery underwent an
observation was that only 25% of patients necessitated a
initial screening. Te screening included a detailed
second intervention due to sufficient weight loss from
medical interview, physical examination, anthropometric
LSG, thus LSG is nowadays used as an independent
measurements, and an initial quality of life assessment.
surgical bariatric procedure. LSG gained popularity in
Obesity related comorbidities that persist for more than
this decade representing 28% of bariatric procedures
3 years were noted.
made worldwide [8]. As advantages of the LSG we can
Quality of life assessment
mention that it is faster and safer procedure and you can
Te quality of life in patients treated surgically for
still reach the duodenum with gastroscopy. One of the
morbid obesity was assessed with licensed, standardized
more important disadvantages of the LSG is that it is
and developed for medical purposes forms, SF-36 (Short
irreversible. If we compare quality of life (QoL) after
Form Health Survey) and MA-QoLQII (Moorehead-
LSG and LRYGB we can find the same or even better
Ardelt Quality of Life Questionnaire II).
improvement due to the mentioned advantages [9,10].
Te SF-36 [11] is a 36-item measure of general
Te main objective of this study is to investigate the
health related quality of life (HRQoL), consisting of
weight changes and the impact of laparoscopic sleeve
eight subscales
(physical functioning, role physical,
gastrectomy on quality of life one year after the
bodily pain, general health, vitality, social functioning,
procedure. Te relation between the excessive weight
role emotional and mental health) and two summary
loss and the improvement in the QoL questionnaires
scores
(Physical Component Summary
[PCS] and
was also assessed. As secondary endpoints we noted the
Mental Component Summary
[MCS]). Te two
effect of this bariatric procedure on obesity related
summary scores represent independent indices based on
comorbidities.
factor analysis of subscale scores using the Medical
Outcomes Study data. Scores on all subscales and PCS
Material and Methods
and MCS range from 0 to 100, where 100 represent the
best HRQoL. Scores for PCS and MCS are norm based,
Patients
with a mean of 50 and a standard deviation of 10. Te
Te present study was conducted by a surgical team
SF-36 has been shown to have strong psychometric
from January 2011 to December 2015. Te cases were
properties [11].
22
Dejeu et al
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
ORIGINAL ARTICLE
Te use of a disease-specific QoL instrument has
been recommended in combination with a generic
questionnaire [12]. One of the most commonly used
questionnaires to assess bariatric surgery outcomes is the
Bariatric Analysis and Reporting Outcome System
(BAROS). It includes three main fields of analysis, weight
loss, improvement of medical conditions, and QoL.
Changes of QoL in BAROS are assessed by means of the
Moorehead-Ardelt Quality of Life Questionnaire II (MA
QoLQII), considered an adequate tool to examine the
Figure 1. Laparoscopic sleeve gastrectomy -
QoL of severely obese individuals [13,14]. Individuals are
staplers placed on the resection margins
questioned about their self-esteem, physical activity, social
life, labor, sexual activity, and the way they approached
itself. Te last stapler is fired lateral to Belsy’s fat leaving
food, in scores ranging from -0.5 to +0.5 [13]. Te sum
the esophagus unharmed.
of these 6 scores generates an overall QoL score. Each
Finishing: next, the left trocar site is dilated and the
score is classified into 5 categories (very poor: -3.0 to -2.1;
resected stomach is removed. Subsequently, this trocar
poor: -2.0 to -1.1; average: -1.0 to +1.0; good: 1.1 to 2.0:
site is closed at fascia level. Te gastric tube is removed
and very good: 2.1 to 3.0).
by the anesthesiologist under laparoscopic vision. Staple
Surgical technique
line bleeding is controlled by clips and when necessary
Two different known approaches have been
with sutures. Only in case of bleeding, stapling
described in the literature
[15,16]: the stapling first
problems, or other difficulty, a drain is placed along the
technique or the full mobilization of the greater gastric
sleeve gastrectomy. Over-sewing of the staple line is not
curvature first technique. As a tight gastric sleeve, which
routinely performed. Next, the trocars are removed
is important for an optimal weight loss result, seems to
under sight and the skin is closed.
be realized best by the gastric mobilization first
Follow-up
technique [17] this is the only LSG technique used for
12 months after the surgical procedure the patients
this study.
who entered the study were reevaluated. Tis assessment
Starting: after achieving pneumoperitoneum, with a
included a physical examination, anthropometric
Veress needle in the left upper quadrant, five trocars are
measurements, reevaluation of the QoL questionnaires
placed according to the surgeons preference.
and obesity related comorbidities.
Mobilization: the greater curvature is dissected
Percentage of excess weight loss
(%EWL) was
downward to 2-3cm proximal to the pylorus. Next the
calculated by dividing the amount of weight loss after
greater curve is further mobilized up to the angle of His,
surgery by the amount of preoperative excess body
visualizing the complete left diaphragm crus. While
weight (calculated as that excess to yield a BMI of 25kg/
mobilizing the greater curve all gastro-pancreatic
m2) and multiplied by 100 [18].
adhesions at the dorsal smaller gastric curve are also
Statistical analysis
released in upward direction towards the angle of His.
We used MedCalc version
12.5.0.0
(MedCalc®
Tis step is important in order to be able to realize a
Software, Mariakerke, Belgium) for statistical analysis.
small gastric sleeve without redundant fundus at the
Te Kolmogorov-Smirnov test was applied to examine
dorsal gastric wall. Staplin: a linear 60 mm endoscopic
normal distribution. Continuous variables with normal
stapler is introduced through the right trocar and fired
distribution are presented as mean and standard
at the antrum, leaving just enough space for a gastric
deviation
- SD (in brackets); those with skewed
boogie to pass. Next an orally introduced gastric tube is
distribution as median and interquartile range
(in
inserted up to the pylorus. Tis gastric tube is 34 French
brackets). Categorical variables were presented as
(Fr) in diameter as it is important to create a small
number of patients and percentage. Because this is a
gastric sleeve. A tight sleeve is realized by firing another
follow-up study we used the paired sample t-test,
4-5 60mm long linear staple lines using the same trocar
respectively the Wilcoxon test to study the evolution of
site. Te stapler is placed tight to the tube while
the objectives comparing pairwise results. Te
stretching the greater curve (Figure 1). Each time after
correlation between weight loss and QoL improvement
placing the stapler the gastric tube is moved by the
was assessed by the Spearman rank correlation
anesthesiologist under laparoscopic vision in order to
coefficient. All p-values are two-sided with statistical
ensure that the stapler has not been placed on the tube
significance evaluated at the 0.05 alpha levels.
23
Correlation between Excessive Weight Loss and Quality of Life Improvements 12 Months after Laparoscopic
Sleeve Gastrectomy
ORIGINAL ARTICLE
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
Results
remained only 44 (48.8% decrease) - p=0.0001. Te
overall one-year self-reported OSAS remission rate was
Te baseline characteristics of the analyzed
185
63.9% (53 patients from 83 initially) - p=0.0001.
patients are presented in the next Table.
For all quality of life parameters assessed with the
Following the surgical treatment, a significant body
SF-36 form, statistically significant change was noted in
mass reduction was achieved in all patients. Te average
time. Te average value of the global quality of life index
body mass index, measured in the studied group during
was 143.6 (±29.5) and was statistically significant versus
the follow-up visit 12 months post-surgery was 34.4kg/
the initial value of 68.9 (±25.1). All the components of
m2 (ranging from
23.3 to
45.9kg/m2)
(p<0.0001
the QoL questionnaire improved significantly
12
compared to pre-surgery values). Te average percentage
months after surgery.
excessive weight loss (%EWL) was 59.6%.
On the basis of answers given by patients to
During the follow-up visits, significant reduction in
questions in the Moorhead-Ardelt Quality of Life
severity of comorbidities was also observed. Type
2
Questionnaire II we registered the following results
diabetes mellitus presented significant reduction in
(illustrated also in Figure 2). Before surgery in 3 patients
antidiabetic treatment in 58 patients from 81 (71.6%)
(1.6%), the quality of life was assessed as very bad, in 38
- p<0.0001; and complete remission (no treatment
(20.5%) patients, as bad, and in 110 (59.5%), as an
needed) in 17 cases (20.9%) - p=0.0884. Hypertension
average. Te quality of life assessed as good and as very
were resolved (normal values without medication) in
good was described in 25 (13.5%) and in nine (4.9%)
37.6% of cases (50 patients out of 133 initially) -
patients, respectively.
12 months after the surgical
p<0.0001 and incomplete improvement (reduction of
procedure no patient was assessed as very bad, in three
antihypertensive therapy) in 43.6% of cases (58patients
(1.6%) patient, the quality of life was assessed as bad,
from 133) - p<0.0001. From 86 patients who took lipid
and in 52 (28.2%), as an average. Te quality of life was
lowering
medication before surgery after
1 year
assessed as good and very good in 70 (37.8%) and in 60
Table I. Baseline characteristics of the patients (before surgery)
Characteristics
Surgery group (n=185)
Age (years) - mean (SD)
44.2
(10.6)
Gender (Male/Female) - number (percentage)
49/136 (1:2.8)
BMI (kg/m2) - mean (SD)
53.9
(7.8)
Hypertension - number (percentage)
133 (71.9%)
T2DM - number (percentage)
81 (43.8%)
Lipid disorders with statin therapy - number (percentage)
86 (46.5%)
OSAS - number (percentage)
83 (44.9%)
SD - standard deviation; BMI - body mass index; T2DM - type 2 diabetes mellitus; OSAS - obstructive
sleep apnea syndrome
Table II. Summary of results for the SF-36 questionnaire obtained before and 1 year after surgery
Component - mean (SD)
Pre-surgery
Post-surgery
p
Physical function
35.1
(28.4)
56.2
(27.1)
<0.0001
Role physical
32.3
(40.2)
55.7
(41.2)
<0.0001
Body pain
45.6
(21.8)
58.1
(27.2)
<0.0001
General health
38.2
(25.7)
53.9
(23.5)
<0.0001
Vitality
41.3
(21.6)
56.1
(23.1)
<0.0001
Social functioning
43.1
(30.2)
52.3
(26.3)
0.0019
Emotional role
31.9
(40.8)
52.8
(41.8)
<0.0001
Mental health
39.3
(20.1)
50.2
(18.9)
<0.0001
Physical component
38.2
(10.0)
57.1
(12.1)
<0.0001
Mental component
39.8
(8.9)
50.8
(10.8)
<0.0001
Global quality of life
68.9
(25.1)
143.6
(29.5)
<0.0001
SD - standard deviation
24
Dejeu et al
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
ORIGINAL ARTICLE
(32.4%) patients, respectively
(Figure
2).
Te
Discussion
comparison of these results showed significant
improvement also in the terms of the disease specific
Te fact of the negative effect of obesity and its
QoL instrument (p<0.0001).
related diseases on the quality of life is commonly
To answer the question whether a rate of body mass
known [19]. Numerous clinical studies and publications
loss influences a degree of the quality of life
showed clearly that the quality of life of obese people is
improvement, the obtained index for assessment of
worse than of people with normal body weight. Tis
bariatric treatment effectiveness (%EWL) was correlated
concerns not only the quality of life related to physical
with average changes in the global quality of life. Te
function, for example, intolerance of physical exercise,
non-parametric Spearman’s correlation was used for a
problems with moving, or pain, but also the quality of
statistical analysis. No significant correlation was found
life related to psychical aspects, including lack of
for analyzed variables: rho=-0.0134, p=0.8563
acceptance of themselves, increased stress level, reduced
(Figure 3).
self-esteem and mood, or depressive states
[20]. A
continuous increase in the number of obese people is,
therefore, tantamount to a continuous increase in the
group of people with reduced quality of life, in its
physical and mental dimensions.
Current expectations of patients suffering of morbid
obesity towards medical care include actions not only
improving their health but also leading to their psychical
and emotional well-being [21]. An effective method for
treatment of patients with morbid obesity, resulting in a
permanent weight loss, is surgical treatment. BMI
reduction post-surgery is also accompanied by
advantageous metabolic changes, which in some patients
result in observed reduced severity or complete reversal
of diseases caused by obesity. Tus, the reduced body
mass together with a general health improvement lead
Figure 2. Results of the Moorhead-Ardelt Quality of Life
Questionnaire II - number of cases in different categories
to improvement on the quality of life of treated patients.
before and 12 months after sleeve gastrectomy
Terefore, improvement on the quality of life, besides
Figure 3. Correlation between SF-36 total score difference and extra weight loss
percentage - no linear correlation found between the weight loss and QoL
improvement
25
Correlation between Excessive Weight Loss and Quality of Life Improvements 12 Months after Laparoscopic
Sleeve Gastrectomy
ORIGINAL ARTICLE
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
treatment of obesity and diseases accompanying it, has
concerning the quality of life assessed on a basis of the
become one of the main aims of bariatric treatment.
SF-36 questionnaire in the group of patients operated
During the follow-up visit that took place one year
only with the LRYGB method. Similarly to our study,
after the surgery, the average body mass index was
the author observed a significant improvement in all
34.36kg/m2, and this means an average body mass index
studied parameters. In most cases, their values for the
reduction of
19.55kg/m2). Te obtained results are
studied population post-surgery exceeded the standard
statistically significant (p<0.0001). Tese results do not
[27]. Similar results were also presented by Sarwer.
differ from data that can be found in the literature. For
Interestingly, a significant improvement for all
example, in the Coupaye report, the body mass index
parameters specified in the questionnaire was noted
loss one year post sleeve gastrectomy was 15.9kg/m2
already after 20 weeks from the surgical treatment, and
[22]. Whereas in the Swedish study, Torgerson and
with time, changes progressed further, but to a much
Sjöström showed an average percentage excessive weight
smaller extent. Tis was a period in which the body
loss (%EWL) post-surgery was 58.8% [23].
mass reduction did not reach its final value and diseases
Our findings of considerably lower frequencies of
accompanying obesity probably were not reversed [29].
diabetes, hypertension, dyslipidemia and sleep disorders
Tis supports our hypothesis that the very fact of having
12 months after surgery are in agreement with other
a surgery resulted in a significant improvement on the
studies [24,25]. Martínez et al. observed an improvement
quality of life. Te results obtained in our study are
in diabetes mellitus and hypertension control, a marked
therefore consistent with reports of other authors.
decrease in lipid alterations, and complete resolution of
When analyzing results obtained with the MA
sleep apnea syndrome [26].
QoLQII questionnaire post-surgery, it was found that
After surgery, all the domains of SF-36, as well as
the quality of life assessed with this tool also was
physical and mental summary measures were better
improved after surgical treatment. In as many as 70.2%
than before surgery, and reached levels similar to those
of
185 patients, the quality of life post bariatric
observed in normal populations [27]. Tese results are
treatment was assessed as very good or good. In the
in agreement with the findings of marked improvement
group of remaining people, in the significant majority,
or even normalization of all
8 domains of SF-36
the quality of life was assessed as average that is,
obtained prospectively by other investigators [27,28].
corresponding to the general standard. Al Harakeh
Te average value for the whole studied group was 68.9
presented similar results concerning improvement on
points, significantly differing from the accepted
the quality of life post bariatric surgery, as estimated on
standard, and this signifies a deteriorated quality of life
a basis of the BAROS questionnaire [30].
in its psychical dimension in all treated people. In
It was also found that the degree of the body mass
Sarwer’s study, in analyzing the effect of the LRYGB
reduction post-surgery does not influence the degree of
procedure on the quality of life of operated patients, the
quality of life improvement. Both people with low and
SF-36 questionnaire was also used. Te quality of life
high values for parameters evaluating the bariatric
index value was only 52.3. Te quality of life index in its
treatment effectiveness
(%EWL) reached similar
physical and psychical dimensions was estimated to be
improvement on the quality of life. Tese observations,
48.7 and 62 points, respectively. Tus, these values were
despite lack of extensive literature on this subject, seem
lower than in the group studied by us [29].
to be the most interesting result of the conducted study.
In the whole studied group, the quality of life one
Tere are opinions in the literature indicating significant
year post-surgery was 143.6 points. Tis value visibly
differences in treatment results for such diseases as type
exceeds the standard for the Romanian population, and
2 diabetes mellitus, hypertension, or lipid disorders
this may seem strange, as hardly any of the patients
depending on the body mass reduction rate and type of
achieved an optimal body weight following bariatric
the surgery. However, the results of the conducted study
treatment. Despite still being overweight or even obese,
indicate a completely different effect of the bariatric
the quality of life post-surgery was better than the
surgeries on the quality of life. It seems that the very fact
hypothetical quality of life of an overweight person not
of bariatric surgery is more important for improvement
qualifying for surgical treatment. Some patients post-
on the quality of life than the body mass reduction rate.
surgery still
required treatment for diseases
Terefore, following the conducted study, we are of the
accompanying obesity, but still, their quality of life was
opinion that there is no relationship between the degree
higher than average. Analogous observations were made
of body mass reduction and the level of improvement
when analyzing individual determinants for the quality
on the quality of life. Also, in the Sarwer study, no
of life. In similar studies, de Zwaan presented results
significant differences were observed for improvement
26
Dejeu et al
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
ORIGINAL ARTICLE
on the quality of life in relation to the degree of body
5.
Maggard MA, Shugarman LR, Suttorp M, Maglione
mass reduction [29]. However, data in the literature
M, Sugerman HJ, Livingston EH, et al. Meta-analysis:
confirming our observation is scarce. Terefore, it seems
surgical treatment of obesity. Ann Intern Med.
necessary to conduct more extensive studies in that area.
2005;142(7):547-59.
Study limitations
6.
Sjöström L, Narbro K, Sjöström CD, Karason K,
Te study population was relatively small; this
Larsson B, Wedel H, et al. Effects of bariatric surgery
might result in inadequate power to detect a slight
on mortality in Swedish obese subjects. N Engl J Med.
difference in clinical outcomes in time. Terefore, it will
2007;357(8):741-52.
be more informative if a larger sample size is studied. In
7.
Buchwald H, Avidor Y, Braunwald E, Jensen MD, Pories
addition, there are confounding risk factors that couldn’t
W, Fahrbach K, et al. Bariatric surgery: a systematic review
be evaluated related to the changes in health related
and meta-analysis. JAMA. 2004;292(14):1724-37.
quality of life (changes in economic, social or familial
8.
Buchwald H, Oien DM. Metabolic/bariatric surgery
circumstances). Tese can constitute limitations of the
worldwide 2011. Obes Surg 2013;23(4):427-36.
present study.
9.
Peterli R, Borbely Y, Kern B, Gass M, Peters T,
Turnheer M, et al. Early results of the Swiss Multicentre
Conclusions
Bypass or Sleeve Study (SM-BOSS). Annals of Surgery.
2013;258(5):690-5.
It should be emphasized again that for people with
10.
Overs SE, Freeman RA, Zarshenas N, Walton KL,
morbid obesity, surgical treatment results in a significant
Jorgensen JO. Food tolerance and gastrointestinal
improvement in the quality of their life, regardless of how
quality of life following three bariatric procedures:
much it has been deteriorated by the disease. Additionally,
adjustable gastric banding, Roux-en-Y gastric bypass
it also is surprising that the extent of body weight loss
and sleeve gastrectomy. ObesSurg. 2012;22(4):536-43.
achieved by a patient following the surgery is not
11.
Ware J, Snow K, Kosinski M, Gandek B. SF-36
proportionally reflected in improvement of the quality of
Health Survey: Manual and Interpretation Guide. Te
life. Te fact that the quality of life post bariatric treatment
Health Institute, New England Medical Center,
is so spectacularly improved is a strong argument
Boston, MA, 1993.
supporting qualification of patients with morbid obesity
12.
LeMonte D, Moorehead MK, Parish MS, Reto CS,
for surgical treatment, despite a high level of difficulty of
Ritz SJ. Suggestions for the pre-surgical psychological
the procedure and related potential risks. Nonetheless,
assessment of bariatric surgery candidates. American
long-term observation of the quality of life after bariatric
Society for Bariatric Surgery, October, 2004. Available
surgery seems to be necessary.
Duality of interest -no conflicts of interest.
13.
Moorehead MK, Ardelt-Gattinger A, Lachner H,
Oria HE. Te validation of the Moorehead-Ardelt
Quality of Life Questionnaire II. Obes Surg.
References
2003;13(5):684-92.
14.
Oria E, Moorehead MK. Bariatric Analysis and
1. Calle EE, Tun MJ, Petrelli JM, Rodriguez C, Heath
Reporting Outcome System
(BAROS). Obes Surg.
CW Jr. Body-mass index and mortality in a prospective
1998;8(5):487-99.
cohort of U.S. adults. N Engl J Med.
15.
Chu CA, Gagner M, Guinn T, et al. Two stage
1999;341(15):1097-105.
laparoscopic biliopancreatic diversion with duodenal
2. World Health Organisation. Obesity and overweight.
switch: an alternative approach to super-super morbid
Fact Sheet. 2006;311.
obesity. SurgEndosc. 2002;16:S069.
3. Elte JWF, Castro Cabezas M, Vrijland WW, Ruseler
16.
Wölnerhanssen B, Peterli R. State of the art: sleeve
CH, Groen M, Mannaerts HH. Proposal for a
gastrectomy. Dig Surg. 2014;31(1):40-7.
multidisciplinary approach to the patient with morbid
17.
Gadiot R, Biter LU, Zengerink HJ, de Vos tot
obesity: the SintFranciscus Hospital morbid obesity
NederveenCappel RJ, Elte JW, Castro Cabezas M, et
program. Eur J Intern Med. 2008;19(2):92-8.
al. Laparoscopic sleeve gastrectomy with an extensive
4. Gloy VL, Briel M, Bhatt DL, Kashyap SR, Schauer
posterior mobilization: technique and preliminary
PR, Mingrone G, et al. Bariatric surgery versus non-
results. Obes Surg. 2012;2(2):320-9.
surgical treatment for obesity: a systemic review and
18.
Biesemeier C, Garland J. ADA pocket guide to bariatric
meta-analysis of randomised controlled trials. BMJ.
surgery. Chicago, IL, USA: American Dietetic
2013;347:15934.
Association, 2009.
27
Correlation between Excessive Weight Loss and Quality of Life Improvements 12 Months after Laparoscopic
Sleeve Gastrectomy
ORIGINAL ARTICLE
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
19.
Kushner RF, Foster GD. Obesity and quality of life.
26.
Martínez Y, Ruiz-López MD, Giménez R, Pérez de La
Nutrition. 2000;16(10):947-52.
Cruz AJ, Orduña R. Does bariatric surgery improve the
20.
Kolotkin RL, Meter K. Quality of life and obesity.
patient’s quality of life? Nutr Hosp. 2010;25(6):925-
Obes Rev. 2001;2(4):219-29.
30.
21.
Fontaine KR, Cheskin LJ, Barofsky I. Health-related
27.
De Zwaan M, Lancaster KL, Mitchell JE, Howell
quality of life in obese persons seeking treatment. J
LM, Monson N, Roeriq JL, et al. Health related
FamPract. 1996;43(3):265-70.
quality of life in morbidly obese patients: effect of gastric
22.
Coupaye M et al. Comparison of nutritional status
bypass surgery. Obes Surg. 2002;12(6):773-80.
during the first year after sleeve gastrectomy and Roux-
28.
Dymek MP, Le Grange D, Neven K, Alverdy J.
en-Y gastric bypass. Obes Surg. 2014;24(2):276-83.
Quality of life and psychosocial adjustment inpatients
23.
Torgerson JS, Sjöström L. Te Swedish Obese Subjects
after Roux-en-Y gastric bypass: a brief report. Obes
(SOS) study-rational and results. Int J Obes. 2001;25:S2-4.
Surg. 2001;11(1):32-9.
24.
Christou NV, Sampallis JS, Liberman M, Look D,
29.
Sarwer DB,Wadden TA,Moore RH,Eisenberg
Auger S, McLean AP, et al. Surgery decreases long-term
MH,Raper SE,Williams NN.Changes in quality of life
mortality, morbidity and health care use in morbidly
and body image after gastric bypass surgery.
obese patients. Ann Surg. 2004;240(3):416-23.
SurgObesRelat Dis. 2010;6(6):608-14.
25.
Hell E, Miller K, Moorehead MK, Norman S. Evaluation
30.
Al Harakeh AB, Larson CJ, Mathiason MA, Kallies
of health status and quality of life after bariatric surgery:
KJ, Kothari SN.BAROS results in 700 patients after
comparison of standard Roux en-Y gastric bypass, vertical
laparoscopic Roux-en-Y gastric bypass with subset
banded gastroplasty and laparoscopic adjustable gastric
analysis of age, gender, and initial body mass index.
banding. Obes Surg. 2000;10(3):214-19.
SurgObesRelat Dis. 2011;7(1):94-8.
28
Dejeu et al
GENERAL REVIEW
TREATMENT OF PRIMARY OSTEOPOROSIS
Cristina Căpățînă, Cătălina Poiană
“CI Parhon” National Institute of Endocrinology, București, România and “Carol Davila” University of Medicine and
Pharmacy, București
Address for correspondence:
Cristina Căpățână
Dept. Endocrinology, “Carol Davila” UMPh, Bucharest, “CI Parhon” National Institute of Endocrinology,
Pituitary and Neuroendocrine Diseases Dept.
Bd. Aviatorilor 34-36, sector 1, Bucharest
E-mail: cristina.capatina@yahoo.com
Received: 24.02.2016
Accepted: 30.06.2016
Med Con June 2016 Vol 11, No 2, 29-35
Abstract
the United States alone [1]. Primary osteoporosis is
thought to be a bone disorder of relatively unknown
Primary osteoporosis is a disorder with a rising
origin that occurs with aging and accelerates at
prevalence, especially among postmenopausal women.
menopause. It is a metabolic bone disease characterized
Its high prevalence, numerous complications and huge
by low bone mass and micro-architectural deterioration
costs imposed on health services worldwide, make
of bone tissue, leading to enhanced bone fragility and
optimal management of osteoporosis a leading priority.
increased fracture risk. In contrast, secondary
At present, the available therapeutic options include
osteoporosis has a direct cause (medications, various
non-pharmacologic measures, calcium and vitamin D
medical conditions). Seventy percent of people with
supplementation as well as a wide range of active
osteoporosis are women. Men start with higher bone
medications: bisphosphonates, denosumab, teriparatide.
density and lose calcium at a slower rate than women,
Other classes of drugs, widely used in the past, are much
therefore their risk is lower. Nevertheless, older men are
less frequently used nowadays (estrogens, calcitonin).
also at risk for osteoporosis.
Te priority of the research in this field led to the
Te main risk factors for osteoporosis are: female
discovery of many active molecules, currently assessed
gender, age over 65, menopause, estrogen deficiency in
in clinical studies.
women, low levels of testosterone in men, low body
In conclusion, the treatment of primary osteoporosis
weight, calcium and vitamin D deficiencies tobacco,
is complex, can involve many active drugs and it is
excessive alcohol use and family history of fractures
recommended to be performed under the guidance of a
associated with osteoporosis. Because osteoporosis can
skilled clinician with good expertise in the field of
occur with few symptoms, bone density testing is
osteoporosis.
recommended for all women age 65 or older, women
Keywords:
osteoporosis,
vitamin
D,
under age
65 with one or more risk factors for
bisphosphonates, denosumab, teriparatide
osteoporosis, all men over age 70 and men ages 50-70
with one or more risk factors for osteoporosis.
Introduction
Treatment of osteoporosis is directed toward
preserving the bone mass, decreasing the risk for fragility
Osteoporosis affects more than 200 million people
fractures and their associated comorbidities and
worldwide, leading to more than 2 million fractures in
ensuring optimal nutrition status [2]. Te final aim of
Treatment of Primary Osteoporosis
29
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
anti-osteoporotic treatment is to increase the bone mass
7-dehydrocholesterol, under the action of solar
and reduce fracture risk.
ultraviolet radiations [4]. An important source of VD is
General measures
found in certain foods (eggs, diary products and fatty
Nutritional intervention is related to calcium,
fish). Both forms need to be activated through 2 steps of
protein and vitamin D (VD) intake. Current guidelines
enzymatic hydroxylation. Te first step takes place in
recommend daily supplementation with a minimum of
the liver, under the action of 25-hydroxylase (leading to
1000mg elemental calcium,
800 international units
the synthesis of 25 hydroxyVD, 25OHD, calcidiol), the
(IU) VD and 1g/kg of proteins [2]. Specific measures to
second one in the kidney, catalyzed by 1α-hidroxilaseleads
decrease the risk of falling include: evaluation and
to the final active product, 1,25 dihydroxyvitamin D
adequate correction of visual problems (ophtalmological
(1,25 OH2D, calcitriol). Te serum concentrations of
evaluation, glasses prescription, if necessary); decreasing
25OHD is positively correlated with the bone mineral
as much as possible the use of certain substances (e.g.
density (BMD) [5]. VD supplementation increases the
anxiolytics, antidepressants, alcohol) associated with
BMD and reduces the loss of bone mass in elderly
possible impairment of balance and/or conscience;
patients (aged over 65 years) [6,7].
removing all obstacles present in the patient’ home or its
Te seric concentration of 25OHD is significantly
surroundings, proper lighting of the access ways used by
negatively correlated with the fracture risk [8]. Daily
the patient in his/her own home and covering slippery
supplementation with a minimum of
800IU VD
surfaces with anti-skid materials [3].
decreases the risk of hip and non-vertebral fracture [9].
Te pharmacologic treatment of osteoporosis affects
Te target concentration of 25OHD that needs to be
the bone metabolism and influences both resorbtion
achieved for a consistent anti-fracture effect is at least
and formation of bone. Te most widely used are
75nmol/l (equivalent to30ng/ml) [10,11]. Te daily D3
raloxifene (a member of the class of selective estrogen
dose needed to reach target is around
20-25μg
receptor modulators, SERM, progressively less used
(equivalent to 800-1000UI) [12].
with the advent of new therapies), bisphosphonates
Te administration of VD also exerts beneficial
(alendronate, ibandronate, risedronate), parathormone
effects indirectly, by improving the muscle function and
derivatives, strontium ranelate and denosumab.
performance. Te serum
25OHD concentration is
Hormonal replacement treatment is used nowadays
directly correlated with the muscle strength (corrected
only in selected cases.
for age and gender)
[14], as well as with various
Calcium and vitamin D
musculoskeletal perfomance markers (such as walking
Native vitamin D (VD) exists in 2 forms: vitamin
speed, time obtained in the sit-to-stand test aso) [13].
D2 (synthesised by plants) and vitamin D3, sinthesised
VD supplementation also has a significant effect to
in the skin, by transforming its precursor,
increase the muscle strength in individuals with severe
Table I. Pharmacologic options in the treatment of osteoporosis
Indication
Decreasing fracture risk
Comments
Prevention Treatment
Vertebral
Non-vertebral Hip
Antiresorbtive agents
Alendronate
yes
yes
yes
yes
yes
Weekly administration
Monthly oral administration
Ibandronate
yes
yes
yes
-
-
or iv each 3 months
Weekly or monthly
Risedronate
yes
yes
yes
yes
yes
administration
Zoledronate
-
yes
yes
yes
yes
Yearly iv administration
Raloxifene
yes
yes
yes
-
-
Breast cancer prevention
Calcitonin
-
yes
yes
-
-
Twice yearly subcutaneous
Denosumab
-
yes
yes
yes
yes
administration
Estrogen
yes
-
yes
yes
yes
Adverse reactions
Anabolic agents
Daily subcutaneous
Teriparatide
-
yes
yes
yes
-
administration
Other
Strontium ranelate
-
yes
yes
yes
30
Căpățînă et al
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
GENERAL REVIEW
VD deficiency (25OHD≤25nmol/L), but not in those
A rare adverse reaction is the osteonecrosis of the
with lesser degrees of deficit [14].
mandible. Tis has been reported especilly in oncological
VD supplementation is associated with a significant
patients, with dental problems, suboptimal oral hygiene
decrease of the incidence of falling episodes but only at
or needing invasive dental procedures. In osteoprotic
higher doses (800-1000UI), if adequate post-therapeutic
patients, the incidence of this adverse reaction is almost
concentrations are reahed and only in patients with VD
insignificant - 1/100,000 [2].
deficiency at baseline [15].
Selective Estrogen-Receptor Modulators, SERM
Te role of the standard association of calcium to VD
Drugs in the SERM class have binding affinity for
treatment is reinforced by the studies reporting that this
the estrogen recepotor and act as agonists or antagonists
association leads to a supplementary reduction in fracture
of this receptor in various tissues, leading to different
risk. Te relative risk for hip fracture was 1.1 in studies
cascades of intracellular events in each target tissue.
assessing the exclusive administration of VD (investigated
Raloxifene is the only SERM available in clinical
in a large meta-analysis) while the combined relative risk
practice for the prevention and treatment of
was only 0.82 in the studies involving combined calcium
postmenopausal osteoporosis. Te MORE study
and VD administration [16].
(Multiple Outcomes of Raloxifene Evaluation)
[19]
Calcitriol is not routinely used in the treatment of
proved a 30-50% risk reduction for vertebral fractures
osteoporosis (mostly because of its higher risk of adverse
in women with or without prevalent vertebral fractures
reactions, especially hypercalcemia) but it is approved
but no significant effect on non-vertebral fractures.
for the treatment of renal bone disease [17].
However, a post hoc analysis of the patients included in
Bisphosphonates
the MORE study revealed also the reduction of non-
Bisphosphonates are the most widely used class of
vertebral fractures risk in patients with very high risk at
drugs in the treatment of osteoporosis. Tey exert a
baseline (i.e. those with prevalent vertebral fractures at
potent anti-resorbtive effect by decreasing osteoclast
baseline) [20]. Te only severe adverse effect was an
activation and osteoclast progenitor development and
increase in the incidence of deep venous thrombosis
recruitment and also by promoting osteoclast apoptosis
during treatment.
[18].
An important effect is the very significant decrease
When administered orally, they have a relatively low
(around 60%) of the risk of invasive breast cancer [21],
bioavailability (below 1%) and there is also a risk for
effect comparable to that of tamoxifene in the population
esophageal mucosal irritation. Terefore, they need to
at high risk for malignancy
[22]. Regarding the
be administered on an empty stomach, with a large glass
presumed risk of ischemic cardiac disease, according to
of water and after administration it is recommended to
the RUTH study
(an international, multicenter,
avoid the lying position for at least 30 minutes (in order
randomized, double-blind, placebo-controlled trial)
to decrease the risk of adverse esophageal reactions). At
[23] raloxifene is not a significant risk factor. However,
least 50% of the bisphosphonates quantity administered
the benefits of raloxifene in reducing the risk of invasive
is deposited in the bone and have a very long half-life.
breast cancer and vertebral fracture need to be carefully
Bisphosphonates administration is contraindicated
balanced opposed to the risk of venous thromboembolism
in patients with hypocalcemia and needs to be carefully
and fatal stroke [23].
adjusted in those with significant renal impairment
Denosumab
(glomerular filtration rate below
30-35ml/min) or
Denosumab is a specific monoclonal antibody
severe problems of the upper digestive tract. Te
directed against the receptor activator of the nuclear
intravenous administration is relatively frequently
factor kappa-B ligand (RANKL) with a potent effect of
associated with acute phase reactions, reversible with
inhibiting bone resorbtion
(exerted through the
symptomatic treatment.
inhibition of formation, action and lifespan of
Table II. Relative antifracture efficacy of bisfosphonates
Vertebral fractures Hip fractures Non-vertebral fractures Reference
Comments
FIT study
In women with prevalent
Alendronate
↓50%
[34;35]
vertebral fractures
In women with prevalent
Risedronate
↓50%
↓33%
vertebral fractures
Ibandronate
↓
-
↓
[36]
Zoledronate iv
↓70%
↓40%
[37]
31
Treatment of Primary Osteoporosis
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
osteoclasts). It is administered as subcutaneous injections
vertebral fractures risk [30,31]. In a placebo-controlled
every 6 months. It is highly efficient both in primary
study of 5 years duration, the administration of 200IU
osteoporosis (reducing the risk of vertebral, hip and
salmon calcitonin as nasal spray to a large cohort of
non-vertebral fractures) and in secondary osteoporosis
postmenopausal osteoporotic women, reduced the risk
(occuring in patients with malignant or rheumatic
of new vertebral fractures by 33% and increased by 1%
disorders). Te initial concerns related to the long-term
the lumbar BMD [31].
administration of a biological product were not
Estrogen replacement tretament
sustained by the published studies which reported no
Estrogen administration in postmenopausal
serious adverse effects to date [24].
osteoporosis reduces the accelerated bone turnobver and
Teriparatide, peptidesrelated to parathormone (PTH)
decreases the risk of vertebral and non-vertebral fractures
Although chronic excess of PTH leads to cortical
by around 30% [32]; however, the effect does not persist
bone resorption, the intermittent administration
(in
after the therapy is interrupted
[33]. Te Women’s
daily subcutaneous injection) induces bone mass
Health Initiative (WHI) study suggested that the risk/
increase, in the cortical as well as in the trabecular bone
benefit ratio is unfabvourable in long-term
[25].
administration of replacement therapy. Te combined
In the treatment of osteoporosis both intact PTH
use of conjugated estrogens and medroxyprogesterone
(whole peptide molecule consisting of 84 amino acids;
acetate has been associated with an increase of around
1-84) and especially the N-terminal fragment of the
30% in the risk of ischemic heart disease and breast
PTH (consisting of
34 amino acids:
1-34), called
cancer as well as a 40% increase in stroke prevalence
teriparatide are used. Te equivalent dose of teriparatide
[34,35]. In women receiving only conjugated estrogens
is around 40% of that of the intact PTH: 20μg daily in
(hysterectomised women) no increased risk of breast
subcutaneous injections. At this dose, teriparatide
cancer or ischemic heart disease was noted, which raised
significantly reduces the risk of vertebral and non-
the idea of a possible deleterious effect of the progestative
vertebral fracture (as opposed to the intact molecule,
component. Tere is an ongoing debate regarding this
which only decreases the risk of vertebral fracture) [2].
subject; in the meantime hormonal replacement therapy
Te maximum duration for treatment with PTH
is definitely not any more a first-line treatment in
derivatives is
24 months. Among the most frequent
postmenopausal osteoporosis. A related drug, tibolone,
cited adverse reactions are digestive problems, myalgias,
has the advantage to decrease both fractures and breast
headache, diziness and transient hypercalcemia. PTH-
cancer rates but increases the risk of stroke [26].
related peptides are contraindicated in patients with
Combined treatment
high bone turnover (e.g. primary hyperparathyroidism,
Te anti-resorbtive effect can be augmented by the
Paget disease, primary or secondary bone neoplasia) and
concomitant administration of two anti-osteoporotic
in severe renal failure [2]. Tis class of drugs is most
medications from two different classes of drugs.
frequently recommended in patients with severe
However, the net result is generally not an additive
osteoporosis unresponsive or intolerant to anti-
decrease of the fracture risk. In the study of Ettinger et
resorbtive treatment [26].
al [36] in patients treated long-term with antiresorbtives
Strontium ranelate
(mainly bisphosphonates) who later received anabolic
Strontium ranelate is an anti-osteoporotic agent
medications (e.g. teriparatide) the therapeutic efficcacy
combining the anti-resorbtive with the bone formation
was not different from that observed in patients naive to
mechanism. In administration of the daily recommended
antiosteoporotic treatment despite the fact that the
dose of 2g orally it reduces both the risk of vertebral and
BMD increase occurs later in pretreated cases [36].
non-vertebral fractures
[27]. It is contraindicated in
Tere are no proofs of a potential synergic effect of
patients with severe renal failure. Strontium ranelate has
the concomitant administration of teriparatide and
been associated with an increased incidence of venous
bisphosphonates
- some authors even consider that
thromboembolism in phase III studies, leading to
such use might reduce the anabolic effects of the PTH
relative contraindications in patients with personal
[37]. Terefore it is not recommended to use the two
history of deep venous thrombosis.
classes of drugs (or at least alendronate) concomitantly
Calcitonin
but rather sequentially [38]. Other studies suggest that
Calcitonin is a polypeptidic hormone with anti-
different bisphosphonates (e.g. egrisedronate) or SERMs
resorbtive effects
[28]. It can be administered in
(raloxifene) do not decrease the anabolic effect of PTH
injections or as nasal spray, and induces a slight increase
[39]. Sequential administration can be beneficial in
of the BMD [29] as well as a limited reduction of
both directions: an anti-resorbtive administered after
32
Căpățînă et al
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
GENERAL REVIEW
teriparatide treatment will consolidate the beneficial
double-blind trial. J Clin Endocrinol Metab.
bone effects of the latter [40].
1995;80(4):1052-8.
Te lumbar and hip BMD rise during treatement
8.
Bischoff-Ferrari HA. Vitamin D and fracture
with alendronate is directly correlated with the decrease
prevention. Rheum Dis Clin North Am.
of the fracture risk [41], but for risedronate or raloxifene
2012;38(1):107-13.
the correlation is not as good [42,43].
9.
Bischoff-Ferrari HA, Willett WC, Orav EJ. A pooled
Also for strontium ranelate [44] and teriparatide
analysis of vitamin D dose requirements for fracture
[45] the anti-fracture efficacy is significantly influenced
prevention. N Engl J Med. 2012;367(1):40-9.
by the BMD change at the hip level.
10.
Dawson-Hughes B, Mithal A, Bonjour JP. IOF
Compliance to treatment
position statement: vitamin D recommendations for
Compliance to treatment is of paramount
older adults. Osteoporos Int. 2010;21(7):1151-4.
importance taking into account that osteoporosis is a
11.
Holick MF, Binkley NC, Bischoff-Ferrari HA.
chronic, mostly asymptomatic disorder which needs
Evaluation, treatment, and prevention of vitamin D
long-term treatment. Low compliance to anti-
deficiency: an Endocrine Society clinical practice
osteoporotic treatment is associated with persistent high
guideline. J Clin Endocrinol Metab. 2011;96(7):1911-
turnover, high fracture risk and decrease of the BMD
30.
[46]. Terefore the clinician must take measure for
12.
Dawson-Hughes B, Heaney RP, Holick MF, Lips P,
ensure a long-term treatment.
Meunier PJ, Vieth R. Estimates of optimal vitamin D
Conflict of interests: nothing to declare
status. Osteoporos Int. 2005;16(7):713-6.
13.
Bischoff-Ferrari HA, Dietrich T, Orav EJ. Higher
25-hydroxyvitamin D concentrations are associated with
References
better lower-extremity function in both active and
inactive persons aged > or =60 y. Am J Clin Nutr.
1.
Sheyn D, Shapiro G, Tawackoli W, Jun DS, Koh Y,
2004;80(3):752-8.
Kang KB, et al. PTH Induces Systemically Administered
14.
Stockton KA, Mengersen K, Paratz JD, Kandiah D,
Mesenchymal Stem Cells to Migrate to and Regenerate
Bennell KL. Effect of vitamin D supplementation on
Spine Injuries. MolTer. 2016;24(2):318-30.
muscle strength: a systematic review and meta-analysis.
2.
Kanis JA, McCloskey EV, Johansson H, Cooper C,
Osteoporos Int. 2011;22(3):859-71.
Rizzoli R, Reginster JY. European guidance for the
15.
Bischoff-Ferrari HA, Dawson-Hughes B, Staehelin
diagnosis and management of osteoporosis in
HB. Fall prevention with supplemental and active forms
postmenopausal
women.
Osteoporos
Int.
of vitamin D: a meta-analysis of randomised controlled
2013;24(1):23-57.
trials. BMJ. 2009;339:b3692.
3.
Kannus P, Sievanen H, Palvanen M, Jarvinen T,
16.
Boonen S, Lips P, Bouillon R, Bischoff-Ferrari HA,
Parkkari J. Prevention of falls and consequent injuries in
Vanderschueren D, Haentjens P. Need for additional
elderly people. Lancet. 2005;366(9500):1885-93.
calcium to reduce the risk of hip fracture with vitamin d
4.
Battault S, Whiting SJ, Peltier SL, Sadrin S, Gerber
supplementation: evidence from a comparative
G, Maixent JM. Vitamin D metabolism, functions and
metaanalysis of randomized controlled trials. J Clin
needs: from science to health claims. Eur J Nutr.
Endocrinol Metab. 2007;92(4):1415-23.
2013;52(2):429-41.
17.
Ringe JD, Schacht E. Prevention and therapy of
5.
Bischoff-Ferrari HA, Dietrich T, Orav EJ, Dawson-
osteoporosis: the roles of plain vitamin D and alfacalcidol.
Hughes B. Positive association between
25-hydroxy
Rheumatol Int. 2004;24(4):189-97.
vitamin D levels and bone mineral density: a population-
18.
Hughes DE, Wright KR, Uy HL, et al. Bisphosphonates
based study of younger and older adults. Am J Med.
promote apoptosis in murine osteoclasts in vitro and in
2004;116(9):634-9.
vivo. J Bone Miner Res. 1995;10:1478
6.
Dawson-Hughes B, Dallal GE, Krall EA, Harris S,
19.
Ettinger B, Black DM, Mitlak BH. Reduction of
Sokoll LJ, Falconer G. Effect of vitamin D
vertebral fracture risk in postmenopausal women with
supplementation on wintertime and overall bone loss in
osteoporosis treated with raloxifene: results from a 3-year
healthy postmenopausal women. Ann Intern Med.
randomized clinical trial. Multiple Outcomes of
1991;115(7):505-12.
Raloxifene Evaluation (MORE) Investigators. JAMA.
7.
Ooms ME, Roos JC, Bezemer PD, van der Vijgh WJ,
1999;282(7):637-45.
Bouter LM, Lips P. Prevention of bone loss by vitamin
20.
Delmas PD, Genant HK, Crans GG. Severity of
D supplementation in elderly women: a randomized
prevalent vertebral fractures and the risk of subsequent
33
Treatment of Primary Osteoporosis
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
vertebral and nonvertebral fractures: results from the
33.
Bagger YZ, Tanko LB, Alexandersen P. Two to three
MORE trial. Bone. 2003;33(4):522-32.
years of hormone replacement treatment in healthy
21.
Cummings SR, Eckert S, Krueger KA. Te effect of
women have long-term preventive effects on bone mass
raloxifene on risk of breast cancer in postmenopausal
and osteoporotic fractures: the PERF study. Bone.
women: results from the MORE randomized trial.
2004;34(4):728-35.
Multiple Outcomes of Raloxifene Evaluation. JAMA.
34.
Chlebowski RT, Hendrix SL, Langer RD. Influence of
1999;281(23):2189-97.
estrogen plus progestin on breast cancer and
22.
Vogel VG, Costantino JP, Wickerham DL. Effects of
mammography in healthy postmenopausal women: the
tamoxifen vs raloxifene on the risk of developing invasive
Women’s Health Initiative Randomized Trial. JAMA.
breast cancer and other disease outcomes: the NSABP
2003;289(24):3243-53.
Study of Tamoxifen and Raloxifene (STAR) P-2 trial.
35.
Wassertheil-Smoller S, Hendrix SL, Limacher M.
JAMA. 2006;295(23):2727-41.
Effect of estrogen plus progestin on stroke in
23.
Barrett-Connor E, Mosca L, Collins P. Effects of
postmenopausal women: the Women’s Health Initiative:
raloxifene on cardiovascular events and breast cancer in
a randomized trial. JAMA. 2003;289(20):2673-84.
postmenopausal women. N Engl J Med.
36.
Ettinger B, San MJ, Crans G, Pavo I. Differential
2006;355(2):125-37.
effects of teriparatide on BMD after treatment with
24.
Bogado CE, Boailchuk JA, Zanchetta MB, Massari
raloxifene or alendronate. J Bone Miner Res.
FE, Zanchetta JR. Denosumab: an update. Drugs
2004;19(5):745-51.
Today (Barc). 2011;47(8):605-13.
37.
Black DM, Greenspan SL, Ensrud KE. Te effects of
25.
Hock JM, Gera I. Effects of continuous and intermittent
parathyroid hormone and alendronate alone or in
administration and inhibition of resorption on the
combination in postmenopausal osteoporosis. N Engl J
anabolic response of bone to parathyroid hormone. J
Med. 2003;349(13):1207-15.
Bone Miner Res. 1992;7(1):65-72.
38.
Finkelstein JS, Hayes A, Hunzelman JL, Wyland JJ,
26.
Eastell R. Osteoporosis. Oxford Textbook of
Lee H, Neer RM. Te effects of parathyroid hormone,
Endocrinology and Diabetes. New York: Oxford
alendronate, or both in men with osteoporosis. N Engl J
University Press Inc, 2011:701-11.
Med. 2003;349(13):1216-26.
27.
Reginster JY, Sarlet N, Lejeune E, Leonori L.
39.
Deal C, Omizo M, Schwartz EN. Combination
Strontium ranelate: a new treatment for postmenopausal
teriparatide and raloxifene therapy for postmenopausal
osteoporosis with a dual mode of action. Curr
osteoporosis: results from a
6-month double-blind
Osteoporos Rep. 2005;3(1):30-4.
placebo-controlled trial. J Bone Miner Res.
28.
Reginster JY. Effect of calcitonin on bone mass and
2005;20(11):1905-11.
fracture rates. Am J Med. 1991;91(5B):19S-22S.
40.
Black DM, Bilezikian JP, Ensrud KE. One year of
29.
Cranney A, Wells G, Willan A. Meta-analyses of
alendronate after one year of parathyroid hormone (1-
therapies for postmenopausal osteoporosis. II. Meta-
84) for osteoporosis. N Engl J Med. 2005;353(6):555-
analysis of alendronate for the treatment of
65.
postmenopausal women. Endocr Rev. 2002;23(4):508-
41.
Cummings SR, Karpf DB, Harris F. Improvement in
16.
spine bone density and reduction in risk of vertebral
30.
Cranney A, Guyatt G, Griffith L, Wells G, Tugwell P,
fractures during treatment with antiresorptive drugs.
Rosen C. Meta-analyses of therapies for postmenopausal
Am J Med. 2002;112(4):281-9.
osteoporosis. IX: Summary of meta-analyses of therapies
42.
Watts NB, Geusens P, Barton IP, Felsenberg D.
for
postmenopausal osteoporosis. Endocr Rev.
Relationship between changes in BMD and nonvertebral
2002;23(4):570-8.
fracture incidence associated with risedronate: reduction
31.
Chesnut CH, III, Silverman S, Andriano K. A
in risk of nonvertebral fracture is not related to change in
randomized trial of nasal spray salmon calcitonin in
BMD. J Bone Miner Res. 2005;20(12):2097-104.
postmenopausal women with established osteoporosis: the
43.
Sarkar S, Mitlak BH, Wong M, Stock JL, Black DM,
prevent recurrence of osteoporotic fractures study.
Harper KD. Relationships between bone mineral density
PROOF Study Group. Am J Med. 2000;109(4):267-
and incident vertebral fracture risk with raloxifene
76.
therapy. J Bone Miner Res. 2002;17(1):1-10.
32.
Cauley JA, Robbins J, Chen Z. Effects of estrogen plus
44.
Bruyere O, Roux C, Detilleux J. Relationship between
progestin on risk of fracture and bone mineral density:
bone mineral density changes and fracture risk reduction
the Women’s Health Initiative randomized trial. JAMA.
in patients treated with strontium ranelate. J Clin
2003;290(13):1729-38.
Endocrinol Metab. 2007;92(8):3076-81.
34
Căpățînă et al
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
GENERAL REVIEW
45. Chen P, Miller PD, Delmas PD, Misurski DA, Krege
46. Reginster JY, Rabenda V, Neuprez A. Adherence,
JH. Change in lumbar spine BMD and vertebral
patient
preference
and dosing
frequency:
fracture
risk
reduction in teriparatide-treated
understanding the relationship. Bone.
2006;38(4
postmenopausal women with osteoporosis. J Bone Miner
Suppl 1):S2-S6.
Res. 2006;21(11):1785-90.
35
Treatment of Primary Osteoporosis
Transmittal Letter
In consideration of the Medical Connections/Conexiuni Medicale taking action in reviewing and
editing the above-named Article, effective upon acceptance of the Article by the Medical Connections/
Conexiuni Medicale (hereinafter reffered to as Med Con), the Autor(s) hereby assign(s) to the Med Con,
its legal representatives, successors and assigns, all publishing rights and each and every other right to the
Article throughout the world, in any language and in any medium, whether as an audiovizual work,
collective work, compilation, derivative work, joint work, literary work, phonorecord, pictorial, graphic or
sulptural work, sound recording, work of visual art, computer program, or any other medium now existing
or which hereafter may come into existence, including the copyright and the right to register the copyright
as well as the right to secure any renewals, reissues, and extensions of any such copyrights in Romania or
in any foreign country. Author(s) may request permission to reuse the manuscript or portions thereof.
Such requests must be in writing and permission by the Med Con shall not be unreasonably withheld. Te
Author(s) appoint(s) the Med Con as the Author’s(s’) attorney-in-fact to execute any documents the Med
Con deems necessary to record any of these grants with the Romanian copyright office or elsewhere. Te
Autor(s) also warrant(s) to the Med Con that the Article is original work of the Author(s) except for
material in the public domain and such excerpts from other works as may be included with the prior
written permission of the copyright owners; that the Article has not been previously published, submitted,
or accepted for publication elsewhere; that the Author(s) have no relationship, financial or otherwise, with
any manufacturers or distributors of products evaluated in this paper, or alternatively any such relationship
has been disclosed in a footnote to the paper, or the requirement is irrelevant to this paper.
Manuscript Title: _ __________________________________________________________
Name:
Signature/Date:
_ ___________________________________
_ ___________________________________
_ ___________________________________
_ ___________________________________
_ ___________________________________
_ ___________________________________
_ ___________________________________
_ ___________________________________
_ ___________________________________
_ ___________________________________
_ ___________________________________
_ ___________________________________
_ ___________________________________
_ ___________________________________
Please fax this signed form to the Med Con Editorial Office.
Fax: +40-261-710456
GENERAL REVIEW
THE OVARIAN CANCER UNDER THE HISTORIES MAGNIFYING GLASS,
THERAPY POSSIBILITIES OVER THE TIME. AN OVERVIEW
Ionuț Marcel Cobec1,2
1Clinic of Obstetrics and Gynecology, Diakonie Klinikum, Schwäbisch Hall, Akademisches Lehrkrankenhaus der
Universität Heidelberg, Germany and 2University of Medicine and Pharmacy “Victor Babeş”, Timişoara, Romania
Address for correspondence:
Ionut Marcel Cobec, MD
Tel: +40 729099289, +4915163654211
E-mail: cobec_i@yahoo.com
Received: 02.05.2016
Accepted: 30.06.2016
Med Con June 2016 Vol 11, No 2, 37-40
Abstract
among gynecological cancers and the seventh cause of
cancer in women [4-6], it has the highest mortality
Te ovarian cancer is a pathology which over the
(yearly the death number represents more than half of
time issued not only controversies, but also questions,
the number of the new diagnosed cases [3]) among
many of those remaining without an answer until
gynecological carcinomas, it is also called „silent killer”
nowadays. Over the time were done continue efforts
[7-13].
which represents a cornerstone of the actual therapeutic
Following a brief history of the ovarian cancer, we
standard used in the ovarian tumor therapy.
can observe the continual attempts to identify the causes
In this paper are followed gradually the steps done by our
of this pathology, the continue wish to classify, also the
predecessors in their pioneer work represented not only by
diverse therapy possibilities, invasive or non-invasive,
the surgical, but also by the drug therapy, the latest researches
used between the time, each time existing the hope of a
in this field and also by the written specialty literature, allover
successful therapy in the fight with this malady of the
representing nowadays a rich scientific dowry.
XXI century, the cancer.
Starting with the first surgical attempts, followed by
In the middle of the XIXth century, as a result of
diverse drug or radiological therapy options, which had
the increase of the surgical acts began to be observed
more or less success and reaching the actual
with increased attention the ovarian tumor and was
therapeutically standard, this paper sums up a history
persuaded the so called at that time ovariotomy,
page of the ovarian cancer.
nowadays the oophrectomy. In 1809 was done the first
Keywords: ovarian cancer, therapy, history, options.
ovariotomy by Ephraim McDowell, but also by the
surgery pioneers Spencer Wells and Lawson Tait [14].
Te cancer represents a pathology which makes real
In 1870 Heinrich Waldeyer did a paper about the
problems in the public health systems, in Romania its’
epithelial ovarian tumor, for the first time being
incidence is among the lowest in central and south-
suggested a histogenesis which is generally accepted
eastern Europe, but with a high rate of mortality [1]. In
until nowadays. Two years later E. Randolph did the
cancers’ pathology are involved not only functions, but
first book which describes in detail the ovarian
also immune response, and agiogenesis, hypoxia and
pathology, being called Ovarian tumors: Pathology,
inflammation can be identified to the cellular level [2].
Diagnostic and their Treatment, especially through
Ovarian cancer has an incidence of
42 out of
Ovariotomy. One of the first important contributions
100.000 cases [3], represents the second cause of death
belongs to Hermann Johannes Pfannenstiel through the
The Ovarian Cancer Under the Histories Magnifying Glass, Therapy Possibilities Over the Time
37
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
book published in
1898, where he introduces the
synergic role and same effects. Bevacizumab used in
concept of borderline neoplasm and is detailed the term
combination with cisplatin increased the survival
malign. Krukenberg described with the age of 25 in a
[19,20]. Based on the fact that ovarian tumors have a
work consisting of 35 pages the Krukenberg lesion,
rich vascularization dependent on angiogenesis mediated
described as a sarcoma, being recognized as a metastasis
by VEGF, were elaborated therapy attempts not only in
by Schlagenhaufer in 1902. In 1907 Brenner describes
the clinical, but also in the preclinical field. One of the
in a thesis the tumor, which has his name; he worked in
most used therapies is the one with bevacizumab in
a relative obscurity in South Africa, there being
order to neutralize the circulated VEGF and to suppress
discovered by Harold Speert, the one who published in
the angiogenesis. In a phase III clinical study of ovarian
1958 the book Obstetric and Gynecologic Milestones. In
cancer, it is shown that bevacizumab prolongs the
1925 John Albertson Sampson, overnamed as the father
survival without tumor progress when it is administrated
of endometriosis, speaks about the association of ovarian
in combination with chemotherapy, although this
endometriosis with endometrial carcinoma [14].
administration is limited because the anti-VEGF
In the period
1956-1957 the World Health
therapy is associated with hard side effects [19,20,21].
Organization
(WHO) tried to realize various
Te prolonged use of anti-VEGF therapy leads to the
classifications in what concerns the ovarian tumor.
generation of other proangiogenic factors, so that the
Te first classification of the surface epithelial
use and production of an independent therapy of the
stromal tumors was done in 1961 by the International
tumor VEGF is critical.
Federation of Obstetrics and Gynecology (FIGO).
Because of the bleak prognosis of the ovarian cancer,
In 1963, and afterwards in 1965, were organized
Sato and Itamochi [22] reused in a study the idea of
meetings between the FIGO and WHO representatives,
radiotherapy, which was used in the 1950s, but they
having as purpose commune collaboration in order to
renounced afterwards due to side effects. In a phase I/II
avoid the parallelisms. Te final form of the ovarian
pilot study of ovarian cancer, FIGO III (R1 or R2<1cm)
tumor classification was published in 1973 by WHO
after surgical resection and adjuvant chemotherapy
[14]. Te ovarian cancers’ stadialization was accepted by
based on platin were included 6 cycles of carboplatin or
FIGO in 1988, having a similar form as the actual one.
cisplatin and paclitaxel or docetaxel in a
3 weeks
Over the time, many studies showed that the FIGO
administration interval [22]. Afterwards was decided
stadialization needs to be reviewed and modified, in
the radiotherapy with modulating intensity because of
order to be reached a more efficient disease prognosis
the advanced technology having the possibility to reduce
[15]. In 2014 was approved the new FIGO stadialization
the side effects through the protection of the organs at
of the ovarian cancer, which takes into consideration all
risk, such as kidneys, liver, bone marrow [23].
the proposed recommendations in order to be efficient
Over the time, various research groups tried to settle
when it is used in the treatment decision of this disease.
an efficient therapy of the ovarian cancer. In those
In 1983 was identified a polypeptide in a Guinea
attempts were various periods in which were tried
pig tumor cell line medium [16] with a role in the
diverse antitumor therapy combinations, having more
permeability of the tumor vascularization, called at that
or less success, but all having as purpose to improve the
time vascular permeability factor (VPF). Afterwards, in
ovarian cancer prognosis and playing the role of a
1989 was isolated from bovine pituitary follicular cells
cornerstone to the actual surgical and drug therapy
and renamed Vascular Endothelial Growth Factor
standards.
(VEGF) [17,18].
In
1976 was the first success of the efficiency
VEGF is involved in the process of tumor growth,
through the use of cisplatin, produced by the
invasion and dissemination to the level of lymph nodes,
combination of the platin based chemotherapy. Te
liver, lungs. Tis is why are used various drug agents
years
1980-1990 are another moment of therapy
having as target the role of VEGF in ovarian cancer, in
success, though the discover of paclitaxel, in the hard
peritoneal carcinomatosis and/or presence of ascites.
road to identify an efficient therapy. Ulterior studies
Trough the agents used as having a role in the
proved the superior efficiency of the cisplatin use in
neutralization of VEGF is bevacizumab, which is a
combination with paclitaxel, in contradistinction to the
human recombined monoclonal antibody, which acts
combination cisplatin-cyclophosphamide, in this way
through preventing the binding of VEGFRs with all
becoming the first line therapy option. Ulterior was
VEGF izoforms, in this way preventing the tumor
tried to be identified therapy combinations in which to
growth and the production of ascites. Paclitaxel can be
be reduced the chemotherapy side effects. It was
used in combination with bevacizumab, having a
observed the carboplatin, an analog of cisplatin, which
38
Cobec et al
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
GENERAL REVIEW
shows fewer side effects than cisplatin. Over the time,
8.
Kim A, Ueda Y Naka T, Enomoto T. Terapeutic
from the necessity of an efficient therapy with reduced
strategies in epithelial ovarian cancer. Journal of
side effects, were tried diverse therapy combinations;
Experimental & Clinical Cancer Research.
among those was the try to substitute the paclitaxel with
2012;31:14.
docetaxel. Until this moment this substitution can be
9.
Lalwani N, Prasad SR, Vikram R, et al. Histologic,
done just in the case of high neurotoxicity, the standard
Molecular and Cytogenetic Features of Ovarian Cancers:
therapy remaining carboplatin-paclitaxel [24].
Implications
for
Diagnosis
and Treatment.
In present a new medicine is used as maintenance
RadioGraphics. 2011;31:625-46.
therapy, the oral therapy with olaparib, poli-(ADP-
10.
Cho KR, Shih IM. Ovarian Cancer. Annu Rev Pathol.
ribose) polimerase
(PARP) inhibitor. Tis is
2009;4:287-313.
administrated to the patients with platin sensitive
11.
Barua A, Bitterman P, Abramowicz JS, et al.
recurrent ovarian cancer in whom was proved the
Histopathology of ovarian tumors in laying hens, a
existence of a BRCA mutation and had two or more
preclinical model of human ovarian cancer. Int J
platin based chemotherapies and showed a partial or
Gynecol Cancer. 2009;19(4):531-9.
complete response to the most recent used platin based
12.
Shih I.M., Davidson B. Pathogenesis of ovarian cancer:
chemotherapy [25,26].
clues from selected overexpressed genes. Future Oncol.
Te clinical studies which take place in the present
2009;5(10):1641-64.
are tested diverse monotherapy or therapy combinations
13.
Karst AM, Drapkin R. Ovarian Cancer Pathogenesis:
from the necessity to discover an efficient therapy in
A Model in Evolution. Hindawi Publishing
order to improve the life quality of the patients under
Corporation Journal of Oncology. 2010;1-13.
therapy.
14.
Zoung RH. A brief history of the pathology of the
gonads. Modern Pathology. 2005;18,S3-S17.
15.
Suh DH, Kim TH, Kim JW, et al. Improvements to the
Referencies
FIGO staging for the ovarian cancer: reconsideration of
lymphatic spread and intraoperative tumor rupture. J
1.
Vrdoljak E, Wojtukiewicz MZ, Pienkowski T, Bodoky
Gynecol Oncol. 2013;24(4):352-8.
G, Berzinec P, Finek J, Todorović V, Borojević N,
16.
Senger DR, Galli SJ, Dvorak AM, et al. Tumor cells
Croitoru A. South Eastern European Research Oncology
secrete a vascular permeability factor that promotes
Group. Cancer epidemiology in Central, South and
accumulation
of
ascites
fluid.
Science.
Eastern European countries. Croat Med J.
1983;219(4587),983-5.
2011;52(4):478-87.
17.
Ferrara N, Henzel WJ. Pituitary follicular cells secrete
2.
Markert EK, Levine AJ, Vazquez A. Proliferation and
a novel heparin-binding growth factor specific for
tissue remodeling in cancer: the hallmarks revisited. Cell
vascular endothelial cells. Biochemical and Biophysical
Death Dis. 2012;3:e397.
Research Communications. 1989;161(2):851-8.
3.
McLemore MR, Miaskowski C, Aouizerat BE, et al.
18.
Connolly DT, Olander JV, Heuvelman D, et al.
Epidemiologic and Genetic Factors Associated with
Human vascular permeability factor. Isolation from
Ovarian Cancer. Cancer Nurs. 2009;32(4):281-90.
U937 cells. Journal of Biological Chemistry.
4.
Yoneda A, Lendorf ME, Couchman JR, et al. Breast
1989;26(33):20017-24.
and Ovarian Cancers: A Survey and Possible Roles for
19.
Masoumi Moghaddam S, Amini A, Morris DL,
the Cell Surface Heparan Sulfate Proteoglycans. Journal
Pourgholami MH. Significance of vascular endothelial
of Histochemistry & Cytochemistry. 2012;60(I):9-
growth factor in growth and peritoneal dissemination of
21.
ovarian cancer. Cancer Metastasis Rev. 2012;31(1-
5.
Moghaddam SM, Amini A, Morris DL, et al.
2):143-62.
Significance of vascular endothelial growth factor in
20.
Leamon CP, Lovejoy CD, Nguyen B. Patient selection
growth and peritoneal dissemination of ovarian cancer.
and targeted treatment in the management of platinum-
Cancer metastasis Rev. 2012;31:143-62.
resistant ovarian cancer. Pharmgenomics Pers Med.
6.
Saad AF, Hu W, Sood AK. Microenvironment and
2013;6:113-25.
Pathogenesis of Epitelial Ovarian Cancer. Horm
21.
Cho R K. Ovarian cancer update: Lessons from
Cancer. 2010;1(6): 277-90.
Morphology, Molecules and Mice. Arch Pathol Lab
7.
Rosen DG, Yang G, Liu G, Mercado-Uribe I, et al.
Med. 2009;133(11):1775-81.
Ovarian cancer: pathology, biology, and disease models.
22.
Sato S, Itamochi H. Neoadjuvant chemotherapy in
Front Biosci. 2010;14:2089-102.
advanced ovarian cancer: latest results and place in
39
The Ovarian Cancer Under the Histories Magnifying Glass, Therapy Possibilities Over the Time
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
therapy. Terapeutic Advances in Medical Oncology.
25. Ledermann J, Harter P, Gourley C, et al. Olaparib
2014;6(6),293-304.
maintenance therapy in patientins with platinum-sensitive
23. Rochet N, Jensen AD, Sterzing F, et al. Adjuvant
relapsed serous ovarian cancer: a preplanned retrospective
whole abdominal intensity modulated radiotherapy
analysis of outcomes by BRCA status in a randomized phase
(IMRT) for risk stage FIGO III patients with ovarian
2 trial. Lancet Oncol. 2014;15(8):852-61.
cancer (OVAR-IMDT-01)-Pilot trial of phase I/II study:
26. Oza AM, Cibula D, Benzaquen AO, et al. Olaparib
study protocol. BMC Cancer. 2007;7:227.
combined with chemotherapy for recurrent platinum-
24. Kim A, Ueda Y, Naka T, Enomoto T. Terapeutic
sensitive ovarian cancer: a randomised phase 2 trial.
strategies in epithelial ovarian cancer. J Exp Clin
Lancet Oncol. 2015;16(1):87-97.
Cancer Res. 2012;31:14.
40
Cobec et al
GENERAL REVIEW
CEREBRAL INTRAVENTRICULAR HEMORRHAGE. A GESTATIONAL
PATHOLOGICAL EVENT - REVIEW
Zamfir-Radu Ionescu1, Georgiana-Cristina Ionescu2
1Pediatric Hospital, Pitești, Argeș County, România,
2Department of Pediatrics and Neonatology, “Carol Davila”
University of Medicine and Pharmacy
Address for correspondence:
Dr. Zamfir-Radu Ionescu, M.D., Ph.D.
Departament of Pathology, Te Pediatric Hospital of Pitești, acia Bvd, Nr. 1, Pitești, Argeș county, Romania
Tel: 0040346086086.
E-mail:dr.raduionescu@yahoo.com
Received: 09.02.2016
Accepted: 28.02.2016
Med Con June 2016 Vol 11, No 2, 41-44
Abstract
singletons and LBW twins, while a higher birth weight
predisposes the future adult to a high body mass index
Intraventricular hemorrhage (IVH) is defined as the
(BMI) as a cardiovascular risk factor [1]. As broadly
cerebrovascular event that caused hemorrhage to appear
accepted, LBW is defined as a birth weight of a live born
inside one or two ventricles of the brain. IVH is very
below or equal to 2,499 grams (5.5 pounds), regardless of
common in neonates during the immediate perinatal
gestational age. Tis weight should be measured in the
period, with early or late onset, usually having an
first hour from birth to maintain temporal distance from
inconspicuous evolution with later cognitive or motor
any postnatal mass loss. Risk factors for LBW status are
impairement during the development of the child. Tis
either PTB from gestations with less than 37 weeks or
is usually detectable by the transfontanelar ultrasound,
restricted foetal intrauterine growth (RFIG). Te World
combined with flow and magnetic resonance imagery,
Health Organization
(WHO) studies detected many
which might discover IVH during the first hours of life
environmental circumstances that lead to LBW and short
of the premature newborn. Postural techniques, careful
gestational duration: poor or inadequate maternal diet in
examination, manipulation and pharmacological
pregnancy, living in high altitudes, short stature women,
prophylaxis of the premature babies help preventing
exposure to toxic
(alcohol, maternal smoking) or
further complications of the IVH. Te aim of this article
infectious material
(HIV, syphilis) and hypertension.
is a fast review of the available medical literature and to
Some babies have only LBW or PTB, and some others
provide an illumination on the matter.
have both of these conditions, that WHO states as a
Keywords:
intraventricular
hemorrhage,
major disadvantage for babies and main indicator for
prematurity, newborn, neurology, cognitive impairment
immediate postnatal mortality and morbidity [2]. Te
purpose of this article is to offer a review on the pathogeny
Introduction
and investigational attitude for neonatal intraventricular
haemorrhage (IVH) in premature babies.
In modern literature, low birth weight (LBW) and
prematurity in babies (PTB) became a risk factor for
Pathogeny
cardiovascular disease, while intervening modifiable risk
factors could lower the importance of these risks. Tis
Te development of the cerebral blood flow and
implies hypertension and high systolic pressure in
subsequent oxygenation increases along with
Cerebral Intraventricular Hemorrhage. A Gestational Pathological Event
41
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
embryological evolution. As the placenta is removed
become a protective mechanism for the brain to prevent
from circulation and the baby is exposed to outer
further tissue damage. Blood might become observable,
environment, the circulation must meet metabolic
microscopically to the immediate ventricular vicinity.
demands for oxygen two to three times more than those
Also, clots and secondary inflammatory arachnoiditis in
inside the uterus. Different studies show that the
Sylvius aqueduct might imply ventricular enlargement
cerebral flow decreases during the first two hours after
and progressive hydrocephalia [6]. Te main area in
birth and remains with a low pressure for approximately
brain that receive the highest amount of blood before 32
24 hours. Afterwards, the blood flow increases slowly,
weeks of gestation is the caudate nucleus, with a delicate
however inconsistely together with blood pressure,
yet very complex vascularization that allow high local
blood density and oxygenation levels, thus, exposing the
metabolism in order to aid the evolution of neuronal
PTB to increasing risks. Te increasing pressure of
and glial cells to proliferate, differentiate, and migrate to
cerebral blood flow may become dangerously high
later structures [7].
during hypercapnia in babies with respiratory
insufficiency, becoming an etiopathogenic factor for
Staging of the IVH
IVH [3]. Also, it seems that vitamin K deficiency
(VKD) remains a ubiquitous factor for IVH. Divided in
Te first classification for IVH was performed by
early onset VKD, within the first 24 hours, classic VKD
Papile according to CT neuroimaging, still widely used
with evolution in 1 to 7 days interval after birth, and
by pediatric imagists and radiologist, extrapolated to
late onset VKD with highest risk in between 3 weeks to
cranial ultrasonography. Tis grading scale is as follows:
8 months postgestational period. Tis is due to lack of
grade 1 - germinal matrix hemorrhage, grade 2 - IVH
neonatal prophylaxis with vitamin K and exclusive
without ventricular dilation; grade
3
- IVH with
breast-feeding. Late onset VKD is usually associated
ventricular dilation and grade 4 - IVH extended into
with intracranial haemorrhage, in most investigated
adjacent periventricular brain parenchyma [8]. Volpe et
cases being situated in the subdural area (40%) with a
al [9], suggested on pathological findings, that the IV
lesser contribution to IVH (10%). Vitamin K therapy
grade IVH should be noted separately as it mostly
may resolve the haemorrhage in minute, therefore, the
associates with parenchymal involvement. Te system of
early detection of neurological signs combined with
grading is described in percent a manner, like this: grade
neuroimaging should be imperative: rapid ultrasound as
1 - no IVH or IVH occupying less than 10% of the
an efficient screening test, combined with MRI tests or
ventricular area on a parasagittal view; grade 2 - IVH
CT scan, especially in case of MRI equivocal results [4].
occupying 10 to 50% of the ventricular area on a
In every risky gestation, many obstetricians use different
parasagittal view; grade 3 - IVH occupying more than
pharmacological agents in order to decrease uterine
50% of the ventricular area on a parasagittal view. It is
contractility, like indomethacin, a cyclooxygenase
very important to note that periventricular venous
inhibitor that blocks conversion of arachidonic acid to
hemorrhagic infarction should be mentioned separately
prostaglandin. Tis has raised different issues in several
and not attributed, in this case, any grade - like grade
studies, as indomethacin crossed the placental barrier
IV [9].
and inhibits prostaglandin synthesis inside the fetal
body. Te risk of severe IVH according to Papile staging
Detection, evaluation and quantification
- graded III and IV - were significantly higher in infants
of the IVH
from those patients who received tocolysis with
indomethacin, together with necrotizing entercolitis,
First
of
all,
amplitude-integrated
bronchopulmonary dysplasia and increased neonatal
electroencephalography (aEEG) interpreted by at least
mortality [5].
two experienced neonatologists in EEG should be
performed twice in a weeks starting as early as 48h after
Pathology
birth, in order to appreciate continuity and cicling of
cerebral brainwaves at a very early stage and detection of
In some cases, the cerebral hemorrhage in infants is
very short period seizures. In severe IVHs, the typical
confined in the subependymal area of the lateral
aEEG might detect a more discontinuous background
ventricles, and if the evolution progresses, further
pattern, a lack of sleep-wake cycles and a higher
involvement would be visible in the third and fourth
likelihood for seizure activity. Tis investigation should
ventricles. Sometimes, the evacuation of initial bleeding
be performed on a continuous basis in neonatal intensive
from the germinal matrix to the lateral ventricle might
care unit. Some authors perform brain ultrasound
42
Ionescu et al
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
GENERAL REVIEW
assessment with a 8.0 MHz transducer, at 7 days after
for disseminated intravascular coagulopathy or
birth, from 1 to 4 weeks until patient is discharged from
pulmonary embolism [13]. Postural prophylaxis seems
neonatology department. Severe IVHs graded III and
also to contribute to a lower intracranial pressure due to
IV should be additionaly evaluated with magnetic
jugular vascular pressure. Terefore, maintaining a
resonance imagery (MRI) at a correspondent 36 weeks
midline position for the infant head seems to lower risk
with prior parental consent, in order to permit early
for IVH than a sharp turning to a side that can cause, to
detection
of
porencephalic
cysts,
persistent
an extent, the obstruction of the ipsilateral jugular vein
hydrocephalus, cerebellum involution, ventriculomegaly,
and, thus, increasing the intracranial blood pressure.
periventricular
leukomalacia
and parenchymal
Body-tilt, head-elevated and supine repositioning seems
hemosiderin deposits [10]. Together with many other
to be the safer postural position for better cerebral
dangers for PTB, it seems that LBW becomes a frequent
oxygenation with low cranial pressure and a lower
circumstantial factor for cerebral IVH as an additive
chance for IVH [14]. Rapid fluid infusions and volume
condition to subsequent white matter injury and
accelerated repletion should be avoided as they imply
ventriculomegaly. In general practice, IVH might be
further hemodynamic stress both for hearth and brain.
detected either supratentorial or cerebellar. Different
It was observable, in current practice, that speed of
neuroimaging techniques with volumetric quantification
circulatory volume repletion or depletion was not a
might prove decreased cerebellar volume with
major risk, but the amount or volume of that portion
supratentorial neuronal injury and IVH, as an expression
being infused or withdrawn
[15]. Te infants who
of hypoxic and ischemic effects on cerebellum both due
needed ventilation and intubation and received
to volumetric enlargement of the unilateral afflicted
intermittent doses of morphine with no sedation seemed
ventricle and intracranial hypertension [11]. Cerebral
to have reduced IVH incidence, but the poor neurologic
blood flow evaluation might become useful during
outcome remained unmodified [16]. Routine caretaking
immediate antenatal period and the first hour after
like diaper changing, feeding, hot baths, or incubator
birth, either due to Doppler ultrasound techniques or
door opening, heel stabbing for tests or rough
NIRS technology regarding the Beer - Lamber law
manipulation seem to make the friable vasculature of
based on the amount of light absorption by the blood
the PTBs brain prone to high risk for rupture, due to
oxygen, by offering the possibility immediate recovery
high increase in blood volume [17]. In general, during
in a case of a severe blood flow and decreasing nursing
the immediate antenatal period, a complete treatment
costs with more than 400%. However, this technique is
with corticosteroids, had been shown to reduce the risk
not yet popular, as it is still in evaluation in different
for IVH [18]. Also delayed cord clamping could help
neonatal reference centers [12].
better IVH prophylaxis while, during the postnatal time
period, treatment regarding adding surfactant
[19],
Treatment
proper thermoregulation, prophylactic indomethacin
[20] and gentle neonatal care, may significantly reduce
Coagulopathy screening seems to improve survival
the PTB risk for IVH.
of PTBs, especially to those between 23 to 26 weeks
gestation. Some studies suggest using factor VII in
Conclusion
prevention of IVH, with no further increasing the risk
Intraventricular hemorrhage remains an important
risk factor for all children with a degree of prematurity
and perinatal issues. Te main sequelae after IVH
remain motor deficit, later cognitive impairment in
afflicted child, muscular weakness and hypertonia. In
the majority of cases, these anomalies are the direct
result of improper neonatal handling, aggressive tests
and blood sampling or bad positioning of the new-born.
Treatment regarding intracerebral hemorrhages in
general, and IVH in particular are a necessity for
immediate course of action, as an early intervention
might limit later cognitive and motor impairment of the
Figure 1. Transfontanelar ultrasound aspect of IVH staged as a
child. Still having a high incidence, IVH keeps also a
IIIrd degree with unilateral right ventricular enlargment of a
high rate of mortality among new-born children.
35 weeks and two days old live birth (personal collection)
43
Cerebral Intraventricular Hemorrhage. A Gestational Pathological Event
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
References
Intraventricular Hemorrhage and White Matter Injury
on Preterm Cerebellar Growth. J Pediatr.
1.
Kwok MK, Yeung SLA, Leung GM, Mary Schooling C.
2011;158(3):366-71.
Birth weight and adult cardiovascular risk factors using
12.
Elser HE, Holditch-Davis D, Brandon DH. Cerebral
multiple birth status as an instrumental variable in the
Oxygenation Monitoring: A Strategy to Detect
British 1958 birth cohort. Prev Med P. 2016;84:69-75.
Intraventricular Hemorrhage and Periventricular
2.
World Health Organization and UNICEF. Low
Leukomalacia.
Neuroprotective
Strateg.
Birthweight: Country, Regional and Global Estimates.
2011;11(3):153-9.
13.
Dani C, Poggi C, Ceciarini F, Bertini G, Pratesi S,
publications/index_24840.html
Rubaltelli FF. Transfusion Practice: Coagulopathy
3.
Cooke RWI, Rolfe P, Howat P. Apparent cerebral
screening and early plasma treatment for the prevention
blood-flow in newborns with respiratory disease. Dev
of intraventricular hemorrhage in preterm infants.
Med Child Neurol.
1979;21(2):154-60. DOI:
Transfusion (Paris). 2009;49(12):2637-44.
10.1111/j.1469-8749.1979.tb01596.x
14.
Schrod L, Walter J. Effect of Head-Up Body Tilt
4.
Volpe JJ. Intracranial Hemorrhage in Early Infancy—
Position on Autonomic Function and Cerebral
Renewed Importance of Vitamin K Deficiency. Pediatr
Oxygenation in Preterm Infants. Neonatology.
Neurol. 2014;50(6):545-6.
2002;81(4):255-9.
5.
Hammers AL, Sanchez-Ramos L, Kaunitz AM.
15.
Hüning BM, Horsch S, Roll C. Blood sampling via
Antenatal exposure to indomethacin increases the risk of
umbilical vein catheters decreases cerebral oxygenation
severe
intraventricular
hemorrhage, necrotizing
and blood volume in preterm infants. Acta Pædiatrica.
enterocolitis, and periventricular leukomalacia: a
2007;96(11):1617-21.
systematic review with metaanalysis. Am J Obstet
16.
Anand K, Hall RW, Desai N, Shephard B, Bergqvist
Gynecol. 2015;212(4):505.e1-505.e13.
LL, Young TE, et al. Effects of morphine analgesia in
6.
Kenner C, Edds JW, Blackburn ST, Ditzenbeger GR.
ventilated preterm neonates: primary outcomes from the
Neurologic system. In: Comprehensive neonatal care: an
NEOPAIN randomised trial. Te Lancet.
interdisciplinary approach.
4th ed. St. Louis: W.B.
2004;363(9422):1673-82.
Saunders; 2007. p. 267-99.
17.
Gagnon RE, Leung A, Macnab AJ. Variations in
7.
Bassan H. Intracranial Hemorrhage in the Preterm
Regional Cerebral Blood Volume in Neonates Associated
Infant: Understanding It, Preventing It. Neurol
with Nursery Care Events. Amer J Perinatol.
Newborn Infant. 2009;36(4):737-62.
2008;16(01):7-11.
8.
Papile LA, Burstein J, Burstein R, Koffler H. Incidence
18.
Chawla Sanjay, Natarajan Girija, Rane Sharayu,
and evolution of subependymal and intraventricular
Tomas Ronald, Cortez Josef, Lua Jorge. Outcomes of
hemorrhage: A study of infants with birth weights less
extremely low birth weight infants with varying doses
than 1,500 gm. J Pediatr. 1978;92(4):529-34.
and intervals of antenatal steroid exposure. J Perinat
9.
Volpe J. Intracranial hemorrhage: germinal matrix -
Med. 2010;38(4):419.
intraventricular hemorrhage. In: Neurology of the
19.
Walti H, Paris-Llado J, Egberts J, Brand R, Bevilacqua
Newborn. 5th ed. Philadelphia, PA: Elsevier Saunders;
G, Gardini F, et al. Prophylactic Administration of
2008. p. 492-581.
Porcine-Derived Lung Surfactant Is a Significant Factor
10.
Sohn JA, Kim H-S, Lee EH, Lee J, Lee JA, Choi CW,
in Reducing the Odds for Peri-Intraventricular
et al. Developmental change of amplitude-integrated
Haemorrhage in Premature Infants. Neonatology.
electroencephalographic activity in preterm infants with
2002;81(3):182-7.
intraventricular hemorrhage. Early Hum Dev.
20.
Ment LR, Vohr BR, Makuch RW, Westerveld M,
2013;89(12):961-6.
Katz KH, Schneider KC, et al. Prevention of
11.
Tam EWY, Miller SP, Studholme C, Chau V, Glidden
intraventricular hemorrhage by indomethacin in male
D, Poskitt KJ, et al. Differential Effects of
preterm infants. J Pediatr. 2004;145(6):832-4.
44
Ionescu et al
GENERAL REVIEW
TRANSPERITONEAL VS. RETROPERITONEAL LAPAROSCOPIC
NEPHRECTOMY FOR RENAL CELL CARCINOMA: A GENERAL
REVIEW
Cristian Bogdan Rusu1, Bogdan Ovidiu Feciche1, Lilian Gorbatai1, Tiberiu Botezan1,
Bogdan Bumbuluț2, Andrei Bumbuluț3, Rumelia Koren4
1Department of Urology, Satu Mare County Emergency Hospital, 2Department of Urology, Sibiu County Emergency
Clinical Hospital,
3Faculty of Medicine, ”Iuliu Haţieganu” University of Medicine and Pharmacy, Cluj Napoca,
4Department of Pathology, Hasharon Hospital, Petah-Tikva, affiliated to Sackler School of Medicine Tel-Aviv University,
Israel
Address for correspondence:
Dr. Cristian Bogdan Rusu
Departament of Urology, Satu Mare County Emergency Hospital
1 Prahova St, Satu Mare, Satu Mare County, România
E-mail:cbrusu@yahoo.com
Received: 20.03.2016
Accepted: 29.04.2016
Med Con June 2016 Vol 11, No 2, 45-47
Abstract
laparoscopic partial nephrectomy, retroperitoneal
laparoscopic partial nephrectomy, length of hospital
Renal cell carcinoma is the most common type of
stay, estimated blood loss, surgical time
kidney cancer in adults. Surgical resection - radical or
partial - of the kidney remains the only known curative
Introduction
treatment for localized renal cell carcinoma.
Laparoscopic radical or partial resection can be
Renal cell
carcinoma
(RCC) represents
performed either the transperitoneal or retroperitoneal
approximately
3% of all cancers, being the most
approach, and each of them has its own advantages and
common type of kidney cancer in adults, with 90-95%
limitations, with no definitive conclusions regarding the
of neoplasms arising from the kidney. With a mean
objective differences in outcomes. Te studies suggest
increase of 2-3% per year, and the highest incidence
that the retroperitoneal approach has a shorter time to
occurring in Western countries, the incidence rates of
renal vascular control and a shorter operating time than
RCC have risen steadily during three decades of the
the transperitoneal. In appropriately selected patients, as
twentieth century in most of the world [1].
those with posteriorly located renal tumours, the
Surgical resection of the kidney - radical nephrectomy
retroperitoneal approach may be faster and equally safe
(RN), or the tumour - partial nephrectomy (PN), remains
compared with the transperitoneal approach. In the
the only known curative treatment for localized renal cell
extremely obese patient, the retroperitoneal approach
carcinoma. Traditionally, RN or PN has been performed
tended to have advantages in blood loss, operative
using the open surgical approach through a large flank
duration, specimen weight, open conversion rate, and
incision, intervention associated with substantial pain
duration of hospital stay.
and morbidity. Clayman et al. [2] performed in 1991 the
Keywords: renal cell carcinoma, transperitoneal
first transperitoneal laparoscopic radical nephrectomy
laparoscopic radical nephrectomy, retroperitoneal
(TLRN). After
1991, TLRN has gained increasing
laparoscopic radical nephrectomy, transperitoneal
worldwide acceptance because of its benefits regarding
Transperitoneal vs. Retroperitoneal Laparoscopic Nephrectomy for Renal Cell Carcinoma
45
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
patient recovery and perioperative morbidity. Several
tumors, RLRN may be faster and equally safe compared
long-term studies have shown that the outcomes of
with TLRN. One advantage of the retroperitoneoscopic
TLRN are similar to those of open surgery [3-6].
access seems to be a shorter total surgical time [7]. Te
Laparoscopic RN or PN can be performed either
transperitoneal approach should be chosen based on
the transperitoneal (TLRN, TLPN), or retroperitoneal
tumor size and location to minimize vascular injury
approach (RLPN, RLRN), and each of them has its
[11].
own advantages and limitations, with no definitive
Regarding the operating time for PN, pooled data
conclusions regarding the objective differences in
[10] showed that operating time was significantly
outcomes. Tis is the reason that we performed a general
shorter in retroperitoneal laparoscopic partial
review of the available literature to compare the
nephrectomy (RLPN) than transperitoneal laparoscopic
outcomes of the two approaches.
partial nephrectomy (TLPN). Te warm ischaemia time
(WIT) for PN showed no significant difference between
Methods
TLPN and RLPN.
Pooled data from the studies that reported the
A search of MEDLINE library was performed to
estimated blood loss
(EBL) for RN, showed no
identify relevant studies; the search terms were
significant difference between RLRN and TLRN,
‘(laparoscopic nephrectomy)
[Title/Abstract] AND
respective between TLPN and RLPN [10,11-20].
(transperitoneal OR retroperitoneal) [Title/Abstract].’
For the postoperative variables, there were no
Articles were also searched using the ‘related articles’
significant differences between TLRN and RLRN in the
function. Te reference lists of retrieved articles were
LOS or time to first oral intake. Several studies reported
manually searched to identify related articles. Te latest
LOS for PN a significant difference favouring RLRN.
date of this search was 28 February 2016.
No significant difference in analgesic requirements
(morphine, pethidine, non-steroidal anti-inflammatory
Results
drugs) was found between TLRN and RLRN, as well
between TLPN and RLRN [10].
Transperitoneal
laparoscopic
and
Te surgical complication rate was significantly lower
retroperitoneoscopic partial nephrectomy provide
in RLRN than TLRN and also significantly lower in
comparable surgical and functional results [7]. Although
RLRN than in TLRN. Tere were no significant
both transperitoneal laparoscopic radical nephrectomy
differences between RLRN and TLRN in postoperative
and retroperitoneal laparoscopic radical nephrectomy
complication rate, open conversion rate or blood
are feasible options, RLRN is associated with
transfusion rate. Te overall complications, intra-
significantly less pain, less analgesic requirement, shorter
operative complication rate, postoperative complication
length of hospital stay (LOS), and short convalescence
rate, or open conversion rate, had no significant
as compared with TLRN [8].
differences between TLPN and RLPN [10].
Both TLRN and RLRN are safe, feasible and
Regarding oncological variables there were no
effective for surgical management of complex localized
significant differences between TLRN and RLRN in
tumors, but TLRN offers larger operative space with
overall recurrence rate, local recurrence rate, or distant
better exposure; RLRN better promotes postoperative
recurrence rate; for PN there were no significant
recovery of the patients [9].
difference between TLPN and RLPN [10].
A meta-analysis [10] which included 12 studies
In the extremely obese patient, RLRN tended to
comparing RLRN with TLRN and six studies
have advantages in EBL, operative duration, specimen
comparing RLPN with TLPN, demonstrate regarding
weight, open conversion rate, and duration of hospital
the perioperative variables that the operating time for
stay. RLRN provides direct access to the renal hilum,
RN was slightly shorter in RLRN than TLRN; time to
and avoids the pannus and voluminous intra-abdominal
renal artery control was significantly longer in TLRN
fat encountered during TLRN [21].
than RLRN and time to renal vein control was also
significantly longer in TLRN then RLRN, as the
transperitoneal
approach requires considerable
References
mobilization to access the renal hilum, whereas the
retroperitoneal approach provides direct and rapid
1. Mathew A, Devesa SS, Fraumeni JF Jr, Chow WH.
access to the renal hilum. Tis meta-analysis
[10]
Global increases in kidney cancer incidence, 1973-1992.
indicates that in patients with posteriorly located renal
Eur J Cancer Prev. 2002;11:171-8.
46
Rusu et al
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
GENERAL REVIEW
2.
Clayman RV, Kavoussi LR, Soper NJ et al.
12.
Tsujihata M, Nonomura N, Momohara C et al.
Laparoscopic nephrectomy: initial case report. J Urol.
Clinical
experience
with laparoscopic radical
1991;146:278-82.
nephrectomy for renal cell carcinoma. Urol Int.
3.
Burgess NA, Koo BC, Calvert RC et al. Randomized
2008;81:301-5.
trial of laparoscopic v open nephrectomy. J Endourol.
13.
Xu ZL, Wang LH, Chen W et al. Transperitoneal
2007;21:610-3.
versus retroperitoneal laparoscopic radical nephrectomy:
4.
Permpongkosol S, Chan DY, Link RE et al. Long-term
a comparison of clinical outcomes. Acad J Second
survival analysis after laparoscopic radical nephrectomy. J
Military Med Univ. 2011;32:938-41.
Urol. 2005;174:1222-5.
14.
Desai MM, Strzempkowski B, Matin SF et al.
5.
Portis AJ, Yan Y, Landman J et al. Long-term followup
Prospective randomized comparison of transperitoneal
after laparoscopic radical nephrectomy. J Urol.
versus retroperitoneal laparoscopic radical nephrectomy. J
2002;167:1257-62.
Urol. 2005;173:38-41.
6.
Luo JH, Zhou FJ, Xie D et al. Analysis of long-term
15.
Negoro H, Shiraishi Y, Sugino Y et al. Laparoscopic
survival in patients with localized renal cell carcinoma:
radical nephrectomy for renal cell carcinoma at Kobe
laparoscopic versus open radical nephrectomy. World J
City General Hospital. Acta Urol Jpn. 2005;51:369-
Urol. 2010;28:289-93.
72.
7.
Marszalek M, Chromecki T, Al-Ali BM, Meixl H,
16.
Nambirajan T, Jeschke S, Al-Zahrani H et al.
Madersbacher S, Jeschke K, Pummer K, Zigeuner R.
Prospective, randomized controlled study: transperitoneal
Laparoscopic partial nephrectomy: a matched-pair
laparoscopic
versus
retroperitoneoscopic
radical
comparison of the transperitoneal versus theretroperitoneal
nephrectomy. Urology. 2004;64:919-24.
approach. Urology. 2011;77(1):109-13.
17.
Nadler RB, Loeb S, Clemens JQ et al. A prospective
8.
Garg M, Singh V, Sinha RJ, Sharma P. Prospective
study of laparoscopic radical nephrectomy for T1 tumors
randomized comparison of transperitoneal vs
- is transperitoneal, retroperitoneal or hand assisted the
retroperitoneal laparoscopic simple nephrectomy. Urology
best approach? J Urol. 2006;175:1230-4.
2014;84(2):335-9.
18.
Jung MH, Tae HK, Won YC et al. Comparison of
9.
Pu X, Xu Z, Liu J, Zheng X, Li D, Luo Y, Xian Z.
techniques for laparoscopic radical nephrectomy in a
Clinical efficacy of transperitoneal versus retroperitoneal
single center: transperitoneal vs. retroperitoneal vs. hand-
laparoscopic partial nephrectomy for renal tumors with
assisted. Korean J Urol. 2009;50:675-81.
R.E.N.A.L score over 7. Nan Fang Yi Ke Da Xue Xue
19.
Ha US, Hwang TK, Kim YJ et al. Comparison of
Bao/Journal of Southern Medical University.
oncological
outcomes
of
transperitoneal
and
2014;34(12):1818-21.
retroperitoneal laparoscopic radical nephrectomy for the
10.
Fan X, Xu K, Lin T, Liu H, Yin Z, Dong W, Huang H,
management of clear-cell renal cell carcinoma: a multi-
Huang J. Comparison of transperitoneal and
institutional study. BJU Int. 2011;107:1467-72.
retroperitoneal laparoscopic nephrectomy for renal cell
20.
Okegawa T, Noda H, Horie S et al. Comparison of
carcinoma: a systematic review and meta-analysis. BJU
transperitoneal
and retroperitoneal laparoscopic
Int. 2013;111(4):611-21.
nephrectomy for renal cell carcinoma: a single-center
11.
Taue R, Izaki H, Koizumi T, Kishimoto T, Oka N,
experience of 100 cases. Int J Urol. 2008;15:957-60.
Fukumori T, Takahashi M, Kanayama HO.
21.
Berglund RK, Gill IS, Babineau D, Desai M, Kaouk
Transperitoneal versus retroperitoneal laparoscopic radical
JH. A prospective comparison of transperitoneal and
nephrectomy: a comparative study. Int J Urol.
retroperitoneal laparoscopic nephrectomy in the extremely
2009;16(3):263-7.
obese patient. BJU Int. 2007;99(4):871-4.
47
Transperitoneal vs. Retroperitoneal Laparoscopic Nephrectomy for Renal Cell Carcinoma
Medical Connections/Conexiuni Medicale
Conflict-of-Interest Statement
Medical Connections/Conexiuni Medicale (Med Con) requires all authors and reviewers to declare any
conflicts of interest that may be inherent in their submissions.
Conflict of interest for a given manuscript exists when a participant in the peer review and publication
process-author, reviewer, or editor - has ties to activities that could inappropriately influence his or her
judgment, whether or not judgment is in fact affected.
Financial relationships with industry, for example, through employment, consultancies, stock
ownership, honoraria, expert testimony, either directly or through immediate family, are usually considered
to be the most important conflicts of interest. However, conflicts can occur for other reasons, such as
personal relationships, academic competition, and intellectual passion.
Public trust in the peer review process and the credibility of published articles depend in part on how
well conflict of interest is handled during writing, peer review, and editorial decision making. Bias can
often be identified and eliminated by careful attention to the scientific methods and conclusions of the
work. Financial relationships and their effects are less easily detected than other conflicts of interest.
Participants in peer review and publication should disclose their conflicting interests, and the information
should be made available so that others can judge their effects for themselves.
Authors: When they submit a manuscript, whether an article or a letter, authors are responsible for
recognizing and disclosing financial and other conflicts of interest that might bias their work. Tey should
acknowledge in the manuscript all financial support for the work and other financial or personal
connections to the work.
Reviewers: External peer reviewers should disclose to editors any conflicts of interest that could bias
their opinions of the manuscript, and they should disqualify themselves from reviewing specific
manuscripts if they believe it appropriate. Te editors must be made aware of reviewers’ conflicts of interest
to interpret the reviews and judge for themselves whether the reviewer should be disqualified. Reviewers
should not use knowledge of the work, before its publication, to further their own interests.
Manuscript Title: _ __________________________________________________________
I declare no conflict of interest
I declare the following potential conflict of interest:
_ _________________________________________________________________________
_ _________________________________________________________________________
_ _________________________________________________________________________
_ _________________________________________________________________________
_ _________________________________
_ _________________________________
Name
Signature/Date
Please fax or mail this signed form to the Med Con Editorial Office.
Fax: +40-261-710456
Mail: colmedsm@gmail.com
GENERAL REVIEW
TREATMENT WITH HUMAN MILK FOR ADULTS CONDITIONS
Mihaela N. Niță
Romanian Lactation Consultants Association
Address for correspondence:
Mihaela N. Niță MD, IBCLC
E-mail: mihaelanita11@gmail.com
Received: 14.05.2016
Accepted: 01.06. 2016
Med Con June 2016 Vol 11, No 2, 49-52
Abstract
practice, donated milk can serve many purposes to the
same beneficiary [3].
Breastfeeding is the standard method of feeding
Breast milk can be considered a biological dynamic
infants and small children. When own mother’s milk is
system species-specific, which contains specific bioactive
not available, the first choice, if available, is donated
factors and immunomodulators: gastrointestinal
human milk. Human milk banks prioritize deliveries of
hormones, immunoglobulins, lactoferrin, lysozyme,
donated human milk. Among the indications of human
oligosaccharides, nucleotides, growth factors, enzymes,
milk are also adults with various medical conditions. In
antioxidants and cellular components that provide host
their case, using human milk is therapeutical,
defense against infections, modulates the immune
nutritional, preventive and paleative. Te article’s aim is
response and changes the intestinal bacterial flora [4,5].
to summarize the conclusions of expert articles on the
use of human milk by adults.
Using donated breast milk for adults
Keywords: human milk, donated human milk,
HAMLET, stem cells
Studies concentrated on cultural variations in
breastfeeding say that historically it is not uncommon
Introduction
for women to breastfeed the elderly from their families
[6]. Te theme of breastfeeding the elderly was used in
It is recognized that breastfeeding is the standard
art. For example, the canvas „Roman Charity” presented
method of feeding infants at term exclusively until 6
in Rijkmuseum, Amsterdam shows how the lactating
months of age, followed by complemantary feeding along
mother breastfeeds her father enprisoned and sentenced
with breastfeeding until the age of 2 years and beyond.
to death by starvation.
Te benefits of breastfeeding for healthy babies at term
Te scientific basis for this practice were until not
and their mothers are well known. Own mother’s milk is
long ago unknown.
the first choice for all infants, including premature
Te study elaborated by a team of researchers from
neonates, but when it is not available or not in sufficient
the University of Gothenburg and Lund, Sweden,
quantity donated breast milk is the next option [1].
wanted to investigate the antimicrobial activity of
Breast milk is not only optimal nutrition for
human milk. Te study found that breast milk killed
neonates and infants but is used prophylactically and
cancer cells in vitro, a property due to an alpha-
therapeutically against many diseases of infants and
lactalbumin - multimeric protein.
young children and in certain circumstances even for
Tis protein together with a fatty acid, oleic acid, is
adults
[2]. Using donated milk can be divided into
forming the compound of HAMLET (Human Alpha-
nutritional, medicinal, therapeutic and preventive. In
lactalbumin Made Lethal to Tumour cells). Tis
Treatment with Human Milk for Adults Conditions
49
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
formation occurs after treating human milk in casein in
Using donated milk may be beneficial for adults
low pH [7,8]. Childrens’ gastric acidity promotes the
with cancer and other medical conditions.
formation of HAMLET. Tis mechanism may
Small amounts of donated milk may improve IgA
contribute to the anticancer effect of breastfeeding
levels in individuals with imunodeficiencies as those
against tumors in childhood [9]. Laboratory experiments
who undergo treatments such as radiotherapy and
have shown that this compound kills 40 types of cancer
chemotherapy [10].
cells. Te anticancer activity affects embryonic cells, but
Breast milk is the richest source available in IgA
not the mature cells [8,10].
being used successfully for infants, children and adults
Based on this discovery HAMLET compound has
with immunodeficiencies [15].
been used in patients with bladder cancer. Excretion in
IgA deficiency is associated with high mortality
the urine of dead cancer cell was observed every time
(42% to 120 days) after liver transplantation. Most of
HAMLET was used, leading to hopes for future
the deaths were related to intestinal infections. Breast
development of bladder cancer treatment [8,11].
milk or donated human milk have beneficial effects
Because malignant brain tumors represent a major
because of the protection against microbial translocation
therapeutic challenge, the study by Fischer and his
and enteric infections [16].
colleagues tested the intratumoral administration of
In a study, two IgA deficient patients received breast
HAMLET, noting prolonged survival in a human
milk orally for
10 days perioperative after liver
glioblastoma xenograft model by inducing selective
transplantation. Both patients had a postoperative
apoptosis of tumor cells. HAMLET therapy reduced
period without infection, with increased levels of IgA.
tumor volume and delayed signs of intracranial
Researchers have concluded that breast milk can be used
hypertension. In vivo HAMLET caused apoptosis of
in IgA deficient patients after liver transplantation to
the tumoral cells but not of the adjacent brain tissue and
reduce infectious complications in the postoperative
astrocytes, and did not have apparent toxic side effects.
period [16].
Te study identified HAMLET as a new candidate in
Donated human milk is used for liver regeneration.
anticancer therapy for controlling progression of
A liver transplant unit in Oklahoma Cityis is using
glioblastomas [12].
donated human milk to treat adult patients with
Programmed cell death in response to HAMLET is
transplants. Donated milk is infused into the surgical
independent of caspases, p53 and Bcl-2, even if
field and in the intestinal tract during surgery. Te
HAMLET activates an apoptotic response. Using other
patient then received daily oral doses of donated milk to
mechanisms of apoptosis allows HAMLET to have an
improve the levels of IgA. Surgeons have noticed that it
activity that is not affected by anti-apoptotic strategies
has improved immunological status of patients and that
present in tumor cells [13].
fewer cases of transplant reject occurred [10].
Recent study by Zang and al. investigated the anti-
Te relationship between breastfeeding and better
cancer activity of alpha-lactalbumine and oleic acid
post-transplant outcomes has been established in the
complex
(Compound HAMLET). By using modern,
case of breastfed children receiving renal transplants
innovative techniques, the study concluded that HAMLET
from their mothers [17].
affects the stability of the cytoskeleton, cell motility, inhibits
Breast milk promotes maturation of the
the DNA, lipids and synthesis of adenosine triphosphate,
gastrointestinal tract and protects babies against
leading to cell stress and activation of apoptosis, thus
gastrointestinal diseases.
establishing the theoretical basis for its action with
An article published the case of a 24 year old man
possibilities for use in cancer therapy [14].
who has had two episodes of severe gastro-esophageal
Te study by Petterson and al. aimed to see if
reflux with no digestive tolerance not even for
HAMLET-like complexes are present in other species.
rehydration salts. After the administration of milk or
Tey studied human milk, bovine, equine and porcine
donated human milk his condition and digestive
milk. Te conclusion was that the natural formation of
tolerance was greatly improved [18].
complexes HAMLET is unique to human milk casein,
Breast milk contains several compounds that may
which has the highest oleic acid content [7].
explain the evolution of the case presented above. Tese
Donated milk may help to recolonize the digestive
compounds are growth factors, anti-inflammatory
tract in people who have had gastrointestinal side effects
factors and opioid-like peptides. Epidermal growth
after anticancer conventional treatment. It can protect
factor
(EGF) is one of the most active peptides in
the gastrointestinal mucosa of subsequent aggression
human milk. It increases mitosis and proliferation of
[10].
epithelial cells in the lungs, the gastrointestinal system
50
Niță et al
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
GENERAL REVIEW
and in other tissues of epidermal origin. Accelerates
Mammary stem cells are responsible for the changes
wound healing of the cornea and other epidermal tissue
through which the mammary gland passes during lactation.
of origin. In addition, EGF inhibits histamine-
Tey are present in breast milk and the breastfed infant
stimulated secretion of gastric acid, thereby helping the
ingested them. Tese cells are pluripotent stem cells and
healing of gastric ulcers [18].
can differentiate not only into specific cells in the breast
Growth factors in human milk stimulates the
but also into other types of cells such as neuronal-like cells.
production of mucus in the stomach and duodenum, a
Tey can be used in the „cell replacement therapies” for
dose-dependent effect of protecting the intestinal
patients suffering from central nervous system injury, with
mucosa. EGF is stable during pasteurization in the
possible applications in regenerative medicine, in diseases
presence of acid and is resistant to enzymatic digestion.
such as diabetes and Parkinson’s disease [21].
In tissue culture, EGF stimulated DNA synthesis in the
Te results of studying the components of breast
cells which have stopped growing [18].
milk does not cease to surprise us.
Te anti-inflammatory properties of human milk
Te implications of these findings go beyond the
are important in limiting the immune responses to
nutriton of infants and small children to the
reduce inflammation.
therapeutical effects on the medical conditions in adults.
Opioid-like peptides, prostaglandins and mucin-
like compounds have cytoprotective effect on the
gastrointestinal mucosa that is less exposed to aggressive
References
factors. It is possible that these compounds act in a
synergistic manner.
1.
American Academy of Paediatrics. Breastfeeding and use
Breast milk could enter în the therapeutic aproaches
of human milk. Pediatrics. 2012;129:e827-41.
of serious gastrointestinal diseases in adults [18].
2.
Tully MR. Recipient Prioritization and Use of Human
Breast milk can be used to improve the quality of
Milk in the Hospital Setting. Journal of Human
life of cancer patients and to alleviate the side effects of
Lactation. 18(4):393-6.
medication. In a study in which milk has been used for
3.
Arnold LDW. Becoming a Donor to a Human Milk
cancer patients, the pacients stated that it was very well
Bank. LEAVEN. 2000;36(2),19-23.
tolerated, they experienced an alleviation of difficulties
4.
Bertino E, Giuliani F, Occhi L, Coscia A, Tonetto P,
in swallowing, reduced episodes of nausea and vomiting,
Marchino F, Fabris C. Benefits of donor human milk for
weakness and lethargy usually occured after initiation of
preterm infants: Current evidence. Early Human
chemotherapy. Patients reported an improvement of
Development. 2009;85,S9-S10.
their general condition, energy levels, respiratory
5.
Bertino E, Di Nicola P, Giuliani F, Peila C, Cester E,
function and apetite.
Vassia C, Pirra A, Tonetto P, Coscia A. Benefits of human
Te improvement of the quality of life is an important
milk in preterm infant feeding. Journal of Pediatric and
factor for patients with cancer. Patients in this study, with
Neonatal Individualized Medicine. 2012;1(1):19-24.
moderate and severe forms of cancer, have noted an
6.
Baumslag N. Breastfeeding: cultural practices and
improvement in the quality of life- physical, mental and
variations. Adv Int Mat Child Health. 1987;7:36-50.
spiritual. Currently, milk banks are able to meet the needs
7.
Pettersson J, Mossberg AK, Svanborg C. alpha-
of cancer patients who use this therapy
[19]. Using
Lactalbumin species variation, HAMLET formation,
donated milk for adults is temporary and not in large
and tumor cell death. Biochem Biophys Res Commun.
amounts as to influence deposits of donated human milk
2006;345(1):260-70.
for infants [10]. Te average quantity of milk received by
8.
Håkansson A, Zhivotovsky B, Orrenius S, Sabharwal H,
adult cancer patients from
11 Human milk banks
Svanborg C. Apoptosis induced by a human milk
members of Human Milk Bank Association of North
protein. Proc Natl Acad Sci USA. 1995,92:8064-8.
America in 2005 was low, from 4% to 4.5% of the total
9.
Svanborg C, Agerstam H, Aronson A, Bjerkvig R,
human milk donated that year [19].
Düringer C, Fischer W, Gustafsson L, Hallgren O,
Te presence of stem cells in breast milk was
Leijonhuvud I, Linse S, Mossberg AK, Nilsson H,
discovered by dr. Cregan in 2007. Tese cells had a
Pettersson J, Svensson M. HAMLET kills tumor cells by
marker, nestin, characteristic of stem cells. Te presence
an apoptosis-like mechanism-cellular, molecular, and
of such cells indicates that the milk can become an
therapeutic aspects. Adv Cancer Res. 2003;88:1-29.
available, non-invasive stem cells source that can be
10.
Arnold LD. Possibilities for donor milk use in adult
used both in biological research of the mammary gland
clinical settings-a largely unexplored area. J Hum Lact.
and in the stem cell biology [20].
1996;12(1):59-60.
51
Treatment with Human Milk for Adults Conditions
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
11.
Mossberg AK, Wullt B, Gustafsson L, Månsson W,
16.
Merhav HJ, Wright HI, Mieles LA, Van Tiel DH.
Ljunggren E, Svanborg C. Bladder cancers respond to
Treatment of IgA deficiency in liver transplant recipients
intravesical instillation of HAMLET (human alpha-
with human breast milk. Transplant Int. 1995;8:327-
lactalbumin made lethal to tumorcells). Int J Cancer.
9.
2007;121(6):1352-9.
17.
Campbell DA, Lorber MI, Sweeton JC, Turcotte JG,
12.
Fischer W, Gustafsson L, Mossberg AK, Gronli J,
Niederhuber JE, Beer AE. Breast feeding and maternal-
Mork S, Bjerkvig R, Svanborg C. Human alpha-
donor renal allografts. Transplantation. 1984,37:340-
lactalbumin made lethal to tumor cells (HAMLET) kills
4.
human glioblastoma cells in brain xenografts by an
18.
Wiggins PK, Arnold LD. Clinical case history: donor
apoptosis-like mechanism and prolongs survival. Cancer
milk use for severe gastroesophageal reflux in an adult. J
Res. 2004;64(6):2105-12.
Hum Lact. 1998;14(2):157-9.
13.
Hallgren O, Gustafsson L, Irjala H, Selivanova G,
19.
Rough SM, Sakamoto P, Fee CH, Hollenbeck CB.
Orrenius S, Svanborg C. HAMLET triggers apoptosis
Qualitative Analysis of Cancer Patients’ Experiences
but tumor cell death is independent of caspases, Bcl-2
Using Donated Human Milk. J Hum Lact.
and p53. Apoptosis. 2006;11(2):221-33.
2009;25(2):211-9.
14.
Fang B, Zhang M, Fan X, Ren FZ. Te targeted
20.
Cregan MD, Fan Y, Appelbee A, Brown ML, Klopcic
proteins in tumor cells treated with the α-lactalbumin-
B, Koppen J, Mitoulas LR, Piper KM, Choolani MA,
oleic acid complex examined by descriptive and
Chong YS, Hartmann PE. Identification of nestin-
quantitative liquid chromatography-tandem mass
positive putative mammary stem cells in human
spectrometry. J Dairy Sci.
2016. [Epub ahead of
breastmilk. Cell Tissue Res. 2007;329(1):129-36.
print]
21.
Twigger AJ, Hodgetts S, Filgueira L, Hartmann PE,
15.
Tully MR, Lockhart-Borman L, Updegrove K. Stories
Hassiotou F. From Breast Milk to BrainsTe Potential
of Success: Te Use of Donor Milk Is Increasing in North
of Stem Cells in Human Milk. J Hum Lact.
America. J Hum Lact. 2004,20(1):75-7.
2013;29(2)136-9.
52
Niță et al
GUIDANCE FOR DRAWING UP
GUIDANCE FOR AUTHORS
Scope
on which patients or other subjects of your experiments
Te Medical Connections publishes papers reporting
clearly grant permission for the publication of
original clinical and scientific research, which contribute
photographs or other material that might identify them.
to the advancement of knowledge in all field of
If the consent form for your research does not specifically
medicine. Te journal also publishes reviews, editorials
include this, please obtain it or remove the identifying
and short communications on specific topics. Case
material. A statement must be included in the ‘Methods’
reports will be accepted if of great interest and well
section of your paper.
investigated. Letters to the Editor, especially those
mentioning an opinion on an article previously
Ethics Committee approval
published, or expressing a new finding are welcome. Te
You must state clearly in your submission in the
website address of the Medical Connections is http://
Methods section that you conducted studies on human
participants with the approval of the Hospital, or
quarterly and papers are accepted for publication in
University Ethics Committee etc. Similarly, you must
English language. Papers from contributors living
confirm that experiments involving animals adhered to
abroad and from Romanian authors should be addressed
ethical standards.
to the editorial office: dr. Bumbuluţ Călin, assitant
editor in chief of Medical Connections, Eroilor
Copyright assignment
Revoluţiei Pl. no.23-440055 Satu Mare, Romania. Tel./
Papers are accepted for publication on the
Fax: +40-261-710456, e-mail: bumbulutcalin@yahoo.
understanding that exclusive copyright in the paper is
com.
assigned to the Publisher. Authors may use material
from their paper in other works published by themselves.
Redundant or duplicate publication
We ask you to confirm that your paper has not been
Submissions
published in its current form or a substantially similar
All manuscripts submitted to the Medical
form, that it has not been accepted for publication by
Connections are made available for online review. Te
another journal, and that it is not under consideration
journal introduced the electronic submission of
by another publication.
manuscripts in Word format, but also accepts
manuscripts submitted as attachments to electronic
Conflicts of interest
mail (text, figures and tables). Do not send them in
We ask authors to state all possible conflicts of
PDF format. Te word count for electronic submissions
interest, including financial and other relationships. If
is up to 3,500 words for original articles, 2,500 words
you are sure that there is no conflict of interest, please
for case reports, 2,000 for clinical imaging papers, 500
state this also. Te sources of funding should be
words for letters, and 4,500 words for review articles.
acknowledged in your paper.
Authors should NOT in addition post a hard copy
submission to the editorial office, unless they are
Permissions to reproduce previously
supplying artwork, letters or if les that cannot be
published material
submitted electronically, or have been instructed to do
Please send us copies of permission to reproduce
so by the editorial office. For those authors who have no
material (such as illustrations) from the copyright holder.
option but to submit by mail please send one copy of
the article, plus an electronic version on CD-ROM to
Patient consent forms
the Editorial Office, Conexiuni Medicale/Medical
Te protection of a patient’s right to privacy is
Connections, Eroilor Revoluţiei Pl. no.23-440055 Satu
essential. Please send copies of patient’s consent forms
Mare, Romania. Double spacing should be used
Guidance for Authors
53
Guidance for drawing up
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
throughout the manuscript, which should include the
Review articles and case reports should include an
following sections, each starting on a separate page: title
unstructured summary.
page, abstract and key words, text, acknowledgements,
Key words
references, individual tables and legend for figures. Pages
Te abstract should be followed by a list of 3-10
should be numbered consecutively, beginning with the
keywords or short phrases which will assist the cross-
title page, and the Arabic numbers should be placed in
indexing of the article and which may be published.
the top right hand corner of each page.
When possible, the terms used should be from the
Medical Subject Headings 262 list of Index Medicus
Presentation of papers
Title page
Text
Te title page should carry the full title of the paper
Full papers of an original study may be divided into
and a short title to be used as a short ‘running head’ (and
sections headed Introduction, Methods (including ethical
which should be so identified and should comprise up to
and statistical information), Results and Discussion
45 characters). Te first name, middle initial and last
(including a conclusion). Tis so-called
“IMRAD”
name of each author should appear. If the work is to be
structure is not simply an arbitrary publication format,
attributed to a department or institution, its full name
but rather a direct reflection of the process of scientific
should be included. Any disclaimers should appear on the
discovery. Long articles may require subheadings within
title page, as should the name and address of the author
some sections (especially the Results and Discussion
responsible for correspondence concerning the manuscript
sections) to clarify their content. Other types of articles,
and the name, address and e-mail address of the author to
such as case reports, reviews, and editorials, are likely to
whom requests for reprints should be made (the author
require other formats. Excessive use of abbreviations is
should mention if he does not want his e-mail address to
not recommended. Outline statistical methods used.
be published). Finally, the title page should include the
Identify drugs and chemicals used by generic name (if
sources of any support for the work in the form of grants,
trade-marks are mentioned, manufactured name and
equipment, drugs, or any combination of these.
city should be given).
Abstracts
Acknowledgements
Te second page should carry a structured abstract
Acknowledgements should be made only to those
of no less than 200 words. Do not use abbreviations,
who have made a substantial contribution to the study.
footnotes, or references.
Authors are responsible for obtaining written permission
Background & Aims
from people acknowledged by name in case readers infer
Describe the importance of the study and the
their endorsement of data and conclusions.
precise research objective(s) or study question(s).
References
Methods
References should be numbered consecutively in
Methods should include information on the
the order in which they first appear in the text. Tey
following aspects of study design when applicable:
should be assigned Arabic numerals, which should be
Design - describe the basic study design, e.g. randomized
given in brackets, e.g. [12]. References should include
controlled trial, cross sectional study, cohort study, case
the names of all authors when six or fewer; when seven
series, survey etc; Setting - specify whether the study
or more, list only the first three names and add et al.
was conducted in a primary or tertiary care setting, in
References should also include full title and source
an ambulatory care clinic or hospital, in the general
information. Journal names should be abbreviated as
community etc; Participants - indicate the number of
in Index Medicus
study subjects and how they were selected, recruited,
serials/terms_cond.html). No more than
90-100
and assigned to the intervention; Intervention - report
references will be accepted for reviews. For Letters to
the method of administration and duration of the
the Editor, 5-6 references. Avoid or keep as low as
intervention.
possible the use of abstracts as references. Personal
Results
communications and unpublished work should not
Provide the main outcomes of the study, including
feature in the reference list but should appear in
confidence intervals or p values.
parentheses in the text. Unpublished work accepted
Conclusion
for publication but not yet released should be included
State only conclusions that are directly supported
in the reference list with the words
“in press” in
by the evidence and the implications of the findings.
parentheses beside the name of the journal concerned.
54
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
Guidance for drawing up
a) Article:
in the metric system in terms of the International
[1] Otvos L Jr, Shao WH, Vanniasinghe AS, Amon
System of Units (SI).
MA, Holub MC, Kovalsykz I, et al. Toward understanding
Abbreviations and symbols
the role of leptin and leptin receptor antagonism in
Use only standard abbreviations. Avoid
preclinical models of rheumatoid arthritis. Peptides
abbreviations in the title and abstract. Te full term for
2011;32:1567-74.
which an abbreviation stands should precede its first use
b) Papers published only with DOI numbers:
in the text unless it is a standard unit of measurement.
[2] Chaldakov GN, Beltowsky J, Ghenev PI, Fiore
M, Panayotov P, Rancic G, et al. Adipoparacrinology -
Reprints
vascular periadventitial adipose tissue (tunica adiposa) as
Ten reprints of the published articles and two copies
an example. Cell Biol Int
2011;doi:
10.1042/
of the Journal will be supplied free of charge. If required
CBI20110422.
in a greater number, they will be available on payment
c) Book:
of the necessary cost.
[3] Gertler A, editor. Leptin and Leptin Antagonists.
Landes Bioscience, Austin, Texas, USA. 2009.
Editorial policy
d) Book chapter:
We welcome all contributions in the field of
[4] Jeremy L, Abe PD. Treatment Options in
medicine. We invite known personalities with expertise
Superficial (pTa/pT1/CIS) Bladder Cancer. In: Urological
and many published papers in a specific field to write
cancers in clinical practice, Springer-Verlag, London
reviews and editorials in our journal. We accept original
Limited, 2007:75-102.
papers and case reports from all countries. Te
Tables
Conexiuni Medicale/Medical Connections offers
Each table should be assigned a Roman numeral
thorough peer review and immediate publication on
(e.g. Table III) and a brief title. Explanatory matter
acceptance. Te redactor-in-chief or one of the first
should be placed in footnotes. Explain in footnotes all
reads the manuscripts received and in about 1-3 weeks
non-standard abbreviations that are used in each table.
decide upon their priority level: some are immediately
Identify statistical measures of variations, such as
sent to the reviewers, some are rejected without being
standard deviation and standard error of the mean. Each
sent for review and some are returned to authors with
table should be cited in the text.
suggestions for improvement before submitting them
Illustrations
to reviewers.
All graphs, photographs (on glossy paper), diagrams
will be referred to as figures and should be numbered
Peer-review procedure
consecutively in the text in Arabic numerals. If a figure
Te Conexiuni Medicale/Medical Connections
has been published before, the original source must be
promotes evaluation of all the original papers by two or
acknowledged and written permission from the
three independent reviewers, of whom two are
copyright holder for both print and electronic formats
international personalities. Te peer-review process is
should be submitted with the material. Figures may be
essential for ensuring the quality of the scientific
reduced, cropped or deleted at the discretion of the
information disseminated. Te reviewers are asked to
Editor.
evaluate the manuscript by applying the same standards
Legends for illustrations
as for the international journals. Te reviewers send
Captions should have an Arabic numeral
their comments to the Editor. Te Editor will inform
corresponding to the illustration to which it refers with
the authors about the suggestions made by the referee
a title above and explanatory notes below it. Internal
and ask them to answer the questions and make the
scales should be explained and staining methods for
required corrections. Tis information is provided up to
photomicrographs should be identified.
three months from the date they submitted the paper to
Units of measurement
the journal. Te revised manuscript should be sent in no
Measurements of length, height, weight, and
more than one month to the Editor. When the Editor
volume should be reported in metric units
(meter,
receives the corrected version with all changes marked,
kilogram, or litre) or their decimal multiples.
accompanied by a letter with a point-by-point reply to
Temperatures should be given in degrees Celsius. Blood
the reviewers’ comments, he sends those back to the
pressures should be given in mmHg. All hematological
same reviewer, who makes the final recommendation for
and clinical chemistry measurements should be reported
acceptance or rejection of the manuscript.
55
Guidance for Authors
Guidance for drawing up
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
Notice to subscribers
or inside back cover: Euro 350 1 issue, 1400 4 issues. Full
Te annual subscription rates for 2016: 80 RON
colour page ouside back cover: Euro 400 1 issue, 1600 4
individual, 160 RON institutional. Foreing subscribers:
issues. Bank account: Colegiul Medicilor Satu Mare, CUI
75
$ individual, 150
$ institutional. Additional postage:
9839430, Banca Transilvania, branch Agenţia Golescu
surface mail 20
$, for overseas air mail 40
$. Bank
Satu Mare, IBAN: RO21BTRL03101205K39262XX
account: Colegiul Medicilor Satu Mare, CUI 9839430,
(RON) IBAN: RO62 BTRL 0310 2202 K392 62XX
Banca Transilvania, branch Agenţia Golescu Satu Mare,
(USD) Swift: BTRLRO22.
IBAN: RO38 BTRL 0310 1202 K392 62XX (RON)
IBAN: RO62 BTRL 0310 2202 K392 62XX (USD)
© Copyright Conexiuni Medicale
/ Medical
Swift: BTRLRO22. Orders should be sent to the
Connections, Satu Mare, 2016
Editorial Office, Eroilor Revoluţiei Pl. no.23-440055
No part of this publication may be reproduced,
Satu Mare, Romania. Tel./Fax:
+40-261-710456 or
stored in a retrieval system or transmitted in any form or
+40-361-408164, or by e-mail: colmedsm@gmail.com.
by any means without prior permission in writing of
Conexiuni Medicale
/ Medical Connections.
Notice to advertisers
Permission is not however required to copy abstracts of
Applications for advertisement space and for rates
papers or of articles on condition that a full reference to
should be addressed to the Editorial Office of Conexiuni
the source is shown. Correspondence regarding
Medicale / Medical Connections. 2016 advertising rates
permission to reprint all or part of any article
are Euro 200 full (A4) colour page, 1 issue, and Euro 800
published in this journal should be addressed to the
full colour page, 4 issues. Full colour page on inside front
Editor, e-mail: colmedsm@gmail.com
56
EDITORIAL
PRIVIRE DE ANSAMBLU ASUPRA OPȚIUNILOR DE RECUNOAȘTERE
A MEDICINEI DE FAMILIE/MEDICINEI GENERALE CA SPECIALITATE
MEDICALĂ EUROPEANĂ
Călin Bumbuluț
Editor șef-adjunct, Vicepreședinte UEMO
Glosar de termeni:
informațională care leagă transfrontalier autoritățile
naționale, regionale și locale.
Uniunea Europeană a Medicilor Generaliști/
Medici de Familie (Te European Union of General
Situația actuală
Practitioners/Union Européenne des Médecins
Omnipraticiens/Médecins de Famille - UEMO) a fost
Legislația UE (Directivele 2005/36 și 2013/55) are
fondată în
1967, crescând rapid prin cuprinderea
ca obiectiv asigurarea recunoașterii calificărilor, cu
organizațiilor din toate statele membre care compun
scopul de a facilita libera circulație a profesioniștilor, iar
Uniunea Europeană precum și din țări din Asociația
în cazul medicilor, de a stabili cerințe minime pentru a
Europeană de Liber Schimb și alte țări europene. Din
obține o recunoaștere automată.
1992, UEMO are statutul oficial de parte consultativă,
Legile care reglementează profesia la nivel european
sunt: Directiva 2005/36/CE și Directiva 2013/55/CE.
ENMCA este acronimul pentru Rețeaua Europeană a
În prezent, din 28 de țări, 17 (mai mult de 1/2,
Autorităților Competente Medicale/European Network of
peste 2/5) recunosc specialitatea de MF/MG. Din mai
Medical Competent Authorities. Rețeaua reunește
2016, mai sunt două țări care recunosc specialitatea
Autorități Competente europene responsabile pentru
intern, Olanda notificând CE, dovada calificării formale
recunoașterea calificărilor profesionale medicale, în
fiind „Certificatul de înregistrare în registrul special al
concordanță cu Directiva
36/2005/CE privind
medicilor generaliști; Diploma de specialist în
medicină”, precum și Suedia care a modificat în „Dovada
Autoritățile Competente sunt organismele de
de specialist în medicina generală”.
reglementare cu obligații impuse prin Directiva revizuită
Cel puțin 24 de țări aplică programe de formare
2005/36 / CE (PQD) de recunoaștere reciprocă a calificărilor
specifică pentru MF/MG.
profesionale, care controlează accesul la profesiile
„(…) durata minimă de formare din Anexa V a fost
reglementate, titlurile profesionale și vocaționale, precum și
stabilită în timpul ultimei revizuiri a Directivei din
activitățile profesionale care necesită calificări specifice.
2003, (…) majoritatea statelor membre se regăsesc în
Autoritatea Națională furnizează informații
întervalul de patru până la șase ani pentru formarea
privind recunoașterea calificărilor profesionale în fiecare
specialiștilor pentru toate calificările listate în Anexă.
țară UE și ghidează profesioniștii prin formalitățile
Rezultatele studiului evidențiază că unele state membre
administrative.
permit ca pregătirea specialiștilor să fie considerabil mai
Grupul de Coordonatori pentru recunoașterea
scurtă.
calificărilor profesionale, cu misiunea de a stabili cooperarea
Durata minimă de pregătire definită în Anexa V
între autoritățile Statelor membre și Comisie cu privire la
pare să fie determinată pe baza celui mai scurt punct
chestiuni referitoare la recunoașterea calificărilor profesionale.
național de referință. Armonizarea minimă, de exemplu
Anexa V - lista calificărilor supuse recunoașterii
utilizând cel mai scăzut numitor comun al anilor de
automate. Conține Titlul de calificare, Titlul profesional și
formare ca punct de referință precum în Anexa V, nu
Data de referință (de la care se aplică aceste titluri).
contribuie la încrederea reciprocă necesară pentru
IMI - Sistemul Informațional al Pieței Interne
/
sistemul de recunoaștere automată. Dacă autoritățile
Internal Market Information system este o rețea
competente nu pot verifica conținutul specific al
Overview of Options for the Recognition of Family Medicine / General Medicine as a European Medical Specialty
57
Editorial
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
formării în specialitate, ele vor ca cel puțin să fie sigure
1. Perspectiva unui curriculum/program european
că durata de formare permite un grad de specializare
de formare pentru Medicina Generală, ținând seama de
adecvat; cerem o durată minimă care reflectă mai mult
varietatea existentă azi la nivel național, atât în durată
decât cel mai scăzut numitor comun. Solicităm Comisiei
cât și în conținut.
să ia în considerare această deficiență în munca viitoare
2. Recunoașterea prin mecanismul automat ca
asupra Directivei pentru a cere recunoașterea automată
specialitate și nu ca și calificare.
compatibilă cu nevoile siguranței pacientului”
3. Prevenirea interferenței autorităților politice și
(Documentul de poziție al ENMCA privind durata
administrative în reglementarea Medicinei de Familie
minimă de formare în Anexa V, aprilie 2016).
(de exemplu intenția unor guverne de a înlocui medici
Există patru tipuri (până acum) de reglementări ale
generaliști cu asistente medicale).
Medicinei Generale/Medicinei de Familie în Uniunea
4. Egalitatea cu alte specialități pentru accesul la
Europeană și țările afiliate:
formare și EMC, pentru acreditarea evenimentelor,
- Recunoașterea specialității de Medicină Generală/
dreptul de a fi ales și de a vota în cadrul organizațiilor
Medicină de Familie la nivel național și notificarea
medicale naționale reprezentative și pentru reprezentarea
acestui fapt către CE, cu nominalizare în Anexa 5.1.4.
în Europa.
- Recunoașterea ca și calificare specială a Medicinei
5. Există specialități recunoscute doar în unele țări,
Generale/Medicinei de Familie, la nivel național și
dar ele beneficiază de introducerea în Directiva
36,
notificarea acestui fapt către CE cu nominalizarea în
Anexa
5.1.3 precum Neuropsihiatria, care are
Anexa 5.1.4.
recunoaștere națională doar în
10 țări ale UE, sau
- Recunoașterea ca specialitate a Medicinei
Radiologia în 11 țări ale UE, Medicină de Urgență și
Generale/Medicinei de Familie la nivel național în
Accident în 7, Hematologie biologică în 4, Dermatologie
legislația națională specifică, dar notificarea către CE ca
numai în 3 (!) (cel puțin în 2005, cum este notificat în
și calificare în Anexa 5.1.4.
Directiva 36).
- Unificarea cu o altă specialitate nominalizată în
6. Păstrarea Articolelor 28, 29 și 30 din Directiva
Anexa 5.1.3, sub o nouă nominalizare (de exemplu
2005/36 privind cadrul general de calificare în Medicină
medicină generală internă în Elveția).
Generală, este necesară pentru situațiile în care medicul
Argumente pro și contra pentru recunoașterea
nu a obținut specialitatea, ci doar titlul de calificare.
medicinei de familie ca specialitate
7. Îngrijorările privind creșterea cheltuielilor
Aceasta este o listă de verificare cu privire la
pentru plata medicilor generaliști sunt irelevante în
oportunitățile și beneficiile (sau nu) ale recunoașterii ca
măsura în care medicina de familie beneficiază în toate
specialitate.
țările de o alocare bugetară separată
(Principala
Avantajele sunt:
îngrijorare este presupusa convingere a politicienilor cu
58
Bumbuluț
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
Editorial
privire la creșterea finanțării medicilor de familie ca
Căi de recunoaștere europeană
urmare a recunoașterii ca specialiști).
Întrebarea pentru noi este dacă specialitatea noastră
8. Tendința pentru toate specialitățile din Europa
este „una printre alte specialități”, sau dacă vom alege o
este de a reglementa conținutul de formare și examenul
cale cu totul separată. Mai multă integrare cu alte
european; nu putem sta deoparte de acest proces;
specialități, sau mai multă specificitate?
dezvoltarea Cartei formării (similar cu alte specialități)
Scenarii posibile:
pentru specialitatea noastră este o necesitate.
- coexistența a două regimuri la nivel național, în
9. Forța practicienilor generaliști va crește dacă
15 țări ale UE, ceea ce înseamnă menținerea status quo-
argumentele vor fi discutate la un nivel egal cu alte
ului.
specialități, în fața autorităților politice și administrative.
- modificarea Directivei actuale prin mai multe
Dezavantajele sunt:
etape: eliminarea articolului
28, includerea în Anexa
1. Riscul de a ne pierde individualitatea în oceanul
5.1.3, eliminarea Anexei 5.1.4, includerea în Articolul
de specialități
(mai mult de
50)
(deși
«uniunea în
25 a cerințelor de formare în MG. Trebuie să
diversitate” este deviza UE).
recunoaștem, este cea mai puțin plauzibilă din punct de
2. În cazul în care nu toate țările vor avea
vedere politic, deoarece este necesar ca Parlamentul
specialitatea, se va crea un sistem și mai complex pentru
European să voteze toate acestea și nu este de dorit
migrarea medicilor în UE.
pentru acest moment, pentru că există țări din cele
3. Să nu se piardă sistemul simplu pentru libera
șaptesprezece cu un număr mare de MF fără
circulație a medicilor și a recunoașterii automate.
recunoașterea specialității din diferite motive. Interesul
4. Pericolul de a fi
„asimilat” în interesul altor
nostru este de a menține Articolele 28, 29 și 30. Mai
specialități în relațiile cu autoritățile.
mult decât atât, Directiva abordează toate profesiile
5. Riscul de a realiza că „unii sunt mai egali decât alții”.
reglementate și nu numai medicii, astfel încât angajarea
6. Posibilitatea ca un generalist să fie ales într-o
într-un proces legislativ complet pentru o profesie este
organizație medicală națională sau internațională
nerealistă. Acest lucru ar trebui să fie luat în considerare
reprezentativă, poate fi un avantaj, dar, de asemenea, o
dacă/atunci când Directiva va fi revizuită.
pierdere atunci când trebuie să lupte și pentru altceva
- progresul realizat cu Directiva 2013/55 privind
decât pentru interesul specialității lui.
notificarea Anexei V
(lista
calificărilor supuse
7. Menținerea drepturilor dobândite prin articolul
recunoașterii automate) prin schimbarea procedurilor și
30 și nimic mai mult.
introducerea „actului delegat”. La articolul 26, al doilea
8. Ce durată ar trebui să aibă formarea specifică?
paragraf se înlocuiește cu următorul text: „... Comisia
Care ar trebui să fie conținutul? Ar trebui să-și păstreze
este împuternicită să adopte acte delegate în conformitate
specificitatea? (Articolul 28).
cu Articolul 57c în ceea ce privește includerea în punctul
59
Overview of Options for the Recognition of Family Medicine / General Medicine as a European Medical Specialty
Editorial
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
5.1.3 din Anexa V a noi specializări medicale comune la
„UEMO, organizația medicilor generaliști/medicilor
cel puțin două cincimi din statele membre”.
de familie europeni, solicită recunoașterea medicilor
Calea ideală: solicitare din partea Autorității
generaliști în calitate de specialiști.
Competente prin intermediul IMI către Comisia
Medicina generală reprezintă baza solidă a oricărui
Europeană, prezentând actele cu putere de lege și actele
sistem de sănătate cost-eficient, iar medicii generaliști sunt
administrative adoptate în materia emiterii titlului de
medici instruiți, cu o înaltă calificare vocațională.
calificare ca specialist în medicina de familie, inclusiv
După finalizarea cu succes a studiilor medicale ei au o
informații cu privire la durata și conținutul programelor
perioadă de formare în spital, combinată cu formarea
de formare, în vederea adoptării actului delegat în
specializată pentru practica generală, care implică o
conformitate cu Dir. 2013/55, articolul 57c de către
perioadă de muncă supravegheată în cadrul unei practici
Comisia Europeană, pentru introducerea specialității de
de formare specializată.
Medicină Generală/Medicină de Familie în Anexa V,
Există catedre de Medicină Generală/Medicină de
5.1.3 în conformitate cu articolul 26 din Dir. 2005/36
Familie în Universități și majoritatea țărilor europene
revizuită de către Dir. 2013/55 și articolul 21a, condiția
recunosc specialitatea de Medicină Generală/Medicină de
ca noua specialitate care urmează să fie adoptată să fie
Familie.
recunoscută în cel puțin
2/5 din statele UE fiind
UEMO invită toate țările care nu au recunoscut încă
satisfăcută.
Specialitatea să-și evalueze propriile lor sisteme, astfel încât
Ultimele evoluții
- Declarația UEMO privind
să promoveze și să realizeze recunoașterea generaliștilor/
recunoașterea medicilor generaliști/medicilor de
medicilor de familie ca specialiști în domeniul Medicinei
familie în calitate de specialiști adoptată în
Generale/Medicinei de Familie în decurs de un an.
unanimitate de Adunarea Generală din Porto, la 11
De asemenea UEMO se obligă să urmărească acest
iunie 2016:
obiectiv prin intermediul Comisiei Europene și a viitoarei
Directive din 2017 (anexa V, 5.1.3 și 5.1.4)”.
60
Bumbuluț
ORIGINAL ARTICLE
CARACTERISTICI SOCIO-DEMOGRAFICE ASOCIATE
CU PROBABILITATEA CRESCUTĂ A UNUI DIAGNOSTIC ULTERIOR
DE SCHIZOFRENIE
Virgil Radu Enatescu1, Minodora Manea2, Radu Stefan Romosan1, Ana Maria Draghici3,
Valentin Alexandru Pinzaru1, Cristina Ana Bredicean1, Ion Papava1
1Disciplina de Psihiatrie, Universitatea de Medicină și Farmacie „Victor Babeș”, Timișoara, 2Disciplina de Psihologie
Medicală, Universitatea de Medicină și Farmacie „Iuliu Hațieganu”, ClujNapoca și 3Clinica de Psihiatrie „Eduard
Pamfil”, Timișoara, România
Adresa pentru corespondență:
Virgil-Radu Enatescu
Disciplina de Psihiatrie, Universitatea de Medicină și Farmacie „Victor Babeș”, Timișoara, România,
Timișoara, Str Iancu Văcărescu nr 21, PO 300182
Tel: +40 723374896, Fax: +40 356711617
Email: enatescu.virgil@umft.ro
Primit: 09.05.2016
Acceptat: 28.05.2016
Med Con June 2016 Vol 11, No 2, 61-70
Rezumat
episod de psihoză, au fost asociate cu o probabilitate
crescută de evoluție către un diagnostic de schizofrenie
Introducere: Schizofrenia este cea mai dezabilitantă
la episoadele ulterioare.
tulburare psihică a cărei prognostic clinic și funcțional
Concluzii: Identificarea unui profil socio-
este, cel puțin în parte, condiționat de promptitudinea
demografic inițial asociat cu o probabilitate crescută a
inițierii tratamentului. Deseori, stabilirea diagnosticului
unei evoluții ulterioare spre schizofrenie ar putea crește
de schizofrenie este întârziată la primul episod de
acuratețea identificării acestui diagnostic încă de la
psihoză, fapt ce poate afecta managementul corect a
primul episod de psihoză.
pacientului.
Cuvinte cheie: primul episod de psihoză,
Obiectivul cercetării a fost acela de a identifica
schizofrenie, caracteristici socio-demografice
caracteristicile socio-demografice inițiale, de la primul
episod de psihoză, asociate cu o probabilitate crescută de
Introducere
evoluție către un diagnostic de schizofrenie la episoadele
ulterioare de psihoză.
Psihoza este un concept complex, a cărui
Material și metode: Au fost analizate datele
semnificație poate varia de la un simptom clinic singular
înregistrate în foile de observație a
100 de pacienți
la cel de sindrom clinic constând dintr-un grup de
internați în Clinica de Psihiatrie Eduard Pamfil din
simptome bine delimitate și în cele din urmă la cel de
Timișoara, pentru două episoade psihotice succesive.
tulburare psihică distinctă etichetată în cadrul nosologiei
Prima spitalizare s-a suprapus primului episod de psihoză.
psihiatrice.
Rezultate: Analiza prin regresie logistică binară a
De-a lungul ultimelor decade, cercetarea psihiatrică
evidențiat că vârsta medie
(OR=0,90, 95%IC 0,85-
a evidențiat neechivoc că identificarea și detecția
0,95), statutul profesional
(OR=3,75, 95%IC 1,10-
timpurie a primului episod de psihoză poate fi crucială
12,74) și calitatea suportului social (OR=3,47, 95%IC
pentru evoluția acestui tip de tulburare psihică majoră
1,11-10,82), existente în momentul debutului primului
[1]. Mai mult, acuratețea diagnostică reprezintă o
The Socio-Demographic Characteristics Associated with the Increased Likelihood of Subsequent Schizophrenia
61
ORIGINAL ARTICLE
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
provocare frecventă în practica clinică psihiatrică, în
ianuarie 2010 și ianuarie 2015. Prima internare a fost
special când pacientul se confruntă cu debutul unui
considerată drept primul episod de psihoză.
prim episod de psihoză. Referitor la această problemă,
Criteriile de includere au fost: vârsta cuprinsă între
cercetări anterioare au evidențiat că stabilitatea
18 și 65 de ani la momentul primei spitalizări psihiatrice;
diagnosticului, în special în primii ani ai unei tulburări
prezența a cel puțin două internări consecutive în clinica
psihice de severitate și având caracteristici psihotice, este
noastră pentru două episoade distincte de psihoză,
relativ scăzută, ducând la modificări ale diagnosticului la
ambele fiind încadrabile în unul din diagnosticele
următoarele episoade de psihoză [2,3].
aparținând tulburărilor psihice de spectru schizofren
Cercetările au evidențiat, de asemenea, o tendință
conform cu International Statistical Classification of
constantă de a subdiagnostica schizofrenia la primul ei
Diseases and Related Health Problems 10th Revision
episod [4]. Aceasta se poate datora limitării informației
(ICD-10); existența unei perioade de remisiune distinctă
obținute transversal la primul episod de psihoză, sau
între cele două episoade de cel puțin șase luni de zile
poate fi datorată stigmei crescute, asociată cu această
[13], dar nu mai mult de doi ani de zile; lipsa oricărei
etichetă diagnostică [5,6].
alte tulburări psihice comorbide care ar putea interfera
Identificarea și diagnosticarea corectă a schizofreniei
cu interpretarea rezultatelor și existența tuturor datelor
începând cu primul episod de boală, ar putea îmbunătăți
în foile de observație selectate. S-au luat în considerare
strategia terapeutică a pacientului printr-un mai bun
următoarele
diagnostice
psihiatrice
atribuibile
management a cazului, o implicare activă a familiei și
tulburărilor psihice de spectru schizofren, conform
prin stabilirea unui plan complex de recuperare care ia
ICD-10: tulburări psihotice acute și tranzitorii de orice
în considerare, pe lângă remisiunea clinică, obținerea
tip, schizofrenia de orice tip, tulburare delirantă
remisiunii funcționale și a recuperării [7].
persistentă de orice tip și tulburări schizoafective de
Până acum, obiectivul a numeroase cercetări a fost
orice tip. Psihozele organice și psihozele schizofrenia-
acela de a identifica acei markeri biologici, clinici și
like induse de uzul de substanțe sau de o boală medicală
neuroimagistici care ar putea avea un impact semnificativ
generală au fost excluse, întrucât au fost considerate ca
asupra acurateței diagnosticului de schizofrenie încă de
irelevante scopului cercetării actuale. În cercetare nu au
la primul ei episod, ducând astfel la creșterea validității
existat pacienți eligibili cu un diagnostic de tulburare
diagnostice [8-10].
schizotipală sau de tulburare delirantă indusă.
Dat fiind consensul referitor la consecințele negative
Din cei 147 de pacienți eligibili, 33 au fost excluși
notabile a întârzierii diagnosticului de schizofrenie,
deoarece s-au prezentat cu un alt diagnostic decât cel de
considerăm că identificarea caracteristicilor socio-
psihoză din spectru schizofren la cea de a doua internare
demografice care ar putea integra mai bine profilul
(de exemplu, un diagnostic de episod afectiv cu
premorbid a acelor pacienți care se află la un risc crescut
simptome psihotice), iar în situația a 14 pacienți nu s-au
de schizofrenie, ar fi valoroasă în practica clinică pentru
putut obține toate informațiile necesare pentru cercetare.
creșterea în timp util a acurateței diagnostice, chiar de la
În cele din urmă, un număr total de 100 de pacienți au
primul episod de psihoză.
fost analizați.
Scopul studiului nostru este identificarea
Studiul de față a fost realizat în acord cu cerințele
caracteristicilor socio-demografice inițiale ale pacienților
Declarației de la Helsinki, a Ghidurilor Europene de
la primul episod de psihoză încadrabil în una din
Bună Practică și cu cele ale autorităților și comitetelor
tulburările psihice de spectru schizofren, conform ICD-
de etică naționale și regionale.
10 [11,12], care se asociază cu o probabilitate crescută
Metode
de evoluție ulterioară spre un diagnostic ICD-10 de
Toate datele socio-demografice au fost colectate și
schizofrenie la cel de-al doilea episod de psihoză la
procesate în același mod în cadrul unei fișe electronice.
același pacient.
S-au analizat următoarele variabile socio-demografice
inițiale asociate cu primul episod de psihoză: vârsta la
Material și metode
debutul episodului, sexul, nivelul instructiv, statutul
profesional, statutul marital, mediul de rezidență și
Participanții și planul cercetării
calitatea suportului social. Statutul profesional de
Am realizat un studiu retrospectiv longitudinal
pensionar de boală nu a fost datorat vreunei boli psihice,
asupra datelor conținute în foile de observație clinică a
ci unei afecțiuni medicale, dar care nu a putut fi legată
100 de pacienți internați de două ori în Clinica de
cauzal de apariția primul episod de psihoză (de exemplu,
Psihiatrie Eduard Pamfil din Timișoara, pentru două
boli cardiovasculare). De câte ori a fost necesar, au fost
episoade distincte și consecutive de psihoză, în perioada
obținute date suplimentare de la psihiatrii curanți
62
Enatescu et al
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
ORIGINAL ARTICLE
precum și din conținutul unor documente medicale
prezentate în Tabelul I, în funcție de diagnosticul
anexate foilor de observație clinică.
psihiatric stabilit la a doua internare în secția de
Analiza datelor
psihiatrie pentru un episod consecutiv de psihoză.
În scopul analizei datelor a fost utilizat SPSS versiunea
În ceea ce privește vârsta medie de debut pentru
17 pentru Windows. Testul chi-pătrat a fost utilizat
întreg eșantionul studiat, în funcție de diagnosticul
pentru a compara frecvențele variabilelor categoriale, iar
stabilit la al doilea episod de psihoză, am constatat
testul t parametric pentru eșantioane independent a fost
diferențe semnificative, după cum urmează: diagnosticul
utilizat pentru a compara mediile variabilelor continue.
de tulburare schizoafectivă a avut cea mai mică vârstă
Testele de rang non parametrice (testul U Mann-Whitney
medie la debut, în comparație cu pacienții cu tulburări
și testul H Kruskal-Wallis) au fost utilizate pentru a
delirante persistente
(Kruskal-Wallis test; H=35,796,
analiza variabilele ordinale. La fel, datorită distribuției
p<0,001). Subiecții cu un diagnostic de schizofrenie au
anormale a variabilelor reprezentate de vârsta la primul
avut o vârstă medie de debut ușor mai mare decât
episod de psihoză, am ales teste de rang non-parametric
pacienții cu tulburare schizoafectivă, în timp ce subiecții
pentru a analiza diferența dintre subgrupe distincte de
cu un diagnostic stabil de tulburări psihotice acute și
diagnostic. Corelațiile Spearman Rho au fost determinate
tranzitorii la ambele episoade au avut o vârstă medie de
în cazul variabilelor dependente ordinale, în timp ce
debut intermediară. Mai mult decât atât, în funcție de
corelația Pearson a fost utilizată pentru variabile continue.
distribuția genului la al doilea episod de psihoză, când
Testul de omogenitate marginală a fost utilizat pentru a
am comparat vârsta medie de debut a primului episod
evalua stabilitatea diagnosticului psihiatric la al doilea
psihotic la pacienții cu schizofrenie, subiecții de gen
episod de psihoză în comparație cu primul episod.
masculin au avut o vârstă medie mai mică la debut decât
Pentru a evalua valoarea potențială a factorilor socio-
subiecții de gen feminin, cu toate că diferența nu a fost
demografici de la primul episod de psihoză, dar și pentru
semnificativă din punct de vedere statistic
(Mann
predicția unei probabilități crescute de diagnostic de
Whitney U test; U=119.000, Z=-1,363, p=0,181).
schizofrenie în cazul celui de-al doilea episod de psihoză
Distribuția pe gen în cele patru subloturi, în funcție
(luat ca variabilă dependentă binară,
1 a reprezentat
de diagnosticul la al doilea episod de psihoză, a arătat
prezența schizofreniei, iar
0 absența ei, prin urmare
rezultate interesante. În cazul pacienților cu schizofrenie,
prezența unui alt diagnostic de spectru schizofren), am
precum și a celor cu tulburare psihotică acută și
aplicat regresia logistică binară, metoda ENTER, valoarea
tranzitorie, distribuția în funcție de gen a fost egală sau
alfa fiind
0.05. În cadrul procesului statistic, locul de
aproape egală. În mod diferit, pentru pacienții care au
rezidență a fost exclus din analiză, deoarece s-a considerat
fost diagnosticați cu tulburare delirantă persistentă și
a fi mai puțin relevant în cadrul obiectivelor propuse.
tulburare schizoafectivă a predominat genul feminin.
Pentru a facilita analiza statistică, unele variabile
Aceste diferențe nu au avut semnificație statistică
independente au fost regrupate în două categorii
(X2=5,257, p=0,154).
principale: statutul profesional a fost regrupat în persoane
Mediul de proveniență, indiferent dacă urban sau
cu ocupație (a inclus subiecții care aveau statut de angajat
rural, a prezentat o distribuție ușor diferită în funcție de
sau erau studenți la primul episod de psihoză) și persoane
diagnosticul la al doilea episod de psihoză. Repartiția pe
fără ocupație (a inclus subiecții care nu erau angajați sau
bază de rezidență a arătat ca subiecții cu schizofrenie și
erau pensionari din diferite cauze); statutul marital a fost
tulburare schizoafectivă au locuit în zonele urbane și
restructurat în două grupuri, cu partener (căsătoriți sau în
rurale deopotrivă, procentul fiind ușor mai mare pentru
relație de concubinaj) și fără partener (singuri, divorțați,
mediu urban. Pe de altă parte, subiecții cu tulburări
sau fără relație în prezent) și în cele din urmă, suportul
delirante persistente și tulburări psihotice acute și
social a fost reorganizat astfel: persoane cu sprijin social
tranzitorii au locuit mai ales în mediul urban, dar fără
satisfăcător și cu sprijin social nesatisfăcător (cele lipsite
semnificație statistică (X2=3,839, p=0,279).
de suport social au fost incluse la cele cu suport inadecvat).
Pornind de la considerentul că pacienții care au
absolvit cel puțin studiile liceale au prezentat un nivel
Rezultate
mai ridicat de educație în comparație cu ceilalți, s-a
observat că procentul celor care au fost diagnosticați cu
Caracteristicile socio-demografice de la primul
schizofrenie la al doilea episod de psihozăa fost mai mic
episod de psihoză în raport cu diagnosticul psihiatric
comparativ cu cei care au fost diagnosticați cu tulburări
stabilit la al doilea episod de psihoză
psihotice acute și tranzitorii, tulburări delirante și
Caracteristicile socio-demografice ale eșantionului
tulburări schizoafective. Diferențele între nivelul de
studiat înregistrate la primul episod de psihoză sunt
școlarizare în funcție de diagnosticele psihiatrice de la al
63
The Socio-Demographic Characteristics Associated with the Increased Likelihood of Subsequent Schizophrenia
ORIGINAL ARTICLE
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
Tabel I. Caracteristicele socio-demografice ale eșantionului studiat în funcție de diagnosticul psihiatric
stabilit la al doilea episod de psihoză
Parametrii socio-demografici asociați
Schizofrenia
Tulburarea
Tulburarea
Tulburarea
cu primul episod de psihoză
de orice tip
psihotică acută
delirantă
schizoafectivă
(n=36)
și tranzitorie de
persistentă de
de orice tip
orice tip (n=21)
orice tip (n=36)
(n=7)
Media vârstei de debut (ani )
31,8 (9,914)
35,4 (11,097)
48,8 (10,901)
29,4 (7,323)
Distribuția în funcție de gen
Gen feminin
18 (50,0%)
12 (57,1%)
27 (75,0%)
5 (71,4%)
Gen masculin
18 (50,0%)
9 (42,9%)
9 (25,0%)
2 (28,6%)
Mediu de proveniență
Mediu Urban
21 (58,3%)
17 (81,0%)
26 (72,2%)
4 (57,1%)
Mediu Rural
15 (41,7%)
4 (19,0%)
10 (27,8%)
3 (42,9%)
Nivel educațional
Gimnaziu
20 (55,6%)
8 (38,1%)
19 (52,8%)
3 (42,9%)
Liceu
13 (36,1%)
8 (38,1%)
11 (30,6%)
2 (28,6%)
Facultate
3 (8,3%)
5 (23,8%)
6 (16,7%)
2 (28,6%)
Statut profesional
Neangajat
26 (72,2%)
13 (61,9%)
16 (44,4%)
4 (57,1%)
Angajat
1 (2,8%)
6 (28,6%)
11 (30,6%)
3 (42,9%)
Student
4 (11,1%)
0 (0,0%)
0 (0,0%)
0 (0,0%)
Pensionar
5 (13,9%)
2 (9,5%)
9 (25,0%)
0 (0,0%)
Statut marital
Căsătorit / concubinaj
9 (25,0%)
5 (23,8%)
21 (58,3%)
2 (28,6%)
Celibatar
27 (75,0%)
16 (76,2%)
15 (41,7%)
5 (71,4%)
Văduv
0 (0,0%)
0 (0,0%)
0 (0,0%)
0 (0,0%)
Calitatea suportului social
Fără suport social
5 (13,9%)
1 (4,8%)
2 (5,6%)
2 (28,6%)
Suport social nesatisfăcător
14 (38,9%)
9 (42,9%)
8 (22,2%)
0 (0,0%)
Suport social adecvat
17 (47,2%)
11 (52,4%)
26 (72,2%)
5 (71,4%)
Prezența consumului de tutun în anul
anterior primului episod de psihoză PEP
a
15 (41,7%)
9 (42,9%)
11 (30,6%)
4 (57,1%)
Prezența consumului de alcool în anul
12 (33,3%)
7 (33,3%)
12 (33,3%)
5 (71,4%)
anterior primului episod de psihoză PEPa
Vârsta este indicată prin medie (SD)
aPEP - primul epiosd de psihoză
doilea episod de psihoză nu sunt semnificative statistic
pacienții care au fost diagnosticați cu tulburări delirante
(Kruskal-Wallis test; H=2,808, p=0,422).
persistente, în comparație cu cei care au avut
Atunci când am comparat procentul cumulat de
schizofrenie la al doilea episod de psihoză. Pentru
pacienți care au fost șomeri și pensionari, astfel având
pacienții cu tulburări psihotice acute și tranzitorii și
un statut profesional nesatisfăcător, am observat că
tulburare schizoafectivă, rezultatele au fost destul de
acesta a fost mai mare pentru pacienții care au evoluat
asemănătoare cu cele ale pacienților cu schizofrenie.
spre un diagnostic de schizofrenie, în comparație cu
Diferențele legate de calitatea statutului marital relevate
pacienții care au evoluat către celelalte categorii de
de cercetarea noastră au fost semnificative din punct de
diagnostic la al doilea episod de psihoză, cu diferențe
vedere statistic
între
diagnosticele psihiatrice
semnificative statistic între diagnosticele psihiatrice care
(X2=11,033, p=0,012).
au fost luate în considerare în cercetarea noastră
Dacă luăm în considerare existența unui sprijin
(X2=22,521, p=0,007).
social adecvat, subiecții care au evoluat spre schizofrenie
În ceea ce privește statutul marital, rezultatele
la al doilea episod de psihoză, au avut cel mai mic
noastre au arătat că statutul marital la primul episod
procent de sprijin începând cu debutul afecțiunii,
psihotic a fost mai favorabil, ceea ce înseamnă că
comparativ cu pacienții cu tulburări psihotice acute și
subiecții erau căsătoriți sau într-o relație stabilă, pentru
tranzitorii, tulburări delirante persistente și tulburări
64
Enatescu et al
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
ORIGINAL ARTICLE
Tabel II. Regresie logistică binomială pentru probabilitatea unui diagnostic ulterior de schizofrenie
pe baza unor parametri socio-demografici asociați primului episod de psihoză
Parametrii socio-demografici
B
SE
Wald
df
p
Odds
95% CI for Odds
asociați cu primul episod
Ratio
Ratios
de psihoză
Lower Upper
Vârstă debut
-0,101
0,027
13,753
1
0,000
0,904
0,858
0,954
Gen
0,532
0,562
0,896
1
0,344
1,702
0,566
5,123
Nivel educațional
-0,463
0,350
1,752
1
0,186
0,629
0,317
1,249
Statut profesional la primul episod de
1,322
0,624
4,495
1
0,034
3,752
1,105
12,741
psihoză (fără ocupație)
Statut marital la primul episod de
-0,957
0,735
1,699
1
0,192
0,384
0,091
1,620
psihoză (fără partener)
Suport social înainte de primul episod
1,244
0,580
4,598
1
0,032
3,471
1,113
10,823
de psihoză (nesatisfăcător)
Constanta
3,179
1,619
3,855
1
0,050
24,028
Notă: Genul se referă la bărbați comparativ cu femei
schizoafective. Cu toate acestea, nu au fost diferențe
nesatisfăcător la primul episod de psihoză au avut un
semnificative statistic (X2=11,238, p=0,081).
risc de a evolua spre un diagnostic de schizofrenie de trei
Interesant, pacienții cu un diagnostic de tulburare
ori și jumătate în comparație cu omologii lor (OR=3,47,
schizoafectivă, la al doilea episod de psihoză, au raportat
95% CI 1,11-10,82).
că au fumat mai des în anul care a precedat debutul
primului episod psihotic decât subiecții cu alte
Distribuția în funcție de diagnostic conform
diagnostice, dar acest rezultat nu a atins pragul de
ICD-10 și stabilitatea pe termen scurt a
semnificație statistică (X2=1,041, p=0,307).
diagnosticului la al doilea episod de psihoză în
De asemenea, consumul de alcool în anul care a
comparație cu primul episod de psihoză
precedat debutul psihozei a fost semnificativ mai
Procentul distribuției diagnosticului psihiatric la
frecvent raportat de către pacienții cu tulburare
primul episod de psihoză și stabilitatea acestui diagnostic
schizoafectivă, comparativ cu frecvența consumului de
la al doilea episod de psihoză a prezentat un patern de
alcool, raportată de către restul eșantionului (X2=4,101,
evoluție foarte dinamic (Figura 1).
p=0,043).
S-a observat că a existat o reținere evidentă,
manifestată de către psihiatri în punerea diagnosticului
Parametrii socio-demografici inițiali de la primul
de schizofrenie (18%) la primul episod de psihoză, cei
episod de psihoză asociați cu un risc crescut
mai mulți dintre ei preferând în schimb diagnosticul de
pentru un diagnostic de schizofrenie la al doilea
tulburare psihotică acută și tranzitorie de orice tip
episod de psihoză
(78%). Așa cum era de așteptat, cu privire la primul
În ceea ce privește valoarea predictivă a variabilelor
episod de psihoză, un diagnostic de tulburare delirantă
socio-demografice de la primul episod de psihoză, care
persistentă a fost extrem de rar (în studiul nostru, nu a
sunt asociate cu o probabilitate crescută de a evolua spre
existat niciun caz), urmat imediat de tulburare
diagnosticul de schizofrenie la un episod ulterior de
schizoafectivă (4%).
psihoză, am obținut rezultate foarte interesante și
Chiar dacă schizofrenia și tulburarea schizoafectivă
semnificative (Tabel II).
au fost cel mai probabil subdiagnosticate la primul
Astfel, regresia logistică binară a arătat că o vârstă
episod de psihoză, aceste două diagnostice au rămas
mai înaintată la debutul primului episod de psihoză este
stabile la al doilea episod de psihoză (o rată de consistență
asociată cu un risc scăzut de evoluție spre schizofrenie la
de 100% pentru ambele diagnostice). Pentru a analiza
al doilea episod psihotic (OR=0,90, 95% CI 0,85-0,95).
stabilitatea diagnosticului pentru întregul eșantion
Un statut profesional nefavorabil (cum ar fi șomajul) la
studiat între cele două episoade consecutive de psihoză,
primul episod de psihoză a fost asociat cu o creștere de
am efectuat testul de omogenitate marginală, care a
aproape 4 ori mai mare a probabilității unui diagnostic
relevat o diferență semnificativă
(p<0,001) între
de schizofrenie la cel de-al doilea episod psihotic
diagnosticul de la primul episod în comparație cu
(OR=3,75,
95% CI
1,10-12,74). O constatare
distribuția lor ulterioară. Această diferență semnificativă
interesantă este faptul că subiecții cu suport social
este vizibilă din cauza instabilității ridicate a
65
The Socio-Demographic Characteristics Associated with the Increased Likelihood of Subsequent Schizophrenia
ORIGINAL ARTICLE
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
Figura 1. Stabilitatea diagnosticului pshiatric între primul
și al doilea episod de psihoză
diagnosticului de tulburare psihotică acută și tranzitorie,
Legat de aspectul nostru cultural, trebuie să ne
a cărei frecvență a scăzut dramatic (mai mult de 50%) la
întrebăm dacă stigmatizarea asociată cu diagnosticul de
al doilea episod de psihoză.
schizofrenie a contribuit la reținerea demonstrată de către
medicul psihiatru în punerea acestui diagnostic de la
Discuții
primul episod de psihoză, preferând în schimb să-l
încadreze ca tulburare psihotică acută, chiar dacă este
În ciuda duratei de timp relativ scurtă care a fost
vorba despre diagnostice cum ar fi tulburări psihotice
luată în considerare între cele două episoade psihotice,
acute și tranzitorii cu elemente de schizofrenie sau
cercetarea noastră a relevat o instabilitate crescută a
schizofrenia-like. Se pune problema dacă, începând cu
diagnosticului psihiatric. Lipsa stabilității diagnosticului
primul episod de psihoză, diagnosticul excesiv de tulburări
psihiatric, între primul și al doilea episod psihotic, se
psihotice acute, în loc de cel de schizofrenie, nu ar genera
datorează în principal instabilității diagnosticului de
mai multe dezavantaje pentru pacient, probleme de
tulburare psihotică acută și tranzitorie, care frecvent
management a familiei, precum și pentru stabilirea
evoluează spre alte categorii de diagnostic, mai ales spre
strategiei terapeutice pe termen lung. Pe de o parte, a
cel de schizofrenie. Acest aspect a fost reflectat și de
existat un studiu care a relevat caracteristicile clinice
rezultatele altor studii internaționale, ridicând
importante, ce fac diferența între aceste două tulburări
întrebarea cât de bine este definit acest diagnostic
psihice. Astfel, în cazul schizofreniei, prognosticul pe
psihiatric acut și dacă acesta este doar un diagnostic de
termen lung al tulburării este fără îndoială mai rezervat
tranziție, fiind schimbat în cele din urmă cu un
decât pentru pacienții cu tulburări psihotice acute și
diagnostic de schizofrenie sau alte tulburări psihice
tranzitorii [18]. Pe de altă parte, din punct de vedere etic,
majore de intensitate psihotică [14-17]. Pornind de la
trebuie să remarcăm că în conformitate cu politica noastră
principiul îngrijirii medicale continue pe care sistemul
de sănătate la nivel național, protocoalele terapeutice sunt
nostru de sănătate mintală o prevede, trebuie să
mult mai restrictive în ceea ce privește antipsihoticele
menționăm că, în cercetarea noastră,
98% dintre
atipice de nouă generație, inclusiv formele lor injectabile
pacienți au fost tratați în timpul ambelor internări în
cu acțiune prelungită, care nu au voie să fie prescrise
spital de același medic psihiatru și doar 2% din cazuri
pentru alte tipuri de tulburări din spectrul schizofreniei
au fost tratate de către psihiatri diferiți. În consecință,
decât pentru schizofrenie.
nu putem să atribuim acest rezultat unei lipse de
Tulburarea schizoafectivă este mai puțin frecventă
fidelitate diagnostică între evaluatori sau diagnosticieni
decât schizofrenia (mai puțin de jumătate) [19,20], dar,
diferiți. Totodată, se ridică problema acurateței
în studiul nostru, rata a fost de 1:5, ceea ce indică fie că
informațiilor obținute de către medicul psihiatru la
tulburarea schizoafectivă este subdiagnosticată la primul
primul episod de psihoză în ceea ce privește momentul
episod de psihoză în spitalul nostru, fie este o consecință
de debut al simptomelor psihotice. Criteriul de timp de
directă a planului nostru de studiu în care selectarea
o lună este absolut important pentru ambele diagnostice
eșantionului s-a realizat pe baza unor criterii de includere
menționate mai sus.
restrictive.
66
Enatescu et al
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
ORIGINAL ARTICLE
Studiul a relevat o evoluție interesantă în ceea ce
[32,33]. Astfel, performanța slabă academică a
privește tulburările delirante persistente între cele două
pacienților cu schizofrenie indică faptul că un deficit
episoade de psihoză. În cazul în care acest diagnostic a
cognitiv există într-adevăr și de multe ori precede
fost practic absent la primul episod de psihoză, apare
debutul tulburării cu un număr de ani [34,35]. Pe de
aproape la aceeași frecvență cu schizofrenia la al doilea
altă parte, deficitul cognitiv, măsurat prin performanța
episod, făcându-l un diagnostic preferat sau chiar supra-
slabă academică reprezintă un element clinic important
diagnosticat în clinica noastră [21,22].
pentru diferențierea schizofreniei de tulburarea delirantă
Preferința pentru un diagnostic de tulburare
persistentă. Atunci când un pacient se confruntă cu
delirantă persistentă față de cel de schizofrenie ar putea
tulburări cognitive, un diagnostic de schizofrenie devine
fi, de asemenea, cauzată de stigmatizarea mai redusă în
mai valid [29,36].
cultura noastră asociată cu acest diagnostic. Un alt
Referitor la statutul marital, am constatat că
motiv pentru acest lucru poate fi faptul că, în procesul
pacienții cu tulburare delirantă persistentă au avut un
de diagnosticare la al doilea episod de psihoză, decizia
statut marital mai favorabil în comparație cu celelalte
medicul psihiatru curant a fost influențată de prejudecata
trei tulburări psihotice, fapt care se reflectă și în alte
că schizofrenia poate apărea numai la o vârstă mai
studii [29]. Devine evident că pacienții cu schizofrenie,
tânără, fără însă a ține cont de natura bizară a delirului și
tulburare psihotică acută și tranzitorie și tulburare
de prezența constantă a halucinațiilor. Acest lucru ar
schizoafectivă au o funcționalitate socială premorbidă
putea explica supradiagnosticarea tulburării delirante
mai scăzută, în comparație cu pacienții cu tulburări
persistente față de schizofrenie în contextul nostru.
delirante persistente. Acest lucru poate fi atribuit în
Referitor la vârsta medie de debut a subiecților s-au
mare parte vârstei tinere de debut pentru pacienții cu
constatat diferențe semnificative în ceea ce privește
aceste diagnostice comparativ cu tulburarea delirantă
diagnosticul psihiatric de la al doilea episod de psihoză,
persistentă, atunci când ar fi fost prea devreme pentru ca
aceste diferențe fiind în concordanță cu studii similare și
pacienții să formeze o familie [26].
cu cercetările epidemiologice [23-26]. Dintre acestea,
Similar cu alte cercetări, un statut profesional mai
pacienții schizoafectivi au avut cea mai mică vârstă
scăzut este asociat cu schizofrenia la al doilea episod
medie la debut, dar nu în mod semnificativ diferit de cei
psihotic, urmat de pacienți cu psihoză acută și pacienți
cu schizofrenie. Și alte studii au confirmat, de asemenea,
schizoafectivi. Pacienții cu tulburare delirantă persistentă
că subiecții cu tulburări delirante persistente au avut cea
au avut o mai bună funcționalitate premorbidă în sfera
mai mare vârstă de debut, care este statistic diferită de
profesională [26,27,29]. Acest lucru ar trebui să tragă
celelalte diagnostice din cercetarea noastră
[23,25].
un semnal de alarmă în ceea ce privește necesitatea unei
Vârsta medie de debut în cadrul cercetării noastre a fost
abordări terapeutice mai complexe, în special pentru
similară cu cea din alte studii [24,27], chiar dacă au
pacienții cu tulburări din spectrul schizofreniei. Pentru
existat și studii care au evidențiat o vârsta medie
susținerea tratamentului farmacologic, trebuie să se facă
semnificativ mai mică la debut [26]. Acest lucru poate fi
uz și de reabilitare cognitivă și profesională, cu scopul de
explicat parțial prin decalajul de timp dintre punerea
a obține o recuperare mai bună [37,38].
diagnosticului și durata psihozei netratate, singurele
Calitatea suportului social a fost frecvent
excepții fiind pacienți cu psihoza acută și tranzitorie,
nesatisfăcătoare pentru pacienții cu schizofrenie, ceea ce
situație în care criteriul de timp de o lună este esențial
arată că acest diagnostic special implică un nivel ridicat
pentru stabilirea diagnosticului [28]. A existat un studiu
al deficitului cognitiv, cât și social, care afectează
care a demonstrat o întârziere de 3,5±4,3 ani de la debut
pacientul începând cu câțiva ani înainte de debut
până la prima internare la psihiatrie pentru pacienții cu
[34,39]. Acest rezultat reconfirmă necesitatea
tulburare delirantă persistentă [29].
intervențiilor psihosociale, în special la pacienții cu
Distribuția în funcție de gen în eșantionul nostru a
schizofrenie, care în conformitate cu studiile recente ar
fost similară cu alte studii care au arătat că schizofrenia
putea duce la creșterea cogniției sociale [40]. Mai mult
are un raport aproximativ egal între genul feminin/
decât atât, lipsa suportului social și familial pentru
masculin, cu o ușoară creștere a genului masculin și o
pacienții cu schizofrenie reflectă transmiterea genetică a
prezență mai mare în rândul genului feminin pentru
acestei tulburări în cazul rudelor de gradul I [41].
celelalte diagnostice considerate în cercetarea noastră
În studiul nostru, consumul de tutun și alcool nu a
[26,29-31].
prezentat diferențe semnificative statistic pentru
Nivelul educațional al subiecților care au evoluat
pacienții cu schizofrenie, comparativ cu celelalte trei
spre schizofrenie a fost mai scăzut în perioada
categorii de diagnostic, rezultat comparabil cu un studiu
premorbidă comparativ cu celelalte diagnostice studiate
anterior [33]. Totuși, dintre toate tulburările din spectrul
67
The Socio-Demographic Characteristics Associated with the Increased Likelihood of Subsequent Schizophrenia
ORIGINAL ARTICLE
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
schizofreniei analizate, pacienții schizoafectivi au
8.
Burton CZ, Vella L, Harvey PD, Patterson TL,
raportat mai frecvent utilizarea premorbidă de alcool și
Heaton RK, Twamley EW. Factor structure of the
tutun. Aceste comportamente particulare pot fi legate
MATRICS Consensus Cognitive Battery (MCCB) in
de componenta hedonică a tulburării.
schizophrenia. Schizophr Res 2013;146(1-3):244-8.
În cele din urmă, cercetarea a evidențiat că, toate
9.
Chung Y, Cannon TD.Brain imaging during the
variabilele socio-demografice asociate cu primul episod
transition from psychosis prodrome to schizophrenia. J
de psihoză, precum vârsta mai mică de debut, statutul
NervMent Dis. 2015;203(5):336-41.
profesional nesatisfăcător și suportul social mai scăzut,
10.
Xu K, Schadt EE, Pollard KS, Roussos P, Dudley JT.
ar putea avea o valoare predictivă pentru un viitor
Genomic and network patterns of schizophrenia genetic
diagnostic de schizofrenie. Indiferent de diagnosticul de
variation in human evolutionary accelerated regions.
la primul episod de psihoză, acești trei factori socio-
MolBiolEvol. 2015;32(5):1148-60.
demografici împreună indică o probabilitate semnificativ
11.
World Health Organization.
1992. ICD-10
mai mare pentru ca un pacient să evolueze spre un
classifications of mental and behavioural disorder:
diagnostic de schizofrenie la un episod ulterior de
Clinical descriptions and diagnostic guidelines. Geneva:
psihoză [33]. Mai mult, acești pacienți s-ar putea integra
World Health Organization.
mai bine în profilul socio-demografic premorbid al
12.
Ritsner MS, Gottesman II. 2011. Te schizophrenia
persoanelor cu risc crescut de a dezvolta schizofrenie,
construct after 100 years of challenges. In: Handbook of
odată ce a avut loc primul episod de psihoză.
Schizophrenia Spectrum Disorders. Ritsner MS, editor.
Conflicte de interes
Vol 1. Heidelberg, Germany: Springer, pp 1-44.
Autorii nu au de raportat nici un conflict de interes cu
13.
Andreasen NC, Carpenter WT Jr, Kane JM, Lasser
privire la acest studiu.
RA, Marder SR, Weinberger DR. Remission in
Schizophrenia: Proposed Criteria and Rationale for
Consensus. Am J Psychiatry. 2005;162:441-9.
Referințe
14.
Aadamsoo K, Saluveer E, Küünarpuu H, Vasar V,
Maron E. Diagnostic stability over 2 years in patients
1.
McGorry PD. Early intervention in psychosis: obvious,
with acute and transient psychotic disorders. Nord J
effective, overdue. J NervMent Dis. 2015;203(5):310-
Psychiatry. 2011;65(6):381-8.
318.
15.
Farooq S. Is acute and transient psychotic disorder
2.
Schwartz JE, Fenning S, Tanenberg-Karant M, et al.
(ATPD) mini schizophrenia? Te evidence from
Congruence of diagnoses 2 years after a first admission
phenomenology and epidemiology. PsychiatrDanub.
diagnosis of psychosis. Arch Gen Psychiatry.
2012;24(Suppl 3):S311-5.
2000;57:593-600.
16.
Castagnini A, Foldager L, Bertelsen A. Long-term
3.
Subramaniam M, Pek E, Verma S, Chan YH, Chong
stability of acute and transient psychotic disorders. Aust
SA. Diagnostic stability 2 years after treatment initiation
N Z J Psychiatry. 2013;47(1):59-64.
in the early psychosis intervention programme in
17.
Queirazza F, Semple DM, Lawrie SM. Transition to
Singapore. Aust N Z J Psychiatry. 2007;41(6):495-500.
schizophrenia in acute and transient psychotic disorders.
4.
Veen ND, Selten JP, Schols D, et al. Diagnostic
Br J Psychiatry. 2014;204:299-305.
stability in a Dutch psychosis incidence cohort. Br
18.
Pillmann F, MarnerosA. Longitudinal follow-up in
Journal Psychiatry. 2004;185:460-4.
acute and transient psychotic disorders and schizophrenia.
5.
Pini S, de Queiroz V, Dell’Osso L, et al. Cross-sectional
Br J Psychiatry. 2005;187:286-7.
similarities and differences between schizophrenia,
19.
Perala J, Suvisaari J, Saarni SI, et al. Lifetime prevalence
schizoaffective disorder and mania or mixed mania with
of psychotic and bipolar I disorders in a general
mood-incongruent psychotic features. Eur Psychiatry.
population. Arch Gen Psychiatry. 2007;64:19-28.
2004;19(1):8-14.
20.
Olfson M, Marcus SC, Wan GJ. Treatment patterns
6.
Wood L, Birtel M, Alsawy S, Pyle M, Morrison A.
for schizoaffective disorder and schizophrenia among
Public perceptions of stigma towards people with
Medicaid patients. Psychiatr Serv. 2009;60:210-6.
schizophrenia, depression, and anxiety. Psychiatry Res.
21.
Crowe R R. & Roy MA. 2008. Delusional disorders.
2014;220(1-2):604-8.
In Te Medical Basis of Psychiatry. S. H. Fatemi& P. J.
7.
Henry LP, Amminger GP, Harris MG, et al.Te
Clayton (Eds.) New York, USA: Humana Press, pp
EPPIC follow-up study of first-episode psychosis: longer-
125-31.
term clinical and functional outcome 7 years after index
22.
SoykaM, Zingg C, BaumgärtnerG. Prevalence of
admission. J Clin Psychiatry. 2010;71(6):716-28.
delusional disorder among psychiatric inpatients: data
68
Enatescu et al
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
ORIGINAL ARTICLE
from the German hospital register. Neuropsychiatry.
onset, and sex on the course of schizophrenia. Psychiatry
2011;4:319-23.
Res. 2009;168(1):11-7.
23.
Marneros A, Pillmann F, Wustmann T. Delusional
33.
Ramirez N, Arranz B, Salavert J, et al. Predictors of
disorders--are they simply paranoid schizophrenia?
schizophrenia in patients with a first episode of psychosis.
Schizophr Bull. 2012;38(3):561-8.
Psychiatry Res. 2010;175(1-2):11-4.
24.
Castagnini A, FoldagerL. Variations in incidence and
34.
Nuechterlein KH, Ventura J, Subotnik KL,
age of onset of acute and transient psychotic disorders.
BartzokisG. Te early longitudinal course of cognitive
Soc
Psychiatry
PsychiatrEpidemiol.
deficits
in schizophrenia. J Clin Psychiatry.
2013;48(12):1917-22.
2014;75Suppl 2:25-9.
25.
Pagel T, Baldessarini RJ, Franklin J, BaethgeC.
35.
Cuesta MJ, Sánchez-Torres AM, Cabrera B, et al.
Characteristics of patients diagnosed with schizoaffective
Premorbid adjustment and clinical correlates of cognitive
disorder compared with schizophrenia and bipolar
impairment in first-episode psychosis. Te PEPsCog
disorder. Bipolar Disord. 2013;15(3):229-39.
Study. Schizophr Res. 2015;164(1-3):65-73.
26.
Mancuso SG, Morgan VA, Mitchell PB, Berk M,
36.
Mehta UM, Tirthalli J, Subbakrishna DK,
Young A, Castle DJ. A comparison of schizophrenia,
Gangadhar BN, Eack SM, Keshavan MS. Social and
schizoaffective disorder, and bipolar disorder: Results
neuro-cognition as distinct cognitive factors in
from the Second Australian national psychosis survey. J
schizophrenia: a systematic review. Schizophr Res.
Affect Disord. 2014;30;172C:30-7.
2013;148(1-3):3-11.
27.
Pillmann F, Wustmann T, Marneros A. Acute and
37.
Choi KH, Fiszdon JM, Bell MD. Beyond cognition: a
transient psychotic disorders versus persistent
longitudinal investigation of the role of motivation
delusional disorders: a comparative longitudinal
during a vocational rehabilitation program. J NervMent
study. Psychiatry ClinNeurosci. 2012;66(1):44-52.
Dis. 2013;201(3):173-8.
28.
Marshall M, Lewis S, Lockwood A, Drake R, Jones P,
38.
Medalia A, Opler LA, Saperstein AM. Integrating
CroudaceT. Association between duration of untreated
psychopharmacology and cognitive remediation to treat
psychosis and outcome in cohorts of first-episode patients:
cognitive dysfunction in the psychotic disorders. CNS
a systematic review. Arch Gen Psychiatry.
Spectr. 2014;19(2):115-20.
2005;62(9):975-83.
39.
Michaels TM, Horan WP, Ginger EJ, Martinovich Z,
29.
Wustmann T, Pillmann F, Friedemann J, Piro J,
Pinkham AE, Smith MJ. Cognitive empathy contributes
Schmeil A, Marneros A. Te clinical and
to poor social functioning in schizophrenia: Evidence
sociodemographic profile of persistent delusional disorder.
from a new self-report measure of cognitive and affective
Psychopathol. 2012;45(3):200-2.
empathy. Psychiatry Res. 2014;220(3):803-10.
30.
Castagnini A, Berrios GE. Acute and transient psychotic
40.
Lindenmayer JP, McGurk SR, Khan A, et al.
disorders
(ICD-10 F23): a review from a European
Improving social cognition in schizophrenia: a pilot
perspective. Eur Arch Psychiatry ClinNeurosci.
intervention combining computerized social cognition
2009;259(8):433-43.
training with cognitive remediation. Schizophr Bull.
31.
DeRosse P, Burdick KE, Lencz T, Siris SG, Malhotra
2013;39(3):507-17.
AK. Empirical support for DSM-IV schizoaffective
41.
Walder DJ, Faraone SV, Glatt SJ, Tsuang MT,
disorder: clinical and cognitive validators from a large
Seidman LJ. Genetic liability, prenatal health, stress and
patient sample. PLoS One. 2013;8(5):e63734.
family environment: risk factors in the Harvard
32.
Levine SZ, Rabinowitz J. A population-based
Adolescent Family High Risk for schizophrenia study.
examination of the role of years of education, age of
Schizophr Res. 2014;157(1-3):142-8.
69
The Socio-Demographic Characteristics Associated with the Increased Likelihood of Subsequent Schizophrenia
Past and Present: Te North Teater
from Satu Mare
(Trecut și prezent: Teatrul de Nord
Satu Mare)
ORIGINAL ARTICLE
CORELAȚIE ÎNTRE SCĂDEREA GREUTĂȚII EXCESIVE ȘI ÎMBUNĂTĂȚIREA
CALITĂȚII VIEȚII LA 12 LUNI DUPĂ GASTRECTOMIA VERTICALĂ
LAPAROSCOPICĂ
Viorel Dejeu1,3, Dănuț-Aurel Dejeu1,3, Paula Dejeu2, Aurel Babeș3
1Clinica Chirurgie 1, Spitalul Clinic Județean de Urgență, Oradea, România, 2Laboratorul Spitalului Clinic Județean de
Urgență, Oradea, România, 3Facultatea de Medicină și Farmacie, Universitatea din Oradea, România
Adresa pentru corespondență:
Viorel Dejeu
P-ța Nucetului, 22, Bl. BC4, Ap. 111
Oradea, Romania
E-mail: viodejeu@yahoo.com
Primit: 02.02.2016
Acceptat: 28.06.2016
Med Con June 2016 Vol 11, No 2, 71-78
Rezumat
procesului de scădere în greutate în urma intervenției
chirurgicale nu se reflectă direct proporțional în
Scopul lucrarii: Chirurgia bariatrică oferă cel mai
îmbunătățirea QoL.
bun tratament pentru o scădere ponderală suficientă la
Cuvinte cheie: rezecție gastrică verticală
pacienții suferinzi de obezitate morbidă. Efectele
laparoscopică, obezitate morbidă, calitate a vieții, exces
negative ale obezității asupra calității vieții (QoL) sunt
ponderal, comorbidități
din ce în ce mai des menționate. Scopul principal al
acestui studiu este să investigăm relația dintre scăderea
Introducere
ponderală în urma intervenției laparoscopice de rezecție
gastrică verticală și efectul ei asupra calității vieții la un
Obezitatea este o problemă globală. Induce probleme
an după procedură. A fost analizată corelația dintre
de sănătate, probleme psiho-sociale, scade calitatea vieții
pierderea excesului ponderal (EWL) și îmbunătățirea
și crește costurile publice. Când un pacient ajunge în faza
observată în chestionarele de calitate a vieții (QoL).
obezității morbide, riscul de boală crește foarte rapid [1].
Material și metodă: 185 de pacienți cu obezitate
Creșterea continuă a numărului de persoane obeze este
morbidă au fost evaluați înaintea rezecției gastrice
acompaniată de creșterea frecvenței bolilor legate de
verticale și la
12 luni după intervenția chirurgicală.
obezitate, incluzând diabetul zaharat tip 2, hipertensiunea
Evaluarea a inclus măsurători antropometrice, SF-36 și
arterială, dislipidemii sau boli ischemice [2].
Moorehead-Ardelt Quality of Life Questionnaire II
Obezitatea morbidă este definită ca și un indice de
(MA-QoLQ).
masă corporală (IMC)≥40 sau IMC≥35kg/m2 combinat
Rezultate: Procentajul mediu de pierdere a greutății
cu cel puțin una din comorbiditățile: diabet zaharat tip
excesive a fost de 59,6%. Toate domeniile SF-36 și MA-
2, hipertensiune arterială, dislipidemie sau apnee
QoLQ au arătat îmbunătățiri semnificative la un an
obstructivă de somn.
(p<0,0001). Nu s-a putut demonstra o corelație între
În
1946 Organizația Mondială a Sănătății în
EWL și diferențe între scorul total al chestionarelor
constituția ei a definit sănătatea ca și o bunăstare
QoL (rho=-0.0134, p=0,8563).
completă fizică, mentală și socială, nu numai absența
Concluzii:
Tratamentul chirurgical
aduce
bolilor sau a dizabilităților. Astfel, conceptul modern al
îmbunătățiri semnificative în calitatea vieții. Anvergura
sănătății acoperă și calitatea vieții, sensul sănătății în
Correlation between Excessive Weight Loss and Quality of Life Improvements 12 Months after Laparoscopic
71
Sleeve Gastrectomy
ORIGINAL ARTICLE
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
sine fiind unul dintre determinanții de bază. Conform
efectele procedurii bariatrice asupra comorbidităților
mai multor autori, actualmente sensul sănătății este
legate de obezitate.
considerat o condiție fundamentală în determinarea
unei calități bune a vieții. Între numeroasele complicații
Material și metode
legate de obezitate și supraponderalitate, în afară de
bolile somatice afectând funcțiile unor organe
Acest studiu a fost condus de o echipă chirurgicală
individuale și sisteme, efectele negative asupra calității
în perioada ianuarie 2011 - februarie 2016. Cazurile au
vieții sunt tot mai frecvent menționate.
fost selectate din rândul pacienților internați în Clinica
Cadrele medicale se confruntă cu numeroase
de Chirurgie I a Spitalului Clinic Județean de Urgență
opțiuni pentru scăderea în greutate, dar numai chirurgia
Oradea și Clinica Medlife-Genesys Arad, pentru rezecție
bariatrică oferă cel mai bun tratament pe termen lung
gastrică verticală laparoscopică electivă în perioada
pacienților suferinzi de obezitate morbidă
[3,4]. Pe
ianuarie 2011 - decembrie 2015.
lângă scăderea în greutate are efecte profunde asupra
Design-ul studiului a fost aprobat de Comisia de
comorbidităților asociate obezității, cum sunt diabetul
Etică din ambele spitale, iar semnarea consimțământului
zaharat de tip 2, hipertensiunea și apneea de somn [5,6].
informat a fost un criteriu esențial în intrarea în studiu.
Bypass-ul gastric pe ansă Roux-în-Y (LRYGB) a fost
Criteriile de includere pentru acest studiu au
considerat cea mai bună opțiune chirurgicală pentru
cuprins: IMC peste 40kg/m2 sau IMC peste 35kg/m2
obezitatea morbidă și încă este una dintre cele mai
când se asociază cu o boală legată de obezitate, incluzând
frecvente proceduri bariatrice efectuate la nivel mondial
diabetul zaharat tip
2, hipertensiunea arterială,
[7,8]. Această procedură are avantaje, fiind reversibilă,
dislipidemii sau apneea obstructivă de somn cu un
bine documentată în ceea ce privește complicațiile
istoric de peste 3 ani; vârsta între 18 și 65 de ani.
precoce și rezultatele pe termen lung, fiind o intervenție
Criteriile de excludere au constat în: pacienți cu
efectuată de mai mult de 50 de ani și considerată ”gold
boală psihică sau psihologică, boală simptomatică de
standard” în chirurgia bariatrică și metabolică.
reflux gastro-esofagian, antecedente de chirurgie
Sleeve-ul gastric laparoscopic
(LSG) este o
bariatrică, antecedente de chirurgie abdominală majoră,
procedură relativ nouă, care a început ca un prim pas în
incapacitatea citirii sau înțelegerii chestionarelor legate
cadrul intervenției de duodenal switch (DS) la pacienții
de calitatea vieții.
superobezi, pentru a reduce mortalitatea perioperatorie.
Utilizând criteriile de selecție descrise mai sus, am
Rezultatele după această procedură au fost excelente,
selectat
237 pacienți. Din aceștia,
205 pacienți au
astfel ca nevoia convertirii la DS a mai fost necesară doar
semnat consimțământul informat pentru a participa la
la un sfert dintre pacienți. Actualmente, procedura de
studiu. La urmărire, doar 187 de pacienți s-au prezentat
sleeve gastric este o intervenție de sine stătătoare la
și 185 au completat chestionarele de evaluare a QoL.
pacienții care suferă de obezitate morbidă. LSG a
Pacienții care au fost acceptați pentru intervenția
devenit tot mai populară și a reprezentat aproximativ 28
chirurgicală au fost supuși unei evaluări inițiale. Această
% din procedurile bariatrice în 2011 [8]. LSG are niște
evaluare a inclus obținerea unui istoric medical detaliat,
dezavantaje, deși este o procedură mai rapidă și mai
o examinare clinică și paraclinică completă, măsurători
sigură, duodenul fiind accesibil pentru endoscopie. Cel
antropometrice, evaluarea inițială a calității vieții. De
mai serios dezavantaj poate fi considerat faptul că este
asemenea, a fost notată prezența comorbidităților legate
ireversibilă și fistula după sleeve gastric este mai greu de
de obezitate, care persistă mai mult de 3 ani.
tratat decât după un bypass. Calitatea vieții (QoL) pare
Evaluarea calității vieții
a fi similară, sau mai bună după LSG în comparație cu
Calitatea vieții pentru pacienții cu tratament
LRYGB, din cauza avantajelor menționate [9,10].
chirurgical pentru obezitate morbidă a fost evaluată cu
formulare medicale, standardizate: SF-36 (Short Form
Scopul studiului
Health Survey) și MA-QoLQII
(Moorehead-Ardelt
Quality of Life Questionnaire II).
Obiectivele principale al acestui studiu au fost
Chestionarul SF-36 [11] este o măsură a calității
investigarea modificărilor ponderale și impactul
generale a vieții legată de sănătate formată din 36 de
gastrectomiei verticale laparoscopice asupra calității
întrebări, compusă din opt scale (funcție fizică, rol fizic,
vieții la un an după intervenția chirurgicală. A fost de
durere somatică, sănătate generală, vitalitate, funcție
asemenea evaluată relația dintre scăderea greutății
socială, rol emoțional și sănătate mentală) în două
excesive și ameliorarea chestionarelor referitoare la
categorii mari: componenta fizică (PCS) și componenta
calitatea vieții. Ca și rezultate secundare am notat și
mentală
(MCS). Scorurile pentru cele
2 categorii
72
Dejeu et al
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
ORIGINAL ARTICLE
reprezintă indicatori independenți, bazate pe analiza
factorială a scorurilor din scalele subsecvente. Scorul
pentru toate scalele și pentru PCS și MCS este de la 0 la
100, unde 100 reprezintă cea mai bună performanță
vizând calitatea vieții legată de sănătate. Rezultatele pentru
PCS și MCS sunt cu distribuție normală (gaussiană), cu o
medie de 50 și deviație standard de 10. Chestionarul SF-
36 prezintă proprietăți psihometrice puternice [11].
Utilizarea instrumentelor de QoL, specifică anumitor
afecțiuni, în combinație cu chestionarele generice a fost
Figura 1. Gastrectomia verticală laparoscopică
întotdeauna recomandată [12]. Unul dintre cele mai
utilizate chestionare pentru evaluarea rezultatelor
unui tub gastric până la pilor. Tubul gastric are o
chirurgiei bariatric este Bariatric Analysis and Reporting
dimensiune de
34 French (Fr) în diametru și este
Outcome System (BAROS). Acesta include 3 domenii
important pentru realizarea unui tub gastric remanent
principale de analiză: scăderea ponderală, ameliorarea
mic. Restrângerea stomacului sub formă de mânecă se
afecțiunilor medicale și calitatea vieții. Modificările de
realizează prin obținerea a 4-5 linii de capsare lungi de
QoL în BAROS sunt evaluate cu ajutorul Moorehead-
60mm folosind staplerul prin același trocar. Stapler-ul
Ardelt Quality of Life Questionnaire II (MA-QoLQII),
este fixat strâns pe tubul gastric strângând curbura mare
considerat un instrument adecvat pentru examinarea
a stomacului
(Figura
1). După fiecare declanșare a
calității vieții la indivizii cu obezitate severă
[13,14].
stapler-ului, tubul gastric este mișcat de către anestezist
Persoanele sunt chestionate despre stima lor de sine,
sub vizualizare laparoscopică pentru a asigura că nu s-a
activitățile fizice, viața socială, capacitatea de lucru,
pus capsa direct pe tub. Ultima capsă se declanșează
activitatea sexuală și modul în care abordează mâncarea,
lateral de grăsimea lui Belsy lăsând esofagul neatins.
obținând scoruri între -0,5 și +0,5 [13]. Suma acestor 6
Terminarea: în următoarea fază, locul trocarului din
note generează un scor total de calitate a vieții. În funcție
stânga este dilatat și piesa gastrică rezecată este
de acest scor, fiecare pacient va fi clasificat în una din cele
îndepărtată. Ulterior, acest loc de trocar este închis la
5 categorii (foarte proastă: de la -3,0 la -2,1; proastă: de la
nivelul fasciei. Tubul gastric este îndepărtat de către
-2,0 la -1,1; medie: de la -1,0 la +1,0; bună: de la 1,1 la
anestezist sub vizualizare laparoscopică. Hemoragiile de
2,0; foarte bună: de la 2,1 la 3,0).
la nivelul liniilor de rezecție sunt controlate de obicei
Intervenția chirurgicală
prin capse, sau dacă este necesar, prin sutură. Numai în
Există două abordări diferite descrise în literatură
cazul sângerării, problemelor de capsare, sau alte
[15,16]: întâi capsarea, sau mai întâi mobilizarea totală a
dificultăți tehnice, se lasă tub de dren de-a lungul
curburii mari a stomacului. Având în vedere că
stomacului rezecat. Sutura peste linia de capsare nu se
închiderea strânsă a bontului gastric, care este
efectuează de rutină. Ulterior trocarele sunt îndepărtate
importantă pentru o scădere ponderală optimă, pare să
sub control vizual și pielea este închisă.
fie obținută cu tehnica mobilizării gastrice întâi [17],
Urmărirea
aceasta este singura tehnică folosită în această lucrare.
Reevaluarea standard pentru pacienții din acest studiu
Pornirea: după obținerea pneumoperitoneului
a fost la 12 luni după procedura chirurgicală. Această
printr-un ac Veress în hipocondrul stâng, 5 trocare sunt
evaluare a inclus o examinare clinică completă, măsurători
poziționate în funcție de preferința chirurgului.
antropometrice, repetarea chestionarelor de calitate a
Mobilizarea: curbura mare a stomacului este disecată la
vieții și reevaluarea comorbidităților legate de obezitate.
2-3cm distanță de la pilor, mobilizându-l spre unghiul
Procentul de pierdere a greutății excesive (%EWL) a
lui His, vizualizând tot hemidiafragmul stâng. În timpul
fost calculat prin împărțirea sumei totale de greutate
mobilizării curburii mari, toate aderențele gastro-
pierdută după intervenția chirurgicală, cu greutatea
pancreatice de la nivelul curburii mici sunt eliberate,
excesivă preoperatorie (calculată ca și excesul de greutate
urcându-se spre unghiul lui His. Acest pas este important
peste IMC de 25kg/m2) și multiplicată cu 100 [18].
pentru a permite realizarea unui tub gastric mic, fără un
Analiza statistică
fund remanent la nivelul peretelui gastric dorsal.
S-a utilizat programul de statistică medicală
Capsarea: un stapler endoscopic linear de 60mm este
MedCalc versiunea
12.5.0.0
(MedCalc® Software,
introdus prin trocarul din dreapta și declanșat la nivelul
Mariakerke, Belgia). Verificarea pentru distribuţia
antrum-ului gastric, lăsând spațiu numai pentru trecerea
valorilor comparativ cu populaţia normală s-a făcut cu
unui mandren gastric. Următorul pas este introducerea
testul Kolmogorov-Smirnov. În funcţie de rezultatul
73
Correlation between Excessive Weight Loss and Quality of Life Improvements 12 Months after Laparoscopic
Sleeve Gastrectomy
ORIGINAL ARTICLE
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
acestui test, variabilele continue cu distribuţie normală
an după efectuarea procedurii chirurgicale a fost în
vor fi reprezentate prin medie şi deviaţie standard în
medie de 34,4kg/m2 (variind de la 23,3 până la 45,9kg/
paranteză, iar cele cu distribuţie asimetrică prin mediana
m2) - p<0,0001 comparat cu valorile preoperatorii.
şi intervalele interquartile (IQR) în paranteză. Variabilele
În timpul vizitelor postoperatorii s-a observat
categorice vor fi descrise prin valorile lor absolute şi
ameliorarea semnificativă a comorbiditățior. Diabetul
procente în paranteză. Fiindcă este vorba de un studiu
zaharat de tip 2 a prezentat o reducere semnificativă a
de urmărire, am utilizat testele Student pentru loturi
tratamentului la 58 de pacienți din 81 (71,6%) - p<0,0001;
pereche și testul Wilcoxon pentru urmărirea obiectivelor
remisie completă (abolirea completă a tratamentului) în 17
propuse, comparând rezultatele pereche. Corelația între
cazuri (20,9%) - p=0,0884. Hipertensiunea s-a rezolvat
scăderea ponderală și ameliorarea calității vieții a fost
(valori normale fără medicație) în 37,6% din cazuri (50 de
evaluată cu ajutorul coeficientului de corelare Spearman.
pacienți din 133 inițial)- p<0,0001 și remisie parțială
Toate valorile ipotezei nul (p) sunt pe două brațe, cu o
(reducerea tratamentului) în 43,6% din cazuri (58 de
semnificație statistică sub valoarea de 0,05.
pacienți din 133) - p<0,0001. Din 86 de pacienți care au
luat tratament hipolipemiant înainte de intervenția
Rezultate
chirurgicală, la un an postoperator, doar 44 (o scădere de
48,8%) mai luau tratament - p<0,0001. Per general,
Caracteristicile demografice și clinice inițiale a celor
pacienții au raportat la un an postoperator o remisie a
185 de pacienți care au fost incluși în studiu sunt
OSAS de 63,9 % (53 de pacienți din 83 inițial) - p<0,0001.
prezentate în Tabelul I.
Comparând rezultatele chestionarelor înainte de
Toți pacienții au prezentat scădere ponderală
intervenția chirurgicală și la un an după procedura
semnificativă în urma tratamentului chirurgical.
bariatrică, am notat modificări semnificative statistic
Valoarea medie a procentului de pierdere a greutății
pentru toți parametrii calității vieții evaluați
prin
excesive (%EWL) a fost de 59,6%. IMC măsurat la un
formularul SF-36.
Tabel I. Caracteristicile inițiale demografice și clinice (preoperator)
Caracteristică
Lotul de studiu (n=185)
Vârstă (ani) - medie (DS)
44,2 (10,6)
Sexul (masculin/feminin) - număr (raport)
49/136 (1:2,8)
IMC (kg/m2) - medie (DS)
53,9 (7,8)
Hipertensiune arterială - număr (procente)
133 (71,9%)
T2DM - număr (procente)
81 (43,8%)
Dislipidemie în tratament cu statine - număr (procente)
86 (46,5%)
OSAS - număr (procente)
83 (44,9%)
DS - deviație standard; IMC - indice de masă corporală; T2DM - diabet zaharat tip 2; OSAS - sindromul apneei
obstructive de somn
Tabel II. Sumarul rezultatelor chestionarului SF-36 obținute înainte și la 1 an după procedura bariatrică
Componenta - medie (DS)
Preoperator
12 luni postoperator
p
Funcție fizică
35,1 (28,4)
56,2 (27,1)
<0,0001
Rol fizic
32,3 (40,2)
55,7 (41,2)
<0,0001
Durere somatică
45,6 (21,8)
58,1 (27,2)
<0,0001
Sănătate generală
38,2 (25,7)
53,9 (23,5)
<0,0001
Vitalitate
41,3 (21,6)
56,1 (23,1)
<0,0001
Funcție socială
43,1 (30,2)
52,3 (26,3)
0,0019
Rol emoțional
31,9 (40,8)
52,8 (41,8)
<0,0001
Sănătate mentală
39,3 (20,1)
50,2 (18,9)
<0,0001
Componenta fizică
38,2 (10,0)
57,1 (12,1)
<0,0001
Componenta mentală
39,8 (8,9)
50,8 (10,8)
<0,0001
Scor global de calitate a vieții
68,9 (25,1)
143,6 (29,5)
<0,0001
DS - deviație standard
74
Dejeu et al
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
ORIGINAL ARTICLE
Valoarea medie a scorului global de calitate a vieții a
niciun pacient nu s-a mai încadrat la catergoria foarte
fost de 143,6 (±29,5) la un an postoperator și a prezentat
proastă, la 3 bolnavi (1,6%) calitatea vieții a fost evaluată
o creștere semnificativă statistic față de valoarea inițială
ca și proastă, iar la 52 (28,2%) ca și medie. O calitate a
de 68,9 (±25,1). Toate componentele chestionarului
vieții bună și foarte bună a fost apreciată de către 70
QoL s-au ameliorat semnificativ la
12 luni după
(37,8%) respectiv 60 (32,4%) de pacienți (Figura 2).
intervenția chirurgicală.
Compararea acestor rezultate a arătat o îmbunătățire
Pe baza răspunsurilor date de pacienți la chestionarul
semnificativă și din perspectiva instrumentului de
Moorhead-Ardelt Quality of Life Questionnaire II, am
evaluare a calității vieții specifică bolii (p<0,0001).
înregistrat următoarele rezultate (ilustrate și în Figura
Pentru a răspunde la întrebarea dacă pierderea masei
2). Înainte de intervenția chirurgicală, la trei pacienți
corporale influențează gradul de îmbunătățire a calității
(1,6%) calitatea vieții a fost evaluată ca și foarte proastă,
vieții, criteriul de evaluare a eficacității tratamentului
la
38 de bolnavi (20,5%) ca și proastă, iar la
110
bariatric
(procentul de pierdere a greutății excesive -
(59,5%) ca și medie. O descriere a calității vieții ca și
%EWL) a fost corelată cu media schimbărilor survenite
bună și foarte bună a apărut la 25 (13,5%) respectiv 9
în scorul total din formularul SF-36. În acest scop a fost
(4,9%) pacienți. La 12 luni după intervenția chirurgicală,
calculată diferența dintre scorul general inițial și cel
postoperator pentru fiecare pacient și corelată cu
procentul de pierdere a greutății excesive cu ajutorul
testului statistic Spearman. Rezultatul acestui test nu
demonstrează corelație semnificativă între cele două
variabile (rho=-0,0134, p=0,8563) (Figura 3).
Discuții
Efectul negativ al obezității și a bolilor legate de
obezitate asupra calității vieții este universal cunoscut
[19]. Numeroase studii clinice și articole au demonstrat
clar că, față de persoanele normoponderale, calitatea
vieții la persoanele supraponderale este mai precară.
Aceasta se referă nu numai la calitatea vieții legată
Figura 2. Rezultatele Moorhead-Ardelt Quality of Life
funcția fizică a organismului, ca de exemplu intoleranța
Questionnaire II preoperator și la un an după SG
la exerciții fizice, probleme cu mișcarea sau durerea
Figure 3. Corelația între diferența de scor total SF-36 (preoperator și postoperator)
și procentul de pierdere a greutății excesive după SG
75
Correlation between Excessive Weight Loss and Quality of Life Improvements 12 Months after Laparoscopic
Sleeve Gastrectomy
ORIGINAL ARTICLE
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
somatică, ci și la calitatea vieții legată de aspectele
68,9 puncte, departe de standardul acceptat, aceasta
psihice, incluzând lipsa de acceptare a ei înșiși, niveluri
semnificând o calitate a vieții deteriorată în dimensiunea
crescute de stress, stimă de sine redusă și furie sau stări
fizică și mentală pentru toți pacienții tratați în cadrul
depresive [20]. Astfel, creșterea continuă a numărului de
acestui studiu. În studiul condus de Sarwer analiza
persoane obeze este echivalentă cu o creștere continuă a
efectelor procedurii RYGB asupra calității vieții la
grupului de persoane cu o calitate a vieții precară, în
bolnavii operați s-a efectuat, de asemenea, cu ajutorul
dimensiunile ei fizice și mentale.
chestionarului SF-36. Valoarea scorului general inițial a
Așteptările actuale a pacienților suferind de obezitate
fost de numai 52,3. Valoarea medie a scorului adunat
morbidă față de îngrijirile medicale includ nu numai
pentru componenta fizică și mentală a fost estimată la
ameliorarea stării de sănătate, ci și conducerea lor spre o
48,7, respectiv 62 de puncte. Se observă că aceste valori
bună-stare fizică și emoțională [21]. O metodă efectivă
sunt inferioare celor găsite în cadrul acestui studiu [29].
în tratamentul pacienților cu obezitate morbidă, care să
Scorul general al calității vieții pentru întreg lotul
ducă la o scădere ponderală permanentă, este tratamentul
de studiu, la un an postoperator, a fost de 143,6 puncte.
chirurgical. Reducerea IMC postoperatorie este asociată,
Această valoare depășește vizibil standardul înregistrat în
de asemenea, de numeroase schimbări metabolice
populația României, iar acest lucru este ciudat având în
avantajoase, care, în anumite cazuri, duce la reducerea
vedere faptul că niciun pacient nu a atins greutatea
severității sau dispariția completă a bolilor cauzate de
ideală după tratamentul bariatric în această perioadă de
obezitate. Astfel, reducerea masei corporale împreună cu
urmărire. În ciuda faptului că încă sunt supraponderali
ameliorarea sănătății în general duce la o îmbunătățire a
sau chiar obezi, calitatea vieții postoperator a fost mai
calității vieții la pacienții tratați corespunzător.
bună decât calitatea vieții a unei persoane supraponderale
Îmbunătățirea calității vieții, alături de tratamentul
ipotetice care nu se poate califica pentru tratamentul
obezității și a comorbidităților corelate, a devenit astfel
chirurgical. Unii pacienți, postoperator, mai au nevoie
unul dintre obiectivele principale ale chirurgiei
de tratamente pentru comoribiditățile legate de
bariatrice.
obezitate, dar, totuși, calitatea vieții lor au fost mai bună
La controlul postoperator la un an după intervenție,
decât media generală. Observații similare au fost făcute
indicele mediu de masă corporală era de 34,36kg/m2,
și la analiza factorilor individuali determinanți ai calității
ceea ce înseamnă o reducere a lui cu
19,55kg/m2.
vieții. În studii asemănătoare, de Zwaan a prezentat
Rezultatele obținute sunt semnificative statistic
rezultatele referitoare la calitatea vieții evaluată cu
(p<0,0001). Aceste rezultate nu diferă de datele care pot
ajutorul chestionarului SF-36 într-un grup de pacienți
fi găsite în literatură. De exemplu, în raportul Coupaye,
operați cu metoda RYGB. Asemănător studiului nostru,
reducerea indicelui de masă corporală la un an post
autorul a observat o îmbunătățire semnificativă a tuturor
rezecție gastrică verticală era de 15,9kg/m2 [22]. Într-un
paramentrilor evaluați. În cele mai multe cazuri, valorile
studiu suedez, Torgerson și Sjöström au arătat o scădere
înregistrate la populația studiată postoperator au depășit
a excesului de masă corporală
(%EWL), după
standardul general
[27]. Rezultate similare au fost
intervenție, de 58,8% [23].
prezentate și de Sarwer. Ceea ce pare interesant este
Descoperirile noastre cu privire la ameliorarea sau
faptul că o ameliorare semnificativă a fost notată pentru
remisia completă a diabetului, hipertensiunii,
toți parametrii din chestionar, chiar din primele 20 de
dislipidemiei și apneei de somn, la
12 luni după
săptămâni după tratamentul chirurgical, iar cu timpul,
intervenția chirurgicală, sunt în acord cu alte studii
aceste modificări au progresat, dar cu o viteză mult mai
[24,25]. Martínez și colab. au observat o îmbunătățire a
mică. În această perioadă, scăderea ponderală nu a atins
diabetului și a controlului hipertensiunii, o reducere
încă valoarea ei finală și comorbiditățile legate de
marcată a tulburărilor din metabolismul lipidic și
obezitate probabil încă nu s-au rezolvat [29]. Aceste
rezoluția completă a apneei de somn [26].
observații susțin ipoteza noastră conform căreia, faptul
După tratamentul chirurgical, toate scalele
în sine de a trece printr-o operație bariatrică, determină
formularului SF-36, alături de suma componentelor
o ameliorare semnificativă a calității vieții. Rezultatele
fizice și mentale, au arătat rezultate mai favorabile,
obținute în cadrul acestui studiu sunt astfel în
atingând chiar nivelul observat în populația normală
conformitate cu raportările altor autori.
[27]. Aceste rezultate sunt în concordanță cu descrierea
Analizând rezultatele obținute cu ajutorul
unor îmbunătățiri marcate, sau chiar normalizarea
chestionarului
MA-QoLQII după intervenția
tuturor celor 8 domenii a SF-36 în studii prospective
chirurgicală, am observat de asemenea ameliorarea
conduse de alți cercetători
[27,28]. Valoarea medie
calității vieții, evaluată cu ajutorul acestei metode. Nu
inițială a scorului general pentru lotul de studiu a fost de
mai puțin de 70,2% din cei 185 de pacienți au apreciat
76
Dejeu et al
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
ORIGINAL ARTICLE
calitatea vieții lor după chirurgia bariatrică ca fiind
În plus, este suprinzător faptul că procentul de exces de
foarte bună sau bună. În restul grupului de bolnavi, la
masă corporală pierdută după intervenție, nu se reflectă
marea majoritate calitatea vieții a fost evaluată ca și
direct proporțional în îmbunătățirea calității vieții.
medie, corespunzând standardului general. Al Harakeh
Îmbunătățirea spectaculoasă a calității vieții este un
a prezentat rezultate similare referitor la îmbunătățirea
argument puternic în vederea efectuării unei intervenții
calității vieții după chirurgia bariatrică, estimată pe baza
chirugicale, în ciuda nivelului crescut de dificultate a
chestionarului BAROS [30].
unei astfel de intervenții și al riscurilor potențiale. Cu
Rezultatele noastre sugerează că gradul de scădere a
toate acestea, sunt necesare studii care să evalueze
masei corporale postoperatorii nu influențează gradul de
calitatea vieții în urma unei intervenții bariatrice, pe o
ameliorare a calității vieții. Atât pacienții cu valori mici,
perioadă cât mai lungă de timp.
cât și cei care au atins valori mari ai parametrilor care
Conflict potențial de interese: declarăm lipsa
evaluează eficiența chirurgiei bariatrice
(%EWL), au
conflictelor de interese.
ajuns la o îmbunătățire similară a calității vieții. Această
observație, în ciuda lipsei unei literaturi extensive pe
această temă, pare să fie cel mai interesant rezultat al
Referințe
acestui studiu. Există opinii în literatura de specialitate
care indică diferențe semnificative în rezultatele
1.
Calle EE, Tun MJ, Petrelli JM, Rodriguez C, Heath
tratamentelor pentru diabet zaharat tip 2, hipertensiune
CW Jr. Body-mass index and mortality in a prospective
arterială sau dislipidemii, în funcție de rata de reducere a
cohort of U.S. adults. N Engl J Med.
masei corporale și în funcție de tipul intervenției
1999;341(15):1097-105.
chirurgicale. Cu toate astea, datele din prezenta lucrare
2.
World Health Organisation. Obesity and overweight.
indică un efect complet diferit al chirurgiei bariatrice
Fact Sheet. 2006;311.
asupra calității vieții la un an postoperator. Se pare că
3.
Elte JWF, Castro Cabezas M, Vrijland WW, Ruseler
însuși faptul intervenției chirurgicale bariatrice este mai
CH, Groen M, Mannaerts HH. Proposal for a
important pentru ameliorarea calității vieții decât rata
multidisciplinary approach to the patient with morbid
scăderii ponderale. Astfel, pe baza datelor din acest studiu,
obesity: the SintFranciscus Hospital morbid obesity
suntem de părere că nu există legătură directă între gradul
program. Eur J Intern Med. 2008;19(2):92-8.
de reducere a masei corporale și nivelul de ameliorare a
4.
Gloy VL, Briel M, Bhatt DL, Kashyap SR, Schauer PR,
calității vieții la
12 luni după gastrectomia verticală
Mingrone G, et al. Bariatric surgery versus non-surgical
laparoscopică. Nici în studiul lui Sarwer nu s-au observat
treatment for obesity: a systemic review and meta-analysis of
diferențe semnificative pentru îmbunătățirea calității
randomised controlled trials. BMJ. 2013;347:15934.
vieții în legătură cu gradul de reducere a masei corporale
5.
Maggard MA, Shugarman LR, Suttorp M, Maglione
[29]. Cu toate acestea, datele din literatură care confirmă
M, Sugerman HJ, Livingston EH, et al. Meta-analysis:
observația noastră sunt insuficiente. Astfel, sunt necesare
surgical treatment of obesity. Ann Intern Med.
desfășurarea unor studii mai extensive pe această temă.
2005;142(7):547-59.
Limitările studiului
6.
Sjöström L, Narbro K, Sjöström CD, Karason K,
Grupul de studiu a fost relativ mic; aceasta poate
Larsson B, Wedel H, et al. Effects of bariatric surgery
duce la inabilitatea de a detecta diferențe mici în
on mortality in Swedish obese subjects. N Engl J Med.
rezultatele clinice, în timp. Astfel, ar fi mai semnificativ
2007;357(8):741-52.
dacă un grup mai mare de studiu ar fi luat în calcul. De
7.
Buchwald H, Avidor Y, Braunwald E, Jensen MD,
asemenea, există factori care se suprapun și a căror
Pories W, Fahrbach K, et al. Bariatric surgery: a
influență asupra calității vieții nu poate fi evaluată foarte
systematic
review and meta-analysis. JAMA.
concret
(schimbări în statutul economic, social, sau
2004;292(14):1724-37.
circumstanțele de familie). Toate acestea se pot constitui
8.
Buchwald H, Oien DM. Metabolic/bariatric surgery
în limitări ale studiului prezent.
worldwide 2011. Obes Surg 2013;23(4):427-36.
9.
Peterli R, Borbely Y, Kern B, Gass M, Peters T,
Concluzii
Turnheer M, et al. Early results of the Swiss Multicentre
Bypass or Sleeve Study (SM-BOSS). Annals of Surgery.
Trebuie accentuat din nou faptul că, pentru oamenii
2013;258(5):690-5.
care suferă de obezitate morbidă, tratamentul chirurgical
10.
Overs SE, Freeman RA, Zarshenas N, Walton KL,
duce la o îmbunătățire semnificativă a calității vieții,
Jorgensen JO. Food tolerance and gastrointestinal
indiferent cât de mult a reușit obezitatea să o deterioreze.
quality of life following three bariatric procedures:
77
Correlation between Excessive Weight Loss and Quality of Life Improvements 12 Months after Laparoscopic
Sleeve Gastrectomy
ORIGINAL ARTICLE
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
adjustable gastric banding, Roux-en-Y gastric bypass
22.
Coupaye M et al. Comparison of nutritional status
and sleeve gastrectomy. ObesSurg. 2012;22(4):536-43.
during the first year after sleeve gastrectomy and Roux-
11.
Ware J, Snow K, Kosinski M, Gandek B. SF-36
en-Y gastric bypass. Obes Surg. 2014;24(2):276-83.
Health Survey: Manual and Interpretation Guide. Te
23.
Torgerson JS, Sjöström L. Te Swedish Obese Subjects
Health Institute, New England Medical Center,
(SOS) study-rational and results. Int J Obes.
Boston, MA, 1993.
2001;25:S2-4.
12.
LeMonte D, Moorehead MK, Parish MS, Reto CS,
24.
Christou NV, Sampallis JS, Liberman M, Look D,
Ritz SJ. Suggestions for the pre-surgical psychological
Auger S, McLean AP, et al. Surgery decreases long-term
assessment of bariatric surgery candidates. American
mortality, morbidity and health care use in morbidly
Society for Bariatric Surgery, October, 2004. Available
obese patients. Ann Surg. 2004;240(3):416-23.
25.
Hell E, Miller K, Moorehead MK, Norman S.
13.
Moorehead MK, Ardelt-Gattinger A, Lachner H, Oria
Evaluation of health status and quality of life after
HE. Te validation of the Moorehead-Ardelt Quality of
bariatric surgery: comparison of standard Roux en-Y
Life Questionnaire II. Obes Surg. 2003;13(5):684-92.
gastric bypass, vertical banded gastroplasty and
14.
Oria E, Moorehead MK. Bariatric Analysis and
laparoscopic adjustable gastric banding. Obes Surg.
Reporting Outcome System
(BAROS). Obes Surg.
2000;10(3):214-19.
1998;8(5):487-99.
26.
Martínez Y, Ruiz-López MD, Giménez R, Pérez de La
15.
Chu CA, Gagner M, Guinn T, et al. Two stage
Cruz AJ, Orduña R. Does bariatric surgery improve the
laparoscopic biliopancreatic diversion with duodenal
patient’s quality of life? Nutr Hosp. 2010;25(6):925-
switch: an alternative approach to super-super morbid
30.
obesity. SurgEndosc. 2002;16:S069.
27.
De Zwaan M, Lancaster KL, Mitchell JE, Howell
16.
Wölnerhanssen B, Peterli R. State of the art: sleeve
LM, Monson N, Roeriq JL, et al. Health related
gastrectomy. Dig Surg. 2014;31(1):40-7.
quality of life in morbidly obese patients: effect of gastric
17.
Gadiot R, Biter LU, Zengerink HJ, de Vos tot
bypass surgery. Obes Surg. 2002;12(6):773-80.
NederveenCappel RJ, Elte JW, Castro Cabezas M, et
28.
Dymek MP, Le Grange D, Neven K, Alverdy J.
al. Laparoscopic sleeve gastrectomy with an extensive
Quality of life and psychosocial adjustment inpatients
posterior mobilization: technique and preliminary
after Roux-en-Y gastric bypass: a brief report. Obes
results. Obes Surg. 2012;2(2):320-9.
Surg. 2001;11(1):32-9.
18.
Biesemeier C, Garland J. ADA pocket guide to bariatric
29.
Sarwer DB,Wadden TA,Moore RH,Eisenberg
surgery. Chicago, IL, USA: American Dietetic
MH,Raper SE,Williams NN.Changes in quality of life
Association, 2009.
and body image after gastric bypass surgery.
19.
Kushner RF, Foster GD. Obesity and quality of life.
SurgObesRelat Dis. 2010;6(6):608-14.
Nutrition. 2000;16(10):947-52.
30.
Al Harakeh AB, Larson CJ, Mathiason MA, Kallies
20.
Kolotkin RL, Meter K. Quality of life and obesity.
KJ, Kothari SN.BAROS results in 700 patients after
Obes Rev. 2001;2(4):219-29.
laparoscopic Roux-en-Y gastric bypass with subset
21.
Fontaine KR, Cheskin LJ, Barofsky I. Health-related
analysis of age, gender, and initial body mass index.
quality of life in obese persons seeking treatment. J
SurgObesRelat Dis. 2011;7(1):94-8.
FamPract. 1996;43(3):265-70.
78
Dejeu et al
GENERAL REVIEW
TRATAMENTUL OSTEOPOROZEI PRIMARE
Cristina Căpățînă, Cătălina Poiană
Institutul Național de Endocrinologie CI Parhon, București, România și Universitatea de Medicină și Farmacie Carol
Davila București
Adresa pentru corespondență:
Cristina Căpățână
Departament Endocrinologie UMF Carol Davila București, Secția de Patologie hipofizară și neuroendocrină
a Institutului National de Endocrinologie CI Parhon
Bd. Aviatorilor 34-36, sector 1, București
E-mail: cristina.capatina@yahoo.com
Primit: 24.02.2016
Acceptat: 30.06.2016
Med Con June 2016 Vol 11, No 2, 79-85
Rezumat
Unite cu peste
2 milioane de fracturi anual
[1].
Osteoporoza primară este o afecțiune a cărei etiopatogenie
Osteoporoza primară este o afecțiune cu o prevalență
este încă incomplet cunoscută și care apare la vârstnici și
în continuă creștere, în special în grupul femeilor
în perioada postmenopauză. Este o boală metabolică
postmenopauză. Atât prevalența ridicată cât și numărul
osoasă caracterizată prin masa osoasă scăzută, deteriorarea
mare de complicații și costurile enorme aduse sistemelor
microarhitecturii țesutului osos, cu fragilitate osoasă
de sănătate de către acestea, fac ca tratamentul osteporozei
consecutivă și risc crescut de fractură. Prin contrast,
să fie un domeniu prioritar. În prezent arsenalul
osteoporoza secundară are o cauză bine precizată (anumite
terapeutic dispune de un mare număr de mijloace de
afecțiuni cronice, administrare de medicamente, etc).
tratament începând de la mijloace non-farmacologice,
Osteoporoza afectează primordial sexul feminin (peste
suplimente cu calciu și preparate de vitamina D, până la
două treimi din cazuri). O explicație este aceea că masa
un mare număr de medicamente active: bisfosfonați,
osoasă de vârf este mai crescută la bărbați, de aceea riscul
denosumab, teriparatid. Alte clase de medicamente
lor global este mai redus. Totuși, bărbații vârstnici sunt și
folosite pe scară largă în trecut se folosesc tot mai puțin
ei expuși riscului de osteoporoză. Factorii de risc principali
astăzi
(estrogeni, calcitonină). Prioritatea cercetării în
pentru osteoporoză sunt sexul feminin, vârsta peste 65 de
acest domeniu a dus la descoperirea a numeroase
ani, menopauza, deficitul hormonilor gonadici, greutate
molecule active aflate în studii clinice.
corporală redusă, deficitul de calciu și vitamină D,
În concluzie, tratamentul osteoporozei primare
fumatul sau consumul cronic de alcool, istoricul familial
este complex, putând face uz de un mare număr de
de fracturi de fragilitate. Întrucât osteoporoza este
preparate active - tratamentul este necesar a fi condus
oligosimptomatică, testarea masei oase este recomandată
de către un specialist cu expertiză în domeniu.
la toate femeile sub 65 de ani sau bărbații între 50-70 de
Cuvinte cheie: osteoporoza, vitamina D,
ani cu factori de risc pentru osteoporoză, precum și la
bisfosfonați, denosumab, teriparatid
toate femeile peste 65 de ani, sau bărbații peste 70 de ani.
Tratamentul osteoporozei are drept scop conservarea
Introducere
masei osoase, scăderea riscului de fracturi de fragilitate și a
comorbidităților asociate, asigurarea nutriției optime [2].
Osteoporoza afectează peste
200 de milioane de
Obiectivul final al tratamentului este reducerea riscului
indivizi la nivel global și este asociată numai în Statele
de fractură de fragilitate.
Treatment of Primary Osteoporosis
79
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
Măsuri generale
gras. Pentru a fi activate ambele forme ale VD sunt
Aspectele nutriționale se adresează aportului de
necesare două etape de hidroxilare enzimatică. Prima are
calciu, proteine, vitamină D și recomandă suplimentarea
loc în ficat sub acțiunea 25 hidroxilazei (producând 25
zilnică cu cel puțin 1000mg de calciu, 800UI vitamină
hidroxi VD,
25OHD, calcidiol), cea de-a doua în
D și 1g/kg corp de proteine [2]. Măsurile specifice
rinichi, catalizată de 1α-hidroxilază și duce la producerea
adresate scăderii riscului de cădere cuprind următoarele:
substanței active,
1,25 dihidroxivitamina D
(1,25
evaluarea și corectarea tulburărilor de vedere (consult
OH2D, calcitriol). Concentrația serică a 25OHD se
oftalmologic, prescriere de ochelari); reducerea, pe cât
corelează pozitiv cu densitatea minerală osoasă (DMO)
posibil, a consumului de substanțe
(de exemplu
[5]. Administrarea de VD crește DMO şi reduce
anxiolitice, antidepresive, alcool) care sunt asociate cu
pierderea de masă osoasă la indivizii cu vârste de peste
afectarea echilibrului și/sau a stării de conștiență;
65 de ani [6,7].
îndepărtarea obstacolelor prezente pe traseele casnice ale
Concentraţia serică a
25OHD este semnificativ
pacientului; iluminare corespunzătoare a căilor de acces
corelată negativ cu riscul de fractură [8]. Suplimentarea
folosite de către pacient în mediul casnic; acoperirea
cu VD în doză de minim 800UI/zi scade riscul de
suprafețelor alunecoase cu materiale antiderapante, etc
fractură de şold şi nonvertebrală [9]. Nivelul ţintă al
[3].
concentraţiei de
25OHD care trebuie atins pentru
Tratamentul
farmacologic
al
osteoporozei
susţinerea unui efect consistent antifractură este de
influențează metabolismul osului și intervine atât în
minim 75nmol/l (echivalent cu 30ng/ml) [10,11]. Doza
procesul de resorbție, cât și de formare a osului. Cele
zilnică de vitamina D3 necesară pentru a atinge acest
mai utilizate terapii sunt raloxifenul (care face parte din
nivel este de cca 20-25μg/zi (echivalent cu 800-1000UI)
clasa modulatori selectivi de receptori estrogenici
-
[12].
SERM), bisfosfonații
(alendronat,
ibandronat,
Administrarea preparatelor de VD are efecte
risedronat), derivații de parathormon, ranelatul de
benefice și indirect, prin îmbunătățirea funcției și
stronțiu, densumsab. Tratamentul de substituție
performanței musculare. Concentrația serică a 25OHD
hormonală este folosit ca o a doua linie de tratament.
este direct corelată cu forţa musculară corectată pentru
Calciul și Vitamina D
vârstă şi sex [14], cu diverși indicatori de performanță
Vitamina D
(VD) nativă există sub
2 forme:
musculoscheletică (de exemplu viteza mersului, timpul
vitamina D2 (sintetizată de către plante) și vitamina D3,
de realizare a testului sit-to-stand) [13].
sintetizată la nivel cutanat prin transformarea
Suplimentarea cu VD are un efect semnificativ
precursorului
-
7-dehidrocolesterolul
- sub efectul
asupra forţei musculare la indivizi cu deficit semnificativ
radiațiilor solare [4]. O sursă importantă de VD sunt
de VD (25OHD≤25 nmol/L), dar nu și la cei fără deficit
alimentele, printre care: ouăle, produsele lactate, peștele
marcat de VD [14].
Tabel I. Mijloace de tratament farmacologic disponibile pentru managementul osteoporozei
Indicație
Scăderea riscului de fractură
Comentarii
Prevenție Tratament Vertebrală
Non-
Șold
vertebrală
Agenți antiresorbtivi
Alendronat
da
da
da
da
da
Administrare săptămânală
Administrare orală lunar sau
Ibandronat
da
da
da
-
-
iv la 3 luni
Administrare săptămânală
Risedronat
da
da
da
da
da
sau lunară
Zoledronat
-
da
da
da
da
Administrare iv anuală
Raloxifen
da
da
da
-
-
Prevenție cancer mamar
Calcitonină
-
da
da
-
-
Denosumab
-
da
da
da
da
Injectabil la 6 luni
Estrogen
da
-
da
da
da
Reacții adverse
Agenți anabolici
Teriparatid
-
da
da
da
-
Injectabil subcutanat
Alte
Ranelat de stronțiu
-
da
da
da
80
Căpățînă et al
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
GENERAL REVIEW
Administrarea de VD se asociază cu scăderea
stomatologice invazive, igienă orală deficitară. La
incidenţei căderilor, dar numai la doze mari
(800-
pacienții cu osteoporoză incidența acestei reacții adverse
1000UI), cu atingerea unor concentrații postterapeutice
este extrem de redusă 1/100.000 [2].
satisfăcătoare și numai la pacienții cu deficit de VD
Modulatorii selectivi ai receptorilor estrogenici
bazal [15].
(Selective Estrogen-Receptor Modulators, SERM)
Rolul asocierii uzuale a calciului la tratamentul cu
Preparatele din clasa SERM au afinitate de legare
VD este susținut de studiile care raportează că asocierea
pentru receptorul estrogenic și funcționează ca agoniști
este necesară pentru a scădea riscul de fractură. Riscul
sau antagoniști ai acestora în diverse țesuturi, în funcție
relativ de fractură de șold în cazul administrării exclusive
de ansamblul de evenimente intracelulare declanșate în
de VD a fost de 1,1 într-o metaanaliză a studiilor
fiecare țesut-țintă de legarea SERM de receptorul
publicate, în timp ce pentru asocierea cu calciu, riscul
estrogenic. Raloxifenul este singurul preparat din clasa
relativ combinat a fost de 0,82 [16].
SERM disponibil în practica clinică pentru prevenția și
Calcitriolul nu este în mod uzual folosit în
tratamentul osteoporozei postmenopauză. Studiul
tratamentul osteoporozei
(printre altele din cauza
Multiple Outcomes of Raloxifene Evaluation (MORE)
riscului mai crescut de reacții adverse și al hipercalcemiei),
[19] a demonstrat reducerea cu 30-50 % a riscului de
dar este aprobat pentru tratamentul bolii renale osoase
fracturi vertebrale la femei cu sau fără fracturi vertebrale
[17].
prevalente, dar fără efect semnificativ pe fracturile non-
Bifosfonații
vertebrale. Totuși, o analiză posthoc a pacienților incluși
Bifosfonații sunt clasa cea mai utilizată în
în studiul MORE a arătat și scăderea riscului de fracturi
tratamentul osteoporozei. Administrarea acestora
non-vertebrale la pacienții cu riscul bazal maxim,
exercită un efect antiresorbtiv potent prin scăderea
respectiv cei cu fracturi vertebrale prevalente la baseline
activării
osteoclastelor și stimularea apoptozei
[20]. Unicul efect advers sever a fost creșterea incidenței
osteoclastelor [18].
trombozei venoase profunde pe durata tratamentului.
Biodisponibilitatea în administrare orală este destul
Deosebit de importantă este scăderea semnificativă
de redusă (sub 1%) și există riscul de iritare a mucoasei
(cu cca 60%) a riscului de carcinom mamar invaziv
esofagiene. Din acest motiv se recomandă ca
[21], efect comparabil cu al tamoxifenului în populația
administrarea orală să fie a jeun, cu o cantitate suficientă
cu risc crescut de malignitate [22]. În ceea ce privește
de apă și cu evitarea clinostatismului minim
30 de
riscul cardiopatiei ischemice, conform studiului RUTH
minute
(pentru a scădea riscul de reacții adverse
(un studiu internațional multicentric randomizat,
esofagiene). Bifosfonații sunt stocați în proporție de
dublu-orb, placebo controlat) [23], Raloxifenul nu este
aproximativ
50% în sistemul osos, unde timpul de
un factor de risc semnificativ. Beneficiile Raloxifenului
înjumătățire este foarte lung.
în reducerea riscului de cancer mamar invaziv și fractură
Administrarea bifosfonaților este contraindicată la
vertebrală trebuie evaluate în raport cu creșterea riscului
pacienții cu hipocalcemie și necesită multă precauție la
de tromboembolism venos și accident vascular cerebral
cei cu afectare semnificativă a funcției renale (rată a
fatal [23].
filtrării glomerulare sub 30-35ml/min) și cu afectare a
Denosumab
tractului gastrointestinal superior. Administrarea
Denosumab-ul este un anticorp monoclonal specific
intravenoasă se asociază relativ frecvent cu reacții de fază
anti-receptor activator al ligandului factorului nuclear
acută, care răspund la tratament simptomatic.
kappa B (Receptor activator of nuclear factor kappa-B
O reacție adversă rară este osteonecroza
ligand, RANKL), cu efect potent de inhibare a resorbției
mandibulară, raportată în special la pacienți oncologici,
osoase prin inhibarea formării, acțiunii și duratei de
mai ales la cei cu afecțiuni stomatologice, proceduri
viață a osteoclastelor. Se administrează sub forma de
Table II. Eficacitatea relativă a diverșilor bifosfonați
Fracturi vertebrale Fracturi șold Fracturi non-vertebrale Referință
Comentarii
studiul FIT
la femei cu fracturi
Alendronat
↓50%
[34;35]
vertebrale prevalente
la femei cu fracturi
Risedronat
↓50%
↓33%
vertebrale prevalente
Ibandronat
↓
-
↓
[36]
Zoledronat iv
↓70%
↓40%
[37]
81
Treatment of Primary Osteoporosis
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
injecții subcutanate la interval de 6 luni. Este eficient
precum și reducerea modestă a riscului de fracturi
atât în osteoporoza primară unde reduce riscul de
vertebrale [30,31].
fractură vertebrală, de șold și non-vertebrală, dar și în
Într-un studiu placebo-controlat pe durata a 5 ani,
cea secundară afecțiunilor maligne și reumatologice.
administrarea a 200UI calcitonină de somon (sub formă
Contrar temerilor inițiale legate de administrarea pe
de spray nazal) a redus cu 33% riscul de noi fracturi
termen lung a unui preparat biologic, studiile raportate
vertebrale și a crescut cu 1% DMO la nivel lombar
până în prezent nu au ridicat problema unor reacții
într-o cohortă largă de femei postmenopauză
adverse grave [24].
diagnosticate cu osteoporoză [31].
Teriparatid, peptid din familia parathormonului
Tratamentul de substituție estrogenică
Deși administrarea continuă de parathormon
Administrarea de estrogeni în osteoporoza indusă de
(PTH) (sau excesul cronic de PTH) duce la resorbția
statusul postmenopauză reduce accelerarea turnoverului
osului cortical, administrarea intermitentă de PTH (în
osos, scade riscul de fracturi vertebrale și non-vertebrale
injecții zilnice subcutanate) induce creșterea masei
cu cca 30% [32]; efectul nu prezintă însă remanență la
osoase, atât la nivelul osului cortical, cât și al celui
întreruperea administrării [33]. Studiul Women’s Health
trabecular [25].
Initiative (WHI) a sugerat că raportul risc/beneficiu este
În tratamentul osteoporozei se folosesc atât PTH
destul de defavorabil în administrarea pe termen lung a
intact
(molecula peptidică având
84 de aminoacizi:
tratamentului de substituție hormonală. Utilizarea
1-84), cât mai ales fragmentul N-terminal având 34 de
combinată de estogeni conjugați și medroxiprogesteron
aminoacizi (1-34), numit teriparatid (doza echivalentă
acetat a fost asociată cu o creștere de cca 30% a riscului de
fiind de cca 40% din molecula intactă de PTH 1-84).
cardiopatie ischemică cronică și cancer mamar, precum și
Astfel, doza de teriparatid recomandată este de 20μg
o creștere de
40% a accidentelor vasculare cerebrale
zilnic în injecție subcutanată, doză care reduce nu doar
[34,35]. La femeile care au primit doar estrogeni conjugați
riscul de fractură vertebrală, dar și pe cel de fractură
(femei cu antecedente de histerectomie) nu s-a observat
non-vertebrală (spre deosebire de molecula intactă care
un risc crescut semnificativ de cancer mamar sau afectare
reduce doar riscul de fractură vertebrală) [2].
cardiacă ischemică, ceea ce a ridicat problema unui posibil
Durata maximă de administrare aprobată pentru
efect imputabil componentei progesteronice. Deși
preparatele derivate din PTH este de până la 24 de luni.
controversele asupra acestui aspect continuă, tratamentul
Reacțiile adverse sunt digestive, mialgii, cefalee, amețeli,
de substituție hormonală nu mai reprezintă prima linie de
hipercalcemie tranzitorie. Peptidele din familia PTH
tratament a osteoporozei postmenopauză.
sunt contraindicate la pacienții cu turnover osos crescut
Un preparat derivat, tibolonul, are avantajul de a
(de exemplu hiperparatiroidism primar, boala Paget,
reduce atât rata fracturilor, cât și pe cea a cancerului
neoplazii osoase primare sau secundare) și în insuficiența
mamar, dar crește riscul de accident vascular cerebral
renală severă
[2]. Preparatele din această clasă sunt
[26].
recomandate pacienților cu osteoporoză severă care sunt
Tratamentul combinat
neresponsivi, sau nu tolerează terapia antiresorbtivă
Efectul antiresorbtiv poate fi potențat prin
[26].
administrarea concomitentă a două medicamente
Ranelatul de stronțiu
antiosteoporotice din clase diferite, efectul nu se traduce
Ranelatul de stronțiu este un agent antiosteoporotic
în general prin scăderea suplimentară semnificativă a
care combină mecanismul antiresorbtiv cu cel
riscului de fractură. Ettinger și colab. [36], la pacienții
osteoformator. În administrare zilnică reduce atât riscul
tratați un timp îndelungat cu agenți antiresorbtivi (de
de fractură vertebrală, cât și non-vertebrală la doza
obicei bifosfonați) care primesc ulterior tratament cu
recomandată de 2g zilnic în administrare orală [27].
medicamente anabolice
(de exemplu teriparatid),
Preparatul este contraindicat la pacienți cu insuficiență
beneficiază de o eficiență terapeutică similară cu cea
renală severă. Ranelatul de stronțiu a fost asociat cu o
înregistrată de pacienții naivi la orice formă de tratament
incidență crescută a tromboembolismului venos în
antiosteoporotic, în ciuda faptului că efectul pe DMO
studiile de fază III, ceea ce a dus la contraindicarea
se instalează mai târziu la pacienții pretratați [36].
relativă a acestuia la pacienții cu antecedente personale
Nu există însă dovezi privind un efect sinergic al
de tromboză venoasă profundă.
teriparatidului și bifosfonaților în administrare
Calcitonina
concomitentă, unii autori considerând chiar că utilizarea
Calcitonina este un hormon polipeptidic cu efecte
concomitentă de alendronat reduce efectele anabolice
antiresorbtive [28]. Poate fi administrată injectabil sau
ale PTH [37]. Astfel, nu se recomandă ca cele două clase
transnazal și are ca efect o ușoară creștere a DMO [29],
de medicamente (sau cel puțin alendronatul) să fie
82
Căpățînă et al
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
GENERAL REVIEW
folosite concomitent, ci secvențial [38]; există studii care
6.
Dawson-Hughes B, Dallal GE, Krall EA, Harris S,
sugerează că alți bifosfonați (de exemplu risedronat), sau
Sokoll LJ, Falconer G. Effect of vitamin D
unele SERM (raloxifen), nu reduc efectul anabolic al
supplementation on wintertime and overall bone loss in
PTH [39]. În administrare secvențială se poate proceda
healthy postmenopausal women. Ann Intern Med.
și în sens contrar: un antiresorbtiv administrat după o
1991;115(7):505-12.
perioadă de tratament cu teriparatid consolidează
7.
Ooms ME, Roos JC, Bezemer PD, van der Vijgh WJ,
efectele benefice osoase ale acestuia [40].
Bouter LM, Lips P. Prevention of bone loss by vitamin
Creșterea DMO la coloană și șold în cursul
D supplementation in elderly women: a randomized
tratamentului cu alendronat este direct corelată cu
double-blind trial. J Clin Endocrinol Metab.
scăderea riscului de fractură
[41], însă în cazul
1995;80(4):1052-8.
risedronatului sau raloxifenului corelația nu este atât de
8.
Bischoff-Ferrari HA. Vitamin D and fracture
bună [42,43].
prevention. Rheum Dis Clin North Am.
Și în cazul ranelatului de stronțiu eficacitatea
2012;38(1):107-13.
antifractură este major determinată de modificările
9.
Bischoff-Ferrari HA, Willett WC, Orav EJ. A pooled
BMD la nivelul șoldului [44] și în proporție de cca 30%
analysis of vitamin D dose requirements for fracture
în cazul teriparatidului [45].
prevention. N Engl J Med. 2012;367(1):40-9.
Complianța la tratament
10.
Dawson-Hughes B, Mithal A, Bonjour JP. IOF
Complianța la tratament este un aspect de
position statement: vitamin D recommendations for
importanță majoră, având în vedere că osteoporoza este
older adults. Osteoporos Int. 2010;21(7):1151-4.
o afecțiune cronică, în mare parte asimptomatică și care
11.
Holick MF, Binkley NC, Bischoff-Ferrari HA.
necesită un tratament de lungă durată. Complianța
Evaluation, treatment, and prevention of vitamin D
scazută la tratament se asociază în osteoporoză cu
deficiency: an Endocrine Society clinical practice
persistența turnoverului osos crescut, risc crescut de
guideline. J Clin Endocrinol Metab. 2011;96(7):1911-
fractură și continuarea declinului densității minerale
30.
osoase [46]. De aceea, clinicianul trebuie să ia măsuri
12.
Dawson-Hughes B, Heaney RP, Holick MF, Lips P,
pentru a asigura tratamentul de lungă durată.
Meunier PJ, Vieth R. Estimates of optimal vitamin D
Conflict de interese: nimic de declarat.
status. Osteoporos Int. 2005;16(7):713-6.
13.
Bischoff-Ferrari HA, Dietrich T, Orav EJ. Higher
25-hydroxyvitamin D concentrations are associated with
Referințe
better lower-extremity function in both active and
inactive persons aged > or =60 y. Am J Clin Nutr.
1. Sheyn D, Shapiro G, Tawackoli W, Jun DS, Koh Y,
2004;80(3):752-8.
Kang KB, et al. PTH Induces Systemically Administered
14.
Stockton KA, Mengersen K, Paratz JD, Kandiah D,
Mesenchymal Stem Cells to Migrate to and Regenerate
Bennell KL. Effect of vitamin D supplementation on
Spine Injuries. MolTer. 2016;24(2):318-30.
muscle strength: a systematic review and meta-analysis.
2. Kanis JA, McCloskey EV, Johansson H, Cooper C,
Osteoporos Int. 2011;22(3):859-71.
Rizzoli R, Reginster JY. European guidance for the
15.
Bischoff-Ferrari HA, Dawson-Hughes B, Staehelin
diagnosis and management of osteoporosis in
HB. Fall prevention with supplemental and active forms
postmenopausal
women.
Osteoporos
Int.
of vitamin D: a meta-analysis of randomised controlled
2013;24(1):23-57.
trials. BMJ. 2009;339:b3692.
3. Kannus P, Sievanen H, Palvanen M, Jarvinen T,
16.
Boonen S, Lips P, Bouillon R, Bischoff-Ferrari HA,
Parkkari J. Prevention of falls and consequent injuries in
Vanderschueren D, Haentjens P. Need for additional
elderly people. Lancet. 2005;366(9500):1885-93.
calcium to reduce the risk of hip fracture with vitamin d
4. Battault S, Whiting SJ, Peltier SL, Sadrin S, Gerber
supplementation: evidence from a comparative
G, Maixent JM. Vitamin D metabolism, functions and
metaanalysis of randomized controlled trials. J Clin
needs: from science to health claims. Eur J Nutr.
Endocrinol Metab. 2007;92(4):1415-23.
2013;52(2):429-41.
17.
Ringe JD, Schacht E. Prevention and therapy of
5. Bischoff-Ferrari HA, Dietrich T, Orav EJ, Dawson-
osteoporosis: the roles of plain vitamin D and alfacalcidol.
Hughes B. Positive association between
25-hydroxy
Rheumatol Int. 2004;24(4):189-97.
vitamin D levels and bone mineral density: a population-
18.
Hughes DE, Wright KR, Uy HL, et al. Bisphosphonates
based study of younger and older adults. Am J Med.
promote apoptosis in murine osteoclasts in vitro and in
2004;116(9):634-9.
vivo. J Bone Miner Res. 1995;10:1478
83
Treatment of Primary Osteoporosis
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
19.
Ettinger B, Black DM, Mitlak BH. Reduction of
postmenopausal women with established osteoporosis: the
vertebral fracture risk in postmenopausal women with
prevent recurrence of osteoporotic fractures study.
osteoporosis treated with raloxifene: results from a 3-year
PROOF Study Group. Am J Med. 2000;109(4):267-
randomized clinical trial. Multiple Outcomes of
76.
Raloxifene Evaluation (MORE) Investigators. JAMA.
32.
Cauley JA, Robbins J, Chen Z. Effects of estrogen plus
1999;282(7):637-45.
progestin on risk of fracture and bone mineral density:
20.
Delmas PD, Genant HK, Crans GG. Severity of
the Women’s Health Initiative randomized trial. JAMA.
prevalent vertebral fractures and the risk of subsequent
2003;290(13):1729-38.
vertebral and nonvertebral fractures: results from the
33.
Bagger YZ, Tanko LB, Alexandersen P. Two to three
MORE trial. Bone. 2003;33(4):522-32.
years of hormone replacement treatment in healthy
21.
Cummings SR, Eckert S, Krueger KA. Te effect of
women have long-term preventive effects on bone mass
raloxifene on risk of breast cancer in postmenopausal
and osteoporotic fractures: the PERF study. Bone.
women: results from the MORE randomized trial.
2004;34(4):728-35.
Multiple Outcomes of Raloxifene Evaluation. JAMA.
34.
Chlebowski RT, Hendrix SL, Langer RD. Influence of
1999;281(23):2189-97.
estrogen plus progestin on breast cancer and
22.
Vogel VG, Costantino JP, Wickerham DL. Effects of
mammography in healthy postmenopausal women: the
tamoxifen vs raloxifene on the risk of developing invasive
Women’s Health Initiative Randomized Trial. JAMA.
breast cancer and other disease outcomes: the NSABP
2003;289(24):3243-53.
Study of Tamoxifen and Raloxifene (STAR) P-2 trial.
35.
Wassertheil-Smoller S, Hendrix SL, Limacher M.
JAMA. 2006;295(23):2727-41.
Effect of estrogen plus progestin on stroke in
23.
Barrett-Connor E, Mosca L, Collins P. Effects of
postmenopausal women: the Women’s Health Initiative:
raloxifene on cardiovascular events and breast cancer in
a randomized trial. JAMA. 2003;289(20):2673-84.
postmenopausal women. N Engl J Med.
36.
Ettinger B, San MJ, Crans G, Pavo I. Differential
2006;355(2):125-37.
effects of teriparatide on BMD after treatment with
24.
Bogado CE, Boailchuk JA, Zanchetta MB, Massari
raloxifene or alendronate. J Bone Miner Res.
FE, Zanchetta JR. Denosumab: an update. Drugs
2004;19(5):745-51.
Today (Barc). 2011;47(8):605-13.
37.
Black DM, Greenspan SL, Ensrud KE. Te effects of
25.
Hock JM, Gera I. Effects of continuous and intermittent
parathyroid hormone and alendronate alone or in
administration and inhibition of resorption on the
combination in postmenopausal osteoporosis. N Engl J
anabolic response of bone to parathyroid hormone. J
Med. 2003;349(13):1207-15.
Bone Miner Res. 1992;7(1):65-72.
38.
Finkelstein JS, Hayes A, Hunzelman JL, Wyland JJ,
26.
Eastell R. Osteoporosis. Oxford Textbook of
Lee H, Neer RM. Te effects of parathyroid hormone,
Endocrinology and Diabetes. New York: Oxford
alendronate, or both in men with osteoporosis. N Engl J
University Press Inc, 2011:701-11.
Med. 2003;349(13):1216-26.
27.
Reginster JY, Sarlet N, Lejeune E, Leonori L.
39.
Deal C, Omizo M, Schwartz EN. Combination
Strontium ranelate: a new treatment for postmenopausal
teriparatide and raloxifene therapy for postmenopausal
osteoporosis with a dual mode of action. Curr
osteoporosis: results from a
6-month double-blind
Osteoporos Rep. 2005;3(1):30-4.
placebo-controlled trial. J Bone Miner Res.
28.
Reginster JY. Effect of calcitonin on bone mass and
2005;20(11):1905-11.
fracture rates. Am J Med. 1991;91(5B):19S-22S.
40.
Black DM, Bilezikian JP, Ensrud KE. One year of
29.
Cranney A, Wells G, Willan A. Meta-analyses of
alendronate after one year of parathyroid hormone (1-
therapies for postmenopausal osteoporosis. II. Meta-
84) for osteoporosis. N Engl J Med. 2005;353(6):555-
analysis of alendronate for the treatment of
65.
postmenopausal women. Endocr Rev. 2002;23(4):508-
41.
Cummings SR, Karpf DB, Harris F. Improvement in
16.
spine bone density and reduction in risk of vertebral
30.
Cranney A, Guyatt G, Griffith L, Wells G, Tugwell P,
fractures during treatment with antiresorptive drugs.
Rosen C. Meta-analyses of therapies for postmenopausal
Am J Med. 2002;112(4):281-9.
osteoporosis. IX: Summary of meta-analyses of therapies
42.
Watts NB, Geusens P, Barton IP, Felsenberg D.
for
postmenopausal osteoporosis. Endocr Rev.
Relationship between changes in BMD and nonvertebral
2002;23(4):570-8.
fracture incidence associated with risedronate: reduction
31.
Chesnut CH, III, Silverman S, Andriano K. A
in risk of nonvertebral fracture is not related to change in
randomized trial of nasal spray salmon calcitonin in
BMD. J Bone Miner Res. 2005;20(12):2097-104.
84
Căpățînă et al
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
GENERAL REVIEW
43. Sarkar S, Mitlak BH, Wong M, Stock JL, Black DM,
45. Chen P, Miller PD, Delmas PD, Misurski DA, Krege
Harper KD. Relationships between bone mineral density
JH. Change in lumbar spine BMD and vertebral
and incident vertebral fracture risk with raloxifene
fracture
risk
reduction in teriparatide-treated
therapy. J Bone Miner Res. 2002;17(1):1-10.
postmenopausal women with osteoporosis. J Bone Miner
44. Bruyere O, Roux C, Detilleux J. Relationship between
Res. 2006;21(11):1785-90.
bone mineral density changes and fracture risk reduction
46. Reginster JY, Rabenda V, Neuprez A. Adherence,
in patients treated with strontium ranelate. J Clin
patient preference and dosing frequency: understanding
Endocrinol Metab. 2007;92(8):3076-81.
the relationship. Bone. 2006;38(4 Suppl 1):S2-S6.
85
Treatment of Primary Osteoporosis
Scrisoare de informare
Având în vedere activităţile revistei Medical Connections/Conexiuni Medicale privind recenzia şi
editarea articolului mai jos numit, efective odată cu acceptarea acestuia de către Medical Connections/
Conexiuni Medicale (la care se face referinţă în continuare ca Med Con), autorul (autorii) atribuie prin
prezenta către Med Con, reprezentanţilor legali, succesorilor şi mandataţilor ei, toate drepturile de
publicare şi fiecare şi oricare drept privind articolul în întreaga lume, în orice limbă şi în orice mediu, chiar
şi ca lucrare audiovizuală, colectivă, compilaţie, lucrare derivată, lucrare în comun, operă literară,
înregistrare audio, în imagini, grafică, operă de artă vizuală, program de calculator, sau orice alt mediu
existent acum sau care va deveni ulterior uzual, inclusiv drepturile de autor şi dreptul de a înregistra
dreptul de autor, precum şi dreptul de a asigura orice reînnoire, reeditare şi extinderea unor astfel de
drepturi de autor în România sau în orice ţară străină. Autorul (Autorii) pot solicita permisiunea de a
reutiliza manuscrisul sau porţiuni din acesta. Astfel de cereri trebuie să fie în scris, iar permisiunea dată de
Med Con nu va fi refuzată în mod nejustificat. Autorul (Autorii) desemnează Med Con ca reprezentant
legal al acestuia (acestora) pentru a întocmi orice documente pe care Med Con le consideră necesare
pentru a înregistra oricare dintre aceste garanţii la oficiul de copyright românesc sau din alte ţări. Autorul
(Autorii) garantează de asemenea către Med Con că articolul este lucrarea originală a autorului (autorilor),
cu excepţia materialelor provenite din domeniul public, iar fragmente din alte lucrări pot fi incluse doar cu
acordul prealabil scris al titularilor drepturilor de autor, că articolul nu a fost publicat anterior, nu a fost
prezentat, sau acceptat pentru publicare în altă parte, că autorul (autorii) nu au nicio relaţie, financiară sau
de altă natură, cu orice producător sau distribuitor de produse evaluate în această lucrare, sau, dimpotrivă,
orice astfel de relaţie a fost dezvăluită într-o notă de subsol la articol, sau că această cerinţă este irelevantă
pentru lucrare.
Titlul manuscrisului: _ _______________________________________________________
Nume:
Semnătură/Data:
_ ___________________________________
_ ___________________________________
_ ___________________________________
_ ___________________________________
_ ___________________________________
_ ___________________________________
_ ___________________________________
_ ___________________________________
_ ___________________________________
_ ___________________________________
_ ___________________________________
_ ___________________________________
_ ___________________________________
_ ___________________________________
Vă rugăm trimiteţi pe fax +40-261-710456 această scrisoare la sediul editorului Med Con.
GENERAL REVIEW
CANCERUL OVARIAN SUB LUPA ISTORIEI, MODALITĂŢI
TERAPEUTICE DE-A LUNGUL TIMPULUI. O REVISTĂ GENERALĂ
Ionuț Marcel Cobec1,2
1Clinica de Obstetrică-Ginecologie, Diakonie Klinikum, Schwäbisch Hall, Akademisches Lehrkrankenhaus der
Universität Heidelberg, Germania și 2Universitatea de Medicină şi Farmacie „Victor Babeş”, Timişoara, România
Adresa pentru corespondenţă:
Ionut Marcel Cobec, MD
Tel: +40 729099289, +4915163654211
e-mail: cobec_i@yahoo.com
Primit: 02.05.2016
Acceptat: 30.06.2016
Med Con June 2016 Vol 11, No 2, 87-90
Rezumat
Cancerul ovarian, cu o incidenţă la nivel mondial
de 42 de cazuri la 100.000 [3], reprezintă a doua cauză
Cancerul ovarian este o patologie care de-a lungul
de deces între cancerele ginecologice şi a şaptea cauză de
istoriei a stârnit atât controverse, cât şi întrebări, unele
cancer la femei [4-6], el având cea mai mare mortalitate
rămânând până în zilele noastre fără răspuns. De-a
(anual numărul de decese reprezintă mai mult de
lungul timpului s-au depus eforturi continue care au
jumătate din numărul de cazuri noi identificate [3])
reprezentat o piatră turnantă la actualul standard
între carcinoamele ginecologice, fiind supranumit
terapeutic existent în abordarea tumorilor ovarului.
„silent killer” [7-13].
În această lucrare se urmăresc treptat paşii făcuţi de
Urmărind un scurt istoric al cancerului ovarian
înaintaşii noştrii în munca de pionierat reprezentată atât
putem observa tentativele continue de a identifica
de terapia chirurgicală, cât şi de cea medicamentoasă,
cauzele acestei patologii, dorinţa continuă de a o
dar şi de noile descoperiri în domeniu, precum şi
clasifica, precum şi diferitele mijloace terapeutice, fie ele
literatura de specialitate elaborată, per total reprezentând
invazive ori non-invazive, folosite de-a lungul timpului,
o bogată zestre ştiinţifică.
de fiecare dată existând speranţa unui tratament victorios
Pornind de la primele tentative chirurgicale, urmate
în lupta cu această maladie a secolului XXI, cancerul.
de diversele terapii medicamentoase ori radiologice
La mijlocul secolului al XIX-lea ca urmare a
elaborate, soldate cu mai mult ori mai puţin succes şi
creşterii numărului de acte chirurgicale începe
ajungând la terapiile actuale, această lucrare sumează o
observarea cu atenţie a tumorilor ovariene și efectuarea
filă de istorie a cancerului ovarian.
a ceea ce era numit la acea vreme ovariotomie,
Cuvinte cheie: cancer ovarian, terapie, istoric,
actualmente oofrectomie. În anul 1809 a fost efectuată
opţiuni
prima ovariotomie de către Ephraim McDowell, dar şi
de către pionierii în chirurgie Spencer Wells şi Lawson
Cancerul reprezintă o patologie care pune adevarate
Tait [14].
probleme sistemelor de sănătate publică, în România
În anul 1870 Heinrich Waldeyer a elaborat o lucrare
incidenţa acestuia fiind printre cele mai scăzute din
legată de tumorile ovariene epiteliale, pentru prima dată
Europa centrală şi de sud-est, dar cu o rată mare a
fiind sugerată o histogeneză care este general acceptată
mortalităţii [1]. În patogenia cancerului sunt implicate
în zilele noastre. Doi ani mai târziu, E. Randolph a
atât funcţiile, cât şi răspunsul imun, iar angiogeneza,
elaborat prima carte care abordează în detaliu patologia
hipoxia și inflamaţia pot fi identificate la nivel celular [2].
ovariană, fiind intitulată Tumorile ovariene: patologia,
The Ovarian Cancer Under the Histories Magnifying Glass, Therapy Possibilities Over the Time
87
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
diagnosticul şi tratamentul lor, în special prin ovariotomie.
VEGFRs asupra tuturor izoformelor VEGF, prevenind
O primă contribuţie importantă a fost făcută de
creşterea tumorală şi producerea de ascită. Paclitaxel-ul
Hermann Johannes Pfannenstiel prin cartea publicată în
poate fi folosit în combinaţie cu bevacizumab-ul, având
anul 1898 în care se introduce conceptul de neoplasme
rol sinergic şi aceleaşi efecte. Bevacizumab folosit în
intermediare şi este detaliat termenul de malign.
combinaţie cu cisplatin duce la creşterea supravieţuirii
Krukenberg a descris la doar 25 de ani într-o lucrare de
[19,20]. Bazându-se pe faptul că tumorile ovariene
35 de pagini leziunea Krukenberg, ca un sarcom, ea
beneficiază de o bogată vascularizaţie dependentă de
fiind recunoscută ca o metastază de către Schlagenhaufer
angiogeneză mediată de VEGF, s-au elaborat tentative
în anul 1902. În anul 1907 Brenner descrie într-o teză
terapeutice, atât în domeniul clinic, cât şi în cel preclinic.
tumora care îi poartă numele, el lucrând într-o
Una din cele mai utilizate terapii este cea cu bevacizumab
obscuritate relativă în Africa de Sud unde a fost
pentru a neutraliza VEGF circulant şi pentru a suprima
descoperit de Harold Speert, cel care a publicat în anul
angiogeneza. Într-un studiu clinic de fază III asupra
1958 cartea Obstetric and Gynecologic Milestones. În anul
cancerului ovarian se arată că bevacizumab-ul
1925 John Albertson Sampson, supranumit tatăl
prelungeşte supravieţuirea fără progres tumoral când
endometriozei, vorbeşte despre asocierea endometriozei
este administrat în combinaţie cu chimioterapia, deşi
ovariene cu carcinomul endometrial [14].
această aplicare este limitată, deoarece terapia cu anti-
În perioada
1956-1957 Organizaţia Mondială a
VEGF este asociată cu efecte adverse destul de dure
Sănătăţii
(WHO) a încercat să realizeze numeroase
[19,20,21]. Folosirea îndelungată a terapiei anti-VEGF
clasificări privind tumorile ovariene.
duce la producerea de alți factori proangiogenici, astfel
Prima clasificare a tumorilor stromale epiteliale de
încât folosirea şi producerea unei terapii independente
suprafaţă a fost elaborată în 1961 de către Federaţia
de VEGF tumoral este critică.
Internaţională de Obstetrică şi Ginecologie (FIGO).
Datorită prognozei sumbre a cancerului ovarian,
În 1963 şi ulterior în 1965 s-au desfășurat întâlniri
Sato și Itamochi [22] în cadrul unui studiu au revenit la
între reprezentanţii FIGO şi cei ai WHO în vederea
idea de a folosi radioterapia, utilizată în anii 1950, însă
elaborării unei clasificări comune pentru evitarea
au renunţat ulterior datorită efectelor adverse. În cadrul
paralelismelor. Varianta finală a clasificării tumorilor
unui studiu pilot de fază I/II asupra cancerului ovarian,
ovariene a fost publicată în 1973 de către WHO [14].
FIGO III (R1 sau R2<1cm), după rezecţia chirurgicală
Stadializarea cancerului ovarian a fost acceptată de
şi chimioterapia adjuvantă bazată pe platină, s-au inclus
FIGO în 1988 într-o formă asemănătoare cu cea actuală.
6 cicluri de carboplatină sau cisplatină şi paclitaxel sau
De-a lungul timpului au fost multe studii ce au arătat
docetaxel la interval de 3 săptămâni [22]. Ulterior s-a
necesitatea reviziei şi a modificării stadializării FIGO
decis tratamentul cu radioterapie de intensitate
pentru o diferenţiere mai eficientă a prognosticului bolii
modulată, datorită avansării tehnologiei având
[15]. În 2014 a fost aprobată noua stadializare FIGO a
posibilitatea de a reduce efectele adverse prin protecţia
cancerului ovarian, ţinând cont de toate recomandările
organelor aflate la risc precum rinichii, ficatul, măduva
propuse pentru a fi cât mai eficientă în tratarea maladiei.
osoasă hematogenă [23].
În 1983 a fost identificat un polipeptid într-un
În decursul timpului, numeroase grupuri de
mediu cu linii celulare tumorale de porc de Guineea
cercetare au încercat stabilirea unei terapii eficiente în
[16], cu rol în permeabilitatea vascularizării tumorale,
cazul cancerului ovarian. În cadrul acestor tentative au
numit factor vascular de permeabilitate (VPF). Ulterior,
fost numeroase perioade în care s-au încercat diverse
în 1989 a fost izolat din celulele foliculare pituitare
combinaţii terapeutice antitumorale, cu mai mult sau
bovine şi redenumit Vascular Endothelial Growth Factor
mai puţin succes, toate având ca scop îmbunătăţirea
(VEGF), factor pentru celulele vasculare endoteliale
prognozei cancerului ovarian şi fiind o placă turnantă a
[17,18].
actualelor standarde terapeutice, atât chirurgicale, cât şi
VEGF este implicat în procesul de creştere tumorală,
medicamentoase.
invazie şi diseminare la nivelul ganglionilor limfatici,
În 1976 semnalăm un prim succes al eficienţei
ficatului, plămânilor. Aceasta este rațiunea pentru care
utilizării cisplatinei, produs de combinaţia chimioterapiei
sunt folosiţi numeroşi agenţi medicamentoşi având ca
bazată pe platin. Anii 1980-1990 sunt un alt moment
ţintă rolul purtat de VEGF în cancerul ovarian,
de succes terapeutic în cadrul drumului anevoios al
carcinomatoza peritoneală şi/sau prezenţa ascitei. Printre
identificării unui tratament eficient, prin descoperirea
agenţii folosiţi cu rol în neutralizarea VEGF se numără
paclitaxelului. Studii ulterioare au dovedit eficienţa
bevacizumab, un anticorp monoclonal uman
superioară a folosirii cisplatinului în combinaţie cu
recombinant ce acţionează prin împiedicarea legării
paclitaxel, spre deosebire de combinația cisplatin-
88
Cobec et al
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
GENERAL REVIEW
ciclofosfamid, devenind astfel un tratament de primă
6.
Saad AF, Hu W, Sood AK. Microenvironment and
linie terapeutică. Ulterior au încercat să fie identificate
Pathogenesis of Epitelial Ovarian Cancer. Horm
combinaţii terapeutice în cadrul cărora să fie reduse
Cancer. 2010;1(6): 277-90.
efectele adverse ale chimioterapeuticelor. A fost încercat
7.
Rosen DG, Yang G, Liu G, Mercado-Uribe I, et al.
carboplatinul, un analog al cisplatinului, prezentând
Ovarian cancer: pathology, biology, and disease models.
mai puţine efecte adverse decât cisplatinul. În decursul
Front Biosci. 2010;14:2089-102.
timpului, din necesitatea unui tratament nu doar
8.
Kim A, Ueda Y Naka T, Enomoto T. Terapeutic
eficient, ci şi cu efecte adverse reduse, au fost încercate
strategies in epithelial ovarian cancer. Journal of
diverse combinaţii terapeutice, printre acestea
Experimental & Clinical Cancer Research. 2012;31:14.
numărându-se şi încercarea de a substitui paclitaxel-ul
9.
Lalwani N, Prasad SR, Vikram R, et al. Histologic,
cu docetaxel-ul. Până în acest moment această substituire
Molecular and Cytogenetic Features of Ovarian Cancers:
poate fi facută doar în cazul neurotoxicităţii de grad
Implications
for
Diagnosis
and Treatment.
înalt, tratamentul standard rămânând carboplatin-
RadioGraphics. 2011;31:625-46.
paclitaxel [24].
10.
Cho KR, Shih IM. Ovarian Cancer. Annu Rev Pathol.
În prezent, un nou medicament este folosit ca terapie
2009;4:287-313.
de menţinere, terapia orală cu olaparib, un inhibitor al
11.
Barua A, Bitterman P, Abramowicz JS, et al.
poli-(ADP-ribozei) polimerazei
(PARP). Acesta este
Histopathology of ovarian tumors in laying hens, a
administrat pacientelor cu cancer ovarian seros recurent
preclinical model of human ovarian cancer. Int J
platin sensibil, la care s-a dovedit existenţa unei mutaţii la
Gynecol Cancer. 2009;19(4):531-9.
nivelul BRCA şi care au avut două sau mai multe cure de
12.
Shih I.M., Davidson B. Pathogenesis of ovarian cancer:
chimioterapie bazate pe platin şi au arătat un răspuns
clues from selected overexpressed genes. Future Oncol.
parţial ori complet la cura de chimioterapie cea mai recent
2009;5(10):1641-64.
utilizată bazată pe platin [25,26].
13.
Karst AM, Drapkin R. Ovarian Cancer Pathogenesis:
Studiile clinice care se desfăşoară în prezent testează
A Model in Evolution. Hindawi Publishing
diverse monoterapii ori combinaţii terapeutice din
Corporation Journal of Oncology. 2010;1-13.
necesitatea descoperirii unei terapii eficiente, pentru a
14.
Zoung RH. A brief history of the pathology of the
îmbunătăţi calitatea vieţii pacientelor aflate sub
gonads. Modern Pathology. 2005;18,S3-S17.
tratament.
15.
Suh DH, Kim TH, Kim JW, et al. Improvements to the
FIGO staging for the ovarian cancer: reconsideration of
lymphatic spread and intraoperative tumor rupture. J
Referințe
Gynecol Oncol. 2013;24(4):352-8.
16.
Senger DR, Galli SJ, Dvorak AM, et al. Tumor cells
1. Vrdoljak E, Wojtukiewicz MZ, Pienkowski T, Bodoky
secrete a vascular permeability factor that promotes
G, Berzinec P, Finek J, Todorović V, Borojević N,
accumulation
of
ascites
fluid.
Science.
Croitoru A. South Eastern European Research Oncology
1983;219(4587),983-5.
Group. Cancer epidemiology in Central, South and
17.
Ferrara N, Henzel WJ. Pituitary follicular cells secrete
Eastern European countries. Croat Med J.
a novel heparin-binding growth factor specific for
2011;52(4):478-87.
vascular endothelial cells. Biochemical and Biophysical
2. Markert EK, Levine AJ, Vazquez A. Proliferation and
Research Communications. 1989;161(2):851-8.
tissue remodeling in cancer: the hallmarks revisited. Cell
18.
Connolly DT, Olander JV, Heuvelman D, et al.
Death Dis. 2012;3:e397.
Human vascular permeability factor. Isolation from
3. McLemore MR, Miaskowski C, Aouizerat BE, et al.
U937 cells. Journal of Biological Chemistry.
Epidemiologic and Genetic Factors Associated with
1989;26(33):20017-24.
Ovarian Cancer. Cancer Nurs. 2009;32(4):281-90.
19.
Masoumi Moghaddam S, Amini A, Morris DL,
4. Yoneda A, Lendorf ME, Couchman JR, et al. Breast
Pourgholami MH. Significance of vascular endothelial
and Ovarian Cancers: A Survey and Possible Roles for the
growth factor in growth and peritoneal dissemination of
Cell Surface Heparan Sulfate Proteoglycans. Journal of
ovarian cancer. Cancer Metastasis Rev. 2012;31(1-
Histochemistry & Cytochemistry. 2012;60(I):9-21.
2):143-62.
5. Moghaddam SM, Amini A, Morris DL, et al.
20.
Leamon CP, Lovejoy CD, Nguyen B. Patient selection
Significance of vascular endothelial growth factor in
and targeted treatment in the management of platinum-
growth and peritoneal dissemination of ovarian cancer.
resistant ovarian cancer. Pharmgenomics Pers Med.
Cancer metastasis Rev. 2012;31:143-62.
2013;6:113-25.
89
The Ovarian Cancer Under the Histories Magnifying Glass, Therapy Possibilities Over the Time
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
21. Cho R K. Ovarian cancer update: Lessons from
24. Kim A, Ueda Y, Naka T, Enomoto T. Terapeutic
Morphology, Molecules and Mice. Arch Pathol Lab
strategies in epithelial ovarian cancer. J Exp Clin
Med. 2009;133(11):1775-81.
Cancer Res. 2012;31:14.
22. Sato S, Itamochi H. Neoadjuvant chemotherapy in
25. Ledermann J, Harter P, Gourley C, et al. Olaparib
advanced ovarian cancer: latest results and place in
maintenance therapy in patientins with platinum-sensitive
therapy. Terapeutic Advances in Medical Oncology.
relapsed serous ovarian cancer: a preplanned retrospective
2014;6(6),293-304.
analysis of outcomes by BRCA status in a randomized
23. Rochet N, Jensen AD, Sterzing F, et al. Adjuvant
phase 2 trial. Lancet Oncol. 2014;15(8):852-61.
whole abdominal intensity modulated radiotherapy
26. Oza AM, Cibula D, Benzaquen AO, et al. Olaparib
(IMRT) for risk stage FIGO III patients with ovarian
combined with chemotherapy for recurrent platinum-
cancer (OVAR-IMDT-01)-Pilot trial of phase I/II study:
sensitive ovarian cancer: a randomised phase 2 trial.
study protocol. BMC Cancer. 2007;7:227.
Lancet Oncol. 2015;16(1):87-97.
90
Cobec et al
GENERAL REVIEW
HEMORAGIA CEREBRALĂ INTRAVENTRICULARĂ. UN EVENIMENT
PATOLOGIC INTRAGESTAȚIONAL
Zamfir-Radu Ionescu1, Georgiana-Cristina Ionescu2
1Spitalul de Pediatrie, Pitești, jud. Argeș, România, 2Departamentul de Pediatrie și Neonatologie, Universitatea de
Medicină și Farmacie „Carol Davila”
Adresă pentru corespondență:
Dr. Zamfir-Radu Ionescu, M.D., Ph.D.
Departamentul de Anatomie Patologică, Spitalul de Pediatrie Pitești
Bd. Dacia, Nr. 1, Pitești, jud. Argeș, România,
Tel: 0040346086086
E-mail: dr.raduionescu@yahoo.com
Primit: 09.02.2016
Acceptat: 28.02.2016
Med Con June 2016 Vol 11, No 2, 91-94
Rezumat
ceilalți factori modificabili intercurenți pot reduce
importanța acestora. Aceasta implică hipertensiunea și
Hemoragia intraventriculară (IVH) se definește ca
presiunea sistolică ridicată la copii proveniți din sarcini
fiind un eveniment cerebrovascular care a determinat ca
singulare și gemelare cu GMN, în timp ce greutatea mare
hemoragia să apară în unul sau ambii ventriculi cerebrali.
la vârsta gestațională predispune viitorul adult la un index
IVH este foarte obișnuită la nou-născuți în timpul
de masă corporală crescut, potential factor de risc
perioadei perinatale imediate, cu debut timpuriu sau
cardiovascular [1]. GMN este definit ca fiind greutatea la
tardiv, de obicei având o evoluție frustă, cu afectare
naștere a unui nou-născut viu mai mică sau egală decât
motorie sau cognitivă în timpul dezvoltării ulterioare a
2.499 grame (5,5 livre), indiferent de vârsta gestațională.
copilului. Aceasta poate fi detectabilă cu ajutorul
Această greutate ar trebui măsurată în primele ore de la
ecografiei transfontanelare combinată cu imagistica prin
naștere pentru a menține o distanță temporală dincolo de
rezonanță magnetică în primele ore de viață ale nou-
orice pierdere ulterioară de greutate postnatală. Factorii
născutului prematur. Tehnicile posturale, examinarea,
de risc pentru GMN sunt fie prematuritatea din sarcini
manipularea atentă și profilaxia farmacologică a
cu vârsta sub 37 de săptămâni, fie restricția de creștere
copilului prematur ajută la prevenția complicațiilor
intrauterină (IUGR). Organizația Mondială a Sănătății
ulterioare ale IVH. Scopul acestei lucrări este o revedere
consideră drept circumstanțe care conduc la GMN și
rapidă a literaturii medicale disponibile și de a atrage
durata scurtă a gestației, o dietă maternă insuficientă,
atenția asupra acestui tip de problemă medicală.
săracă în timpul sarcinii, traiul la altitudine mare, statura
Cuvinte cheie: hemoragie intraventriculară,
mică a femeilor, expunerea la toxice (alcoolism, fumat
prematuritate,
nou-născut, neurologie, afectare
matern) sau infecții (HIV, sifilis) și hipertensiune. Unii
neurologică
copii au doar GMN sau CP iar alții au ambele
caracteristici, pe care OMS le recunoaște ca un dezavantaj
Introducere
major pentru aceștia și ca un indicator principal pentru
mortalitatea și morbiditatea imediat postnatală
[2].
În literatura modernă, greutatea mică la naștere
Scopul acestui articol este de a oferi o revedere asupra
(GMN) și prematuritatea la copii (CP) au devenit un
patogeniei și a atitudinii investigaționale pentru IVH
factor de risc pentru boala cardiovasculară, în timp ce
neonatal la copiii cu prematuritate.
Cerebral Intraventricular Hemorrhage. A Gestational Pathological Event
91
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
Patogenie
vizibilă în ventriculii al treilea și al patrulea. Uneori,
extinderea sângerării inițiale de la nivelul matricei
Dezvoltarea fluxului sanguin cerebral și oxigenarea
germinale până la al patrulea ventricul poate deveni un
cerebrală secundară cresc pe măsura dezvoltării
mecanism de protecție pentru creier cu scopul de a
embrionare. Odată cu scoaterea placentei din circulația
preveni leziuni tisulare ulterioare. De asemenea,
fetală, copilul fiind expus la mediul exterior, circulația
cheagurile și arahnoidita secundară în apeductul Sylvius
lui trebuie să facă față necesarului de oxigen de două
pot produce lărgirea ventriculară și hidrocefalia
până la de trei ori mai mare decât cel furnizat anterior la
progresivă [6]. Principala zonă din creier care primește
nivel intrauterin. Fluxul cerebral descrește în decursul
cea mai mare cantitate de sânge, înainte de
32 de
primelor două ore de la naștere și rămâne scăzut pentru
săptămâni de gestație, este nucleul caudat, care are o
aproximativ 24 de ore. Ulterior, fluxul sanguin crește
vascularizație delicată, complexă și care permite un
ușor, totuși, disproporționat cu presiunea sanguină,
metabolism local crescut cu scopul de a asista evoluția
densitatea sanguină și nivelul de oxigenare, expunând
celulelor neuronale și gliale să prolifereze, să se
CP la riscuri crescute. Creșterea presiunii fluxului
diferențieze și să migreze către structuri ulterioare [7].
sanguin cerebral poate deveni periculos de mare în
timpul hipercapniei la copii cu insuficiență respiratorie,
Stadializarea IVH
devenind un factor etiopatogenic pentru IVH
[3].
Deficiența de vitamină K (VKD) rămâne un factor
Prima clasificare a IVH a fost elaborată de Papile în
ubicuitar pentru IVH. Clasificată în VKD cu debut
concordanță cu neuroimagistica CT și extrapolată la
timpuriu, în timpul primelor 24 de ore, VKD clasică, cu
ultrasonografia craniană: gradul 1 - hemoragia matricei
evoluție într-un interval de la 1 până la 7 zile de la
germinale, gradul 2 - IVH fără dilatare ventriculară,
naștere și VKD cu debut tardiv având cel mai mare risc
gradul 3 - IVH cu dilatare ventriculară și gradul 4 -
între
3 și
8 săptămâni de perioadă postgestațională.
IVH extinsă în parenchimul cerebral adiacent
Aceasta se întâmplă datorită lipsei profilaxiei neonatale
ventriculilor [8]. Volpe și colab., pe baza descoperirilor
cu vitamina K și a alimentației exclusiv la sân. VKD cu
anatomo-patologice, au sugerat că gradul IV de IVH ar
debut tardiv este de obicei asociată cu hemoragia
trebui menționat separat, deoarece, cel mai adesea, se
intracraniană, fiind situate în zona subdurală (40%) cu
asociază cu leziuni parenchimatoase. Sistemul de
o mai mică contribuție atribuită IVH (10%). Terapia cu
grading Volpe este descris într-o manieră procentuală:
vitamina K poate rezolva hemoragia în decursul
gradul 1 - fără IVH sau IVH care ocupă sub 10% din
minutelor. Detectarea timpurie a semnelor neurologice
aria ventriculară pe secțiune parasagitală; gradul
2 -
împreună cu investigații de neuroimagistică ar trebui să
IVH ocupând între 10 și 50% din aria ventriculară pe
devină obligatorie: ultrasonografia rapidă este un test de
secțiune parasagitală; gradul 3 - IVH ocupând mai mult
screening eficient, combinat cu teste RMN sau CT, în
de
50% din suprafața ventriculară, pe o secțiune
special în cazurile cu RMN echivoc [4]. În fiecare sarcină
parasagitală. Infarctul venos periventricular hemoragic
cu risc, se folosesc diferiți agenți farmacologici cu scopul
ar trebui menționat separat și nu atribuit, în acest caz,
de a scădea contractilitatea uterină, cum ar fi
vreunui grad - cum ar fi gradul IV [9].
indometacinul, un inhibitor de cicloxigenază care
blochează
conversia
acidului
arachidonic
în
Detecția, evaluarea și cuantificarea IVH
prostaglandine. Indometacinul ar traversa bariera
placentară și ar inhiba sinteza prostaglandinelor în
Electroencefalografia cu amplitudine integrată
interiorul corpului fetal. Riscul de IVH sever conform
(aEEG) interpretată de cel puțin doi neonatologi
stadializării Papile - gradul III și IV - a fost semnificativ
experimentați în examinarea EEG ar trebui efectuată de
mai mare la copiii a căror mame au primit tocoliză cu
două ori pe săptămână, începând cel mai devreme la 48
indometacin, acesta fiind asociat cu enterocolita
de ore de la naștere, cu scopul de a evalua continuitatea
ulceronecrotică,
displazia
bronhopulmonară și
și ciclicitatea undelor cerebrale la un stadiu foarte
mortalitatea neonatală crescută [5].
timpuriu, cât și detecția perioadelor convulsive foarte
scurte. În IVH severe, aEEG tipic poate depista un tipar
Patologie
de fundal discontinuu, o lipsă a ciclurilor somn-veghe și
o mare probabilitate pentru activitatea convulsivă.
În unele cazuri, hemoragia cerebrală la copii este
Această investigație ar trebui efectuată permanent, în
limitată la zona subependimară a ventriculilor laterali, și
secția de terapie intensivă neonatală. Unii autori
dacă evoluția progresează, implicarea ulterioară ar fi
efectuează ultrasonografie cerebrală cu un transductor
92
Ionescu et al
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
GENERAL REVIEW
de 8 MHz, la 7 zile de la data nașterii, chiar între 1-4
studii sugerează utilizarea factorului VII în prevenirea
săptămâni până la externarea pacientului din secția de
IVH, fără creșterea ulterioară a riscului pentru
neonatologie. În plus, gradele III și IV de IVH ar trebui
coagulopatie intravasculară diseminată sau embolie
evaluate cu rezonanță magnetică nucleară (RMN) la
pulmonară [13]. Profilaxia posturală pare, de asemenea,
vârsta corectată de 36 de săptămâni, cu consimțământ
să contribuie la o presiune scăzută intracraniană prin
parental anterior, având scopul de a permite detecția
reducerea celei jugulare. Menținerea capului copilului
timpurie a chisturilor porencefalice, hidrocefaliei
într-o poziție pe linia mediană pare să inducă un risc
persistente, involuției cerebeloase, ventriculomegaliei,
mai scăzut pentru IVH, față de o răsucire bruscă
leucomalaciei periventriculare și a depozitelor
cervicală către o parte, care poate cauza, uneori,
parenchimatoase de hemosiderină [10]. Împreună cu
obstrucția venei jugulare ipsilaterale și implicit creșterea
multe alte pericole ale CP, se pare că GMN devine un
presiunii sanguine intracraniene. Aplecarea corpului, cu
factor circumstanțial pentru IVH ca o afecțiune
capul pe un plan superior în repoziționare supină pare să
adăugată leziunilor secundare ale substanței albe și ale
fie mai sigură pentru o mai bună oxigenare cerebrală cu
ventriculomegaliei. În practica generală, IVH poate fi
o presiune scăzută craniană și în consecință reducerea
depistată atât supratentorial cât și cerebelos. Diferite
șanselor de a produce IVH [14]. Perfuziile rapide cu
tehnici de neuroimagistică și cuantificare volumetrică
lichide și repleția volemică accelerată ar trebui să fie
pot detecta un volum cerebelos scăzut cu leziuni
evitate pe măsură ce acestea implică un stres suplimentar
neuronale supratentoriale și IVH, ca expresie a efectelor
hemodinamic atât pentru inimă, cât și pentru creier.
ischemice și hipoxice asupra cerebelului, deopotrivă,
Viteza de repleție volemică circulatorie sau depleția nu
prin lărgirea de volum a ventriculului afectat unilateral
au fost un risc major, ci cantitatea sau volumul care a
cât și prin hipertensiune intracraniană [11]. Evaluarea
fost administrat sau recoltat [15]. Copiii care au avut
fluxului cerebral poate deveni folositoare în timpul
nevoie de ventilație mecanică și intubație și care au
perioadei neonatale imediate și în prima oră după
primit doze intermitente de morfină fără sedare au avut
naștere, prin tehnici de ultrasonografie Doppler sau
o incidență redusă a IVH, prognosticul neurologic
tehnologie NIRS, în prisma principiului Beer-Lamber
rămânând nemodificat [16]. Îngrijirea de rutină, cum ar
care se bazează pe cuantificarea absorbției cantității de
fi schimbarea scutecelor, hrănirea, băile fierbinți sau
lumină de către oxigenul sanguin, în virtutea faptului că
deschiderea ușilor incubatorului, recoltarea din călcâi
oferă posibilitatea recuperării imediate în cazul fluxului
pentru analize sau manipularea grosolană par să
sanguin sever afectat, dar și a reducerii costurilor de
determine vascularizația fină a creierului prematurului
nursing cu mai mult de 400%. Cu toate acestea, tehnica
să se supună riscului de ruptură, prin creșterea bruscă a
nu este încă foarte populară, fiind încă în evaluare în
volumului sanguin [17]. În general, în timpul perioadei
diferite centre neonatale de referință [12].
imediate antenatale, un tratament cu corticosteroizi
reduce riscul pentru IVH [18]. De asemenea, clamparea
Tratament
întârziată a cordonului ombilical poate ajuta profilaxiei
mai bune a IVH, în timp ce în timpul perioadei
Screeningul coagulopatiilor pare să îmbunătățească
postnatale
tratamentul
cuprinzând
adăugarea
supraviețuirea la CP, în special acelora care se găsesc în
surfactantului
[19],
termoreglarea
adecvată,
perioada de gestație dintre 23 și 26 de săptămâni. Unele
indometacinul profilactic
[20] și îngrijirea neonatală
atentă pot reduce semnificativ riscul pentru IVH la
prematuri.
Concluzie
Hemoragia intraventriculară rămâne un important
factor de risc pentru toți copiii cu un grad de
prematuritate și afecțiuni perinatale. Principalele sechele
rezultante după IVH rămân deficitul motor, afectarea
cognitivă ulterioară, slăbiciunea musculară și hipertonia
axială. În majoritatea cazurilor, aceste anomalii
hemoragice sunt rezultatul direct al manipulării
Figura 1. Aspect de ecografie transfontanelară a unei IVH
neonatale inadecvate, recoltării agresivede analize și
diagnosticată ca stadiul III și dilatație ventriculară dreaptă la
sânge de la nou-născuți. Tratamentul hemoragiilor
un nou-născut la 35 de săptămâni și 2 zile (colecție personală)
93
Cerebral Intraventricular Hemorrhage. A Gestational Pathological Event
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
intracerebrale în general și IVH în particular sunt o
electroencephalographic activity in preterm infants with
necesitate pentru inițierea imediată a acțiunilor, deoarece
intraventricular hemorrhage. Early Hum Dev.
o intervenție timpurie poate limita afectarea cognitivă și
2013;89(12):961-6.
motorie ulterioară a copilului. Având o incidență
11.
Tam EWY, Miller SP, Studholme C, Chau V, Glidden
ridicată, IVH păstrează de asemenea o rată înaltă de
D, Poskitt KJ, et al. Differential Effects of Intraventricular
mortalitate a nou-născuților.
Hemorrhage and White Matter Injury on Preterm
Cerebellar Growth. J Pediatr. 2011;158(3):366-71.
12.
Elser HE, Holditch-Davis D, Brandon DH. Cerebral
Refernițe
Oxygenation Monitoring: A Strategy to Detect
Intraventricular Hemorrhage and Periventricular
1.
Kwok MK, Yeung SLA, Leung GM, Mary Schooling
Leukomalacia.
Neuroprotective
Strateg.
C. Birth weight and adult cardiovascular risk factors
2011;11(3):153-9.
using multiple birth status as an instrumental variable
13.
Dani C, Poggi C, Ceciarini F, Bertini G, Pratesi S,
in the British
1958 birth cohort. Prev Med P.
Rubaltelli FF. Transfusion Practice: Coagulopathy
2016;84:69-75.
screening and early plasma treatment for the prevention
2.
World Health Organization and UNICEF. Low
of intraventricular hemorrhage in preterm infants.
Birthweight: Country, Regional and Global Estimates.
Transfusion (Paris). 2009;49(12):2637-44.
14.
Schrod L, Walter J. Effect of Head-Up Body Tilt
publications/index_24840.html
Position on Autonomic Function and Cerebral
3.
Cooke RWI, Rolfe P, Howat P. Apparent cerebral
Oxygenation in Preterm Infants. Neonatology.
blood-flow in newborns with respiratory disease. Dev
2002;81(4):255-9.
Med Child Neurol.
1979;21(2):154-60.
15.
Hüning BM, Horsch S, Roll C. Blood sampling via
DOI:10.1111/j.1469-8749.1979.tb01596.x
umbilical vein catheters decreases cerebral oxygenation
4.
Volpe JJ. Intracranial Hemorrhage in Early Infancy -
and blood volume in preterm infants. Acta Pædiatrica.
Renewed Importance of Vitamin K Deficiency. Pediatr
2007;96(11):1617-21.
Neurol. 2014;50(6):545-6.
16.
Anand K, Hall RW, Desai N, Shephard B, Bergqvist
5.
Hammers AL, Sanchez-Ramos L, Kaunitz AM.
LL, Young TE, et al. Effects of morphine analgesia in
Antenatal exposure to indomethacin increases the risk of
ventilated preterm neonates: primary outcomes from the
severe
intraventricular
hemorrhage, necrotizing
NEOPAIN randomised trial. Te Lancet.
enterocolitis, and periventricular leukomalacia: a
2004;363(9422):1673-82.
systematic review with metaanalysis. Am J Obstet
17.
Gagnon RE, Leung A, Macnab AJ. Variations in
Gynecol. 2015;212(4):505.e1-505.e13.
Regional Cerebral Blood Volume in Neonates Associated
6.
Kenner C, Edds JW, Blackburn ST, Ditzenbeger GR.
with Nursery Care Events. Amer J Perinatol.
Neurologic system. In: Comprehensive neonatal care: an
2008;16(01):7-11.
interdisciplinary approach.
4th ed. St. Louis: W.B.
18.
Chawla Sanjay, Natarajan Girija, Rane Sharayu,
Saunders; 2007. p. 267-99.
Tomas Ronald, Cortez Josef, Lua Jorge. Outcomes of
7.
Bassan H. Intracranial Hemorrhage in the Preterm
extremely low birth weight infants with varying doses
Infant: Understanding It, Preventing It. Neurol
and intervals of antenatal steroid exposure. J Perinat
Newborn Infant. 2009;36(4):737-62.
Med. 2010;38(4):419.
8.
Papile LA, Burstein J, Burstein R, Koffler H. Incidence
19.
Walti H, Paris-Llado J, Egberts J, Brand R, Bevilacqua
and evolution of subependymal and intraventricular
G, Gardini F, et al. Prophylactic Administration of
hemorrhage: A study of infants with birth weights less
Porcine-Derived Lung Surfactant Is a Significant Factor
than 1,500 gm. J Pediatr. 1978;92(4):529-34.
in Reducing the Odds for Peri-Intraventricular
9.
Volpe J. Intracranial hemorrhage: germinal matrix -
Haemorrhage in Premature Infants. Neonatology.
intraventricular hemorrhage. In: Neurology of the
2002;81(3):182-7.
Newborn. 5th ed. Philadelphia, PA: Elsevier Saunders;
20.
Ment LR, Vohr BR, Makuch RW, Westerveld M,
2008. p. 492-581.
Katz KH, Schneider KC, et al. Prevention of
10.
Sohn JA, Kim H-S, Lee EH, Lee J, Lee JA, Choi CW,
intraventricular hemorrhage by indomethacin in male
et al. Developmental change of amplitude-integrated
preterm infants. J Pediatr. 2004;145(6):832-4.
94
Ionescu et al
GENERAL REVIEW
NEFRECTOMIA TRANSPERITONEALĂ VS. RETROPERITONEALĂ
PENTRU CARCINOMUL RENAL: O REVISTĂ GENERALĂ
Cristian Bogdan Rusu1, Bogdan Ovidiu Feciche1, Lilian Gorbatai1, Tiberiu Botezan1,
Bogdan Bumbuluț2, Andrei Bumbuluț3, Rumelia Koren4
1Secția de Urologie, Spitalul Județean de Urgență Satu Mare, 2Secția de Urologie, Spitalul Clinic Județean de Urgență
Sibiu, 3Facultatea de Medicină, Universitatea de Medicină și Farmacie „Iuliu Haţieganu”, Cluj Napoca, 4Spitalul
Hasharon, afiliat la Facultatea de Medicină Sackler, Universitatea din Tel Aviv
Adresa pentru corespondență:
Dr. Cristian Bogdan Rusu
Secția Urologie, Spitalul Județean de Urgență Satu Mare
Strada Prahova nr 1, Satu Mare, județul Satu Mare, România
E-mail:cbrusu@yahoo.com
Primit: 20.03.2016
Acceptat: 29.04.2016
Med Con June 2016 Vol 11, No 2, 95-97
Rezumat
nefrectomie radicală laparoscopică retroperitoneală,
nefrectomie parțială laparoscopică transperitoneală,
Carcinomul renal cu celule clare este cel mai
nefrectomie parțială laparoscopică retroperitoneală,
frecvent tip de cancer renal la adulți. Rezecţia
durata internării, pierdere de sânge estimată, timp
chirurgicală - radicală sau parțială - a rinichiului rămâne
operator
singurul tratament curativ cunoscut pentru carcinomul
renal cu celule clare localizat. Rezecția laparoscopică
Introducere
radicală sau parțială poate fi efectuată fie prin abord
transperitoneal, fie retroperitoneal, fiecare dintre
Carcinomul cu celule renale
(CCR) reprezintă
aborduri având propriile sale avantaje și limitări, fără a
aproximativ 3% din toate cazurile de cancer, fiind cel
putea trage concluzii definitive în ceea ce privesc
mai frecvent tip de cancer renal la adulți, cu o proporție
diferențele obiective în rezultate. Studiile sugerează că
de 90-95% din neoplasmele care provin din rinichi.
abordarea retroperitoneală are un timp mai scurt pentru
Având o creștere medie de 2-3% pe an și cea mai mare
controlul vascular renal și un timp operator mai scurt
incidență în țările occidentale, ratele de incidență ale
decât cea transperitoneală. La pacienții selectați în mod
CCR au crescut constant pe parcursul a trei decenii ale
corespunzător, precum cei cu tumori renale localizate
secolului al XX-lea, în cea mai mare parte din lume [1].
posterior, abordarea retroperitoneală poate fi mai rapidă
Rezecția chirurgicală a rinichiului
- nefrectomie
și la fel de sigură în comparație cu abordarea
radicală
(NR), sau a tumorii - nefrectomie parțială
transperitoneală. La pacientul cu obezitate extremă,
(NP), rămâne singurul tratament curativ cunoscut
abordarea retroperitoneală are tendința de a avea
pentru carcinomul localizat cu celule renale. În mod
avantaje în ceea ce privește pierderea de sânge, durata
tradițional, NR sau NP a fost realizată folosind
operatorie, greutatea specimenului, rata de conversie
abordarea chirurgicală deschisă, printr-o incizie mare în
deschisă și durata internării.
flanc, intervenție asociată cu durere și morbiditate
Cuvinte cheie: carcinom renal cu celule clare,
substanțiale. Clayman și colab. [2] au efectuat în 1991
nefrectomie radicală laparoscopică transperitoneală,
prima
nefrectomie
radicală
laparoscopică
Transperitoneal vs. Retroperitoneal Laparoscopic Nephrectomy for Renal Cell Carcinoma
95
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
transperitoneală (NRLT). După 1991, NRLT a câștigat
transperitoneală necesită o mobilizare considerabilă
o acceptare tot mai mare la nivel mondial datorită
pentru a avea acces la hilul renal, în timp ce abordarea
beneficiilor sale în ceea ce privește recuperarea
retroperitoneală oferă acces direct și rapid la hilul renal.
pacientului și a morbidității perioperatorii. Mai multe
Această meta-analiză [10] indică faptul că la pacienții cu
studii pe termen lung au arătat că rezultatele NRLT sunt
tumori renale localizate posterior, NRLR poate fi mai
similare cu cele ale chirurgiei deschise [3-6].
rapidă și la fel de sigură în comparație cu NRLT. Un
NR, sau NP laparoscopică, pot fi realizate fie
avantaj al accesului retroperitoneoscopic pare a fi un
transperitoneal
(NRLT, NPLT), fie prin abord
timp total operator mai scurt [7]. Abordul transperitoneal
retroperitoneal (NRLR, NPLR), fiecare dintre ele având
trebuie să fie ales în funcție de mărimea tumorii și
propriile sale avantaje și limitări, neputând fi trase
localizare, pentru a minimaliza leziunile vasculare [11].
concluzii definitive în ceea ce privesc diferențele
În ceea ce privește timpul operator pentru NP, datele
obiective în rezultate. Acesta este motivul pentru care
colectate
[10] au arătat că timpul de operare a fost
am realizat o revizuire generală a literaturii disponibile,
semnificativ mai scurt în nefrectomia parțială
pentru a compara rezultatele celor două abordări.
laparoscopică retroperitoneală (NPLR) decât nefrectomia
parțială laparoscopică transperitoneală (NPLT). Timpul
Metode
de ischemie caldă (WIT) pentru NP nu a arătat nicio
diferență semnificativă între NPLT și NPLR.
A fost efectuată o căutare în biblioteca MEDLINE
Datele rezultate din studiile care au raportat
pentru a identifica studiile relevante; termenii căutării
pierderea de sânge estimat (EBL) pentru NR, nu au
au fost „(nefrectomie laparoscopică) [Titlu/Abstract] ȘI
arătat nicio diferență semnificativă între NRLR și
(transperitoneală
SAU retroperitoneală)
[Titlu/
NRLT, respectiv între NPLR și NPLT [10,11-20].
Abstract].” Articolele au fost căutate, de asemenea,
Pentru variabilele postoperatorii, nu au existat
folosind funcția „articolele conexe”. Listele de referință
diferențe semnificative între NRLT și NRLR în LOS
ale articolelor obținute au fost căutate manual pentru a
sau timpul până la primul aport oral. Mai multe studii
identifica articole conexe. Ultima dată pentru această
au raportat LOS pentru NP cu o diferență semnificativă
căutare a fost 28 februarie 2016.
care favorizează NRLR. Nu a fost găsită nicio diferență
semnificativă în necesitățile de analgezice
(morfină,
Rezultate
petidină,
medicamente antiinflamatoare
non-
steroidiene) între NRLT și NRLR, precum și între
Nefrectomia parțială laparoscopică transperitoneală
NPLT și NPLR [10].
și retroperitoneală furnizează rezultate chirurgicale și
Rata de complicații chirurgicale a fost semnificativ
funcționale comparabile [7]. Deși ambele nefrectomii
mai mică în NRLR decât în NRLT și de asemenea,
radicale laparoscopice transperitoneală si retroperitoneală
semnificativ mai mică în NPLR decât în NPLT. Nu au
sunt opțiuni fezabile, NRLR este asociată cu semnificativ
existat diferențe semnificative între NRLR și NRLT în
mai puțină durere, necesități mai reduse de analgezic,
rata complicațiilor postoperatorii, rata conversiei
durată mai scurtă de spitalizare (LOS) și convalescență
deschise, sau rata transfuziei. Complicațiile generale,
scurtă, în comparație cu NRLT [8].
rata complicațiilor intra-operatorii, rata complicațiilor
Atât NRLT cât și NRLR sunt sigure, fezabile și
postoperatorii, sau rata de conversie deschisă, nu au avut
eficiente pentru managementul chirurgical al tumorilor
diferențe semnificative între NPLT și NPLR [10].
complexe localizate, dar NRLT oferă spațiu operativ
În ceea ce privesc variabilele oncologice nu au existat
mai mare, cu o mai bună expunere; NRLR promovează
diferențe semnificative între NRLT și NRLR în rata
o mai bună recuperare postoperatorie a pacienților [9].
generală de recurență, rata de recidivă locală, sau rata de
O meta-analiză [10], care a inclus 12 studii care au
recurență la distanță; pentru NP nu au existat diferențe
comparat NRLR cu NRLT și șase studii care au
semnificative între NPLT și NPLR [10].
comparat NPLR cu NPLT, demonstrează în ceea ce
La pacientul cu obezitate extremă, NRLR a avut
privesc variabilele perioperatorii că timpul operator
tendința de a avea avantaje în ceea ce privește EBL,
pentru NR a fost puțin mai scurt în NRLR decât în
durata operatorie, greutatea specimenului, rata de
NRLT; timpul pentru controlul arterei renale a fost
conversie deschisă și durata spitalizării. NRLR oferă
semnificativ mai mare în NRLT decât NRLR, iar timpul
acces direct la hilul renal și evită panusul și grăsimea
de control al venei renale a fost semnificativ mai mare în
voluminoasă intra-abdominală întâlnite în timpul
NRLT decât în NRLR, deoarece abordarea
NRLT [21].
96
Rusu et al
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
GENERAL REVIEW
Referințe
radical nephrectomy: a comparative study. Int J Urol.
2009;16(3):263-7.
1.
Mathew A, Devesa SS, Fraumeni JF Jr, Chow WH.
12.
Tsujihata M, Nonomura N, Momohara C et al.
Global increases in kidney cancer incidence,
1973-
Clinical
experience
with laparoscopic radical
1992. Eur J Cancer Prev. 2002;11:171-8.
nephrectomy for renal cell carcinoma. Urol Int.
2.
Clayman RV, Kavoussi LR, Soper NJ et al. Laparoscopic
2008;81:301-5.
nephrectomy: initial case report. J Urol. 1991;146:278-82.
13.
Xu ZL, Wang LH, Chen W et al. Transperitoneal
3.
Burgess NA, Koo BC, Calvert RC et al. Randomized
versus retroperitoneal laparoscopic radical nephrectomy:
trial of laparoscopic v open nephrectomy. J Endourol.
a comparison of clinical outcomes. Acad J Second
2007;21:610-3.
Military Med Univ. 2011;32:938-41.
4.
Permpongkosol S, Chan DY, Link RE et al. Long-term
14.
Desai MM, Strzempkowski B, Matin SF et al.
survival analysis after laparoscopic radical nephrectomy.
Prospective randomized comparison of transperitoneal
J Urol. 2005;174:1222-5.
versus retroperitoneal laparoscopic radical nephrectomy. J
5.
Portis AJ, Yan Y, Landman J et al. Long-term followup
Urol. 2005;173:38-41.
after laparoscopic radical nephrectomy. J Urol.
15.
Negoro H, Shiraishi Y, Sugino Y et al. Laparoscopic
2002;167:1257-62.
radical nephrectomy for renal cell carcinoma at Kobe
6.
Luo JH, Zhou FJ, Xie D et al. Analysis of long-term
City General Hospital. Acta Urol Jpn. 2005;51:369-
survival in patients with localized renal cell carcinoma:
72.
laparoscopic versus open radical nephrectomy. World J
16.
Nambirajan T, Jeschke S, Al-Zahrani H et al.
Urol. 2010;28:289-93.
Prospective, randomized controlled study: transperitoneal
7.
Marszalek M, Chromecki T, Al-Ali BM, Meixl H,
laparoscopic
versus
retroperitoneoscopic
radical
Madersbacher S, Jeschke K, Pummer K, Zigeuner R.
nephrectomy. Urology. 2004;64:919-24.
Laparoscopic partial nephrectomy: a matched-pair
17.
Nadler RB, Loeb S, Clemens JQ et al. A prospective
comparison of the transperitoneal versus theretroperitoneal
study of laparoscopic radical nephrectomy for T1 tumors
approach. Urology. 2011;77(1):109-13.
- is transperitoneal, retroperitoneal or hand assisted the
8.
Garg M, Singh V, Sinha RJ, Sharma P. Prospective
best approach? J Urol. 2006;175:1230-4.
randomized comparison of transperitoneal vs
18.
Jung MH, Tae HK, Won YC et al. Comparison of
retroperitoneal
laparoscopic simple nephrectomy.
techniques for laparoscopic radical nephrectomy in a
Urology 2014;84(2):335-9.
single center: transperitoneal vs. retroperitoneal vs. hand-
9.
Pu X, Xu Z, Liu J, Zheng X, Li D, Luo Y, Xian Z.
assisted. Korean J Urol. 2009;50:675-81.
Clinical efficacy of transperitoneal versus retroperitoneal
19.
Ha US, Hwang TK, Kim YJ et al. Comparison of
laparoscopic partial nephrectomy for renal tumors with
oncological
outcomes
of
transperitoneal
and
R.E.N.A.L score over 7. Nan Fang Yi Ke Da Xue Xue
retroperitoneal laparoscopic radical nephrectomy for the
Bao/Journal of Southern Medical University.
management of clear-cell renal cell carcinoma: a multi-
2014;34(12):1818-21.
institutional study. BJU Int. 2011;107:1467-72.
10.
Fan X, Xu K, Lin T, Liu H, Yin Z, Dong W, Huang
20.
Okegawa T, Noda H, Horie S et al. Comparison of
H, Huang J. Comparison of transperitoneal and
transperitoneal
and retroperitoneal laparoscopic
retroperitoneal laparoscopic nephrectomy for renal cell
nephrectomy for renal cell carcinoma: a single-center
carcinoma: a systematic review and meta-analysis. BJU
experience of 100 cases. Int J Urol. 2008;15:957-60.
Int. 2013;111(4):611-21.
21.
Berglund RK, Gill IS, Babineau D, Desai M, Kaouk
11.
Taue R, Izaki H, Koizumi T, Kishimoto T, Oka N,
JH. A prospective comparison of transperitoneal and
Fukumori T, Takahashi M, Kanayama HO.
retroperitoneal laparoscopic nephrectomy in the extremely
Transperitoneal versus retroperitoneal laparoscopic
obese patient. BJU Int. 2007;99(4):871-4.
97
Transperitoneal vs. Retroperitoneal Laparoscopic Nephrectomy for Renal Cell Carcinoma
Medical Connections/Conexiuni Medicale
Declaraţia de conflict de interese
Medical Connections/Conexiuni Medicale (Med Con) solicită tuturor autorilor şi recenzorilor să declare
orice conflict de interese care ar putea interveni în contribuţiile lor.
Conflictul de interese pentru un anumit manuscris există atunci când un participant în procesul de
recenzie inter pares (peer review) şi de publicare - autor, referent, sau editor - are legături cu activităţi care
l-ar putea influenţa necorespunzător pe el sau judecata lui, indiferent dacă aceasta este sau nu afectată.
Relaţiile financiare cu industria medicală, de exemplu prin muncă salarială, consultanţă, deţinere de
acţiuni, onorarii, testimoniale ca şi expert, fie direct, fie prin intermediul familiei, sunt de obicei considerate
a fi cele mai importante conflicte de interese. Cu toate acestea, pot apărea conflicte din alte motive, cum ar
fi relaţiile personale, concurenţa academică şi implicarea intelectuală.
Încrederea publicului în procesul de revizuire inter pares şi credibilitatea articolelor publicate depinde
în parte de cât de bine este administrat posibilul conflict de interese în timpul redactării, recenziei inter
pares şi a luării deciziilor editoriale. Părtinirea poate fi de multe ori identificată şi eliminată prin atenţia
crescută asupra metodelor ştiinţifice şi concluziilor lucrării. Relaţiile financiare şi efectele lor sunt mai uşor
de identificat decât alte conflicte de interese. Participanţii la peer review şi în procesul de publicare trebuie
să-şi dezvăluie posibilele conflictele de interese, iar informaţiile trebuie să fie puse la dispoziţie, astfel încât
şi alţii să poată aprecia aceste efecte pentru ei înşişi.
Autori: atunci când trimit un manuscris sau o scrisoare, autorii sunt responsabili pentru recunoaşterea
şi divulgarea conflictelor financiare şi altor conflicte de interese care ar putea să le influenţeze activitatea. Ei
trebuie să recunoască în manuscris orice sprijin financiar pentru activitate, precum şi orice alte legături
financiare sau personale în munca lor.
Recenzorii: evaluatorii externi inter pares trebuie să dezvăluie editorilor orice conflicte de interese care
le-ar putea părtini opiniile asupra manuscrisului şi ar trebui să se recuze de la recenzia anumitor manuscrise
în cazul în care cred că este oportun. Editorii trebuie să fie conştienţi de posibilele conflicte de interese ale
recenzorilor în interpretarea recenziilor şi trebuie să judece pentru ei dacă recenzorul ar trebui să fie recuzat.
Recenzorii nu trebuie să utilizeze informaţiile în munca lor, înainte de publicare, pentru a-şi promova
propriile interese.
Titlul manuscrisului: _ _______________________________________________________
Declar că nu există conflict de interese
Declar că există următoarele conflicte de interese potenţiale:
_ _________________________________________________________________________
_ _________________________________________________________________________
_ _________________________________________________________________________
_ _________________________________________________________________________
_ _________________________________
_ _________________________________
Nume
Semnătura/Data
Vă rugăm trimiteţi acest formular semnat pe fax sau mail la sediul editorului Med Con.
Fax: +40-261-710456
Email: colmedsm@gmail.com
GENERAL REVIEW
TRATAMENTUL CU LAPTE UMAN AL AFECȚIUNILOR ADULȚILOR
Mihaela N. Niță
Asociația Consultanților în Lactație din România
Adresa pentru corespondență:
Mihaela N. Niță MD, IBCLC
E-mail: mihaelanita11@gmail.com
Primit: 14.05.2016
Acceptat: 01.06.2016
Med Con June 2016 Vol 11, No 2, 99-102
Rezumat
anumite circumstanțe, chiar și pentru afecțiunile
adulților [2]. Utilizarea laptelui uman donat poate fi
Alăptarea este metoda standard de hrănire a
împărțită în nutrițională, medicinală, terapeutică și
sugarilor și a copiilor mici. Atunci când laptele propriei
preventivă. În practică, laptele uman donat poate servi
mame nu este disponibil, prima alegere, în cazul în care
mai multe scopuri aceluiași beneficiar [3].
este disponibilă, este laptele uman donat. Băncile de
Laptele matern poate fi considerat un sistem
lapte prioritizează eliberarea laptelui uman donat.
dinamic biologic specio-specific, care conține factori
Printre indicațiile folosirii laptelui uman sunt și adulții
specifici bioactivi și imunomodulatori: hormoni
cu diversele afecțiuni medicale. În cazul lor, folosirea
gastrointestinali, imunoglobuline, lactoferină, lizozim,
laptelui uman are scop terapeutic, nutrițional, preventiv
oligozaharide, nucleotide, factori de creștere, enzime,
și paleativ. Scopul articolului este de a sumariza
antioxidanți și componente celulare care asigură apărarea
concluziile articolelor de specialitate privind utilizarea
gazdei împotriva infecțiilor, modulează răspunsul imun
laptelui uman de către adulți.
și modifică flora bacteriană intestinală [4,5].
Cuvinte cheie: lapte uman, lapte uman donat,
HAMLET, celule stem
Folosirea laptele matern donat pentru
adulți
Introducere
Studiile care s-au concentrat asupra variațiilor
Este recunoscut faptul că alăptarea este metoda
culturale din domeniul alăptării susțin că, din punct de
standard de hrănire a nou-născuților la termen, exclusiv
vedere istoric, nu este neobișnuit ca femeile să alăpteze
până la vârsta de 6 luni, urmată de diversificare împreună
persoanele în vârstă din familiile lor [6]. Tema alăptării
cu alăptarea, până la vârsta de 2 ani și peste. Beneficiile
vârstnicilor a fost utilizată în artă. De exemplu, pânza
alăptarii pentru nou-născuții sănătoși la termen și
„Roman Charity”, prezentată în Rijkmuseum din
mamele lor sunt bine cunoscute. Laptele propriei mame
Amsterdam, arată modul în care mama își alăptează tatăl
este prima alegere pentru toți nou-născuții, inclusiv
aflat în închisoare și condamnat la moarte prin
pentru prematuri, dar atunci când acesta nu este
înfometare.
disponibil sau nu este în cantitate suficientă, laptele
Baza științifică a acestei practici a fost, până nu
matern donat este următoarea opțiune [1].
demult, necunoscută.
Laptele matern nu este numai modalitatea de
Studiul elaborat de o echipă de cercetători de la
hrănire optimă pentru nou-născuți și sugari, dar poate fi
Universitatea din Gothenburg și Lund, Suedia, a dorit
utilizat și în scop profilactic și terapeutic împotriva
să investigheze activitatea antimicrobiană a laptelui
multor boli ale sugarilor și copiilor de vârstă mică și, în
uman. Studiul a constatat că laptele matern a ucis
Treatment with Human Milk for Adults Conditions
99
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
celulele canceroase in vitro, proprietate datorată unei
laptele bovinelor, cabalinelor și porcinelor. Concluzia a
proteine multimerice - alfa lactalbumina.
fost că formarea naturală a complexelor HAMLET este
Această proteină, împreună cu un acid gras, acidul
unică pentru cazeina din laptele uman, care are cel mai
oleic, formează compusul HAMLET (Human Alpha-
mare conținut de acid oleic [7].
lactalbumin Made Lethal to Tumour cells). Acest proces
Laptele uman donat poate ajuta la recolonizarea
are loc după tratarea laptelui uman în cazeină la pH
tractul digestiv la persoanele care au avut reacții adverse
scăzut [7,8]. Aciditatea gastrică a copiilor promovează
gastro-intestinale după tratamentele anticanceroase
formarea de HAMLET. Acest mecanism poate contribui
convenționale. Acesta poate proteja mucoasa
la efectul anticancerigen al alăptării împotriva tumorilor
gastrointestinală de agresiuni ulterioare [10].
din perioada copilăriei [9]. Experimentele de laborator
Folosirea laptelui uman donat poate fi benefică
au demonstrat că acest compus ucide 40 de tipuri de
adulților cu cancer și alte afecțiuni medicale.
celule canceroase. Activitatea anticancerigenă afectează
Cantități mici de lapte uman donat pot îmbunătății
celulele embrionare, dar nu și celulele mature [8,10].
nivelul de IgA la persoanele cu imunodeficiențe precum
Pe baza acestei descoperiri, compusul HAMLET a
cei care au urmat tratamente, cum ar fi radioterapia și
fost utilizat la pacienți având cancer de vezică urinară.
chimioterapia [10].
Excreția în urină a celulelor canceroase moarte a fost
Laptele matern este cea mai bogată sursă disponibilă
observată de fiecare dată când s-a utilizat HAMLET,
de IgA fiind folosită cu succes pentru sugarii, copiii și
ceea ce duce la speranțe pentru dezvoltarea de tratamente
adulții cu imunodeficiențe [15].
viitoare pentru cancerul vezicii urinare [8,11].
Deficitul de IgA este asociat cu mortalitate ridicată
Pentru că tumorile cerebrale maligne reprezintă o
(42% la 120 de zile) după transplantul hepatic. Cele
provocare majoră terapeutică, studiul efectuat de Fischer
mai multe decese au fost corelate cu infecțiile intestinale.
și colab. a testat administrarea intratumorală a
Laptele matern sau laptele uman donat au efecte
HAMLET, observând prelungirea perioadei de
benefice datorită protecției împotriva translocației
supraviețuire într-un model de xenogrefă de glioblastom
microbiene și împotriva infecțiilor enterice [16].
uman prin inducerea apoptozei selective a celulelor
Într-un studiu, doi pacienți cu deficit de IgA au
tumorale. Terapia cu HAMLET a redus volumul
primit lapte matern oral, timp de 10 zile perioperator
tumorii și semnele tardive de hipertensiune
transplantului hepatic. Ambii pacienți au avut o
intracraniană. In vivo, HAMLET a cauzat apoptoza
perioadă postoperatorie fără infecții, cu niveluri crescute
celulelor tumorale, dar nu și a țesutului cerebral adiacent
de IgA. Cercetătorii au ajuns la concluzia că laptele
și a astrocitelor și nu a avut efecte secundare toxice
matern poate fi utilizat la pacienții cu deficit de IgA
aparente. Studiul a identificat că HAMLET este un nou
după transplantul hepatic pentru a reduce complicațiile
candidat în terapia împotriva cancerului pentru
infecțioase în perioada postoperatorie [16].
controlul progresiei glioblastoamelor [12].
Laptele uman donat este folosit și pentru regenerarea
Moartea celulară programată ca răspuns la HAMLET
hepatică. O unitate de transplant hepatic din orașul
este independentă de caspaze, p53 și Bcl-2, chiar dacă
Oklahoma folosește laptele uman donat pentru tratarea
HAMLET activează un răspuns apoptotic. Utilizarea
pacienților adulți cu transplant. Laptele uman donat este
altor mecanisme ale apoptozei permite ca HAMLET să
infuzat în câmpul operator și în tractul intestinal în
aibă o activitate care nu este afectată de strategiile anti-
timpul intervenției chirurgicale. Pacientul primește apoi
apoptotice prezente în celulele tumorale [13].
doze orale zilnice de lapte uman donat pentru a
Un studiu recent realizat de Zang și colab. a
îmbunătăți nivelul de IgA. Chirurgii au observat că acesta
investigat activitatea anti-cancerigenă a complexului
a îmbunătățit statusul imunologic al pacienților și că au
format de alfa-lactalbumină și acidul oleic (compusul
apărut mai puține cazuri de reject al transplantului [10].
HAMLET). Prin folosirea tehnicilor moderne,
Relația dintre alăptare și rezultate mai bune post-
inovatoare, studiul a ajuns la concluzia că HAMLET
transplant a fost stabilită în cazul copiilor alăptați care
afectează stabilitatea citoscheletului, motilitatea celulară,
primesc transplant renal de la mamele lor [17].
inhibă ADN-ul, lipidele și sinteza adenozin trifosfatului,
Laptele matern promovează maturarea tractului
ceea ce duce la stres celular și activarea apoptozei,
gastrointestinal și protejează sugarii împotriva bolilor
stabilindu-se astfel bazele teoretice pentru acțiunea sa cu
gastrointestinale.
posibilități de utilizare în terapia cancerului [14].
Un articol a publicat cazul unui bărbat de 24 de ani,
Studiul realizat de Petterson și colab. a avut ca scop
care a avut două episoade de reflux gastro-esofagian
cercetarea prezenței compușilor HAMLET-like și la alte
sever cu absența toleranței digestive chiar și pentru
specii. Echipa de cercetători a studiat laptele uman,
sărurile de rehidratare. După administrarea de lapte
100
Niță et al
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
GENERAL REVIEW
matern sau lapte uman donat starea lui și toleranța
donat primită de către pacienții adulți cu cancer de la 11
digestivă au fost mult îmbunătățite [18].
bănci de lapte membre ale Asociației de Bănci de Lapte
Laptele matern conține mai mulți compuși care pot
din America de Nord, în 2005, a fost scăzută, între 4%
explica evoluția cazului prezentat mai sus. Acești
și 4,5% din laptele uman donat total din acel an [19].
compuși sunt factori de creștere, factori antiinflamatori
Prezența celulelor stem în laptele matern a fost
și peptide opioid-like. Factorul de creștere epidermal
descoperită de dr. Cregan în 2007. Aceste celule au un
(EGF) este una dintre cele mai active peptide din laptele
marker, nestina, caracteristic celulelor stem. Prezența
uman. Acesta crește mitoza și proliferarea celulelor
unor astfel de celule indică faptul că laptele poate deveni
epiteliale din plămâni, din sistemul gastro-intestinal și
o sursă accesibilă, non-invazivă de celule stem, care pot
din alte țesuturi de origine epidermică, accelerează
fi utilizate atât în cercetarea biologiei glandei mamare,
vindecarea rănilor de la nivelul corneei și a altor țesuturi
cât și în cercetarea biologiei celulelor stem [20].
de origine epidermică. În plus, EGF inhibă secreția
Celulele stem mamare sunt responsabile de
stimulată de histamină a acidului gastric, contribuind
schimbările prin care trece glanda mamară în timpul
astfel la vindecarea ulcerelor gastrice [18].
lactației. Ele sunt prezente în laptele matern și sugarii le
Factorii de creștere din laptele uman stimulează
ingeră. Aceste celule sunt celule stem pluripotente și se
producerea de mucus la nivelul stomacului și duodenului,
pot diferenția nu numai în celule specifice din glanda
un efect protector al mucoasei intestinale dependent de
mamară, dar și în alte tipuri de celule, cum ar fi celulele
doză. EGF este stabil în timpul pasteurizării, în prezența
neuronal-like. Ele pot fi folosite în „terapiile de înlocuire
acidului și este rezistent la digestia enzimatică. În cultură
celulară” pentru pacienții care suferă de leziuni la nivelul
tisulară, EGF stimulează sinteza ADN-ului în celulele
sistemului nervos central, cu posibile aplicații în
care s-au oprit din creștere [18].
medicina regenerativă și în boli, cum ar fi diabetul și
Proprietățile anti-inflamatorii ale laptelui uman
boala Parkinson [21].
sunt importante în limitarea răspunsurilor imune
Rezultatele studierii componentelor laptelui matern
pentru a reduce inflamația.
nu încetează să ne surprindă.
Peptidele opioid-like, prostaglandinele și compușii
Implicațiile acestor descoperiri depășesc nutriția
mucin-like au efect citoprotector asupra mucoasei
sugarilor și a copiilor mici, ajungând până la efectele
gastro-intestinale, care este mai puțin expusă la factorii
terapeutice asupra afecțiunilor medicale ale adulților.
agresivi. Este posibil ca acești compuși să acționeze
într-o manieră sinergică.
Laptele matern ar putea intra în cadrul variantelor
Referințe
terapeutice ale bolilor gastro-intestinale grave ale
adulților [18].
1. American Academy of Paediatrics. Breastfeeding and use
Laptele matern poate fi utilizat pentru a îmbunătăți
of human milk. Pediatrics. 2012;129:e827-41.
calitatea vieții pacienților cu cancer și pentru a atenua
2. Tully MR. Recipient Prioritization and Use of Human
efectele secundare ale medicației. Într-un studiu în care
Milk in the Hospital Setting. Journal of Human
laptele matern a fost utilizat pentru pacienții cu cancer,
Lactation. 18(4):393-6.
aceștia au declarat că a fost foarte bine tolerat și că au
3. Arnold LDW. Becoming a Donor to a Human Milk
observat o ameliorare a dificultăților de deglutiție,
Bank. LEAVEN. 2000;36(2),19-23.
episoade reduse de greață și vărsături, slăbiciune și
4. Bertino E, Giuliani F, Occhi L, Coscia A, Tonetto P,
letargie, care apar frecvent după inițierea chimioterapiei.
Marchino F, Fabris C. Benefits of donor human milk for
Pacienții au raportat o îmbunătățire a stării lor generale,
preterm infants: Current evidence. Early Human
a nivelul de energie, a funcției respiratorii și a apetitului.
Development. 2009;85,S9-S10.
Îmbunătățirea calității vieții este un factor important
5. Bertino E, Di Nicola P, Giuliani F, Peila C, Cester E,
pentru pacienții cu cancer. Pacienții participanți la acest
Vassia C, Pirra A, Tonetto P, Coscia A. Benefits of human
studiu, cu forme moderate și severe de cancer, au
milk in preterm infant feeding. Journal of Pediatric and
observat o îmbunătățire a calității vieții- fizice, mentale
Neonatal Individualized Medicine. 2012;1(1):19-24.
și spirituale. În prezent, băncile de lapte sunt capabile să
6. Baumslag N. Breastfeeding: cultural practices and
satisfacă nevoile pacienților cu cancer care utilizează
variations. Adv Int Mat Child Health. 1987;7:36-50.
această terapie
[19]. Folosirea laptelui donat pentru
7. Pettersson J, Mossberg AK, Svanborg C. alpha-
adulți este temporară și nu în cantități atât de mari încât
Lactalbumin species variation, HAMLET formation,
să influențeze depozitele de lapte uman donat pentru
and tumor cell death. Biochem Biophys Res Commun.
nou-născuți și sugari [10]. Cantitatea medie de lapte
2006;345(1):260-70.
101
Treatment with Human Milk for Adults Conditions
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
8.
Håkansson A, Zhivotovsky B, Orrenius S, Sabharwal H,
oleic acid complex examined by descriptive and
Svanborg C. Apoptosis induced by a human milk
quantitative liquid chromatography-tandem mass
protein. Proc Natl Acad Sci USA. 1995,92:8064-8.
spectrometry. J Dairy Sci. 2016. [Epub ahead of print]
9.
Svanborg C, Agerstam H, Aronson A, Bjerkvig R,
15.
Tully MR, Lockhart-Borman L, Updegrove K. Stories
Düringer C, Fischer W, Gustafsson L, Hallgren O,
of Success: Te Use of Donor Milk Is Increasing in North
Leijonhuvud I, Linse S, Mossberg AK, Nilsson H,
America. J Hum Lact. 2004,20(1):75-7.
Pettersson J, Svensson M. HAMLET kills tumor cells by
16.
Merhav HJ, Wright HI, Mieles LA, Van Tiel DH.
an apoptosis-like mechanism-cellular, molecular, and
Treatment of IgA deficiency in liver transplant
therapeutic aspects. Adv Cancer Res. 2003;88:1-29.
recipients with human breast milk. Transplant Int.
10.
Arnold LD. Possibilities for donor milk use in adult
1995;8:327-9.
clinical settings-a largely unexplored area. J Hum Lact.
17.
Campbell DA, Lorber MI, Sweeton JC, Turcotte JG,
1996;12(1):59-60.
Niederhuber JE, Beer AE. Breast feeding and maternal-
11.
Mossberg AK, Wullt B, Gustafsson L, Månsson W,
donor renal allografts. Transplantation. 1984,37:340-4.
Ljunggren E, Svanborg C. Bladder cancers respond to
18.
Wiggins PK, Arnold LD. Clinical case history: donor
intravesical instillation of HAMLET (human alpha-
milk use for severe gastroesophageal reflux in an adult. J
lactalbumin made lethal to tumorcells). Int J Cancer.
Hum Lact. 1998;14(2):157-9.
2007;121(6):1352-9.
19.
Rough SM, Sakamoto P, Fee CH, Hollenbeck CB.
12.
Fischer W, Gustafsson L, Mossberg AK, Gronli J,
Qualitative Analysis of Cancer Patients’ Experiences
Mork S, Bjerkvig R, Svanborg C. Human alpha-
Using Donated Human Milk. J Hum Lact.
lactalbumin made lethal to tumor cells (HAMLET) kills
2009;25(2):211-9.
human glioblastoma cells in brain xenografts by an
20.
Cregan MD, Fan Y, Appelbee A, Brown ML, Klopcic
apoptosis-like mechanism and prolongs survival. Cancer
B, Koppen J, Mitoulas LR, Piper KM, Choolani MA,
Res. 2004;64(6):2105-12.
Chong YS, Hartmann PE. Identification of nestin-
13.
Hallgren O, Gustafsson L, Irjala H, Selivanova G,
positive putative mammary stem cells in human
Orrenius S, Svanborg C. HAMLET triggers apoptosis
breastmilk. Cell Tissue Res. 2007;329(1):129-36.
but tumor cell death is independent of caspases, Bcl-2
21.
Twigger AJ, Hodgetts S, Filgueira L, Hartmann PE,
and p53. Apoptosis. 2006;11(2):221-33.
Hassiotou F. From Breast Milk to BrainsTe Potential
14.
Fang B, Zhang M, Fan X, Ren FZ. Te targeted
of Stem Cells in Human Milk. J Hum Lact.
proteins in tumor cells treated with the α-lactalbumin-
2013;29(2)136-9.
102
Niță et al
GUIDANCE FOR DRAWING UP
STANDARDE DE REDACTARE
Scop
materiale care ar putea să îi identifice. Dacă formularele
Revista Conexiuni Medicale publică lucrări de
de accept nu prevăd acest lucru vă rugăm să rugăm
cercetare care contribuie la progresul din toate domeniile
obţineţi acordul, sau îndepărtaţi posibilitatea de
medicinei. Revista publică de asemenea reviste generale,
identificare. O declaraţie în acest sens trebuie inclusă în
editoriale şi scurte comunicări pe domenii specifice.
secţiunea „Metode” a lucrării.
Prezentările de caz sunt acceptate dacă prezintă interes
crescut şi sunt bine investigate. Scrisorile către editor, în
Aprobarea Comitetului de Etică
special cele care prezintă o opinie privind un articol
Precizaţi la secţiunea „Metode” faptul că desfăşuraţi
publicat anterior sau care prezintă noi date, sunt de
studii asupra subiecţilor umani cu aprobarea Spitalului,
asemenea binevenite. Adresa web a revistei este http://
Comitetului de Etică al Universităţii, etc. În mod
similar, confirmaţi dacă experimentele asupra animalelor
trimestrial, articolele sunt acceptate în limba engleză sau
corespund standardelor etice.
română, având cel puţin traducerea în limba engleză a
rezumatului şi cuvintelor cheie. Lucrările pot fi trimise
Asumarea dreptului de copyright
pe adresa: dr. Bumbuluţ Călin, editor şef adjunct,
Lucrările acceptate pentru publicare au implicit
Conexiuni Medicale, P-ţa. Eroilor Revoluţiei nr. 23,
drepturile de copyright cedate către editor. Autorii pot
cod 440055, Satu Mare, România. Tel./Fax: +40-261-
utiliza materiale din lucrările lor în alte articole proprii,
710456, e-mail: bumbulutcalin@yahoo.com.
după obţinerea acceeptului editorului.
Republicarea articolelor
Propunerea pentru publicare
Vă rugăm să confirmaţi că lucrarea dumneavoastră
Toate manuscrisele propuse pentru publicare în
nu a mai fost publicată în forma prezentată sau într-o
Conexiuni Medicale vor fi în format compatibil pentru
formă asemănătoare, sau că nu a fost acceptată pentru
efectuarea recenziei online. Revista acceptă manuscrise
publicare într-o altă revistă.
propuse în formă electronică, în format Word (text,
figuri şi tabele). Nu trimiteţi lucrări în format PDF.
Conflicte de interese
Acceptăm lucrări care nu depăşesc 3.500 de cuvinte
Rugăm autorii să declare posibilele conflicte de
pentru articole originale, 2.500 pentru prezentări de
interese, inclusiv cele de natură financiară. Dacă nu
caz, 2.000 pentru prezentări de imagini clinice, 500
există conflicte de interese, vă rugăm să precizaţi acest
pentru scrisori către editor şi 4.500 de cuvinte pentru
lucru. Sursele de finanţare trebuie precizate în lucrarea
reviste generale. Autorii NU vor trimite prin poştă sub
dumneavoastră.
formă de hârtie propunerea pentru publicare, decât
dacă este vorba de scrisori sau dacă se solicită astfel din
Permiterea de a reproduce materiale
partea redacţiei. Dacă nu există altă opţiune decât
publicate anterior
trimiterea prin poştă, vă rugăm să expediaţi şi versiunea
Vă rugăm să ne trimiteţi o copie a acceptului de
electronică CD-ROM pe adresa redacţiei: Conexiuni
reproducere (de exemplu al ilustraţiilor) de la deţinătorul
Medicale, P-ţa. Eroilor Revoluţiei nr. 23, cod 440055,
dreptului de copyright.
Satu Mare, România. Utilizaţi text la două rânduri şi
includeţi următoarele secţiuni: pagina de titlu,
Formularele de accept ale pacienţilor
rezumatul şi cuvintele cheie, textul, mulţumiri,
Protecţia drepturilor pacienţilor este esenţială; vă
referinţe, tabele şi figuri. Paginile vor fi numerotate
rugăm să ne trimiteţi formularele de accept ale
consecutiv, începând cu pagina de titlu, numerele
pacienţilor sau subiecţilor studiului dumneavoastră,
arabe fiind plasate în colţul din dreapta sus al fiecărei
prin care aceştia permit publicarea fotografiilor sau altor
pagini.
Guidance for Authors
103
Guidance for drawing up
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
Prezentarea lucrării
Nu recomandăm utilizarea excesivă a abrevierilor. Folosiţi
Pagina de titlu
metode de calcul statistic standardizate. Nominalizaţi
Cuprinde titlul întreg şi titlul scurt format din
medicamentele şi substanţele chimice utilizând numele
maxim 45 de caractere, numele şi prenumele fiecărui
generic
(dacă sunt menţionate mărcile înregistrate, se
autor; dacă lucrarea aparţine unui departament sau unei
furnizează numele producătorului şi oraşul).
instituţii, va fi menţionat numele acestuia în întregime.
Mulţumiri
De asemenea numele, e-mail-ul şi adresa autorului
Vor fi adresate celor care au adus contribuţii
împuternicit pentru corespondenţă, sursele de finanţare
importante la studiu.
sau suport utilizate sub forma burselor, echipamentelor,
Referinţe
medicamentelor, sau orice combinaţie a acestora.
Vor fi numerotate între paranteze drepte cu
Rezumatul
numerale arabe, succesiv în ordinea în care sunt
Pagina a doua va cuprinde rezumatul cu minim 200
menţionate în text. Referinţele vor include numele
de cuvinte; nu utilizaţi abrevieri, note de subsol, sau
autorilor până la al şaselea autor, dacă sunt mai mulţi,
referinţe.
enumeraţi primii trei şi apoi adăugaţi „et al”. Referinţele
Introducere în temă şi scopuri
vor include titlul complet şi sursa informaţiei; numele
Descrieţi importanţa studiului şi obiectivul
revistelor va fi abreviat conform Index Medicus (http://
(obiectivele) precise ale cercetării sau întrebarea
(întrebările) pe care le ridică studiul.
acceptă mai mult de 90-100 referinţe; pentru scrisori
Metode
către redacţie se acceptă
5-6 referinţe. Folosiţi ca şi
Includeţi informaţii privind următoarele aspecte ale
referinţe cât mai puţine rezumate. Comunicările
studiului dacă sunt utilizate: proiectul
- descrieţi
personale şi lucrările nepublicate nu vor fi menţionate la
elementele de bază ale studiului, de exemplu studiu
referinţe şi vor apare în text între paranteze. Lucrările
controlat randomizat, studiu cross-secţional, de cohortă,
nepublicate dar aflate în curs de publicare vor fi incluse
de urmărire, serii de cazuri, etc; procedura - specificaţi
în referinţe cu menţiunea „in press” între paranteze,
dacă a fost desfăşurat în sistem de îngrijire primar sau
lângă numele revistei implicate.
terţiar, în ambulator sau spital, în comunitate, etc;
a) Articole:
participanţi - indicaţi numărul subiecţilor şi cum au
[1] Otvos L Jr, Shao WH, Vanniasinghe AS, Amon
fost selectaţi, recrutaţi şi desemnaţi pentru intervenţie;
MA, Holub MC, Kovalsykz I, et al. Toward understanding
intervenţia
- metoda de administrare şi durata
the role of leptin and leptin receptor antagonism in
intervenţiei.
preclinical models of rheumatoid arthritis. Peptides
Rezultate
2011;32:1567-74.
Prezentaţi principalele rezultate ale studiului,
b) Lucrări publicate numai cu numerele DOI:
inclusiv intervalurile de confidenţă sau valorile p.
[2] Chaldakov GN, Beltowsky J, Ghenev PI, Fiore
Concluzii
M, Panayotov P, Rancic G, et al. Adipoparacrinology -
Enunţaţi doar concluziile susţinute direct de dovezi,
vascular periadventitial adipose tissue (tunica adiposa) as
precum şi importanţa descoperirilor. Revistele generale
an example. Cell Biol Int
2011;doi:
10.1042/
şi prezentările de caz vor include un rezumat
CBI20110422.
nestructurat.
c) Cărţi sau manuale:
Cuvinte cheie
[3] Gertler A, editor. Leptin and Leptin Antagonists.
Rezumatul va fi urmat de o listă de 3-10 cuvinte
Landes Bioscience, Austin, Texas, USA. 2009.
cheie sau fraze scurte care vor ajuta la indexare. Dacă
d) Capitole de cărţi sau de manuale:
este posibil, utilizaţi termeni proveniţi din lista Index
[4] Jeremy L, Abe PD. Treatment Options in
Medicus cu
262 subiecte medicale/Medical Subject
Superficial (pTa/pT1/CIS) Bladder Cancer. In: Urological
Headings
262
cancers in clinical practice, Springer-Verlag, London
meshhome.html).
Limited, 2007:75-102.
Textul
Tabele
Un studiu original va fi divizat în secţiuni denumite
Fiecare tabel va fi numerotat cu numerale romane,
Introducere, Metode, Rezultate şi Discuţii
(incluzând
cu un titlu scurt deasupra, la subsolul lor vor fi trecute
concluziile), după formula „IMRAD”. Articolele lungi
notele
explicative,
menţionându-se abrevierele
pot necesita subsecţiuni (în special la Rezultate şi Discuţii)
nestandardizate utilizate; nominalizaţi valorile statistice
pentru clarificare. Alte tipuri de articole precum prezentări
care variază precum deviaţia standard şi eroarea standard
de caz, reviste generale, editoriale, pot urma alt format.
a medianei. Fiecare tabel va fi citat în text.
104
MEDICAL CONNECTIONS • NUMBER 2 (42) • JUNE 2016
Guidance for drawing up
Figuri
acestor sugestii, rugându-i să răspundă la întrebări şi să
Toate graficele, fotografiile, diagramele vor fi
facă necesarele corecţii. Aceste informări sunt făcute în
considerate ca figuri şi vor fi numerotate succesiv în text
cel mult trei luni de la propunerea de publicare.
cu numerale arabe. Dacă o figură a fost publicată
Manuscrisul revizuit de autori va fi reexpediat editorului
anterior, sursa va fi citată cu mulţumiri, menţionându-
în cel mult o lună. La primirea de către editor a versiunii
se permisiunea deţinătorului de copyright. Figurile pot
corectate, însoţită de o scrisoare de răspuns punctuală la
fi reduse, grupate sau şterse la dorinţa editorului.
comentariile recenzorilor, se retrimite manuscrisul
Legenda figurii va fi plasată la subsolul ei; va fi explicată
aceloraşi recenzori, care vor face recomandarea finală
scala utilizată, respectiv metodele de colorare
pentru acceptarea sau respingerea acestuia.
microscopică.
Unităţi de măsură
Abonamente
Măsurătorile lungimii, înălţimii, greutăţii şi
Preţul unui abonament anual pentru 2016 este: 80
volumului vor fi făcute în sistem metric sau multipli
RON individual, 160 RON pentru instituţii, plătiţi în
decimali. Temperaturile vor fi exprimate în grade
contul Colegiului Medicilor Satu Mare RO38 BTRL
Celsius. Tensiunea va fi măsurată în mmHg. Toate
0310
1202 K392
62XX, cod fiscal
9839430, cu
măsurătorile hematologice vor fi exprimate în Sistemul
menţiunea
„pentru abonament Conexiuni Medicale”.
Internaţional de Unităţi (SI).
Solicitarea abonării poate fi trimisă prin poştă: P-ţa.
Abrevieri şi simboluri
Eroilor Revoluţiei nr.
23, cod
440055, Satu Mare,
Utilizaţi doar abrevieri standard. Evitaţi abrevierile
România. Tel./Fax: 0261-710456, 0361-408164, sau
în titlu şi rezumat. Cuvântul va preceda abrevierea la
prin e-mail: colmedsm@gmail.com.
prima utilizare în text, cu excepţia unităţilor de măsură
standard.
Publicitate
Cererile pentru spaţiu publicitar vor fi adresate
Retipăriri
redacţiei Conexiuni Medicale. Preţurile (plătite în lei la
Sunt oferite gratuit zece copii ale articolului publicat
cursul BNR) pentru publicitate pe 2016 sunt 200 euro
şi două ale revistei. Dacă sunt necesare mai multe copii,
pagina (A4) color, un număr şi 800 euro patru numere;
sunt disponibile contra cost.
coperta interioară faţă sau spate: 350 euro un număr,
1400 euro patru numere; coperta exterioară spate: 400
Politica editorială
euro un număr, 1600 euro patru numere. Cont bancar:
Apreciem toate contribuţiile în domeniul medicinei.
Colegiul Medicilor Satu Mare, CUI 9839430, Banca
Invităm personalităţi recunoscute cu expertiză şi articole
Transilvania, agenţia Golescu Satu Mare, IBAN: RO38
din diverse domenii să publice reviste generale şi
BTRL 0310 1202 K392 62XX.
editoriale în revista noastră. Acceptăm de asemenea
lucrări originale şi prezentări de caz din toate ţările.
© Copyright Conexiuni Medicale/Medical
Conexiuni Medicale vă oferă o recenzie atentă şi publicarea
Connections, Satu Mare, 2016
imediată după acceptare. Redactorii vor citi primii
Nicio parte a acestei publicaţii nu poate fi reprodusă,
lucrarea, decizând în decurs de 1-3 săptămâni în funcţie
stocată sau transmisă sub orice formă sau prin orice
de nivelul de prioritate: unele sunt trimise imediat
mijloace, fără permisiunea prealabilă în scris a revistei
recenzorilor, unele pot fi respinse, iar unele sunt
Conexiuni Medicale. Permisiunea nu este necesară
returnate autorilor cu sugestii de îmbunătăţire înainte
pentru a copia rezumate sau articole dacă este indicată
de expedierea spre recenzori.
sursa, cu citarea completă a referinţei. Solicitarea
privind permisiunea de a retipări toată revista sau o
Procedura peer-review
parte a ei, va fi adresată editorului prin e-mail:
Conexiuni Medicale practică o evaluare a tuturor
colmedsm@gmail.com
lucrărilor originale de către doi sau trei recenzori
independenţi, din care doi sunt personalităţi
Revista Conexiuni Medicale apare trimestrial prin
internaţionale. Procesul peer-review este esenţial pentru
efortul logistic şi financiar al Colegiului Medicilor
asigurarea calităţii informaţiei ştiinţifice. Recenzorii
Satu Mare şi Asociaţiei Medicilor de Familie Satu
sunt rugaţi să evalueze manuscrisul aplicând aceleaşi
Mare, în cadrul proiectului comun al Centrului de
standarde ca şi pentru reviste internaţionale; comentariile
Documentare şi Educaţie Medicală Continuă Satu
sunt trimise editorului, care va informa autorii asupra
Mare.
105
Guidance for Authors