MEDICAL CONNECTIONS | CONEXIUNI MEDICALE®
ASSISTANT EDITORS
EDITOR IN CHIEF
Blaga Vasile (Electronic Version)
Koren Rumelia
Andó Ottó (Print Version)
ASSISTANT EDITOR IN CHIEF
Oană Cristian Sever (Editorialist)
Bumbulu Călin
Stăncioiu Tudor (Dental Medicine)
EDITORIAL BOARD
Bauer Adalbert (SCM Satu Mare, România)
Lup Liliana (Synevo Satu Mare, România)
Bidilean Nicolae (Emergency County Hospital,
Kesler Gavriel (Israel)
Satu Mare, România)
Kiss Ladislau (Emergency County Hospital,
Boros Melinda (Bucureşti, România)
Satu Mare, România)
Borcean Gheorghe (Caransebeş Hospital, România)
Mihalca Man Sorina (Emergency County Hospital,
Brândeu Ioan (Emergency County Hospital,
Satu Mare, România)
Satu Mare, România)
Neumann Gad (Hasharon Hospital, Tel Aviv, Israel)
Cârstea Constantin (CMI Braşov, România)
Negru Alina (SCM Satu Mare, România)
Cojocaru Manole (Titu Maiorescu University,
Rath-Wolfson Lea (Hasharon Hospital, Tel Aviv, Israel)
Bucureşti, România)
Rădulescu Viorel (CMI Olt, România)
Comăneanu Raluca Monica (Titu Maiorescu University,
Roatiş Marius Dinu (Emergency County Hospital,
Bucureşti, România)
Satu Mare, România)
Cornean-Santa Corina (Emergency County Hospital, Satu
Rusu Cristian Bogdan (Emergency County Hospital,
Mare, România)
Satu Mare, România)
Feciche Bogdan (Emergency County Hospital,
Shvero Kesler Dana (Hadassa University, Jerusalem, Israel)
Satu Mare, România)
Trip Gheorghe (Emergency County Hospital,
Grosz Gyula (SCM West Satu Mare, România)
Satu Mare, România)
Gruzman Carlos (Hasharon Hospital,
Zilahi Karoly (SCM Praxis, Bixad, România)
Tel Aviv, Israel)
Zeidman Aliza (Hasharon Hospital, Tel Aviv, Israel)
Horber Orsolya (SCM Praxis Bixad, România)
Virag Tiberiu (CMI Satu Mare, România)
EDITOR
ASSOCIATED EDITOR
College of Physicians Satu Mare
Satu Mare Association of Family Physicians
Satu Mare, 23 Eroilor Revolu iei Pl.
A liated with National Society of Family Medicine/
General Medicine
email: colmedsm@gmail.com
Satu Mare, UK 30 Bobocului St.
PARTNERSHIP
EXTERNAL PARTNERSHIP
Titu Maiorescu University, Bucharest
Vasile Goldiş
Hasharon Hospital,
Faculty of Medicine and Dental Medicine
Western University of Arad
Rabin Medical Center
67A Gheorghe Petraşcu St.
94 Revolutiei Blvd., Arad, Romania
A liated with Sackler School of Medicine,
Petah Tikva 49372, Israel
EDITORIAL OFFICE
23 Eroilor Revolu iei Pl., 440055, Satu Mare, Romania, Tel/Fax: 0040261-710456, 0040361-408164
ISSN online 2068 - 8369
ISSN 1843 - 9306
Journal included in e Schedule of Medical Publications of CMR, 5 credits CMR for subscribers
Indexed in Index Copernicus®, CNCS B+ Category, Code 944
Medical Connections/Conexiuni Medicale® is a trademark of College of Physicians Satu Mare and Satu Mare Association of Family Physicians
Printed at TIPOOFFSET, Fabricii st, No. 93-103, Cluj Napoca, Tel.: 0040264-456071, Fax: 0040264-595711
SCIENTIFIC AND PEER REVIEW BOARD | COLECTIV ŞTIIN IFIC ŞI DE RECENZIE
Acad. Prof. Univ. as. Dr. Virgil Enătescu
Prof. Univ. Dr. Tuvia Hadar
(Emergency County Hospital, Satu Mare,
(Beilinson Hospital, Rabin Medical Center, Sackler
Romania)
Faculty of Medicine, Tel Aviv University, Israel)
Acad. Prof. Univ. Dr. Doina Onicescu
Prof. Univ. Dr. Gheorghe Manole
(Titu Maiorescu University, Faculty of Medicine
(Titu Maiorescu University, Faculty of Medicine
and Dental Medicine, Bucharest, Romania)
and Dental Medicine, Bucharest, Romania)
Acad. Senior Scienti c Researcher Dr. Sorin Riga
Prof. Univ. Dr. Dorel Augustin Manu
(Prof. Dr. Al. Obregia Clinic Hospital of Psychiatry,
(Titu Maiorescu University, Faculty of Medicine
Bucharest, Romania)
and Dental Medicine, Bucharest, Romania)
Acad. Senior Scienti c Researcher Dr. Dan Riga
Prof. Univ. Dr. Dan Mănăstireanu
(Prof. Dr. Al. Obregia Clinic Hospital of Psychiatry,
(Titu Maiorescu University, Faculty of Medicine
Bucharest, Romania)
and Dental Medicine, Bucharest, Romania)
Prof. Univ. Dr. Vasile Astărăstoae
Prof. Univ. Dr. Elena Moldoveanu
(Gr. T. Popa University of Medicine and Pharmacy,
(Titu Maiorescu University, Faculty of Medicine
Iaşi, Romania)
and Dental Medicine, Bucharest, Romania)
Prof. Univ. Dr. Rumelia Koren
Prof. Univ. Dr. Adriana Stănilă
(Hasharon Hospital, Rabin Medical Center, Sackler
(Victor Papilian Faculty of Medicine, Sibiu,
School of Medicine, Tel Aviv University, Israel)
Romania)
Prof. Univ. Dr. Petru Armeanu
Prof. Univ. Dr. Maria Lidia Nica Udangiu
(Titu Maiorescu University, Faculty of Medicine
(Titu Maiorescu University, Faculty of Medicine
and Dental Medicine, Bucharest, Romania)
and Dental Medicine, Bucharest, Romania)
Prof. Univ. Dr. Ilie Constantin
Prof. Univ. Dr. Dan Florin Ungureanu
(Victor Babeş University, Faculty of Medicine,
(Titu Maiorescu University, Faculty of Medicine
Timişoara, Romania)
and Dental Medicine, Bucharest, Romania)
Prof. Univ. Dr. Gheorghe Ionel Comşa
Conf. Univ. Dr. Ghinescu Minerva
(Ovidius University, Constan a, Romania)
(Titu Maiorescu University, Bucureşti, România)
Prof. Univ. Dr. Constantin Dumitru
Conf. Univ. Dr. Mircea Sorin Sabău
(Titu Maiorescu University, Faculty of Medicine
(University of Medicine and Pharmacy Târgu
and Dental Medicine, Bucharest, Romania)
Mureş, Romania)
Prof. Univ. Dr. Rivka Gal
Ş. L. Dr. Anca Ciurea
(Hasharon Hospital, Rabin Medical Center, Sackler
(Iuliu Ha ieganu University, Faculty of Medicine,
School of Medicine, Tel Aviv University, Israel)
Cluj Napoca, Romania)
Prof. Univ. Dr. Doina Lucia Ghergic
As. Univ. Dr. Virgil Radu Enătescu
(Titu Maiorescu University, Faculty of Medicine
(Eduard Pam l Universitary Clinic of Psychiatry,
and Dental Medicine, Bucharest, Romania)
Timişoara, Romania)
e Medical Connections/Conexiuni Medicale® is indexed in Journals Master List of Index Copernicus®
CNCS B+ Category, Code 944
© Copyright Medical Connections/Conexiuni Medicale, Satu Mare, 2013
No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form or by any
means without prior permission in writing of Medical Connections/Conexiuni Medicale®. Permission is not
however required to copy abstracts of papers or of articles on condition that a full reference to the source is
shown. Correspondence regarding permission to reprint all or part of any article published in this journal
should be addressed to the Editor, e-mail: colmedsm@gmail.com
MEDICAL CONNECTIONS | CONEXIUNI MEDICALE®
EDITORI ADJUNC I
EDITOR ŞEF
Blaga Vasile (versiunea electronică)
Koren Rumelia
Andó Ottó (versiunea tipărită)
EDITOR ŞEF ADJUNCT
Oană Cristian Sever (editorialist)
Bumbulu Călin
Stăncioiu Tudor (Medicina Dentară)
COMITET EDITORIAL
Bauer Adalbert (SCM West Satu Mare, România)
Kesler Gavriel (Israel)
Bidilean Nicolae (Spital Jude ean de Urgen ă,
Kiss Ladislau (Spital Jude ean de Urgen ă,
Satu Mare, România)
Satu Mare, România)
Boros Melinda (Bucureşti, România)
Mihalca Man Sorina (Spital Jude ean de Urgen ă,
Borcean Gheorghe (Spital Municipal Caransebeş, România)
Satu Mare, România)
Brândeu Ioan (Spital Jude ean de Urgen ă,
Neumann Gad (Spital Hasharon, Tel Aviv, Israel)
Satu Mare, România)
Negru Alina (SCM Satu Mare, România)
Cârstea Constantin (CMI Braşov, România)
Rath-Wolfson Lea (Spital Hasharon, Tel Aviv, Israel)
Cojocaru Manole (Universitatea Titu Maiorescu,
Rădulescu Viorel (CMI Olt, România)
Bucureşti, România)
Roatiş Marius Dinu (Spital Jude ean de Urgen ă,
Comăneanu Raluca Monica (Universitatea Titu Maiorescu,
Satu Mare, România)
Bucureşti, România)
Rusu Cristian Bogdan (Spital Jude ean de Urgen ă,
Cornean-Santa Corina (Spital Jude ean de Urgen ă,
Satu Mare, România)
Satu Mare, România)
Shvero Kesler Dana (Universitatea Hadassa,
Feciche Bogdan (Spital Jude ean de Urgen ă,
Ierusalim, Israel)
Satu Mare, România)
Trip Gheorghe (Spital Jude ean de Urgen ă,
Grosz Gyula (SCM West Satu Mare, România)
Satu Mare, România)
Gruzman Carlos (Spital Hasharon, Tel Aviv, Israel)
Zilahi Karoly (SCM Praxis, Bixad, România)
Horber Orsolya (SCM Praxis Bixad, România)
Zeidman Aliza (Spital Hasharon, Tel Aviv, Israel)
Lup Liliana (Synevo Satu Mare, România)
Virag Tiberiu (CMI Satu Mare, România)
EDITOR
EDITOR ASOCIAT
Colegiul Medicilor Satu Mare
Asocia ia Medicilor de Familie Satu Mare
Satu Mare, P- a Eroilor Revolu iei nr.23
A liată la Societatea Na ională de Medicina Familiei/
Medicină Generală
email: colmedsm@gmail.com
Satu Mare, str. Bobocului UK 30
PARTENER
PARTENER EXTERN
Universitatea Titu Maiorescu Bucureşti
Universitatea de Vest Vasile Goldiş
Hasharon Hospital, Rabin Medical Center
Facultatea de Medicină şi Medicină Dentară
din Arad
A liat la Sackler School of Medicine,
str. Gheorghe Petraşcu 67A
94 Revolu iei Blvd., Arad, România
Universitatea Tel Aviv
7 Keren Kayemet St.,
Petah Tikva 49372, Israel
REDAC IA
P- a Eroilor Revolu iei nr 23, 440055, Satu Mare, Romania, Tel/Fax: 0261-710456, 0361-408164
ISSN online 2068 - 8369
ISSN 1843 - 9306
Revistă inclusă în Nomenclatorul Publica iilor Medicale ale CMR, 5 credite CMR pentru abona i
Indexare în Index Copernicus®, CNCS categoria B+, cod 944
Medical Connections/Conexiuni Medicale® este marcă înregistrată a Colegiului Medicilor Satu Mare şi a Asocia iei Medicilor de Familie Satu Mare
Tipărit la TIPOOFFSET, str. Fabricii, Nr. 93-103, Cluj Napoca, Tel.: 0040264-456071, Fax: 0040264-595711
Contents
EDITORIAL
7
ORIGINAL ARTICLES
e Low Serum Concentrations of 25-OH Vitamin D in Patients with Early Rheumatoid Arthritis
Cojocaru Manole, Rusu Elena, Cojocaru Inimioara Mihaela, Siloși Isabela
9
Discourse Between Parents and eir Children about Sex in the Arab Community in Israel
Joubran Samia, Marcus Ohad, Rath-Wolfson Lea, Tova Hartman, Iancu Iulian, Weizman Abraham,
Ram Edward
13
Epidemiological Aspects of Gastric Cancer in Arad County
Răducan Ionu Daniel, Ciobanu Gheorghe
21
Environmental In uences on Addictive Behavior of the People in Cluj County
Kelemen Alexander, Podea Delia, Pușchi ă Maria
25
GENERAL REVIEW
Oral Manifestations in Patients with Red Blood Series Pathology and Coagulation Disorders.
Review of Literature
Pop Diana-Ioana, ovaru Șerban
29
Intermittent Androgen Deprivation in Treatment of Prostate Cancer.
Review of Literature
Mureșanu Horia, Ioiart Ioan
35
Treatment Approach of Oral Leukoplakia. Review of Literature
Părlătescu Ioanina, ovaru Șerban, Mihai Lelia
39
CASE PRESENTATION
igh Amputations in Diabetic Patients with a History of Femoral Osteosynthesis.
Case Presentation
Aiordăchioaie Gigi Adrian, Pop Alexandru, Dumnici Alexandru, Fruja Dan, Papiu Hora iu Sabin,
Korodi Andrei, Hărăguș Horia
45
MEDICINE AND ART
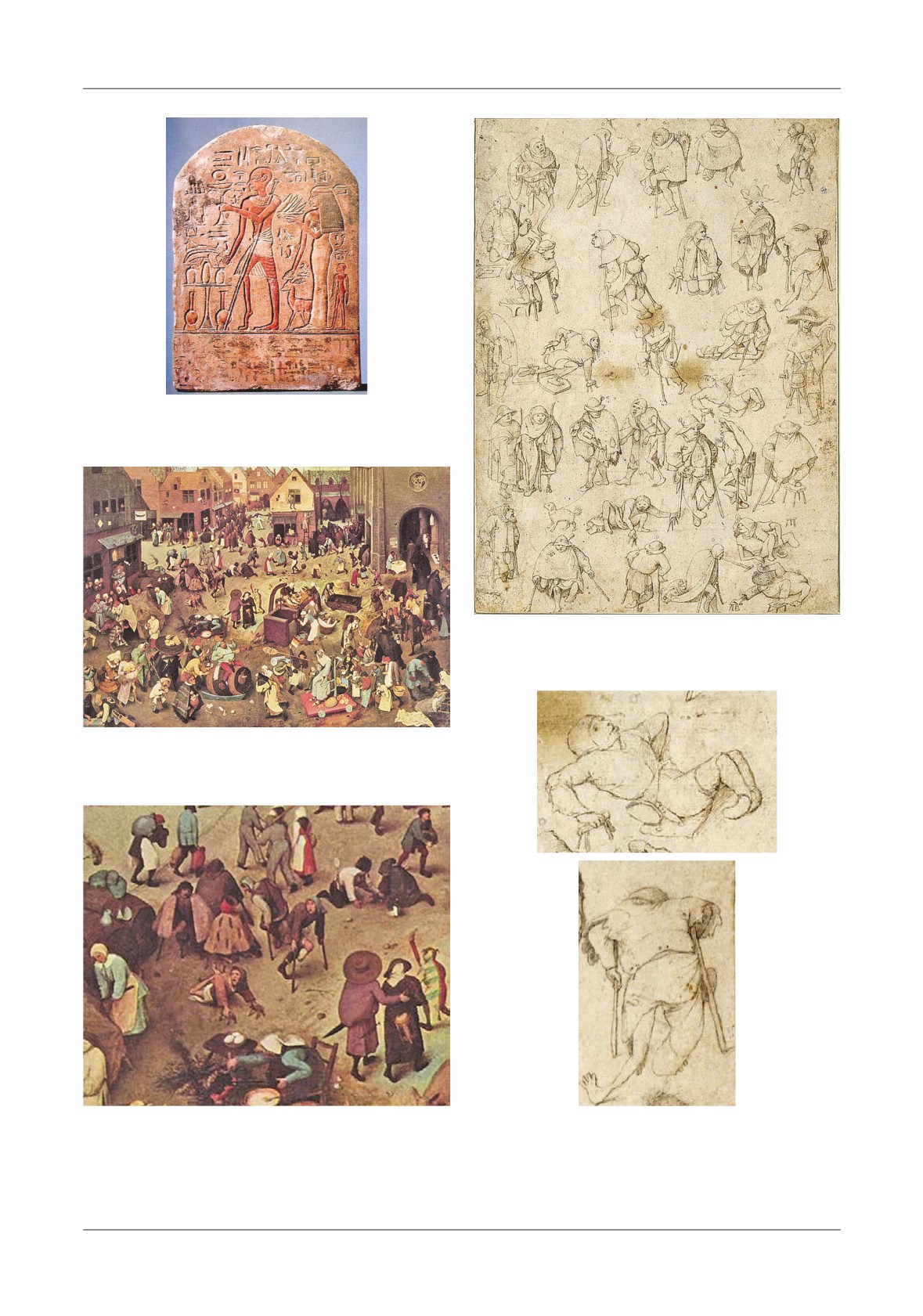
e Description of the Sequels of Poliomyelitis in Art
Bumbulu Călin, Bumbulu Andrei, Oprea Andrea, Koren Rumelia
51
IN MEMORIAM
Professor Dr. oma Ionescu
Bumbulu Călin, Koren Rumelia
55
GUIDANCE FOR AUTHORS
57
Cuprins
EDITORIAL
61
ARTICOLE ORIGINALE
Concentra ii scăzute în ser ale vitaminei D 25-OH la pacien i cu debut de poliartrită reumatoidă
Cojocaru Manole, Rusu Elena, Cojocaru Inimioara Mihaela, Siloși Isabela
63
Discu ia despre sex dintre părin i și copiii lor în comunitatea arabă din Israel
Joubran Samia, Marcus Ohad, Rath-Wolfson Lea, Tova Hrtman, Iancu Iulian, Weizman Abraham,
Ram Edward
67
Aspecte epidemiologice ale cancerului gastric în jude ul Arad
Răducan Ionu Daniel, Ciobanu Gheorghe
75
In uen ele mediului în comportamentul adictiv al persoanelor din jude ul Cluj
Kelemen Alexander, Podea Delia, Pușchi ă Maria
79
REVISTĂ GENERALĂ
Manifestări bucale la pacien ii cu afec iuni ale seriei roșii sanguine și tulburări de coagulare.
Trecere în revistă a datelor din literatură
Pop Diana-Ioana, ovaru Șerban
83
Tratamentul cancerului de prostată prin deprivare androgenică intermitentă. Trecere în revistă
a datelor din literatură
Mureșanu Horia, Ioiart Ioan
89
Abordarea terapeutică a leucoplaziei orale. Trecere în revistă a datelor din literatură
Părlătescu Ioanina, ovaru Șerban, Mihai Lelia
93
PREZENTARE DE CAZ
Amputa iile de coapsă la pacien ii diabetici cu osteosinteză femurală în antecedente.
Prezentare de caz
Aiordăchioaie Gigi Adrian, Pop Alexandru, Dumnici Alexandru, Fruja Dan, Papiu Hora iu Sabin,
Korodi Andrei, Hărăguș Horia
99
MEDICINA ȘI ARTA
Reprezentarea sechelelor poliomielitei în artă
Bumbulu Călin, Bumbulu Andrei, Oprea Andrea, Koren Rumelia
105
IN MEMORIAM
Profesor Dr. oma Ionescu
Bumbulu Călin, Koren Rumelia
109
STANDARDE DE PUBLICARE
111
Colegiul Medicilor
Satu Mare
Colegiul Medicilor Satu Mare este o persoană juridică autonomă, neguvernamentală,
apolitică şi fără scop patrimonial. Este într-o largă accep iune o organiza ie profesională
liberală şi reuneşte peste 626 de medici.
Colegiul Medicilor Satu Mare crede că poate reuşi urmând trei principii: să vorbească doar
când are ceva important de spus, să nu critice până când nu are solu ii şi să nu propună decât
solu ii rezultate din sfatul colectiv. For a Colegiului Medicilor constă în prezentarea în fa a
societă ii ca o voce autentică, permanent validată, a tuturor membrilor săi.
Satu Mare College of Physicians is an autonomous legal entity, non-governamental, apolitical
and non-pro t. In a widley acception it is a liberal professional organization and brings
together over 626 doctors.
Satu Mare College of Physicians believes it can succeed by following three principles: to
speak only when he has something important to say, to make no critics until he has solutions
and to propose only solutions resulted from a of collective advice. e force of Physicians
College consist in showing in front of the society an authentic voice, always validated, from
all its members.
Eroilor Revolu iei Pl. no.23, 440055 Satu Mare, Romania.
Tel./Fax: +40-261-710456, +40-361-408164, e-mail: colmedsm@gmail.com
EDITORIAL
END OF AN ILLUSION
It is a remarkable paradox that at the peak of human
average fatter than the rich.
e economic growth,
material and technological achievements of Romania
which has been until now the engine of progress, has
(compared to all our past), we nd ourselves
reached its limits in developed countries. Statistics that
overwhelmed by anxiety, leaning towards depression,
measures wellbeing and happiness indicates a limitation
anxious as how we appear in the eyes of others, unsure
of indices in civilized countries, while the frequency of
of our friendships, tempted by the consumption, and
the anxiety, depression and social problems is increasing.
lack of community life. In the absence of calm social
For some poor countries the life expectancy increases
relations and emotional satisfaction that we all need, we
rapidly in the early stages of economic development,
seek solace in overeating, obsessive buying, or we fall
and among middle-income countries the growth rate of
prey to alcohol, psychotropic or drugs. How come we
life expectancy slows down. As the living standard rises
experience so much emotional and mental distress
and countries become richer, the relationship between
despite the welfare and comfort unprecedented in our
economic growth and life expectancy becomes weaker.
national history? What we lack is something more than
For the rich countries the accumulation of new wealth
time spent with friends and family. We act as if our lives
does not add anything in life expectancy. e reason for
would be a continuing struggle for psychological
this is given by the fact that we have reached the limits
survival, a ght against stress and emotional exhaustion.
of the biological life expectancy. Even the richest
Some of us want a centered society on values, community
countries bene t from medical progress. What has
and family, away from greed and the excess of recent
changed is that the life expectancy has ceased to be
years. However, most of us have not yet achieved the
related to the material standard of living. With each
material ideal, more illusory, and continues to act
passing decade, life expectancy in rich countries increase
sel shly and irresponsibly in an increasingly fragmented
by 2-3 years, but this is no longer dependent on
society.
e political class does not seem to be interested
economic growth. erefore, U.S. citizens have a higher
in a given topic and stopped to try to provide us a
life expectancy than the Greeks, though they are two
coherent vision able to inspire us to create a better
times richer than them. By more rich is the country, the
society.
e economic crisis has only served to de ect
increasing of material living level contributes more less
attention from the sick society on the sick economy.
to the life expectancy and health in general.
Instead of trying to have a better society for us, each
What else is important for us than the life
individual strives to strengthen its position in the
expectancy and the health status? Of course, the pursuit
existing society. If we want to improve our quality of life
and reaching of happiness that Americans consider so
we have to move our attention and our e orts from
important that they put her in the Constitution as a
material standards to the improvement of psychological
fundamental right. e economist Richard Layard has
and social well-being of the entire society. However,
shown that like life expectancy and health, in very rich
soon as we spoke of psychology, the discussion tends to
countries the happiness cease to be correlated with the
move towards individual solutions.
e Political
accumulation of additional wealth. Happiness grows in
machine is stuck in the mud! I will start by saying that
poor countries in proportion to economic growth, but
statistical evidence shows that economic growth has
by at a certain level of wealth upwards, enters in
reached its limits in terms of providing human
“stagnation.” Of course, the de nition of happiness has
happiness, at least in civilized countries. When wolves
many local cultural particularities. In some societies, not
roamed the streets of the village, good times simply
to say you’re happy means that you admit you’re a loser;
meant to have a full belly and to be safe. For most of us
in others to pretend that you’re happy is an act of
drinking water, heated houses and a full fridge are things
arrogance. However Layard’s studies show that to an
for granted. Many of us want to eat less than we
annual income of over
25,000
$ per capita, the
normally do. For the rst time in history the poor are on
correlation between growth of income and the increasing
7
EDITORIAL
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
of happiness is very weak. Long term studies made in
which the bene ts bringed by increased of wealth is
Japan, the U.S. and the UK shows that over a period of
decreased. Trends in mortality con rm the same model.
time long enough to realize the doubling of income, the
When countries began to grow, the rst which are
happiness has not increased signi cantly.
e same
lowering are the diseases of poverty: malnutrition,
pattern is true for other indicators of welfare such as
tuberculosis, cholera, and measles. ey cease to be the
“measure of economic welfare” and “genuine progress
main causes of death. Instead appear diseases of
indicator” that calculates the net bene ts of development
a uence: cardiovascular disease, diabetes, cancer,
after excluding costs with pollution and tra c jams. In
degenerative diseases. While poverty diseases kill mostly
poor countries, the economic growth continues to be
children, the a uence diseases kill especially adults.
essential to the health and happiness of the inhabitants.
Romania has not reached the threshold of 25,000
$ per
But once reached the threshold of wealth, income
year, but it certainly will get there.
e discussion may
growth matters increasingly less. If you are hungry,
seem premature now, although we already have signs of
bread is essential to your health and wellbeing. But if
su ering caused by the growth. Its purpose is to exploit
you’re full, a hundred of breads might even bother you.
one of the advantages of relative backwardness. We can
Sooner or later, along of the history of economic growth,
develop a model of social development to avoid the
the countries has reached a threshold of a uence at
mistakes made by others. But do we want this?
Sever-Cristian Oană, MD
8
ORIGINAL ARTICLES
THE LOW SERUM CONCENTRATIONS OF 25 OH VITAMIN D IN
PATIENTS WITH EARLY RHEUMATOID ARTHRITIS
Cojocaru Manole1, Rusu Elena2, Cojocaru Inimioara Mihaela3, Siloşi Isabela4
1Department of Physiology, Faculty of Medicine, Titu Maiorescu University, Dr Ion Stoia Center for Rheumatic Diseases,
Bucharest, Romania, 2Department of Biochemistry, Faculty of Dental Medicine, Titu Maiorescu University, 3Department
of Neurology Prof. Gheorghe Marinescu, Colentina Clinical Hospital, Carol Davila University of Medicine and Pharmacy,
Bucharest, Romania, 4Department of Immunology, University of Medicine and Pharmacy, Craiova, Romania
Address for correspondence:
Cojocaru Manole
5 omas Masaryk St., Sector 2, Postal Code 020983
Bucharest, Romania
E-mail: mancojocaru@yahoo.com
Received: 12.08.2013
Accepted: 30.08.2013
Med Con October 2013, Vol 8, No 3, 9-11
Abstract
groups were calculated with Fisher’s exact test and two-
tailed t-test for continuous variables.
Background: Recent studies suggested that
Results: e serum values of 25(OH)D were found
immunoregulatory role of vitamin D. An association
low in 46 of 74 patients with RA (62%) vs. normal
between vitamin D de ciency and the development of
controls (p<0.01). Eight out of 46 patients had 25(OH)
rheumatoid arthritis (RA) has been suggested. Its role in
D at baseline. Serum values of 25(OH)D in early RA
modulating disease activity has not been studies.
showed a direct correlation with high disease activity
Objectives: To evaluate the plasma level of
(r=0.61; p<0.01). Levels of 25(OH)D correlated with
25-hydroxyvitamin D [25(OH)D] in RA patients and
high serum CRP levels (r=0.59; p<0.01).
e mean
to explore the e ects of serum vitamin D levels on
serum concentration of 25(OH)D in early RA patients
clinical outcome in patients with early RA.
28.34±8.7 nmol/L
(ranges from
18.52 to
41.36
Material and Methods: Serum levels of 25(OH)D
nmol/L), as compared to normal controls 52.42±13.4
were investigated in 74 patients with early RA (M/F
nmol/L
(ranges from
36.17 to
70.31 nmol/L);
25/49) with mean of age 35.7±11.4 years (ranges from
(p<0.001).
21.9 years to 58.4 years); mean of arthritis duration
Conclusion: All early RA patients presented a
5.1±4.3 months (ranges from 2 months to 10.2 months)
marked de ciency of
25(OH)D. e low level of
and 80 normal controls (M/F 27/53) with mean of age
25(OH)D had negative consequence on the clinical
34.2±10.7 years (ranges from 22.4 years to 47.8 years).
outcome.
Serum levels of 25(OH)D were tested using by enzyme-
Keywords: vitamin D, rheumatoid arthritis, disease
linked immunosorbent assay (ELISA). e 25(OH)D
activity
concentrations were expressed in nmol/L.
e results
were statistically analyzed by Student t test and a p<0.05
Vitamin D plays a part in the maintenance of
(95% con dence intervals) was considered statistically
immune homeostasis [1,2]. ere is increasing support
signi cant. Correlation analyses were performed using
for the idea that impaired vitamin D homeostasis
Spearman’s rank correlation, and di erences between
contributes to RA processes [3]. Rheumatoid arthritis is
The Low Serum Concentrations of 25-Oh Vitamin D in Patients with Early Rheumatoid Arthritis
9
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
an autoimmune disease presenting as a symmetric and
of 25(OH)D in early RA showed a direct correlation
chronic polyarthritis.
e pathogenesis is only partially
with high disease activity (r=0.61; p<0.01). Levels of
understood, but may include genetic susceptibility
25(OH)D correlated with high serum CRP levels
factors such as major histocompatibility class antigens,
(r=0.59; p<0.01).
e mean serum concentration of
environmental triggers and the activation of the innate
25(OH)D in early RA patients
28.34±8.7 nmol/L
and adaptative immune system. e de ciency could
(ranges from 18.52 to 41.36 nmol/L), as compared to
also potentially be one of the triggers for cartilage
normal controls 52.42±13.4 nmol/L (ranges from 36.17
damage in RA [4,5]. e in uence of vitamin D on
to 70.31 nmol/L); (p<0.001). Serum values of 25(OH)
human autoimmune diseases has not been well de ned.
D, anti-CCP3 IgG titers and high serum CRP levels are
correlated with the disease activity
(r=0.61, r=0.64,
Material and Methods
r=0.73, respectively). Serum values of
25(OH)D in
women patients/healthy women showed a correlation
Serum levels of 25-hydroxyvitamin D [25(OH)D]
(r=0.31); men patients/healthy men (r=0.34); women
were investigated in 74 patients with early RA (M/F
patients/men patients (r=0.63); healthy women/healthy
25/49) with mean of age 35.7±11.4 years (ranges from
men (r=0.84)
21.9 years to 58.4 years); mean of arthritis duration
5.1±4.3 months (ranges from 2 months to 10.2 months)
Discussion
and 80 healthy controls (M/F 27/53) with mean of age
34.2±10.7 years (ranges from 22.4 years to 47.8 years).
We showed that RA patients have an increased risk
e diagnosis of RA depends primarily on the
of vitamin D de ciency.
e extremely low level of
clinical manifestations of the disease, with very limited
25(OH)D had negative consequence on the clinical
serological support.
e distribution of joint
outcome. Low vitamin D levels are linked to increased
involvement at the outset is also very variable.
e
disease activity in RA.
disease may start in one joint or many and may also
Vitamin D also appears to be an important regulator
have a palindromic onset. A growing body of evidence
of immune function. Vitamin D de ciency or reduced
supports the use of anti-CCP3 IgG as a serological
intake has been linked to an increased susceptibility to
marker for early detection of RA.
develop autoimmune diseases. Recently vitamin D
Serum antibodies directed to cyclic citrullinated
de ciency has been implicated as a potential
peptides were tested using anti-CCP3 IgG ELISA kit.
environmental factor triggering several autoimmune
Serum levels of 25(OH)D were tested using ELISA.
disorders such as RA [6-9]. In the last few years, the
e
25(OH)D concentrations were expressed in
possible role of vitamin D in the pathogenesis of RA has
nmol/L.
e results were statistically analyzed by
been raised. Serum levels of 25(OH)D were inversely
Student t test and a p<0.05 (95% con dence intervals)
correlated with the severity of RA
[10-12]. Greater
was considered statistically signi cant. Correlation
intake of vitamin D may be associated with a lower risk
analyses were performed using Spearman’s rank
of RA; although this nding is hypothesis generating.
correlation, and di erences between
groups were calculated with Fisher’s
exact test and two-tailed t-test for
continuous variables.
Results
All patients with RA were positive
for anti-CCP3 IgG antibodies.
e
mean serum concentrations of
25(OH)D in patient groups were
signi cantly lower than those of the
controls. e serum values of 25(OH)
D were found low in 46 of 73 patients
with RA (62%) vs. normal controls
(p<0.01). Eight out of 46 patients had
Figure 1. Mean value of the serum vitamin D concentrations in patients with
25(OH)D at baseline. Serum values
rheumatoid arthritis as compared to normal controls
10
Cojocaru et al
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
ORIGINAL ARTICLES
e pathophysiological role of vitamin D in joint
6.
Costenbader KH, Feskanich D, Holmes M Karlson
in ammation is, however, unclear.
EW, Benito-Garcia E. Vitamin D intake and risk of
systemic lupus erythematosus and rheumatoid arthritis
in women. Ann Rheum Dis 2008;67:530-5.
References
7.
Marques C, Dantas A, Fragoso T, et al. e importance
of vitamin D levels in autoimmune diseases. Bras J
1. Wen H, Baker JF. Vitamin D, immunoregulation, and
Rheumatol 2010;50:73-80.
rheumatoid arthritis. Journal of Clinical Rheumatology
8.
Patel S, Farragragher T, Berry J, et al. Association
2011;17:102-7.
between serum vitamin D metabolite levels and disease
2. Kiran G, Debashish D. Vitamin D and rheumatoid
activity in patients with early in ammatory polyarthritis.
arthritis: is there a link? Int J Rheum Dis 2008;11:206-
Arthritis Rheum 2007;56:2143-9.
11.
9.
Cutolo M, Otsa K, Ypras M, et al. Vitamin D and
3. Cantorna MT. Vitamin D and autoimmunity: is vitamin D
rheumatoid arthritis: comment on the letter by Nielen et
status an environmental factor a ecting autoimmune disease
al [letter]. Arthritis Rheum 2007;56:1719-20.
prevalence? Proc Soc Exp Biol Med 2000;223:230-3.
10.
Haque UJ, Barlett SJ. Relationship among vitamin D,
4. Craig SM, Yu F, Curtis JR, et al. Vitamin D status and
disease activity, pain and disability in rheumatoid
its associations with disease activity and severity in
arthritis. Clin Exp Rheumatol 2010;28:745-7.
African Americans with recent-onset rheumatoid
11.
Szodoray P, Nakken B, Gaal J, et al. e complex role
arthritis. J Rheumatol 2010;37:275-81.
of vitamin D in autoimmune diseases. ScandJ Immunol
5. Leventis P, Payel S. Clinical aspects of vitamin D in the
2008;68:261-9.
management of rheumatoid arthritis. Rheumatology
12.
Holick MF. Vitamin D de ciency. N Engl J Med
2008;47:1617-21.
2007;357:266-81.
The Low Serum Concentrations of 25-Oh Vitamin D in Patients with Early Rheumatoid Arthritis
11
Medical Connections/Conexiuni Medicale
Con ict-of-Interest Statement
Medical Connections/Conexiuni Medicale (Med Con) requires all authors and reviewers to declare any
con icts of interest that may be inherent in their submissions.
Con ict of interest for a given manuscript exists when a participant in the peer review and publication
process-author, reviewer, or editor - has ties to activities that could inappropriately in uence his or her
judgment, whether or not judgment is in fact a ected.
Financial relationships with industry, for example, through employment, consultancies, stock
ownership, honoraria, expert testimony, either directly or through immediate family, are usually considered
to be the most important con icts of interest. However, con icts can occur for other reasons, such as
personal relationships, academic competition, and intellectual passion.
Public trust in the peer review process and the credibility of published articles depend in part on how
well con ict of interest is handled during writing, peer review, and editorial decision making. Bias can
often be identi ed and eliminated by careful attention to the scienti c methods and conclusions of the
work. Financial relationships and their e ects are less easily detected than other con icts of interest.
Participants in peer review and publication should disclose their con icting interests, and the information
should be made available so that others can judge their e ects for themselves.
Authors: When they submit a manuscript, whether an article or a letter, authors are responsible for
recognizing and disclosing nancial and other con icts of interest that might bias their work. ey should
acknowledge in the manuscript all nancial support for the work and other nancial or personal
connections to the work.
Reviewers: External peer reviewers should disclose to editors any con icts of interest that could bias
their opinions of the manuscript, and they should disqualify themselves from reviewing speci c
manuscripts if they believe it appropriate. e editors must be made aware of reviewers’ con icts of interest
to interpret the reviews and judge for themselves whether the reviewer should be disquali ed. Reviewers
should not use knowledge of the work, before its publication, to further their own interests.
Manuscript Title: ___________________________________________________________
I declare no con ict of interest
I declare the following potential con ict of interest:
_________________________________________________________________________
_________________________________________________________________________
_________________________________________________________________________
_________________________________________________________________________
_________________________________
_________________________________
Name
Signature/Date
Please fax or mail this signed form to the Med Con Editorial O ce.
Fax: +40-261-710456
Mail: colmedsm@gmail.com
ORIGINAL ARTICLES
DISCOURSE BETWEEN PARENTS AND THEIR CHILDREN ABOUT
SEX IN THE ARAB COMMUNITY IN ISRAEL
Joubran Samia1, Marcus Ohad2, Rath-Wolfson Lea6,8,Tova Hartman4, Iancu Iulian3,8, Weizman Abraham5,8,
Ram Edward7,8
1
e Bruce Rappaport Faculty of Medicine Technion-Institute of Technology and Emek Medical Center, 2Department of
Psychology,
e Yezreel Valley College, 3,8
e Yavne Mental Health Clinic, 4Department of Education and Gender Bar-
Ilan University Israel, 5,8Geha Mental Health Center, Petah Tikva, Israel, 6,8Department of Pathology, Hasharon Hospital,
Rabin Medical Center, 7,8Division of General Surgery, Hasharon Hospital, Rabin Medical Center, 8Sackler Faculty of
Medicine, Tel Aviv University
Address for correspondence:
Edward Ram
Division of General Surgery, Rabin Medical Center-Campus Golda
Petach Tiqva, 7 Keren Kaiemet St.
Tel: 972-3-9372323, Fax: 972-3-9372401
E-mail: edwardrm@netvision.net.il
Received: 10.01.2013
Accepted: 30.06.2013
Med Con October 2013, Vol 8, No 3, 13-20
Abstract
children about the religious values of sexual intercourse,
while Christians, especially the academic ones, talk with
Nearly half of the global population is less than
their children about contraception. We also found that
twenty- ve years old. Negative outcomes of early
all parents, mainly the religious Muslims, want to know
pregnancy, sexually transmitted infections, violence and
who their children meet with, where they meet them
alcohol consumption threaten the health of people in
and how intimate those meetings are. And nally, we
the second decade of life more than any other age group.
found that all parents, especially the non-religious one
Adolescence is a time of increased freedom to make
(both Muslim and Christian) believe they received
choices, and the ability of the adolescents to confront
either bad or very bad sexual education from their
these choices and make healthy decisions is crucial to
parents.
their development. Parents can have an important
Keywords: Discourse, Parents, Adolescents, Sex
in uence on their children’s behavior, parent-child
Education, Israeli-Arab sector, Muslims, Christians
relationships and parental monitoring and supervision
are associated with delayed sexual activity among
Introduction
children. e e ectiveness of such discourse may depend
on a range of factors, including the gender of the parent
When young people feel unconnected to home,
and the child, the level of relationship between them,
family, and school, they may become involved in
the parent’s attitudes toward adolescents’ sexual activity
activities that put their health at risk. Lack of discourse
and the parent’s ability to discuss sexuality openly and
between children and their parents a ects the children
comfortably. We found that Muslims, especially the
behaviors and attitudes.
ose who reported feelings
religious and non-academic ones, talk with their
like lack of parental warmth, love, or caring were more
Discourse Between Parents and Their Children about Sex in the Arab Community in Israel
13
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
likely to report emotional distress, lower self-esteem,
controversial for parents to express their sexual values
school problems, drug use, and sexual risk behaviors [1].
and beliefs to their children than for teachers or other
Parents can have an important in uence on their
educators to talk about sex in the classroom.
ird,
children’s behaviors. Studies indicated that supportive
greater parent-child discourse of values about sex and
parent-child relationships and parental monitoring and
use of contraception is associated under some conditions
supervision are associated with delayed sexual activity
with a delay in sex or greater use of contraception [10].
among children
[2].
e dynamics of parent-child
Discourse can help reduce sexual risk taking in teenagers
relationships and communications are greatly in uenced
such as unplanned pregnancies and sexually transmitted
by the culture and social environment in which they
diseases. Indeed, e ective education programs on sex
live. Parent-child communication on sexual issues
and sexually transmitted diseases or HIV often increase
remains a challenging issue. Most adolescents do not
parent-child discourse about sex [4].
seem to be comfortable talking about sexuality with
Israel is a valuable resource for providing a multi-
their parents [3].
religious approach to diverse issues. It represents a
e e ectiveness of such discourse may depend on a
variety of religions, ethnic groups, cultures, and
range of factors, including the gender of the parent and
traditions.
e State of Israel has some
7.4 million
the child, the level of relationship between them, the
inhabitants.
e most prominent characteristic of
parent’s attitudes toward adolescent sex and the parent’s
Israel’s population is its high diversity. Besides the main
ability to discuss sexuality openly and comfortably [4].
division of the country’s inhabitants into Jews (80%)
Most adults want youth to know about abstinence,
and Arabs (20%), there are many more subdivisions.
contraception and how to prevent HIV and other
e Jews, for example, are divided into religious and
sexually transmitted infections (STIs). However, parents
secular, while the latter include various immigrant
often have di culty discussing about sex. Studies have
communities that preserve their cultures. e Arabs are
shown that adolescents who reported feeling connected
divided into Muslims, Christians, and Druze.
e
to their parents and family were more likely than others
largest non-Jewish minority in Israel is the Arabs,
to delay initiating sexual intercourse. Teens who said
representing about one- fth of the country’s population.
their families were warm and caring also reported less
e vast majority of Israel’s Arabs are Sunni Muslims,
marijuana use and less emotional distress than their
with only about one-tenth being Christian. Cultural
peers [5]. In a study that explored the sources of rst
di erences between Jews and Arabs in Israel drive the
sexual discussion with children
[6], Moore and
basic values of each sector due to the cultural a liation
Davidson revealed that among unmarried college
derived from four origins: ethnicity, language, religion,
women, those who rst talked about sex with their
and nationality [11].
mother were more likely to use contraception at rst
In Christianity, the Church is the teacher of moral
sexual intercourse than those who learned about sex
and ethical norms; it has received the special mission of
from peers or teachers.
guarding and protecting the lofty dignity of marriage
Adolescence is a time of increased freedom to make
and the most serious responsibility of the transmission
choices, and the ability of the adolescent to confront
of human life. Sex education is a basic right and duty of
these choices and make healthy decisions is crucial to
parents and must always be carried out under their
development [7]. O’Sullivan et al. [8] suggested that for
attentive guidance, whether at home or in educational
some daughters sexual development causes con ict,
centers chosen and controlled by them. e mission to
which impairs discourse with their mothers and
educate demands that Christian parents should present
necessitates obtaining sex education from other sources.
to their children all the topics that are necessary for the
Today’s generation of adolescents is the largest in
gradual maturing of their personality from a Christian
history. Nearly half of the global population is less than
and ecclesial point of view [12]. In Islam, sexuality is
twenty- ve years old. Negative outcomes of early
considered part of identity as human beings: Islam is
pregnancy, sexually transmitted infections, violence and
explicit about many aspects of human sexuality. Also,
alcohol conception threaten the health of people in the
based on the Hadith showing the Prophet’s willingness
second decade of life more than any other age group [9].
to discuss these matters openly, it should be obvious
ose concerned with adolescent sexuality and
that education about matters related to sex is acceptable
reproductive health have striven to increase parent-child
[13]. Teaching about sex does not in itself o end against
discourse about sex for several reasons. First, increasing
modesty, indeed parents are urged not to feel shy or
such discourse is important in itself. Second, in some
embarrassed about providing necessary information
communities, it is more widely accepted and less
about sex to their children [13]. Explaining anatomy
14
Joubran et al
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
ORIGINAL ARTICLES
and the changes one’s body experiences during puberty
anonymously-ompleted questionnaires were sent back
are essential for enabling young people to grow up with
to the investigators by mail. Out of 1,000 questionnaires,
a healthy self-image. In an age where sexual activity in
797 were returned, for a response rate of 79.7%, which
many countries begins at an early age, Muslim
is a high response rate for the Arab community.
adolescents must be informed to better enable them self
to deal with peer pressure. Sex education can be taught
Results
in a way that informs young people about sexuality in
scienti c and moral terms [13].
We wanted to examine the di erences between
is study aims to answer the following questions:
Muslims and Christians regarding the relationship
1. Is there a correlation between parents’ religion
between parents and their children.
(Muslim or Christian) and their discourse with their
e rst thing we wanted to know is what sexual
children? Do the di erences between secular and
topics parents talked about with their children. We
religious parents and between academics and non-
found that 56.7% of the parents talked to their children
academics enhance this correlation?
about the religious values of sexual intercourse, 49.4%
2. Is there a correlation between parents’ religion
talked about puberty,
49.3% talked about sexual
(Muslim or Christian) and how liberal their approach is
intercourse and pregnancy, 48.2% talked about sexual
toward sexual education? Do the di erences between
diseases,
42.3% talked about postponing sex until
secular and religious parents and between academics
marriage and only 28.7% of the parents talked to their
and non-academics enhance this correlation?
children about contraception.
We found a signi cant and medium (Φ=0.20)
Research Methodology
correlation between the parent’s religion and the
religious values of sexual intercourse topic [χ(1)=28.44,
Participants
p<0.001], so that Muslim parents talked to their
e participants were 797 Israeli-Arab parents from
children about the religious values of sexual intercourse
all over Israel whose age range was between 20 and 66
(65.8%) more than Christian parents did (34.8%). In
(M=39). Among them were 371 Christians and 426
addition, among Muslims parents, we found a signi cant
Muslims, 208 males and 589 females; 533 live in cities
and medium (Φ=0.11) correlation between degree of
and 264 in rural areas or villages; 483 academics and
religiousness and the religious values of sexual
314 non-academics. In addition, 545 of the participants
intercourse topic [χ(1)=4.52, p<0.05], so that religious
de ned themselves as secular or traditional and 252
Muslim parents talked to their children about the
de ned themselves as religious or very religious.
religious values of sexual intercourse (71.7%) more than
Questionnaires
non-religious Muslim parents did (61.3%). We also
e study drew on questionnaires developed by
found a signi cant and weak
(Φ=0.15) correlation
Blendon [15] that consisted of forty-two multiple-
between degree of academic and the religious values of
choice questions that examine a parent’s attitude toward
sexual intercourse topic [χ(1)=8.18, p<0.005], so that
sex education.
e questionnaire was translated into
non-academic Muslim parents talked to their children
Arabic (two-way translation) and was proofed by an
about the religious values of sexual intercourse (74.3%)
Arab language specialist. From this questionnaire three
more than academic Muslim parents did (60.2%).
questions were utilized.
We found a signi cant and weak
(Φ=0.09)
e questions that guided this research are:
correlation between parents’ religion and the
(1) Which sexual topics do parents talk about with
contraception topic
[χ(1)=4.90, p<0.05], so that
their children?
Muslim parents talked to their children about
(2) What amount of detail do parents want to
contraception (25.3%) less than Christian parents did
know about who their children meet with? Do they
(32.8%). In addition, among Christian parents, we
wish to know where they meet them? Do they wish to
found a signi cant and weak
(Φ=0.17) correlation
know how intimate those meetings are?
between degree of religiousness and the contraception
(3) Are the parents more liberal nowadays than
topic [χ(1)=8.99, p<0.005], so that religious Christian
their parents were?
parents talked to their children about contraception
Procedure
(17.6%) less than non-religious Christian parents did
e questionnaires were provided to school
(36.9%).
administrators across the country, who sent them to
ere was no signi cant correlation between
randomly selected parents from their schools.
e
religion and any of the other topics, and no signi cant
Discourse Between Parents and Their Children about Sex in the Arab Community in Israel
15
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
In addition, we found a signi cant
di erence between Muslim and
Christian parents on the amount of
detail they want to know about where
their children meet [U(752)=64061.5,
p<0.05], so that Muslim parents (M
=392.99) wanted to know in more
detail where their children meet than
Christian parents did (M=358.44). In
addition, among Muslims, we found a
signi cant
di erence
between
Figure 1. Percent of parents who talked to their children
religious and non-religious parents on
about di erent sexual topics
the amount of detail they want to
know about where their children meet
correlation between degree of religiousness and academic
[U(393)=15597.5, p<0.001], so that religious Muslim
level for any of the other topics among Muslims or
parents (M =216.47) wanted to know in more detail
Christians. Figure 1 represents the above results.
where their children meet than non-religious Muslim
e second thing we wanted to know is what
parents did
(M=182.91). Also, among Muslims, we
amount of detail parents want to know about who their
found a signi cant di erence between academic and
children meet with, where they meet them, and how
non-academic parents on the amount of detail they
intimate are those meetings. We found that 64.8% of
want to know about where their children meet
the parents want to know in detail who their children
[U(393)=16132, p<0.05], so that academic Muslim
meet, 26.3% want just to know who their children
parents (M =187.28) wanted to know in less detail
meet, 8.2% want to know some part of who their
where their children meet than non-academic Muslim
children meet, and 0.7% do not want to know who
parents did (M=211.92).
their children meet. In addition, 64.8% of the parents
And nally, we found a signi cant di erence
want to know in details where their children meet,
between Muslim and Christian parents on the amount
24.9% want just to know where their children meet,
of detail they want to know about how intimate their
9.3% want to know some part of where their children
children’s meetings are [U(754)=69221, p<0.005], so
meet, and 1.1% do not want to know where their
that Muslim parents (M =397.43) wanted to know in
children meet. And nally, 62.6% of the parents want
more detail how intimate the meetings are than
to know in detail how intimate are their children’s
Christian parents did (M=355.45). In addition, among
meetings, 25.2% want just to know how intimate their
Muslims, we found a signi cant di erence between
children’s meetings are, 9.8% wants to know some part
religious and non-religious parents on the amount of
of how intimate their children’s meetings are and 2.4%
detail they want to know about how intimate their
do not want to know how intimate their children’s
children’s meetings are [U(396)=16258, p<0.005], so
meetings are.
that religious Muslim parents (M =215.73) wanted to
We also found a signi cant di erence between
know in more detail how intimate their children’s
Muslim and Christian parents on the amount of detail
meetings are than non-religious Muslim parents did
they want to know about who their children meet with
(M=185.81). Figure 2 represents the above results.
[U(768)=67144.5, p<0.05], so that Muslim parents (M
e third thing we asked the parents was whether
=400.30) wanted to know in more detail who their
they are more liberal than their parents were. We found
children meet with than Christian parents did
that 39.5% of the parents think they are more liberal
(M=366.96). In addition, among Muslims, we found a
than their parents were, 52% think they are partially
signi cant di erence between religious and non-
more liberal than their parents were, and 8.5% think
religious parents on the amount of detail they want to
that they and their parents are equally liberal. We also
know about who their children meet with
found a signi cant di erence between Muslim and
[U(404)=16903, p<0.005], so that religious Muslim
Christian parents about they thought if they are more
parents (M =220.15) wanted to know in more detail
liberal than their parents were [U(709)=57387, p<0.05],
who their children meet with than non-religious Muslim
so that Muslim parents (M=340.44) thought they are
parents did (M=189.55).
less liberal than their parents were than Christian
16
Joubran et al
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
ORIGINAL ARTICLES
parents did
(M=370.71). Figure
3
represents the above results.
e last thing we asked the
parents was what kind of sexual
education they received from their
parents. We found that 45.6% of the
parents think they received a very bad
sexual education from their parents,
30.2% think they received a bad
sexual education from their parents,
16.7% think they received a good
Figure 2. Amount of detail (in percent) that parents want to know who their
sexual education from their parents
children meet with, where they meet them and how intimate those meetings are
and only 7.6% think they received a
very good sexual education from their
parents.
In addition, although we did not
nd signi cant di erences between
the religions about what kind of
sexual education they received from
their parents [U(713)=61434.5, n.s.],
we did nd signi cant di erences
between the degree of religiousness
about what kind of sexual education
they received from their parents, both
Figure 3. Percent of parents who think they are more, partial more or equally
for Muslim parents [U(375)=15085.5,
liberal than their parents were, in general and divided into religion
p<0.05] and for Christian parents
[U(338)=7712, p<0.05], so that
religious Muslim parents (M=201.30)
think they received a better sexual
education form their parents than
non-religious Muslim parents did
(M=177.99) and religious Christian
parents
(M=192.23) think they
received a better sexual education
form their parents than non-religious
Christian parents did
(M=163.67).
Figure 4 represents the above results.
Figure 4. Percent of parents who think they received a very good, good,
bad or very bad sexual education from their parents were, in general
Discussion
and divided into religion and degree of religious
Education is an intentional structured process to
impart knowledge and skills and to in uence an
individual’s developmental course [14]. Sex education
Christian) and their liberal approach toward sexual
enables people to acquire knowledge and develop skills
education, and to nd out if the di erences between
that they can use to protect themselves and others [7].
secular and religious, and between academic and non-
Our study had two goals. e rst was to nd a
academic parents enhance this correlation.
correlation between parent’s religion
(Muslim or
In the present study only half of parents reported
Christian) and their discourse with their children, and
that they talk with their children about sex-related issues
to nd out if the di erences between secular and
and that more than half of them talk about religious
religious and between academics and non-academics
values and ethics of sexual education. Christians discuss
enhance this correlation.
e second was to nd a
contraceptive issues with their children more than
correlation between parent’s religion
(Muslim or Muslims. Secular Christians discuss birth control issues
Discourse Between Parents and Their Children about Sex in the Arab Community in Israel
17
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
more than more religious Christian parents. Secular and
capricious and unpredictable natural forces is equaled
religious Muslims demanded teaching values and morals
only by the subordination of women to men. According
of sexual education; among them the academic Muslims
to this approach, girls must be virgins until marriage. A
demanded these teachings more than non-academic
girl who is not a virgin would bring shame to her family
Muslim parents. Initiating conversations about sexual
and the husband would send her back to her parents. In
issues may be di cult for parents in communities like
some fundamental Muslim countries, they will even
the Arab community in Israel, as they may be unsure as
execute her.
to how to approach such issues. In 1979, Fox reported
Mernissi explain this situation accurately:
“Men
that less than half of the teens actually talked with parents
want access to women for brief sexual encounters before
about basic sexual matters such as the father’s role in
marriage, but once they have decided to marry, they
reproduction and one-quarter had never talked with
launch into a frantic search for a virgin whom no other
their parents at all, not even about menstruation [15].
man has
“de led”.
erefore, Israeli Arab parents’
e most consistent nding in sex education research
concern results from the fear that their children will do
over the past quarter century con rms what should be
things which will harm their future, like loss of virginity
intuitively obvious: children who grow up in families
and unwanted pregnancy.
where sexuality is openly discussed grew up healthier,
Parental supervision and regulation is also related to
had a longer childhood and were more responsible [16].
lower adolescent pregnancy risk.
An important issue in parent-adolescent discourse is
Teens whose parents closely supervise them are
determining why parents fail to engage in meaningful
more likely to be older when they rst have sexual
discussions with their children. Research has suggested
intercourse, have fewer partners and use contraception.
ve classes of concern that parents express about
However, some studies indicate that very strict parental
engaging in such conversations: not having the requisite
monitoring by parents is associated with greater risk of
knowledge and skills to explain things, concern that the
teen pregnancy, suggesting that less intrusive supervision
adolescent will not take the parent seriously, concern
may be more e ective [1].
with whether the communication will make a di erence,
Parents in our study were asked whether they are
di culties in nding the right time and place, and fear
more liberal than their parents. Half responded that
of encouraging sexual activity [17]. Some studies have
they were partially, and approximately 39.5% said they
examined the independent impact of sources such as
were more liberal than their parents. Here too,
parents, peers and media. For example, teenagers’ sexual
Christians were more liberal than Muslims. Liberal and
attitudes and behavior have been shown to be related to
sexual attitudes vary from person to person. ere are as
greater discourse from their parents
[10,17]. In our
many di erent liberal and sexual attitudes as there are
study most parents wanted to know everything about
people in the world. Some of the main in uences of
their children and their relationship with their partner,
liberal and sexual attitudes are socioeconomic
65% of both Muslims and Christians wanted to know
backgrounds, psycho-intellectual and educational
who and where the adolescent meets and how intimate
background, religious and spiritual beliefs, and family
are their encounters. Muslims wanted to know about
size. Children raised in small families receive more
their children more than Christians.
individualized
attention
from their parents.
Religious thought is of enormous in uence on
Furthermore, there are more nancial, economic, and
believers’ views and opinions concerning sexuality.
material resources allocated in small families [21].
Sexuality in Islam is not restricted to procreation as in
In Israel, the fertility rate among Muslim Arab
most other monotheistic religions. Islam does
women is very high compared with the fertility rate
di erentiate between
“legitimate” and
“illegitimate”
among Christian Arab women (2.9% vs. 1.2%). In
sexuality based on marital status [18]. Sexuality within
recent years, there is a downward trend in population
marriage is permitted and socially accepted. Sexuality
growth rate of Muslims in Israel. is decline in growth
outside of marriage is prohibited and socially
rate can be attributed mostly to their level of education
unacceptable [19]. As a consequence, sexuality is not
[11].
only subject to religious rules, but also has consequences
Many of the psychosocial aspects of sexuality, such
for people’s social, economic and public status [18].
as sexual attitudes, have been relatively unexplored in
e Israeli Arab sector is composed mostly of
diverse ethnic groups.
ere is much reason to believe
Christians and Muslims and both religions have a
that ethnic groups di er in sexual values, considering
Mediterranean culture. Mernissi
[20] described this
the disparate cultural, political, historical, and
culture as one in which the subordination of men to
18
Joubran et al
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
ORIGINAL ARTICLES
socioeconomic factors that in uence sexuality in each
in Israel, as they may be unsure as to how to approach
group [22].
such issues.
In the last question, parents were asked about the
Our research is among the few studies conducted
sex education that they received from their parents. e
on sex education in general and Arab society in
majority of them declared that they received no sexual
particular.
is is the rst study that examines the
education at all.
ere were no di erences between
di erences between Christians and Muslims, and the
Christian and Muslims.
rst to examine in-depth the subject of discourse
In the Middle East, cultural taboos are major
between parents and their children on these two
obstacles to informed discussion about sexual and
populations. Our study has contributed signi cantly to
reproductive health issues, particularly with regard to
sex education in Arab society in general, and in
adolescents. Premarital sexual relationships are
particular, it highlights the similarities that exist within
forbidden, and the silence stems in part from the high
this society
value that society puts on a girl’s virginity before
Acknowledgment: to Abhath
-
e Society for
marriage and the belief that talking openly about sexual
Developing Academic Research for her support and help
and reproductive health might encourage unmarried
carrying out this study.
youth to have premarital sex [4].
Parents who participated in the current study were
still teenagers about thirty years ago and they did not
References
receive any sexual education because in that time the
sexual education was not developed enough. In spite of
1.
Resnick MD, Bearman P S, Blum R W, Bauman KE,
the fact that in the past ve decades there has been an
Harris KM, Jones J, Udry JR. Protecting adolescents
increased liberalization of sexual attitudes and education
from harm: Findings from the National Longitudinal
and sexual education does not in itself o end against
Study on Adolescent Health.
e Journal of the
modesty, only half of parents reported that they talk
American Medical Association 1997;278,823-32.
with their children about sex-related issues; of those,
2.
Miller BC, Benson B, Galbraith D. Family
more than half of them talked about religious values and
relationships and adolescent pregnancy risk: A research
ethics of sexual education.
e public opinion of the
synthesis. Developmental Review 2001;21,1-38.
Arab community in Israel’s polls suggests strong support
3.
Carrera MA. Parents and their children learning about
for abstinence as a behavioral goal for adolescence.
sexuality. New York:
e Children’s Aid Society.
Retrieved on
Conclusion
advocatesforyouth.org/parents/experts/carerra.htm.
4.
Kirby D, Lepore G. Sexual risk and protective factors:
e aim of this research was to investigate parents’
Factors a ecting teen sexual behavior, pregnancy,
discourse with their children and to nd the correlation
childbearing and sexually transmitted disease.
between that discourse and the parents’ religion (Muslim
Washington, DC: National Campaign to Prevent
or Christian), education (academic or not) and degree
Teen and Unplanned Pregnancy, 2007.
of religiousness (secular or religious). We showed that
5.
Karofsky PS, Zeng L, Korosok MR. Relationship
only half of the parents talk with their children about
between adolescent parental communication and
sex related issues and if they do talk about sex, it is
initiation of rst intercourse by adolescents. Journal of
mostly about religious values and ethics. In addition,
Adolescent Health, 2000;28,41-5.
most parents wanted to know everything about their
6.
Moore NB, Davidson JK. Parents as rst information
children and their relationship with their partner,
sources: Do they make a di erence in daughters’ sexual
including who and where they meet and how intimate
attitudes and behavior? Journal of Sex Education and
are their encounters. Paradoxically, most of these same
erapy 1999;24(3),155-63.
parents think they are partially or more liberal than their
7.
Beyth-Marom R, Fischho B. Adolescents’ decisions
parents (who gave them no sexual education).
about risks: A cognitive perspective. In Schulenberg T,
Although there are minor di erences between
Maggs J, Hurrelmann K, (Eds.), Health risks and
Christian and Muslims parents, we believe that the Arab
developmental
transition
during
adolescence,
community is the main factor in parents not being
Cambridge: Cambridge University Press 1997, pp.
liberal enough. Initiating conversations about sexual
110-135
issues may be di cult for parents in the Arab community
8.
O’Sullivan LF, Meyer B, Heino FL, Watkins B.
Mother-daughter communication about sex among
Discourse Between Parents and Their Children about Sex in the Arab Community in Israel
19
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
urban African-American and Latino families. Journal
(Eds.), International encyclopedia of social and
of Adolescent Research 2001;16(3),269-92.
behavioral sciences
(14507-14513) Amsterdam:
9.
United Nations Population Fund. e state of the
Elsvier, 2001.
world population: Making one billion count investing in
17.
Fox GL. e family’s in uence on adolescent sexual
adolescents’ health rights. New York: UNFPA, 2006.
behavior. Children Today, 1979;8,21-5, 36.
10.
Miller BC. Families matter: A research synthesis of
18.
Ro man D. Sex and sensibility: e thinking parent’s
family in uences on adolescent pregnancy. Washington,
guide to talking sense about sex. Cambridge,
DC: National Campaign to Prevent Teen Pregnancy,
Massachusetts: Perseus Publishing, 2000.
1998.
19.
Jaccard J, Dittus P. Parent-adolescent communication
11.
Israel Central Bureau of Statistics. Press Release -
about premarital pregnancy. Families in Society
Publication Statistical Abstract of Israel 2007 - No. 58,
1993;74,329-43.
10/09/2007.
20.
Musso S, Fanget D, Cherabi K. An Arab-Muslim
aspx?itemID=7398
view. Prospect 2002;32,207-15.
12.
Pope Paul VI. Gravissimum educations 3. e Vatican,
21.
Gerholm L. Overcoming temptation: On masculinity
1965.
and sexuality among Muslims in Stockholm. Global
13.
Muslim Women’s League. An Islamic perspective on
Networks 2003;3,401-16.
22.
Mernissi F. Virginity and patriarchy. Women’s Studies
mwlusa.org/topics/sexuality/sexuality_pos.html
International Forum 1982;5(2),183-91.
14.
Noibi D. An Islamic perspective, in:
omason R.
23.
Darwin LT. e Religion and Family Connection:
(Ed.), Religion, ethnicity and sex education: Exploring
Social Science Perspectives. Deseret book company, Salt
the issues. London: National Children’s Bureau 1993,
Lake City: Utah, 1988.
pp. 41-57.
24.
Amaro H, Navarro A, Conron K, Raj A, On C.
15.
Blendon R. Sex education in America: General public/
Cultural in uences on women’s sexual health. In
parent’s survey. Cambridge; Harvard University, 2004.
DiClemente RJ, Wingood GM,
(Eds.), Women’s
16.
Schneewind KA. Socialization and education:
sexual and reproductive health. New York: Plenum,
eoretical perspective, in: Smelser NJ, Baltes PB.
2002, pp. 71-92.
20
Joubran et al
ORIGINAL ARTICLES
EPIDEMIOLOGICAL ASPECTS OF GASTRIC CANCER IN ARAD
COUNTY
Răducan Ionu Daniel, Ciobanu Gheorghe
Department of Life Sciences, “Vasile Goldiş” Western University of Arad
Address for correspondence:
Răducan Ionu Daniel
Phone 0740159500
E-mail: dani_raducan@yahoo.com
Received: 04.08.2013
Accepted: 10.09.2013
Med Con October 2013 Vol 8, No 3, 21-24
Abstract
e objective of the study is to identify the main
epidemiological aspects of gastric cancer in Arad County
Gastric neoplasm is one of the most common
between 2005 and 2011.
cancers of the digestive tract responsible for a still high
mortality. Although the prevalence, incidence and
Material and Methods
mortality of gastric cancer declined in the past 60 years
worldwide, according to data from Globocan, it is
In this study we followed the incidence of malignant
estimated that in Romania there are over 5,000 new
tumors of the stomach in Arad County between 2005
cases per year, and 4,000 deaths per year. Areas with
and
2011.
e statistical evaluation of patients
increased mortality are eastern Transylvania (Covasna,
diagnosed with gastric cancer during the studied period
Harghita), western Transylvania (Timiş, Arad, Bihor),
followed epidemiological factors such as gender, age or
Bucharest and Teleorman County.
area of origin, and the assessment of tumor process
Keywords: gastric cancer, epidemiology
extent according to the international TNM classi cation
(the
7th TNM staging of the International Union
Introduction to the subject and purposes
Against Cancer of gastric cancer) [3].
Study data were obtained from the Department of
Cancer is a worldwide major public health problem
Public Health Arad and represents the total number of
by the size of human, medical, economic and social
patients diagnosed with gastric cancer in Arad County
implications.
in the studied period. According to data obtained, the
According to research provided by the World Health
diagnosis was con rmed by radio-imaging and
Organization and
e Globocan Project, over
12
histological methods, and cases have been reported to
million people each year nd they are su ering from
the Public Health Department Arad.
cancer, and there are few who managed to beat the
disease. It is estimated that by 2030 the number of
Results
patients will double.
According to data provided by the World Health
Tables I, II and III summarize the main demographic
Organization and e Globocan Project, in Romania
data. During the studied period, 479 new cases of gastric
gastric cancer mortality ranks fourth after lung,
cancer were diagnosed. In
2005, the number of
colorectal and breast cancer [1,2].
diagnosed cases was 61; in 2006 - 78 cases; in 2007 -
Epidemiological Aspects of Gastric Cancer in Arad County
21
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
79 cases; in 2008 - 81 cases; in 2009 - 48 cases; in 2010
- 87 cases, and in 2011 - 45 cases (Figure 1).
166 patients were diagnosed in the age group 61-70
years, and 128 patients in the 71-80 years age group.
Analysis of the distribution of cases of gastric cancer
by patients’ gender in the studied period showed that
males were predominate with 294 cases (61.378% of
cases) compared with 185 females cases (39% of cases),
the di erence being statistically signi cant as p=0.1424.
Concerning the distribution of cases diagnosed
with gastric cancer in Arad County, we noted a higher
Figure 1. e incidence of malignant tumors of the stomach
incidence of cases among patients in rural areas - 249
in Arad County between 2005 and 2011
(52% of cases) compared with urban
patients
-
230
(48% of cases)
(p=0.0252).
Depending on patients’ age and
area of origin regarding the
distribution of cases of gastric cancer,
we noted that the number of people
diagnosed with gastric cancer was
higher after the age of 60 (315 cases)
and, in the same age group, cases in
rural areas were 183 compared with
132 cases in urban areas. In the age
group 30-60 years, 164 patients were
diagnosed with gastric cancer, of
which 65 cases were from rural areas
Figure 2. International TNM Classi cation of cases diagnosed
and 98 from urban areas.
with gastric cancer in Arad County between 2005 and 2011
e
International
TNM
Classi cation (the 7th TNM staging
of the International Union Against
Table I. Statistical data on the epidemiology
Cancer (UICC) of gastric cancer) of
of gastric cancer in Arad County in urban areas
cases diagnosed with gastric cancer in
General Data
Urban
this period shows only
24 cases
Gen-
Total
31-40
41-50
51-60
61-70
71-80
81-90
Year
diagnosed in stage I,
154 cases
der
nr.
years
years
years
years
years
years
diagnosed in stage II,
176 cases
M
38
0
2
5
6
4
2
2005
diagnosed in stage III,
95 cases
F
23
0
1
3
4
0
0
diagnosed in stage IV, and for 30 cases
M
53
1
3
3
8
5
3
the stage could not be determined
2006
F
25
0
3
1
3
3
1
(Figure 2).
M
47
3
5
6
9
2
2
2007
F
32
1
0
0
10
4
1
Discussions
M
49
1
5
4
3
3
0
2008
F
32
2
4
3
6
2
0
e main problem observed in
Arad County from the statistical study
M
29
0
4
5
2
2
0
2009
performed is that gastric cancer is
F
19
1
1
2
3
1
0
diagnosed in an advanced stage. e
M
51
1
5
7
8
7
1
2010
prevalence of gastric cancer was higher
F
36
1
2
5
12
3
1
in males and in people from rural
M
27
1
2
4
4
1
0
2011
areas.
e highest incidence of gastric
F
18
0
1
0
5
1
0
cancer cases diagnosed in Arad County
Total
479
12
38
48
83
38
11
was seen in people over 60. Most cases
22
Răducan et al
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
ORIGINAL ARTICLES
diagnosed with gastric cancer in this
Table II. Statistical data on the epidemiology
period were discovered in stage III
of gastric cancer in Arad County in rural areas
(Assessment of tumor process extent
General Data
Rural
according to TNM staging).
Gen- Total
31-40
41-50
51-60
61-70
71-80
81-90
Year
Comparing the statistical data
der
nr.
years
years
years
years
years
years
obtained with those from the
M
38
0
2
3
7
6
1
literature, we noted that the most
2005
F
23
0
0
1
8
5
1
common age groups a ected are those
over 60, but in the analysis performed
M
53
0
1
4
9
14
2
2006
we observed that gastric cancer was
F
25
0
2
3
3
6
0
diagnosed in 164 cases under the age
M
47
1
2
2
7
7
1
of 60. e literature indicates a small
2007
number of cases diagnosed before the
F
32
0
0
2
5
9
0
age of
60 compared with cases
M
49
1
4
6
9
10
3
diagnosed in Arad County in this age
2008
F
32
0
2
1
5
7
0
group.
e di erence in incidence
M
29
1
1
2
5
7
0
between
urban
/ rural areas is
2009
insigni cant, but it is higher in
F
19
0
3
3
4
1
0
disadvantaged social categories and
M
51
1
2
3
6
9
1
especially in rural areas [2,3,4,5].
2010
F
36
0
3
2
5
2
0
Following the statistical study
performed, we noted higher gastric
M
27
0
1
2
7
5
0
2011
cancer prevalence in males
(61%)
F
18
0
2
3
3
2
1
than in women (39%). e highest
Total
479
4
25
37
83
90
10
incidence of gastric cancer was found
in people over 60 in both patients
from urban and rural areas. An
Table III. Statistical data on the assessment
increased incidence of the disease is
noted in rural areas (52%) compared
of the tumor process extent according to TNM staging
to urban areas (48%).
General Data
Stage
Worldwide,
gastric
cancer
Gen- Total
NOT
Year
I
II
III
IV
represents approximately
930,000
der patients
DETERMINED
new cases and causes more than
M
38
0
8
17
13
0
700,000 deaths.
e average age at
2005
F
23
1
6
9
7
0
diagnosis is
71 in the U.S. and a
decade earlier in Japan [6].
M
53
1
15
18
14
5
2006
According to our data, this study
F
25
0
4
13
6
2
is the rst of its kind. Future research
M
47
3
13
18
8
5
should determine the causes of
2007
epidemiologic di erences in various
F
32
3
9
13
7
0
geographical areas.
M
49
1
13
20
12
3
2008
Acknowledgement: Vasile Goldiş
F
32
3
13
12
3
1
Western University of Arad. is work
M
29
3
6
12
7
1
was co nanced from the European
2009
Social
Fund through
Sectoral
F
19
1
6
9
2
1
Operational
Programme Human
M
51
3
27
9
9
3
Resources Development
2007-2013,
2010
F
36
1
15
11
2
7
contract no. POSDRU/107/1.5/S/77082
„PhD Scholarships Complex Training in
M
27
3
10
10
3
1
2011
Bio-Economy and Eco-Economy for
F
18
1
9
5
2
1
Food and Feed Safety and Security in
TOTAL
479
24
154
176
95
30
Anthropic Systems”.
Epidemiological Aspects of Gastric Cancer in Arad County
23
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
References
5. Ries L, Melbert D, Krapcho M, et al. Editori. SEER
Cancer Statistics Review, National Cancer Institute,
1.
Bethesda; 2007:1975-2004.
6. Anderson W, Camargo C, Fraumeni J, Correa P,
Rosenberg P, Rabkin C. Age-Speci c Trends in
4. Crew KD, Neugat AI. Epidemiology of Gastric Cancer.
Incidence of Noncardia Gastric Cancer in US Adults.
World J Gastroenterol.2006 ;12(3):354-62.
JAMA 2010;303(17):1723-8.
24
Răducan et al
ORIGINAL ARTICLES
ENVIRONMENTAL INFLUENCES ON ADDICTIVE BEHAVIOR OF
THE PEOPLE IN CLUJ COUNTY
Kelemen Alexander, Podea Delia, Puşchi ă Maria
Faculty of Medicine, “Vasile Goldiş” Western University of Arad, România
Address for correspondence:
Alexander Kelemen
Spitalul Clinic Minicipal Cluj, Psihiatrie Cr. II
126 Decebal St., Cluj-Napoca, Romania
E-mail: Phd.alexander.kelemen@gmail.com
Received: 23.04.2013
Accepted: 20.08.2013
Med Con October 2013 Vol 8, No 3, 25-28
Abstract
e drug was associated to religious rituals and this
conduit is found under the aspect of small customs in
Aim: e speci c objectives are de ned in matters
modern society (i.e. very few celebrations take place in
of data acquirements on issues like: consumers’
the absence of alcohol and tobacco).
prevalence of di erent psychoactive substances,
One of the factors in the emergence of formidable
identi cation of attitudes and knowledge among this
addictive behavior is the social pressure. It refers not
group in terms of drug-use, identify patterns of
only to family occasions, professional, social tolerance
consumption, identify risk and protective agents.
but to economic interests that are require for the selling
Materials and methods: e research method used
of drug [1]. erefore a lot of social preconceptions exist
was quantitative anamnestic psychological interview
regarding the addiction.
e drug reinforces, favors in
and the research instrument applied was a self-applied
some contexts social integration, plays a pledge role in
structured survey consisting of 40 questions regarding
adulthood and resonate with the individual’s own
the knowledge, attitudes, consumption practices of
di culties which is already su ering relational
vulnerable groups, as well as risk and protective factors
inhibition and uncertainty over their own values.
regarding tobacco, alcohol and illegal drugs.
Moreover self-restraint, surprising can lead to
Results: Drug addicts belong to diverse social
disregarding the individual, especially in settings where
layers, and some social groups seem to have a tendency
drug-abuse is a recurrent practice, even without the
towards addiction.
ere are statistically signi cant
existence of addictive risk [2,3].
correlations between addictive behavior throughout life
e epidemiological role of the socio-cultural
and the socio-demographic characteristics of the
factors is demonstrated by the di erent proportions of
subjects.
consumers integrated into social groups being either
Keywords: addiction, maladaptive behavior,
professional or a particular group of society. Addictive
anamnestic background
behavior is also found frequently in professions that
require harder, less quali ed work especially in
Introduction
professions that requiring contact with the public (e.g.
waiters, pigeons, and so on) [4]. A low educational level
Drug abuse is a phenomenon that can be found in
and poor living conditions seem also to be contributing
almost all studied societies from antiquity to nowadays.
factors in choosing to take drug.
Environmental Influences on Addictive Behavior of the People in Cluj County
25
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
Some addictive behaviors are easily recurring in
Data analysis
disadvantaged social classes than in the higher classes,
where there are hidden.
Data analysis was conducted using the SPSS
Sociological studies describe a high consumption
program and has aimed to establish the prevalence of
taken in relation to some cultural norms. In particular,
drug use by socio-demographic variables (i.e. classes,
excessive drug would preferentially occur in a context in
age, sex, education sapling, family environment,
which drug related rules exists and there are no
entourage), consumption models, the perception of the
prescriptive models [5,6]. So it happens in the so called
risk involved, so on. For each of this correlations were
anxious societies, nomadic societies, disorganized
calculated test of statistical signi cance.
communities in disadvantaged environments, especially
in some subcultures in the big cities where the
Results
consumption of alcohol, tobacco and other drugs are
more common [7].
General data
e research sample is build of 50 people from
Material and Method
which 32 (64%) male and 18 (36%) females. e age
distribution is as follows: 6 respondents under 18 years
e study is representative for population consisting
old, 36 subjects were maximum 30 years old and 8
of people with addictive problems in Cluj County.
subjects had over 30 years.
Database sampling was provided by ARAS Cluj and
Regarding the education 57.3% of respondents had
the Municipal Clinic Cluj Hospital - Department of
at least vocational courses, 27.9% of learners in a higher
Psychiatry.
e method was simple random sampling,
education establishment and 14.8% dropout known.
so any subject that is part of the covered category, have
From the environment of origin: 76% in the urban area,
equal opportunity to be part of the study, without any
20% have been living up to a lower age of majority in
discrimination criteria.
e group consisted of
50
the countryside and only 4% of respondents have rural
respondents, all the patients known to the psychiatric
origins (contact with the city being occasionally upbeat
center for methadone treatment.
social events and extracurricular activities).
e research method used was quantitative clinical
Heredo-collateral anamnestic data
interview and the applied research instrument was a
Most of those interviewed subjects were born and
structured questionnaire with 40 questions relating to
reared in the family of workers, with a satisfying
knowledge, attitudes, consumption practices of high-
educational level.
e distribution generated the
school students, as well as the risk and the protective
follow statistics: 8% of respondents said that parents
factors in consumption of tobacco, alcohol and illegal
followed school up to the 8 grade; 20.4% said that
drugs.
their parents have completed a vocational school;
e investigative techniques used for this study was
36,6% secondary education have about half of parents
the self-administered questionnaires. By conduct this
(53.2% of mothers and 43% of fathers); less than
research it was intended to ensure the con dentiality of
8.5% respectively 9.6% of subjects in the sample have
the interviewee’s anonymity.
parents with University studies; 14.2% do not know
e Form Design
- the structured interview
exactly the level of education of parents (either come
questionnaire was divided into strategic questions
from broken families or with parents who abandoned
covering all knowledge areas such as the views and
the family and in this case I can’t indicate the level of
attitudes towards consumption and consumer, the types
schooling).
of drugs covered by consumption, the age of onset for
Emotional ties in the family were described as only
drug use, consumers motivation, the availability of drugs
partially harmonic, the models of adaptation being built
on market and other risk and protective factors for drug
on constellations with prevalence in orality, the
use (self-esteem, involvement in school activities, leisure
relationship with the world and with the family drifted
mode, peer in uence in decision-making, authority and
between addiction and aggression and there wasn’t any
involvement of parents in children’s education, the
psychological development proposed to ascent.
ere
relationship with a group of friends).
were self-harming e ect behaviors and slow adaptation
e pretest interview was done on a signi cant
of self-image and the repetition automatism
number of respondents in Cluj Psychiatric Clinic
(theoretically there would be a traumatic event, never
patients with a diagnosis of chronic alcohol
integrated into psychic life). It could not establish a
consumption.
correlation in terms of socio-economic and social
26
Kelemen et al
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
ORIGINAL ARTICLES
environment of origin; instead it was observed a greater
fully aware of the e ects of drugs and the risk presented
frequency in those whose parents are consumers,
but still opted for occasional drug as a solution.
dependent on various psychotropic medications and in
Mental consciousness and the processing status
those that had broken families.
e locus of control
(Figure
2) assigned was
Drug-abuse occurrence
external to 84% of cases. Half (55%) of respondents
More than a third of the subjects reported mild
were motivated by curiosity consumption,
15% by
drug use (i.e. tobacco, alcohol, ethno botanical) at least
imitation, 8% had drug as an alternative to stress, while
once; over 60% of respondents wanted and repeated the
6% were intended to overcome a strong depressive
experience and more than one in ve subjects responded
state.
e rest of 16% designed the control locus to
positively to consumption in the last 30 days. From the
internal causes (in which 10% low self-trust and 6%
50 subjects researched, 32 were males and from those 29
shines related).
were diagnosed with drug-abuse other than tranquillizers
As regards to the events and personal history of
or sedatives. From the
18 female subjects,
14 were
childhood stand out that: an increased frequency of
diagnosed with benzodiazepines or tranquilizers.
treatment with psychotropic drugs in small childhood;
Generally man prefers marijuana or hashish, and women
early social placements; sub-standard school education;
tranquilizers or sedatives. Moreover, addiction prevails
house leaving
(i.e. family abandonment); sleep
within the male subjects.
distortions; nervous breakdowns; psycho-somatic
Regarding favorite locations and addiction
manifestations.
occurring possibilities, there statistically signi cant data
e association between the prevalence of drug
showing strong correlation between area of residence,
from respondents and how they relate to others, perceive
drug availability and the model used. Analysis of drug
themselves and make decisions is statistically signi cant.
access and a ord-ability for people in Cluj County
us, subjects who reported having used at least once in
indicates that: 33% from the interviewed subjects have
a lifetime drug, compared with those not consuming
absolutely no problem in acquiring the drugs, anytime
background experience di culties in asking for help
they want; 41% declared that it is di cult, but not
when they have problems and (63.6%) and believe that
impossible to acquire drugs; 6% acknowledged that it is
“the only way to deal with bullying is to let others
impossible to do so without the help of somebody; 20%
understand who’s boss”; have less con dence in
stated for the ‘I don’t know/I do not answer’ response
themselves, stating that “sometimes I think I am not
(Figure 1).
good for anything” (60.7%).
e motivation of drug abusers declared by the
investigated subjects is indicated mainly by curiosity
Discussions
(75%), supported by a strong desire to assert personal
a rmation and integration in a micro-groups. Curiosity
In the present study I started from a reality based on
is accompanied by a lack of accurate and complete
the assumption that addiction is the result of a triple
information on drugs and their e ects (75%). ere are
meeting between product, personality and the socio-
also cases (25%) were the respondents nevertheless were
cultural moment.
Figure 1. e accessibility and the availability
Figure 2. e drug abuser’s control locus
of drug acquiring for subjects from Cluj County
among Cluj county patients
Environmental Influences on Addictive Behavior of the People in Cluj County
27
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
e products may be the subject of toxic-maniac
References
addiction in some societies use, but in other cultural
context they are used and socially accepted.
1. Mitrofan, I. Terapia toxicodependen ei - posibilită i şi
e drug is associated with the religious rites and
limite [ erapy drugs dependencies - possibilities and
this conduct can be encounter under the form of small
limitations], Ed. Sper, 2003.
rituals in the modern societies (e.g. fewer festivities take
2. Ades J, et al. Le classi cations de l’alcoolisme, Ed.
place in the absence of alcohol and tobacco).
Masson, 1997.
One of the factors in the emergence of formidable
3. Biro, MA, Prolegomene clinice [Clinical Prolegomena],
addictive behavior is the social pressure. It refers not
Editura Dacia, 2001.
only to family occasions, professional, social tolerance
4. Magura, S. e role of work în substance dependency
but to the economic interests that are required in the
treatment: a preliminary overview. Substance Use and
selling of the drug.
Misuse, 2003.
e drug strengthening in certain contexts the social
5. Planul de Ac iune pentru Implementarea Strategiei
inclusion initiatives, it plays an adult status inductee
Na ionale Antidrog
[Action Plan for the
process and resonate with the individual’s own di culties,
Implementation of the National Drug Strategy]
which already is su ering relational inhibition and
2005-2008.
uncertainty over their values. In addition, abstinence,
6. Strategia Europeană privind Drogurile
[European
surprisingly can lead to the marginalization of the
Strategy on Drugs] 2005-2012.
individual, especially in environments where consumption
7. Winnicott W, et al. Procesuss de Maturation chez
is a common practice, even without the risk of addiction.
l’Enfant, Ed. Payot, 1978.
28
Kelemen et al
GENERAL REVIEW
ORAL MANIFESTATIONS IN PATIENTS WITH RED BLOOD SERIES
PATHOLOGY AND COAGULATION DISORDERS. REVIEW OF
LITERATURE
Pop Diana-Ioana, ovaru Şerban
Department of Oral Medicine, Faculty of Dentistry, Univerity of Medicine and Farmacy „Carol Davila” Bucharest,
Romania
Address for correspondence:
Pop Diana-Ioana, MD
42 Marasesti St., Bl. 1, Ap 121, Sector 4, PO 040255, Bucharest
Tel: 0742377610
E-mail: popdianaioana@yahoo.com
Received: 08.07.2013
Accepted: 15.08.2013
Med Con October 2013 Vol 8, No 3, 29-34
Abstract
whose diseases involve several medical specialties. Oral
pathology of hemopathies has long been neglected by
e present review describe the elementary lesions
dentists and patients were treated for their basic disease
observed in the oral cavity in cases of bleeding syndromes
in hematology clinics, intraoral manifestations of the
and disorders of blood erythroid series. It has been
disease not being considered a priority. It is absolutely
identi ed and described diseases of the red series
essential that your dentist should know the types of
(anaemiae, polyglobuliae) and coagulation disorders
bleeding disorders and oral manifestations that may
(involving both platelet and plasma coagulation factors)
occur in each of them. is way, such complications can
that can cause manifestationss in the mouth and brie y
be prevented and diseases can be treated early to prevent
described these events. Pale mucous, xerostomia,
any inconvenience. Dental procedures like extractions
atrophic glossitis, angular cheilitis, ulcers, gingival
and periodontal surgery are invasive procedures,
bleeding, petechiae, ecchymoses or swelling are common
commonly associated with posttreatment bleeding,
oral manifestationss, some of them being non-speci c
which stop by itself in most cases, if the patient does not
symptoms of coagulation disorders and disorders of
su er from bleeding disorders. A small but signi cant
blood erythroid series. Whether it occurs early, late
number of people presents clotting problems, for which,
during the disease or as an e ect of the treatment, oral
even minimally invasive interventions may lead to
manifestationss are non-pathognomonic and must be
increased risk of bleeding.
considered in their clinical and laboratory context.
Excessive bleeding is not only uncomfortable for
Patients’ dental treatment should be based on the basic
the patient, but can interfere with other medical
hematologic disease for each particular case.
procedures (eg suturing the wound) and can sometimes
Keywords: Hemorrhagic Disorders, Anemia, Oral
compromise the patient’s general health.
Manifestations
Lately, more and more people su er from congenital
or acquired blood disorders as a result of medications,
Introduction
diseases of other organs or alcohol
[1]. Dental
management of these patients should include an
During the past 10 years a growing attention has
accurate knowledge of these conditions by the dentist
been given to interdisciplinary therapies and patients
and his collaboration with the haematologist.
Oral Manifestations in Patients with Red Blood Series Pathology and Coagulation Disorders. Review of Literature
29
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
Oral manifestations of hemopathies have been
Plummer-Vinson syndrome is also called Paterson-
understood by dentists and hematologists in di erent
Kelly syndrome. It is a complex syndrome caused by
ways, according to the evolution, diagnostic methods
chronic iron de ciency
[9]. It is characterized by
and therapeutic advances of the disease.
atrophic glossitis and occasionally keratotic lesions on
Diagnosis of oral manifestations in coagulation
the oral mucosa. Dysphagia and oropharyngeal mucosal
disorders and diseases of the red series is very important
atrophy may be associated [3,10].
for the dentist and the daily practice.
e dentist must
alassemia is a constitutional anemia involving
recognize elementary lesions that occur in the oral cavity
defects in the synthesis of α and β polypeptide chains of
of patients with haematological background; make the
hemoglobin. Depending on the globin chain which has
di erential diagnosis of these lesions to those that occur
the quantitatively synthesis defect, thalassemias are
in other diseases and syndromes at intraoral level;
divided into two main groups: α thalassemia and
develop a treatment plan that takes into account possible
βthalassemia [7]. Oro-facial appearance of patients with
complications that may be associated with bleeding
thalassemia is known as Cooley facies: bosselation of
disorders or anemia [1,2].
frontal and parietal bones, increase of the maxillary
For remote diagnosis of hemorrhagic syndrome it is
bone which causes abnormalities of tooth implantation,
useful to review and acknowledge the basic patterns of
sometimes having monstrous aspects and modi ed
di erent oral lesions in association with modi ed blood
occlusion
(open bite, overjet or other forms of
counts: bleedings in case of thrombopenia, pallor and
malocclusion) [11]. Oral mucosa is pale most of the
glossitis in case of anemia, gingival hyperplasia in
times [11,12]. In cases of α thalassemia, patients are
polyglobulia, Hunter glossitis in Biermer anemia, etc
asymptomatic, but may sometimes have mild anemia,
[3]. Studies in recent years do not contain an adequate
expressed at oral level by mucosal pallor [12,13].
approach of this subject, only in the past decade there is
Biermer pernicious anemia
(megaloblastic
an interdisciplinary interest among dental medicine and
anemia) it occurs when a de ciency of vitamin B12
hematology, results being only a few.
exists. Intraorally, the pathognomonic sign is Hunter
is review presenting the main diseases of the
glossitis, which is the progressive atrophy of the liform
erythroid series and major blood coagulation disorders,
and fungiform papillae [14,15]. ey make the dorsal
their intraoral manifestations and therapeutic features
tongue look shiny red and smooth [15]. Tongue atrophy
for the major types of dental procedure.
can be installed progressively and sometimes complicate
by cracks and/or ulcerative lesions or blisters which
Oral manifestations in blood red series
become painful and sensitive to food contact [2,15,16].
pathology
Depapillation of the entire surface of the tongue can be
distinguished from other types of glossitis [6]. Hunter
Hemopathies of the red series (erythrocytes) are
glossitis is an important sign in Biermer anemia, and
divided according to their increase or decrease in
can occur at any time during the disease [17]. If anemia
anemia, respectively erytremia
(polycythemia or
comes rst, this is suggestive for the diagnosis of Biermer
erytroblastosis).
anemia and permits early treatment [14,18].
Iron de ciency anemia is the most common type of
Aplastic Anemia is a disease characterized by
anemia [4]. In the oral eld, manifestations are frequently
pancytopenia due to the reduced amount of
seen in the pale mucous membranes, xerostomia, aphthae
hematopoietic tissue in the bone marrow. e severity
lesions, atrophic glossitis, purplish-red in ammation
of symptoms depends on the degree of cytopenia [19].
areas, with adjacent pale gums [5]. Atrophic glossitis
At mouth level, gums bleeding and petechiae are mostly
manifests through a depapillated and erythematous
observed. Mucosa is pale, dry and atrophic; dorsal
tongue [4], which can be taken by mistake as migratory
tongue is smooth, ne and painful; angular cheilitis may
glossitis (in this case depapillated and erythematous areas
be present
[20]; sometimes we can notice mucosal
are surrounded by a keratotic halo) [6]. In some cases of
ulceration, superinfection with Candida albicans or
iron de ciency anemia, tongue can have a slight increase
viral infection, the latter being due to immunosuppression
in sensitivity to acid, spicy foods, etc, patients accusing a
(neutropenia, lymphopenia) [8,20].
sensation of stinging. Iron de ciency anemia is often
Sicklemia is a chronic hemolytic anemia related to
associated with atrophic glossitis, angular cheilitis and
the sickling phenomenon of erythrocyte (red blood cells
commissural ulceration [2,7]. Angular cheilitis can get
lose their normal shape, which get the aspect of „sickle”)
suprainfected with Candida albicans and/or other germs
under low oxygen tension
[1]. In this version of
and mucous dehydration can occur [8].
hemoglobin, glutamic acid in position 6 of the normal
30
Pop et al
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
GENERAL REVIEW
βchain is replaced by a valine molecule [21]. Sickle cell
a number of oral manifestations which include:
anemia is characterized by some oro-facial modi cations:
petechiae, hematoma of the tongue, [36] spontaneous
enamel hypomineralization and presence of diastema
gingival bleeding or prolonged gingival bleeding after
[22,23,24], decreased bone density at apical level [25],
surgical intervention
[37]. Minimal trauma such as
anesthesia or paresthesia of the mental nerve [26,27],
tooth brushing or chewing gum may cause prolonged
asymptomatic pulp necrosis
[28]. Mandibular
bleeding in time, even if the depth of the wound is not
osteomyelitis is a common complication observed in
signi cant [37].
patients with sickle cell disease, which is rarely
Vascular phase of hemostasis consists in a process
accompanied by other complications, facilitating
of local vasoconstriction which reduces vascular gap
diagnosis and treatment
[29]. Pain in the jaw can
size. If the vascular phase is altered (generally by an
precede inferior alveolar nerve neuropathy and
abnormality of the blood vessel wall), bleeding occurs
paresthesia of the lower lip. Gingival biopsy may reveal
more frequently at skin level, which expresses by
the presence of modi ed erythrocytes in the blood
petechiae, ecchymosis, or both. Vascular defect causing
vessels of the epithelium [30]. Saint Clair de Velasquez
the hemorrhage may be inherited or acquired [3,36].
reported in a study made on Venezuelan population that
Platelet phase comprises the following stages:
the most common intraoral manifestation in patients
adhesion, platelet aggregation and thrombocyte
with sickle anemia is pale mucosa and malocclusion in
secretion.
Abnormal bleeding associate with
these patients is often present and can be explained by
thrombocytopenia
(low platelets) or thrombasthenia
the changing perioral muscular balance [31].
(altered platelet function) and include: bleeding gums
Erythremia is a condition characterized by
and mouth, prolonged bleeding after surgical
increased red blood cell count (polyglobulia) and bone
intervention [38]. Glanzmann’s thrombasthenia is an
marrow hyperplasia. It is classi ed as polycythemia and
extremely rare abnormality that occurs intraorally by
erythroblastosis [3].
gingival bleeding, purpura and mucosal petechiae [39].
Polycythemia means increased hematocrit,
Clotting occurs through two separate pathways that
hemoglobin and total erythrocyte [32]. Intraorally, we
interact, the intrinsic and the extrinsic pathway.
e
can observe: gum congestion, oedematous, red-violet or
extrinsic pathway is activated by external trauma that
purple ulcerations, gingival bleeding, petechiae,
causes blood to escape from the vascular system.
is
ecchymosis, bleeding manifestations being accentuated
pathway is quicker than the intrinsic pathway. It involves
also by hyperviscosity syndromes [33,34].
factor VII. e intrinsic pathway is activated by trauma
Erythroblastosis is characterized by the appearance
inside the vascular system, and is activated by platelets,
of erythroblasts in the blood and can be observed after
exposed endothelium, chemicals, or collagen.
is
splenectomy, after acute hemorrhage and during any
pathway is slower than the extrinsic pathway, but more
signi cant hemolysis, especially in the hemolytic disease
important. It involves factors XII, XI, IX, VIII. Both
of the newborn. It expresses a reactive manifestation, a
pathways meet and nish the pathway of clot production
stimulation of erythropoiesis, triggered by the loss or
in what is known as the common pathway. e common
destruction of red blood cells. It can sometimes signify a
pathway involves factors I, II, V, and X [40].
primitive bone marrow involvement [7]. Erythroblastosis
Defects in coagulation stage can be conventionally
fetalis may be manifested in the teeth by deposition of
divided into two categories, rst patients with acquired
blood pigment in the enamel and dentin of developing
defects of certain factors (prothrombin, VII factor, IX
teeth giving them a green brown or blue color [35].
factor, X factor), which occur following the treatment
with anticoagulants, the de ciency of vitamin K and as
Oral manifestations of hemorrhagic
a result of liver disease (globin synthesis disorders).
e
syndromes
second categories, the patients with congenital defects
of one or more coagulation factors. In this group of
Under normal circumstances, hemostasis is carried
patients we can observe intraoral purple on the tongue
out in four stages which succeed in a perfect functional
and palate, intraoral hematoma, lips, tongue and oral
harmony: vascular phase, platelet phase, activation
mucosa ecchymosis, spontaneous or posttraumatic
phase of coagulation factors (the actual clotting) and
bleeding gums, prolonged bleeding after extraction.
physiological brinolysis phase. If there are defects in
Hemarthrosis and arthropathy can also occur (most
one or more of these phases, with the balance tilting
often in patients with hemophilia) in the
toward brinolysis, then phenomena of bleeding appear.
temporomandibular joint [35,36,37].
Coagulation disorders (acquired or inherited) may cause
Fibrinolysis phase - Gingival bleeding.
Oral Manifestations in Patients with Red Blood Series Pathology and Coagulation Disorders. Review of Literature
31
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
Dental management of patients with
minimal if treatment stages are carried out with
bleeding disorders
observance and attention.
Choice of drug therapy. Many prescription drugs
e management of patients with coagulation
in dental practice interfere with hemostasis. In addition,
disorders
depends largely
on the disease
other drugs like non-steroid anti-in ammatory agents
ethiopathogenesis, its severity and the type of dental
may potentiate the e ect of oral anticoagulants by
intervention to be carried out. If the dental procedure is
a ecting the platelet function, increasing the risk of
minimally invasive and the haematological disorder is
bleeding [48]. Penicillin, Erythromycin and Miconazole
compensated, dental maneuvers can be performed
also potentiate the e ect of Coumadin [49]. e dentist
without an increased risk.
must consider the patient’s current medication and
If the patient has a severe blood disorder, he needs,
consult with his hematologist to prescribe these drugs.
as far as possible, to treat the basic haematological
In conclusions the oral manifestations in
disease and subsequently ensure a rigorous hemostasis
hemopathies may have di erent chracteristic features,
[41].
depending on the background of haematological
Control of pain. In patients with coagulopathy,
diseases and related complications.
truncal peripheral anesthesia is counteraindicated
Hematologists and dentists should focus their
because there is a very high risk of developing a
attention on oral lesions when dealing with patients
hematoma [42]. Plexus and intraligamentous anesthesia
su ering from hemopathies, this fact being useful for
are preferred in case the treatment can not be carried
early recognition and treatment of various oral diseases
out without anesthesia. If possible, it’s advisable to use
that arise due to haematologic diseases. e dentist must
anesthetic with vasoconstrictor. Patients who undergo
be very familiar with the types of hemopathies and their
intensive treatment in hematology clinics must be fully
oral manifestations and be prepared to face an
anesthetized, and the intervention will be made
intraoperative bleeding, to achieve e cient haemostasis
intraoperatively.
and correct postintervention treatment and the patients’
Oral Surgery. Surgical procedures involve a high
dental treatment should be based on the basic
risk of bleeding, and the additional measures required to
hematologic disease for each particular case.
achieve hemostasis that must be used are: wound suture,
using a local hemostatic, pressure to the wound level,
using local thrombin, topical brin glue
[43] or
Bibliography
vasoconstrictor can be used individually or together
[44,45,46]. Treatment should be delayed until the
1. Schlosser BJ, Pirigyi M, Mirowski GW. Oral
patient has normal blood levels, and the haematologist
manifestations of hematologic and nutritional diseases.
gives its consent on the intervention [46]. If the basic
Otolaryngol Clin North Am 2011;44(1):183-203.
haematological condition persists, a preinterventional
2. Long RG, Hlousek L, Doyle JL. Oral manifestations of
balancing can be achieved using substitution treatment
systemic diseases. Mt Sinai J Med 1998;65(5-6):309-15.
with platelet concentrate, fresh plasma, concentrations
3. Adeyemo TA, Adeyemo WL, Adediran A, Akinbami
of coagulation factors [45].
AJ, Akanmu AS. Orofacial manifestations of
Periodontal Procedures. Periodontal health is of
hematological disorders: anemia and hemostatic
critical importance in patients with coagulation
disorders. Indian J Dent Res 2011;22(3):454-61.
disorders, to which gingival hyperemia and gums
4. McFarlane DB, Pinkerton PH, Dagg JH, Goldberg
bleeding may occur. Periodontitis can cause tooth
A. Incidence of iron de ciency, with and without
mobility and may require the need for extractions,
anaemia, in women in general practice. Br J Haematol
di cult to achieve in these patients [47].
1967;13(5):790-6.
Endodontic and restorative treatment. Restorative
5. Brunner C, Wuillemin WA. Iron de ciency and iron
procedures do not imply bleeding in patients with
de ciency anemia -symptoms and therapy. er Umsch
coagulopathies. However, we should take care not to
2010;67(5):219-23.
harm the gums by di erent procedures: application for
6. Şerban ovaru. Oral Medicine and Pathology. 2nd ed.
rubber dam clamp, subgingival grinding etc. Endodontic
Ed. Quintessence. Bucharest, 2012.
treatment is preferable to extraction in these patients
7. Delia Popescu Mut. Clinical Hematology. Ed.
whenever possible [37].
Medicală, Bucharest, 2001.
Prosthetic treatment.
is treatment should not
8. Zegarelli DJ. Fungal infections of the oral cavity.
represent an increased risk of bleeding, trauma being
Otolaryngol Clin North Am 1993;26(6):1069-89.
32
Pop et al
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
GENERAL REVIEW
9.
Ho man RM, Ja e PE. Plummer-Vinson syndrome. A
24.
Taylor LB, Nowak AJ, Giller RH, Casamassimo PS.
case report and literature review. Arch Intern Med
Sickle cell anemia: a review of the dental concerns and a
1995;155(18):2008-11.
retrospective study of dental and bony changes. Spec
10.
Demirci F, Savaş MC, Kepkep N, et al. Plummer-
Care Dentist 1995;15(1):38-42.
Vinson syndrome and dilation therapy: a report of two
25.
Brown DL, Sebes JI. Sickle cell gnathopathy: radiologic
cases. Turk J Gastroenterol 2005;16(4):224-7.
assessment. Oral Surg Oral Med Oral Pathol
11.
Cannell H. e development of oral and facial signs in
1986;61(6):653-6.
beta-thalassaemia major. Br Dent J 1988;164(2):50-1
26.
Friedlander AH, Genser L, Swerdlo M. Mental nerve
12.
Weatherall JD, Clegg JB. e thalassaemia syndromes.
neuropathy: a complication of sickle-cell crisis. Oral
3rd ed, Oxford: Blackwell Scienti c, 1981: pp. 132-
Surg Oral Med Oral Pathol 1980;49(1):15-7.
74.
27.
Gregory G, Olujohungbe A. Mandibular nerve
13.
Van Dis ML, Langlais RP. e thalassemias: oral
neuropathy in sickle cell disease. Local factors. Oral Surg
manifestations and complications. Oral Surg Oral Med
Oral Med Oral Pathol 1994;77(1):66-9.
Oral Pathol 1986;62(2):229-33.
28.
Andrews CH, England MC Jr, Kemp WB. Sickle cell
14.
Graells J, Ojeda RM, Muniesa C, Gonzalez J,
anemia: an etiological factor in pulpal necrosis. J Endod
Saavedra J. Glossitis with linear lesions: an early sign of
1983;9(6):249-52.
vitamin B12 de ciency. J Am Acad Dermatol
29.
Michaelson J, Bhola M. Oral lesions of sickle cell
2009;60(3):498-500.
anemia: case report and review of the literature. J Mich
15.
Field EA, Speechley JA, Rugman FR, Varga E,
Dent Assoc 2004;86(9):32-5.
Tyldesley WR. Oral signs and symptoms in patients
30.
Mendes PH, Fonseca NG, Martelli DR, Bonan PR,
with undiagnosed vitamin B12 de ciency. J Oral Pathol
de Almeida LK, de Melo LA, Martelli H Jr. Orofacial
Med 1995;24(10):468-70.
manifestations in patients with sickle cell anemia.
16.
Greenberg MS. Clinical and histologic changes of the
Quintessence Int 2011;42(8):701-9.
oral mucosa in pernicious anemia. Oral Surg Oral Med
31.
Saint Clair de Velasquez Y, Rivera H. Sickle cell
Oral Pathol 1981;52(1):38-42.
anemia oral manifestations in a Venezuelan population.
17.
Pontes HA, Neto NC, Ferreira KB, Fonseca FP,
Acta Odontol Latinoam 1997;10(2):101-10.
Vallinoto GM, Pontes FS, Pinto Ddos S Jr. Oral
32.
Lengfelder E. Diagnosis and therapy of polycythemia
manifestations of vitamin B12 de ciency: a case report. J
Vera in the era of JAK2. Dtsch Med Wochenschr
Can Dent Assoc 2009;75(7):533-7.
2013;138(7):331-6.
18.
Lu SY, Wu HC. Initial diagnosis of anemia from sore
33.
Carlson ER, Chewning LC. Polycythemia Vera in an
mouth and improved classi cation of anemias by MCV
oral surgical patient. A case report. Oral Surg Oral Med
and RDW in 30 patients. Oral Surg Oral Med Oral
Oral Pathol 1989;67(6):673-5.
Pathol Oral Radiol Endod 2004;98(6):679-85.
34.
Cao M, Olsen RJ, Zu Y. Polycythemia vera: new
19.
Brennan MT, Sankar V, Baccaglini L, et al. Oral
clinicopathologic perspectives. Arch Pathol Lab Med
manifestations in patients with aplastic anemia. Oral
2006;130(8):1126-32.
Surg Oral Med Oral Pathol Oral Radiol Endod
35.
Sambandan T. Review on Oral Manifestations of Blood
2001;92(5):503-8.
Diseases. JIADS 2010;1:41-3.
20.
Sepúlveda E, Brethauer U, Rojas J, Le Fort P. Oral
36.
Malfait F, De Paepe A. Bleeding in the heritable
manifestations of aplastic anemia in children. J Am
connective tissue disorders: mechanisms, diagnosis and
Dent Assoc 2006;137(4):474-8.
treatment. Blood Rev 2009;23(5):191-7.
21.
Embury SH, Matsui NM, Ramanujam S, Mayadas
37.
Gupta A, Epstein JB, Cabay RJ. Bleeding disorders of
TN, Noguchi CT, Diwan BA, Mohandas N, Cheung
importance in dental care and related patient
AT. e contribution of endothelial cell P-selectin to the
management. J Can Dent Assoc 2007;73(1):77-83.
microvascular ow of mouse sickle erythrocytes in vivo.
38.
Girolami A, Luzzatto G, Varvarikis C, Pellati D, Sartori
Blood 2004;104(10):3378-85.
R, Girolami B. Main clinical manifestations of a bleeding
22.
Kelleher M, Bishop K, Briggs P. Oral complications
diathesis: an often disregarded aspect of medical and surgical
associated with sickle cell anemia: a review and case
history taking. Haemophilia 2005;11(3):193-202.
report. Oral Surg Oral Med Oral Pathol Oral Radiol
39.
Toygar HU, Guzeldemir E. Excessive gingival bleeding
Endod 1996;82(2):225-8.
in two patients with Glanzmann thrombasthenia. J
23.
Okafor LA, Nonnoo DC, Ojehanon PI, Aikhionbare
Periodontol 2007;78(6):1154-8.
O. Oral and dental complications of sickle cell disease in
40.
Kasper DL, Fauci AS, Longo DL, Braunwald E,
Nigerians. Angiology 1986;37(9):672-5.
Hauser SL, Jameson JL. Harrison’s Principles of
Oral Manifestations in Patients with Red Blood Series Pathology and Coagulation Disorders. Review of Literature
33
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
Internal Medicine.
14th ed. Bucharest, Ed. Teora,
patients with bleeding disorders. Oral Surg Oral Med
2002, pp 372-9
Oral Pathol Oral Radiol Endod 2002;93(3):247-50.
41. Gómez-Moreno G, Cutando-Soriano A, Arana C,
46. Rayen R, Hariharan VS, Elavazhagan N, Kamalendran
Scully C. Hereditary blood coagulation disorders:
N, Varadarajan R. Dental management of hemophiliac
management and dental treatment. J Dent Res
child under general anesthesia. J Indian Soc Pedod Prev
2005;84(11):978-85.
Dent 2011 ;29(1):74-9.
42. Behrman, R. E. et al. Nelson Textbook of Pediatrics.
47. Agnihotri R, Bhat KM, Bhat GS, Pandurang P. Periodontal
17th ed. China: Saunders, 2004.
management of a patient with severe aplastic anemia: a case
43. Chabbat J, Tellier M, Porte P, Steinbuch M. Properties
report. Spec Care Dentist 2009;29(3):141-4.
of a new brin glue stable in liquid state.
romb Res
48. Brennan MT, Wynn RL, Miller CS. Aspirin and
1994;76(6):525-33.
bleeding in dentistry: an update and recommendations.
44. Adornato MC, Penna KJ. Hemostatic technique. Using
Oral Surg Oral Med Oral Pathol Oral Radiol Endod
a splint in oral bleeding. N Y State Dent J
2007;04(3):316-23.
2001;67(6):24-5.
49. Terezhalmy GT, Lichtin AE. Antithrombotic,
45. Piot B, Sigaud-Fiks M, Huet P, Fressinaud E, Trossaërt
anticoagulant, and thrombolytic agents. Dent Clin
M, Mercier J. Management of dental extractions in
North Am 1996;40(3):649-64.
34
Pop et al
GENERAL REVIEW
INTERMITTENT ANDROGEN DEPRIVATION IN TREATMENT OF
PROSTATE CANCER. REVIEW OF LITERATURE
Mureşanu Horia, Ioiart Ioan
Department of Urology, Vest University “Vasile Goldiş”, Arad, Romania
Address for correspondence:
Mureşanu Horia
Spitalul Clinic Jude ean de Urgen ă Arad
E-mail: hmuresanu@gmail.com
Received: 29.07.2013
Accepted: 17.08.2013
Med Con October 2013 Vol 8, No 3, 35-38
Abstract
a cancer survival bene t from re-exposure to endogenous
androgens.
Guidelines accept now intermittent androgen
Keywords: Intermittent androgen deprivation,
deprivation (IAD) in the treatment of prostate cancer in
quality of life, side e ects, prostate cancer survival
various clinical settings. Improvement of quality of life
(QoL) by reducing the side e ects during the o
-
In
1978, the concept of intermittent androgen
treatment phase was demonstrated in phase II trials.
deprivation (IAD) was rst suggested by Dr. Willett
Phase II/ III trials helped to clarify the description of
Withmore at Memorial Sloan Kettering Cancer Center
the ideal candidate for IAD
(low tumor burden,
(MSKCC), who gave this treatment to a patient, a
profound PSA response after initiation), but did not
competitive tennis player.
e patient was treated with
demonstrate equivalence/superiority in terms of
diethylstilbestrol
(DES) for prostate cancer (PCa) with
progression to castrate resistance and survival.
bone metastases and he become asymptomatic. His ability
IAD has four bene ts: improved quality of life,
to play competitive tennis was impaired by the hormonal
reduced incidence of side-e ects, decreased cost and the
therapy. Dr. Withmore discontinued the drug, and
potential for an improved duration of the androgen-
during the o -treatment intervals the patient’s tennis
dependent disease. All the evidence to date suggests that
improved dramatically. Once the bone metastases became
there is no decrease in prostate cancer (PCa) survival with
symptomatic again, therapy was resumed and the patient’s
IAD. e duration of the o
-treatment interval can be
symptoms resolved.
prolonged with the use of
5α-reductase inhibitors
After this experience at MSKCC a study with 20
(5α-RIs). Many questions remain still to be answered.
patients with advanced prostate cancer disease was
ese include the optimal induction duration of
conducted. Patients were treated in a similar fashion [1].
androgen deprivation therapy
(ADT), the optimal
e study was conducted in the pre- PSA and pre LHRH
trigger for re-treatment, the importance of complete
agonist era. Once the patients developed symptomatic
androgen blockade (CAB) versus monotherapy during
clinical progression, the treatment with DES was restored.
the induction period, the impact of 5α-RIs used in the
e disease progressed after a median period of 8 months.
o -treatment interval on the duration of androgen
Sexual activity was restored during the o
-treatment
dependence, and the issue of whether some patients derive
interval in 9 of 10 patients who were impotent during the
Intermittent Androgen Deprivation in Treatment of Prostate Cancer. Review of Literature
35
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
treatment. All patients had a rapid clinical response when
and a prostate-speci c antigen (PSA) level of 5 ng/ml or
treatment was restored.
higher received a luteinizing hormone-releasing hormone
In the early 70s, Bruchovsky described the prostate
analogue and an antiandrogen agent for 7 months. We
cell death after removing androgens from the prostate.
then randomly assigned patients in whom the PSA level
is active process termed autophagic lysis is known now
fell to 4 ng/ml or lower to continuous or intermittent
as apoptosis.
en in the 90`s he hypothesized that re-
androgen deprivation, with patients grouped according
exposure of PCa stem cells to androgen would re-induce
to prior or no prior hormonal therapy, performance
the androgen-dependent phenotype [2,3].
status, and extent of disease (minimal or extensive). e
An in vivo assay for stem cells was developed and with
co-primary objectives were to assess whether intermittent
this it was shown that the replacement of one-third or
therapy was non-inferior to continuous therapy with
more of the total stem cell compartment of the tumor by
respect to survival, with a one-sided test with an upper
androgen-independent stem cells represented a su cient
boundary of the hazard ratio of
1.20, and whether
condition for the establishment of castration resistance. In
quality of life di ered between the groups 3 months after
an attempt to avert or delay the progression to the
randomization [10,11].
androgen-independent state, they hypothesized that if
Hussain et al.
[10,11] enrolled a total of
3040
malignant cells which survived the androgen withdrawal
patients, of whom 1535 were included in the analysis:
are forced into a normal pathway of di erentiation by
765 randomly assigned to continuous androgen
androgen replacement, and then apoptotic potential
deprivation and 770 assigned to intermittent androgen
might be restored, thus setting the stage for another
deprivation. e median follow-up period was 9.8 years.
response to androgen withdrawal.
is theory was
Median survival was 5.8 years in the continuous-therapy
con rmed when apoptosis was induced multiple times in
group and 5.1 years in the intermittent-therapy group
the Shionogi tumor model by repeated cycles of androgen
(hazard ratio for death with intermittent therapy, 1.10;
withdrawal and replacement [4,5]. e same treatment
90% con dence interval, 0.99 to 1.23). Intermittent
protocol was applied to clinical prostate cancer a ording
therapy was associated with better erectile function and
an entirely new method of treating this disease which was
mental health (P<0.001 and P=0.003, respectively) at
termed intermittent androgen suppression [2-4].
month 3 but not thereafter. ere were no signi cant
e concept of allowing endogenous androgen levels
di erences between the groups in the number of
to recover and might prolong the duration of androgen
treatment-related high-grade adverse events.
dependence led to a substantial pre-clinical and clinical
e observations of various authors in the literature
research for intermittent ADT (IAD) [2-7].
can be summarized as follows: in the o
-treatment
IAD o ers a quadruple bene t: improved quality of
interval QoL returned to baseline levels [9,10,12,13],
life
(QoL) in the o -treatment interval decreased
PSA nadirs were at 95% of baseline levels, the rst o
-
cardiovascular- and osteoporosis-related morbidity, the
treatment interval in patients whose baseline PSA level
potential for a favorable impact on long-term disease
was <10, 10-20, and >20 ng/ml was 91, 65, and 39 weeks
control, and decreased costs. Few therapeutic modals can
respectively PSA nadir and baseline PSA level were
claim much bene t [7,8]! e key question is however,
powerful predictors for the duration of o
-treatment
whether this approach o ers equivalent (or prolonged)
intervals [14,15,16]. e duration of the o
-treatment
PCa-speci c and overall survival when compared with
interval shortened with each cycle.
is reduction in
continuous ADT.
the duration of the o
-treatment interval re ects the
e largest phase II study was in Canada on 110
gradual progression to androgen independence. By cycle
patients with biochemical failure after de nitive radiation
4, the median o
-treatment interval was 23-29 weeks,
therapy (RT). e results of this study were reported in
regardless of baseline PSA level. Testosterone level
three separate papers, including overall results [7], QoL,
recovered in most patients to >7.5 nmol/L in 75%, 50%,
morbidity results
[9], and biochemical results
[8].
40%, and 30% of men in cycles 1 through 4. is
Patients were treated for 9 months with LHRH agonist
recovery diminished with each cycle. During ADT the
therapy and cyproterone acetate (CPA), and re-treated
hemoglobin level dropped to an average of 11 g/L, and
when the PSA level reached 10 ng/mL.
recovered to baseline levels in the o
-treatment interval.
M. Hussain et al. reported in 2013 the results on
Time to androgen-independent progression was
intermittent versus continuous androgen deprivation in
predicted by baseline PSA level, PSA nadir on treatment, and
PCa [10].
duration of the o -treatment interval [8-11].
Men with newly diagnosed, metastatic, hormone-
ADT using LHRH agonist or antagonist has
sensitive prostate cancer, a performance status of 0 to 2,
advantages like reversibility, lack of tromboembolic e ects,
36
Mureşanu et al
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
GENERAL REVIEW
and absence of gynaecomastia. But androgen deprivation
What patient can be treated with
syndrome with hot ushes, loss of libido and erectile
intermittent androgen deprivation
dysfunction, decrease in energy, loss of bone mineral
therapy and how to use it?
density
(BMD) [17], loss of muscle mass, cognitive
impairment and the metabolic syndrome (MetS) develop
Patients with indication of ADT are candidates for
[13]. MetS is associated with more cardio-vascular side
IAD. Caution should be used in the following situations:
e ects and decreased survival.Osteoporosis is common in
a. Patients with bone metastases except if they have
men, and age related bone loss, alcohol abuse,
an excellent nadir PSA after induction therapy because
hypogonadism associated with prolonged ADT treatment
they have a relatively limited life expectancy as well as a
increase the risk for hip fracture. Fracture risk should be
reduced average o
-treatment interval [11,20,21].
assessed using the FRAX tool [18].
b. Patients with a very long time to PSA failure (>3
IAD trials are conducted in a di erent population
years) and PSA doubling time > 1 year have a long-term
from continuous ADT trials. IAD use conditional
PCa survival
(90-97% at 10 years).
ese patients
recruitment. Patients are treated for 3-9 months and
should be managed with delayed ADT; IAD could be
only responders are randomized.
considered at these points.
e EORTC 30902 trial
e rapid onset of e ect of GNRH antagonists,
suggests that the delayed therapy at a PSA trigger of >20
compared with GNRH agonists, may make them
ng/ml for men aged, 70 years and >50 ng/ml for men
attractive for an intermittent treatment strategy.
>70 years o ers an equivalent outcome to earlier
intervention [22,23].
Androgen deprivation therapy and the
c. Patients should be considered for IAD when
metabolic syndrome
their PSA is in the range of 10 ng/ml after PSA failure
with local therapy and intermediate risk based on PSA
A study reported by Keating et al. [19] showed that
kinetics and/or grade.
LH RH agonist therapy was associated with a higher risk of
d. Patients with nodal metastases, early ADT
diabetes, coronary heart disease, myocardial infarction
improves survival compared to delayed therapy. IAD is
and sudden cardiac death.
an appealing concept in these patients [4,24].
LHRH agonists have been associated with an
increased fasting plasma insulin level, early in the course
Conclusion
of the treatment.
Characteristics of ADT induced MetS are: the
IAD provides improved QoL, reduced incidence of
abdominal fat is mostly subcutaneous and not visceral;
side e ects, decreased cost, and has the potential for an
patients’ body weight and fat body mass increased by
improved duration of the androgen-dependent disease.
2.4% and
9,
4% high-density lipoprotein
(HDL)
To date, all the evidence suggest that there is no decrease in
cholesterol is maintained and not reduced [19].
PCa survival with IAD.
The e ect of intermittent androgen
deprivation therapy on side e ects and
Bibliography
quality of life
1. Klotz LH, Herr HW, Morse MJ, Whitmore WF Jr.
Improvements in QoL are based on the recovery of
Intermittent endocrine therapy for advanced prostate
testosterone during the o
-treatment interval.
cancer. Cancer 1986; 58(11):2546-50.
Bruchovsky et al. [7,9] shown that the incidence of side
2. Bruchovsky N, Rennie PS, Coldman AJ, Goldenberg
e ects was higher when patients were on treatment.
SL, To M, Lawson D. E ects of androgen withdrawal
Fatigue, dyspnea, and hematuria were the most common
on the stem cell composition of the Shionogi carcinoma.
symptoms recorded
(50.5%,
24.8% and
17,
4%).
Cancer Res 1990; 50(8):2275-82.
Myocardial infarction (7.3%), cerebrovascular accident
3. Bruchovsky N, Craven S. Prostatic involution: E ect
(6.4%) and deep vein thrombosis (5.5%) were relatively
on androgen receptors and intracellular androgen
frequent. Qol improved during the o
-treatment
transport. Biochem Biophys Res Comm
1975;
interval, as indicated by a return towards baseline levels
62(4):837-43.
in the scales depicting physical and work functions, hot
4. Akakura K, Bruchovsky N, Coldenberg SL, Rennie
ushes, impotence, sexual performance, urgency and
PS, Buckley AR, Sullivan LD. E ects of intermittent
nicturia.
androgen suppression on androgen-dependent tumors.
Intermittent Androgen Deprivation in Treatment of Prostate Cancer. Review of Literature
37
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
Apoptosis and serum prostate-speci c antigen. Cancer
14.
Goldenberg SL, Bruchovsky N, Gleave ME, Sullivan
1993; 71(9):2782-90.
LD, Akakura K. Intermittent androgen suppression in
5.
Gleave ME, Hsieh JT, Wu HC, von Eschenbach AC,
the treatment of prostate cancer: a preliminary report.
Chung LW. Serum prostate speci c antigen levels in
Urology. 1995; 45(5):839-44; discussion 844-5.
mice bearing human prostate LNCaP tumors are
15.
Oliver RT, Williams G, Paris AM, Blandy JP.
determined by tumor volume and endocrine and growth
Intermittent androgen deprivation after PSA- complete
factors. Cancer Res 1992; 52(6):1598-605.
response as a strategy to reduce induction of hormone-
6.
Mottet N, Lucas C, Sene E, Avances C, Maubach L,
resistant prostate cancer. Urology 1997; 49(1):79-82.
Wol JM. Intermittent androgen castration: a biological
16.
De la Taille A, Zerbib M, Conquy S, et al. Intermittent
reality during intermittent treatment in metastatic
androgen suppression in patients with prostate cancer.
prostate cancer? Urol Int 2005; 75(3):204-8.
BJU Int 2003; 91(1):18-22.
7.
Bruchovsky N, Klotz L, Crook J, Phillips N,
17.
Higano C, Shields A, Wood N, Brown J, Tangen C.
Abersbach J, Goldenberg SL. Quality of life, morbidity,
Bone mineral density in patients with prostate cancer
and mortality results of a prospective phase II study of
without bone metastases treated with intermittent
intermittent androgen suppression for men with evidence
androgen suppression. Urology 2004; 64(6):1182-6.
of prostate-speci c antigen relapse after radiation therapy
18.
for locally advanced prostate cancer. Clin Genitourin
19.
Keating NL, O’Malley AJ, Smith MR. Diabetes and
Cancer. 2008; 6(1):46-52.
cardiovascular disease during androgen deprivation
8.
Bruchovsky N, Klotz L, Crook J, Goldenberg SL.
therapy for prostate cancer. J Clin Oncol
2006;
Locally advanced prostate cancer-biochemical results
24(27):4448-56.
from a prospective phase II study of intermittent
20.
Sato N, Akakura K, Isaka S, e tal. Intermittent
androgen suppression for men with evidence of prostate
androgen suppression for locally advanced and metastatic
speci c antigen recurrence after radiotherapy. Cancer
prostate cancer: preliminary report of a prospective
2007;109(5):858-67.
multicenter study. Urology 2004; 64(2):341-5.
9.
Bruchovsky N, Klotz L, Crook J, et al. Final results of
21.
Calais Da Silva F.Goncalbes F, Santos A, et al. Phase 3
the Canadian prospective phase II trial of intermittent
study of intermittent monotherapy versus combined
androgen suppression for men in biochemical recurrence
androgen deprivation. J Urol 2006; 175(4):315 (abs.
after radiotherapy for locally ad-vanced prostate cancer:
974).
clinical parameters. Cancer 2006; 107 (2):389-95.
22.
Albrecht W, Collette L, Fava C, et al. Intermittent
10.
Hussain M, Tangen CM, Berry DL et al. Intermittent
maximal androgen blockade in patients with metastatic
versus Con-tinuous Androgen Deprivation in Prostate
prostate cancer: an EORTC feasibility study. Eur Urol
Cancer. N Engl J Med 2013; 368 (14):1314-25.
2003; 44(5):505-11.
11.
Hussain M, Tangen CM, Higano C, et al. Absolute
23.
Studer UE, Whelan P, Albrecht W, et al. Immediate or
prostate-speci c antigen value after androgen deprivation
deferred androgen deprivation for patients with prostate
is a strong independent predictor of survival in new
cancer not suitable for local treatment with curative
metastatic prostate cancer: data from Southwest
intent: European Organization for Research and
Oncology Group Trial 9346 (INT-0162). J Clin Oncol
Treatment of Cancer (EORTC) Trial 30891. J Clin
2006; 24(24):3984-90.
Oncol 2006; 24(12):1868-76.
12.
Higano CS, Ellis W, Russell K, Lange PH. Intermittent
24.
Messing EM, Manola J, Yao J et al. Immediate versus
androgen suppression with leuprolide and utamide for
deferred androgen deprivation treatment in patients
prostate cancer: a pilot study. Urology 1996; 48(5):800-4.
with node-positive prostate cancer after radical
13.
Tunn U. Can intermittent hormone therapy ful ll its
prostatectomy and pelvic lymphadenectomy. Lancet
promise? Eur Urol Suppl 2008; 7:752-7.
Oncol 2006; 7(6):472-9.
38
Mureşanu et al
GENERAL REVIEW
TREATMENT APPROACH OF ORAL LEUKOPLAKIA. REVIEW OF
LITERATURE
Părlătescu Ioanina1, ovaru Şerban1, Mihai Lelia2
1Oral Medicine Department, Faculty of Dentistry, University of Medicine and Pharmacy “Carol Davila”, Bucharest, 2Oral
Medicine Department, University of Medicine “Titu Maiorescu”, Bucharest
Address for correspondence:
Dr. Ioanina Părlătescu
Faculty of Dentistry, 4-6 Eforiei St., Bucharest
E-mail: ioaninap@yahoo.com
Received: 08.07.2013
Accepted: 10.08.2013
Med Con October 2013 Vol 8, No 3, 39-43
Abstract
pathologically as any other disease and is not associated
with any physical or chemical causative agent except use
Leukoplakia is the most frequent oral potentially
of tobacco [2]. Leukoplakia is a clinical term and has no
malignant disorder. Its diagnosis is established on
speci c histology. Pathological examination of
clinical and histological basis.
e main aim of oral
leukoplakia can show hyperkeratosis, atrophy, acanthosis
leukoplakia management is to avoid malignant
and di erent degrees of epithelial dysplasia. In evolution
transformation. In order to achieve this aim there are
leukoplakia demonstrates no pattern but it has a
several treatment options. ese vary from total surgical
tendency to malignant transformation. It is important
removal of the lesion to “a wait and see attitude”. ere
that the epithelial dysplasia has no speci c clinical
is no consensus of which is the best. e decision is up
appearance; it can be present in any apparently benign
to the specialist and it is adapted to every patient
clinical white lesion.
ere are two major clinical forms
according to the clinical appearance and histological
of leukoplakia: homogenous and non-homogeneous.
features.
e homogenous type has a at, thin and smooth
Keywords: leukoplakia, dysplasia, treatment
surface (Figure 1).
e non-homogenous form can be speckled (white
Introduction
and red areas but predominantly white), verrucous
(elevated, creased surface) (Figure 2) or nodular (small
Oral leukoplakia is de ned as a white patch of more
white nodules on the surface).
than 5 mm2 which doesn’t rub o and has an unknown
Oral leukoplakia can be a single lesion or it a ects
etiology or is tobacco induced. e WHO Collaborating
many locations thus being multifocal (Figure 3) - which
Centre for Oral Precancerous Lesions in 1978 de ned
is not considered a good sign.
oral leukoplakia as white patches which carry a risk of
Proliferative verrucous leukoplakia is a long term
malignant transformation [1]. Later on in 2007, an
progressive form which initially is homogenous, then
Oral Medicine Working Group designed to re ect the
slowly grows and spread [3]. Lately it involves multiple
advances in understanding of the biology of oral
mucosal areas with con uent, exophytic and proliferative
precancer, leukoplakia was de ned as a white patch or
features.
is kind of leukoplakia is reluctant to any
plaque that cannot be characterized clinically or
treatment, it has a high recurrence rate and occasionally
Treatment Approach of Oral Leukoplakia. Review of Literature
39
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
Dysplastic oral leukoplakia has a 5 times higher risk of
malignancy than non-dysplastic [5]. e patients with
histologically con rmed leukoplakia are reported to
have no malignant transformation in 86.6% after 3
years of follow-up and 82.0% after 5 years [2]. For a
period of 5 years follow-up dysplastic lesions had a
incidence of malignant transformation of
41% and
non-dysplastic lesions 9.5% [2].
Regardless of the advances in molecular biology,
nowadays there are no reliable markers to predict the
Figure 1. Homogenous leukoplakia of the
malignant transformation of oral leukoplakia [6].
e
retrocomisural mucosa in a hard smoker patient
markers Ki-67 (Mib-1) and p53, are considered to be
predictors for malignant transformation, but they are
not generally adopted in clinical practice
[6]. e
treatment options for oral leukoplakia are surgical and
non-surgical but there is no consensus of which is the
best.
e decision is adapted to every patient according
to the clinical appearance (size, location) and histological
features.
Surgical treatment
A consensus considered that surgery is the rst
Figure 2. Verrucous leukoplakia of the gingiva
choice in the management of oral leukoplakia [7], but it
has not been demonstrated that totally removing the
lesion will exclude the malignant transformation. A
randomized control study which evaluated surgical
treatment of leukoplakia does not show the e ciency of
the surgical treatment to assess the incidence of
malignisation
[8].
is does not mean that surgical
removal should be abandoned, mainly for histologic
diagnosis [7]. e surgical treatment is a diagnostic tool
which is used also in the evolution of oral leukoplakia as
part of its surveillance.
ere are di erent surgical techniques: laser, scalpel,
Figure 3. Multifocal leukoplakia of the oor of the
electrocauterisation and cryosurgery.
mouth small homogenous areas and a slightly elevated zone
e laser surgery has been reported as most
appreciated in the last 30 years [7]. ere are two main
bene ts of the laser: the haemostatic e ect and the
progress to verrucous carcinoma or squamous cell
limited scars post treatment. is can be performed for
carcinoma in the range 40-100% [4].
extensive lesions. It also has reduced post operative
Usually leukoplakia is used as a provisional diagnosis
discomfort but the main disadvantage is that the
when at the clinical examination a white lesion cannot
histological diagnosis of the excised area will be missing.
be certainly diagnosed as any other disease or disorder of
Furthermore comparing di erent laser techniques, CO2
the oral mucosa. A biopsy is necessary to establish the
laser, neodymium: yttrium aluminum garnet (NdYAG)
diagnosis. A de nitive diagnosis of leukoplakia is further
laser, and potassium-titanyl-phosphate (KTP) there are
established when any etiological cause
(other than
di erences in recurrence rates (34.2%, 28.9%, and 17
tobacco use) has been eliminated and the
%) [7,9].
histopathological examination was not speci c for other
Conventional surgery refers to scalpel excision of
disease [2].
the lesion. is is followed by secondary healing in case of
Epithelial dysplasia is considered the most
reduced mucosal defects or with a transposition of local
important indicator for malignant transformation.
mucosal aps or even skin graft in case of large defects.
40
Părlătescu et al
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
GENERAL REVIEW
Electrocoagulation can be used alone or as an
biological antioxidizing agent
[14]. A study
[18]
adjuvant to scalpel surgery. It induces thermal damage
evaluated lycopene in oral leukoplakia for a three
in the surrounding tissues thus causing postoperative
months period, with dosages regimes from 4mg/day and
pain and edema and tissue scarring.
8mg/day and patients had clinical resolution 25 and
Cryotherapy is a method which permits the
55%, respectively [14].
destruction of lesion tissue by freezing
Retinoic acid (Vitamin A)
in situ. It is carried out by either an “open” or a
Retinoic acid includes all the natural and synthetic
“closed” system [10].
e open-system cryotherapy is
compounds with an activity similar to that of Vitamin A
the direct application of cryogen on the lesion using a
[14]. is possibility of treatment is not widely accepted
cotton swab [11] or by an open spray [10]. e closed-
due to its side e ects-hypervitaminosis, toxicity,
system of cryotherapy brings a greater degree of control
teratogenic e ects, and alterations in various organic
with more complex and delicate apparatus [10,11]. e
systems [14].
main advantages of cryotherapy are the bloodless
e topical use of
13-cis retinoic acid has been
intervention, o reduced risk of post-operative infection,
shown to be e ective in resolving oral leukoplakia
and a the lack of scarring [12]. Some studies have
[15,19]. But they are limited because recurrences appear
shown cryotherapy as an alternative to treat oral
after short periods of cessation of the treatment [14,15].
leukoplakia [12]. During cryotherapy the ice crystals
In the systemic use with dosage of 300.000 IU of
are formed in both extracellular and intracellular uid
retinoic acid , a clinical resolution of the 50% has been
leading to the cellular dehydration, toxic intracellular
demonstrated [14].
electrolyte concentration, inhibition of enzymes,
In a recent study the results obtained on using
protein damage. ese mechanisms associated with the
topical retinoid for the treatment of proliferative
thermal shock induce the vacuolization of cells, their
verrucous leukoplakia, involving variable concentration
expansion and nally their rupture [12,13]. Also the
of tretinoin or isotretinoin in gel form (0.05% to 0.1%),
vascular changes are followed by ischemic necrosis of
are generally similar to those obtained with systemic
the treated tissue and immunological responses which
retinoid [20].
will produce the damage of tissue by cytotoxic immune
Bleomycin
mechanism [13].
Bleomycin, a cytotoxic antibiotic, is an alternative
treatment of oral leukoplakia. It is taken for squamous
Medical treatment
cell carcinoma of the head and neck region, oesophagus,
and skin [14]. e use of topical 1% bleomycin applied
Carotenoids
once daily resolved oral leukoplakia in 14 days [21]. It is
Betacarotene is a vitamin A precursor.
not very often used in practice for its adverse e ects
Carotenodermy (a state in which the skin becomes
(mucocutaneous reactions, which include stomatitis,
strongly yellowish) is the e ect of excessive beta-carotene
alopecia, pruritic erythema, and vesiculation of the skin)
intake disappears in a few weeks after the reduction of
[14].
consumption
[14].
Betacarotene function is
Photodynamic therapy
accomplished by ligation to oxygen, creating thus an
Photodynamic therapy is a noninvasive method of
unstable reactive molecule, which will reduce the
treatment for head and neck tumors [22]. It is based
damaging e ects of free radicals [15].
on photochemical reaction, initiated by light
Some studies report that clinical resolution of oral
activation of a photosensitizing drug causing tumor
leukoplakia ranges from
4% to 54%, with dosages
cell death. It requires the simultaneous presence of a
regimes from 20 to 90mg/day of beta-carotene in time
photosensitizing drug (photosensitize), oxygen, and
periods from 3 to 12 months[14,16].
visible light and it is a non-thermal reaction [23].
e
Lycopene
photosensitize
(aminolevulinic
acid-ALA)
is
Lycopene is a carotenoid without provitamin A
administered systemically by intravenous injection or
action [14]. It is a fat-soluble red pigment found in
can be topically applied. After a short time it is
some fruit and vegetables. ere is a positive relationship
collected in the target tissue and it is activated
between lycopene consumption and a reduction in the
exposure to low-power visible light of a drug-speci c
risk of the development of degenerative diseases caused
wavelength.
e result will be some reactive oxygen
by free radicals, such as cancer and cardiovascular
species which will induce damage to cell components
diseases [17]. Lycopene does bound to chemical species
(structural
proteins,
enzymes,
DNA, and
that react to oxygen, thus being the most e cient
phospholipids). e important structures of the organ
Treatment Approach of Oral Leukoplakia. Review of Literature
41
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
are maintained with good functional and cosmetic
Bibliography
outcome
[23].
ere are several photosensitizers
which have been developed and approved in time: (1)
1.
Kramer IR, Lucas RB, Pindborg JJ, Sobin LH.
photofrin has been approved in many countries for
De nition of leukoplakia and related lesions: an aid to
the treatment of esophagus cancer and lung cancer;
studies on oral precancer. Oral Surg Oral Med Oral
(2)
5-Aminolaevulinic acid was also approved in
Pathol 1978;46(4):518-39.
several countries for the treatment of skin cancer; (3)
2.
Warnakulasuriya S, Johnson NW, van der Waal I.
vertepor n for the treatment of macular degeneration
Nomenclature and classi cation of potentially malignant
(4) foscan is the only photosensitize that has been
disorders of the oral mucosa. J Oral Pathol Med
approved for the treatment of advanced squamous cell
2007;36(10):575-80.
carcinoma of the head and neck in Europe in the year
3.
Cerero-Lapiedra R, Balade-Martinez D, Moreno-
2001 [23]. ere are several studies [14,24,25] which
Lopez LA, Esparza-Gomez G, Bagan JV. Proliferative
reported the use of
5-Aminolaevulinic acid in the
verrucous leukoplakia: a proposal for diagnostic criteria.
treatment of oral leukoplakia with good results and no
Med Oral Patol Oral Cir Bucal 2010;15(6):e839-45.
recidives for 9 months follow-up.
4.
Bagan JV, Jimenez-Soriano Y, Diaz-Fernandez JM,et
Elimination of risk factors
al. Malignant transformation of proliferative verrucous
e ceasing of tobacco use is a prior action in case
leukoplakia to oral squamous cell carcinoma: a series of
of tobacco associated leukoplakia.
ere are no studies
55 cases. Oral Oncol 2011;47(8):732-5.
on groups of smokers to assess the malignant
5.
van der Waal I, Schepman KP, van der Meij EH,
transformation. But encouraging patient to stop
Smeele LE. Oral leukoplakia: a clinicopathological
smoking will reduce the incidence of leukoplakia and
review. Oral Oncol 1997;33(5):291-301.
can even resolve a large number of lesions [5,26].
6.
Smith J, Rattay T, McConkey C, Helliwell T,
Wait and see attitude
Mehanna H. Biomarkers in dysplasia of the oral cavity:
A possibility of treatment is a strict clinical and
a systematic review. Oral Oncol 2009;45(8):647-53.
histological surveillance.
is involves with frequent
7.
Lodi G, Porter S. Management of potentially malignant
clinic visits and biopsies
(of suspected lesions), but
disorders: evidence and critique. J Oral Pathol Med
without active intervention.
is form of treatment is
2008;37(2):63-9.
intended to diagnose a malignant transformation as
8.
Schwarz F, Maraki D, Yalcinkaya S, Bieling K,
soon as possible, thus giving the best possible prognosis
Bocking A, Becker J. Cytologic and DNA-cytometric
[7]. In present there are studies suggesting that the
follow-up of oral leukoplakia after CO2 - and Er:YAG-
natural history of leukoplakia might be independent
laser assisted ablation: a pilot study. Lasers Surg Med
from the treatment and there are some lesions destined
2005;37(1):29-36.
to malignant transformation regardless of the therapy
9.
Ishii J, Fujita K, Munemoto S, Komori T. Management
adopted [7].
of oral leukoplakia by laser surgery: relation between
recurrence and malignant transformation and
Conclusions
clinicopathological features. J Clin Laser Med Surg
2004;22(1):27-33.
e degree of epithelial dysplasia is mandatory for
10.
Leopard PJ. Cryosurgery, and its application to oral
the correct choice of the treatment. In the presence of
surgery. Br J Oral Surg 1975;13(2):128-52.
moderate or severe epithelial dysplasia, surgical
11.
Yeh CJ. Simple cryosurgical treatment for oral lesions.
treatment is recommended [7]. Mild dysplasia or the
Int J Oral Maxillofac Surg 2000;29(3):212-6.
absence of dysplasia can be completely removed or not.
12.
Yu CH, Chen HM, Chang CC, Hung HY, Hsiao
In this case the decision should consider clinical factors
CK, Chiang CP. Cotton-swab cryotherapy for oral
such as location, size and the patient’s engagement in
leukoplakia. Head Neck 2009;31(8):983-8.
smoking cessation [27].
13.
Reade PC. Cryosurgery in clinical dental practice. Int
Dent J 1979;29(1):1-11.
Acknowledgement:
is paper is supported by the
14.
Ribeiro AS, Salles PR, da Silva TA, Mesquita RA. A
Sectorial Operational Programme Human Resources
review of the nonsurgical treatment of oral leukoplakia.
Development (SOP HRD) 2007-2013, nanced from
Int
J
Dent
2010;2010:186018,
doi:
the European Social Fund and by the Romanian
10.1155/2010/186018.
Government
under
the
contract
number
15.
Kaugars GE, Silverman S Jr., Lovas JG, ompson
POSDRU/107/1.5/S/82839.
JS, Brandt RB, Singh VN. Use of antioxidant
42
Părlătescu et al
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
GENERAL REVIEW
supplements in the treatment of human oral leukoplakia.
22.
Kubler A, Niziol C, Sidhu M, Dunne A, Werner JA.
Oral Surg Oral Med Oral Pathol Oral Radiol Endod
Analysis of cost e ectiveness of photodynamic therapy
1996;81(1):5-14.
with Foscan
(Foscan-PDT) in comparison with
16.
Sankaranarayanan R, Mathew B, Varghese C, et al.
palliative chemotherapy in patients with advanced head-
Chemoprevention of oral leukoplakia with vitamin A and
neck tumors in Germany. Laryngorhinootologie
beta carotene: an assessment. Oral Oncol 1997;33(4):231-6.
2005;84(10):725-32.
17.
Riccioni G, Mancini B, Di Ilio E, Bucciarelli T,
23.
Kubler AC. Photodynamic therapy. Medical Laser
D’Orazio N. Protective e ect of lycopene in
Application 2005;20(1):37-45.
cardiovascular disease. Eur Rev Med Pharmacol Sci
24.
Zakrzewska JM, Lopes V, Speight P, Hopper C.
2008;12(3):183-90.
Proliferative verrucous leukoplakia: a report of ten cases.
18.
Nagao T, Ikeda N, Warnakulasuriya S, et al. Serum
Oral Surg Oral Med Oral Pathol Oral Radiol Endod
antioxidant micronutrients and the risk of oral leukoplakia
1996;82(4):396-401.
among Japanese. Oral Oncol 2000;36(5):466-70.
25.
Chen HM, Yu CH, Tu PC, Yeh CY, Tsai T, Chiang
19.
Kaugars GE, Silverman S, Jr., Lovas JG, et al. A
CP. Successful treatment of oral verrucous hyperplasia
clinical trial of antioxidant supplements in the treatment
and oral leukoplakia with topical
5-aminolevulinic
of oral leukoplakia. Oral Surg Oral Med Oral Pathol
acid-mediated photodynamic therapy. Lasers Surg Med
1994;78(4):462-8.
2005;37(2):114-22.
20.
Poveda-Roda R, Bagan JV, Jimenez-Soriano Y, Diaz-
26.
Roed-Petersen B. E ect on oral leukoplakia of reducing
Fernandez JM, Gavalda-Esteve C. Retinoids and
or ceasing tobacco smoking. Acta Derm Venereol
proliferative verrucous leukoplakia (PVL). A preliminary
1982;62(2):164-7.
study. Med Oral Patol Oral Cir Bucal 2010;15(1):e3-9.
27.
Warnakulasuriya S, Reibel J, Bouquot J, Dabelsteen
21.
Epstein JB, Gorsky M, Wong FL, Millner A. Topical
E. Oral epithelial dysplasia classi cation systems:
bleomycin for the treatment of dysplastic oral leukoplakia.
predictive value, utility, weaknesses and scope for
Cancer 1998;83(4):629-34.
improvement. J Oral Pathol Med 2008;37(3):127-33.
Treatment Approach of Oral Leukoplakia. Review of Literature
43
Transmittal Letter
In consideration of the Medical Connections/Conexiuni Medicale taking action in reviewing and
editing the above-named Article, e ective upon acceptance of the Article by the Medical Connections/
Conexiuni Medicale (hereinafter re ered to as Med Con), the Autor(s) hereby assign(s) to the Med Con,
its legal representatives, successors and assigns, all publishing rights and each and every other right to the
Article throughout the world, in any language and in any medium, whether as an audiovizual work,
collective work, compilation, derivative work, joint work, literary work, phonorecord, pictorial, graphic or
sulptural work, sound recording, work of visual art, computer program, or any other medium now existing
or which hereafter may come into existence, including the copyright and the right to register the copyright
as well as the right to secure any renewals, reissues, and extensions of any such copyrights in Romania or
in any foreign country. Author(s) may request permission to reuse the manuscript or portions thereof.
Such requests must be in writing and permission by the Med Con shall not be unreasonably withheld. e
Author(s) appoint(s) the Med Con as the Author’s(s’) attorney-in-fact to execute any documents the Med
Con deems necessary to record any of these grants with the Romanian copyright o ce or elsewhere. e
Autor(s) also warrant(s) to the Med Con that the Article is original work of the Author(s) except for
material in the public domain and such excerpts from other works as may be included with the prior
written permission of the copyright owners; that the Article has not been previously published, submitted,
or accepted for publication elsewhere; that the Author(s) have no relationship, nancial or otherwise, with
any manufacturers or distributors of products evaluated in this paper, or alternatively any such relationship
has been disclosed in a footnote to the paper, or the requirement is irrelevant to this paper.
Manuscript Title: ___________________________________________________________
Name:
Signature/Date:
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Please fax this signed form to the Med Con Editorial O ce.
Fax: +40-261-710456
CASE PRESENTATION
THIGH AMPUTATIONS IN DIABETIC PATIENTS WITH A HISTORY OF
FEMORAL OSTEOSYNTHESIS. CASE REPORT
Aiordăchioaie Gigi Adrian1, Pop Alexandru2, Dumnici Alexandru1, Fruja Dan2, Papiu Hora iu Sabin1,
Korodi Andrei1, Hărăguş Horia3
1Department of Surgery, “Vasile Goldiş” Western University of Arad, Romania, 2Department of Orthopaedics and
Traumatology, “Vasile Goldiş” Western University of Arad, Romania, 3University of Medicine and Pharmacy “Victor
Babeş” Timişoara
Address for correspondence:
Gigi Aiordăchioae, MD
Department of Surgery, “Vasile Goldiş” Western University of Arad
31 Henri Coandă St., Arad, 310429, Romania
Phone: 0040722166895
Email: gigi_aiordachioaie@yahoo.com
Received: 27.06.2013
Accepted: 12.08.2013
Med Con October 2013 Vol 8, No 3, 45-49
Abstract
the intervention was increased by the presence of metal
Ender rods, extraction being even harder in the case of
igh amputation in the diabetic patient is often an
the middle third amputation.
undesirable solution but life saving, when the
igh amputations in diabetic patients with femoral
gangrenous process is fast growing.
is mutilating
osteosynthesis raise particular problems of diagnosis and
intervention should be reserved only for cases where
treatment. Careful history and radiological examination
other therapeutic means, like vascular surgery and
are mandatory and they show the presence of internal
amputation at lower levels, have been exhausted.
rods. In these cases, the best amputation level is the
Presence of osteosynthesis rods in the thigh bone
third distal thigh, thus ensuring easy extraction of rods
consecutive to old fractures raises additional problems
and preservation of a long stump, with signi cant easing
related mainly to their extraction. Leaving a long stump
of further prosthesis.
allows using prosthesis in good conditions, allowing
Keywords: diabetes, infection, thigh amputation,
social rehabilitation of the patient and signi cantly
femoral osteosinthesis
alleviating his major postoperative handicap.
We discuss 2 cases of diabetic patients with femoral
Introduction
Ender rods that required amputation of the thigh, one
in the distal third, and the other in the medium third.
Lower extremity occlusive macroangiopathy is a
e peculiarity of these cases is the presence of internal
common complication of diabetes, often in elderly
rods which hampers the operation.
patients with associated pathology, with dramatic
igh amputations are made usually as distal as
evolution and raising serious therapeutic di culties
possible to preserve a long stump.
is objective was
[1,2]. Where reconstructive vascular surgery is exceeded,
achieved only in one of the two cases, while in the other
diabetic gangrene appears, amputation of segments of
we were forced to make the incision in the middle third
the lower limb becoming necessary. A prime objective of
due to the high progression of the infectious process as a
the ablative surgery is the removal of the gangrenous
result of late presentation. In both cases the di culty of
segment and stopping the ascending septic process,
Thigh Amputations in Diabetic Patients with a History of Femoral Osteosynthesis. Case Report
45
CASE PRESENTATION
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
saving the life of the patient in this way. A second goal,
which was treated surgically with internal xation with
also essential, is getting a healthy amputation stump and
Ender rods.
as long as possible, which then can support a prosthesis
Laboratory analyzes were pathologically altered
to allow a better social reintegration of the patient.
WBC - 21800/mm³, hemoglobin - 9.8 g/dl and glucose
Presence of osteosynthesis materials like the Ender rods
- 215 mg/dl. X-ray of the pelvis and thigh revealed the
in patients with an indication for amputation is a rare
presence of osteosynthesis material (Ender rods). An
situation that raises additional problems, related mainly
antibiotic
(ceftriaxonum 1gr/8h and metronidazolum
to the extraction. Usually, this is done through an
1gr/12h) and Actrapid insulin (0.5 U/kgC/day divided
incision in the lower 1/3 of thigh above the knee, which
into
4 doses) treatment was established. Emergency
is also the level indicated in thigh amputation realizing
surgery was indicated.
e chosen operative technique
the preservation of a long stump.
was thigh amputation above the knee, supracondylar,
Gritti-Stokes type (Figure 2 A,B,C,D).
is approach
Case Report
allowed a relatively easy removal of intramedullary rods
creating a long stump.
Case no. 1
e postoperative evolution was favorable, with
A male patient, 60 years old, from rural area, was
slow healing, and the patient was discharged 30 days
hospitalized in our clinic as an emergency, presenting
plantar and left ankle ulcerative-necrotic lesions and
signs of cellulitis extending to the medium 1/3 of left
calf evolving for 7 days (Figure 1). General condition of
the patient was altered; he was adynamic with super cial
breaths, oliguria and hypotension.
e medical history reveals type II diabetes
diagnosed 5 years earlier, treated with 1000mg, 2xday
metforminum, HBP stage II in treatment with
reserpinum
0,1 mg and dihidralazynum
10 mg, 2
Figure 1. Preoperative aspect of the lower limb
tablets/day and 40 mg propranololum (1/2 tablets/day)
(extensive skin necrosis with tissue loss
and chronic ischemic cardiopathy. Ten years ago the
on the external side of the left leg;
patient had su ered a fracture of the left distal femur
left ulcerative plantar lesion)
A
C
B
D
Figure 2. A: “Fish mouth” skin incision in 1/3 lower left thigh, B: Subcutaneous tissue incision,
C: Division of muscular plane; minimal bleeding, D: Femur sectioning in 1/3 lower left thigh
emphasizing internal metal rods (arrow)
46
Aiordăchioaie et al
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
CASE PRESENTATION
that the patient is a smoker and known with type II
diabetes for
10 years, treated with
500mgx2/day
metforminum and glimepiridum 2mg 1/day in the
evening.
e patient su ered
15 years ago a right
femoral trochanteric fracture due to which he underwent
internal osteosynthesis surgery with Ender rods.
e
current problem started suddenly 10 days ago, following
an injury with a blunt object, resulting in a 2/3cm calf
wound. e calf wound which was overlooked evolved
due to the patient’s diabetic state into gangrene.
e
blood work-up recorded the following pathological
changes: WBC 25,000/mm³, Hb 9.2 g/dl and glucose
253 mg/dl. X-ray of the pelvis and thigh showed similar
femoral internal rods which migrated slightly lower.
Emergency treatment with antibiotics
(ceftriaxonum
1gr/8h, gentamicin
40mg/12h and metronidazole
1gr/12h) and Actrapid insulin (0.5 U/kgC/day divided
into 4 doses) for the control of his diabetes was started
Figure 3. Residual limb at 1
Figure 4. Prosthetic stump
and emergency surgery was indicated. e ideal choice
year is normal with a supple
of the amputation level should be the lower third of
scar appearance
thigh. Because of the late presentation of the patient,
infection ascended to the top of the knee which forced
after the operation with a viable stump, which was used
us to perform amputation in medium 1/3 of thigh. e
for prosthesis (Figures 3,4).
chosen operative technique was the Marcellin-Duval
elliptic method (Figure 5 A,B,C,D).
e femur was
Case no. 2
sectioned in a circular mode by gentle rotating
A male patient, 68 years old, from rural area, was
movements and so the distal segment of the lower limb
hospitalized as an emergency case in our service with an
was removed successfully. We encountered additional
ulcerated and necrotic area of 10/15 cm in the 1/3
di culties compared to the rst case at the extraction of
medium of the right calf. Extensive edema and cellulites
Ender rods, but nally we managed to remove them by
involved the knee region. e personal history revealed
pulling them out progressively.
A
C
B
D
Figure 5. A: Elliptical skin incision lower third right thigh, B: Vertical incision towards the knee thus
identy ng one end of an Ender rod, C: Extractiong one of the three Ender rods, D: Amputation of the
femour in the lower third along with extraction of the remaining Ender rods
Thigh Amputations in Diabetic Patients with a History of Femoral Osteosynthesis. Case Report
47
CASE PRESENTATION
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
Discussions
relative ease if standard incision is adopted in the lower
third of the thigh by pulling out the distal end of the
Despite the profound mutilating nature of the thigh
rod. After operative wound is healed, we have
amputation, the prognosis of these patients can be
implemented a strategy for prosthesis and physiotherapy,
signi cantly improved by the development of prosthetic
establishing the prerequisites for a good social
possibilities and physiotherapy [3]. However, these are
reintegration.
e success of all these e orts depends
known to be dependent on the viability and size of the
primarily on the patient’s determination and moral
stump. Longer the lengths of stump better the recovery.
support of the family, which is also essential [3].
Choosing the optimal level of amputation has a crucial
role, being one of the most sensitive issues the surgeon is
Conclusions
facing when the upward progression of infectious
process is advanced.
e basic rule is to achieve
igh amputation of diabetic patients with femoral
amputation in the distal third of the thigh, like in case
internal osteosynthesis with Ender rods raises particular
no. 1, ideal situation even for patients with Ender rods
problems of treatment.
because it provides optimal conditions for extraction, as
Establishing the existence of rods is made by a
reported also by other authors [4,5].
careful anamnesis combined with consulting discharge
In neglected cases with cellulites above the knee, the
notes and radiological examination, required in these
incision is necessarily performed at a higher level, in the
situations.
medium 1/3 of the thigh, like in case no. 2. Of course,
In these patients the indication is an elective
this option has left a stump slightly shorter and therefore
sectioning of the distal third of the femur which ensures
more di cult to use for prosthesis and created additional
both easy extraction of rods and preservation of a longer
di culties for intraoperative rods’ extraction. On the
stump with signi cant easing of a further prosthesis.
other hand, amputation within the infected tissues, in the
e therapeutic management of these patients must
distal third of the thigh would have involved serious risk
not end with wound healing but should continue with
of stump gangrene, with dismal predictable consequences,
e orts related to prosthesis and physiotherapy.
perhaps even fatal ones [6].
erefore, to decrease the
Acknowledgements:
is work was supported by
number of high amputations with a high degree of
Structural Funds POSDRU/CPP107/DMI 1.5/S/77082
disability and di culties for prosthesis, it is necessary to
“Burse doctorale de pregătire ecoeconomică şi bioeconomică
educate the patients, encouraging early presentation in
complexă pentru siguran a şi securitatea alimentelor şi
case of potentially necrotic lesions [1,7]. Basically, patients
furajelor din ecosisteme antropice”.
with diabetes, atherosclerosis and thromboangeites
obliterans must examine their feet daily and go to the
doctor for any injury found. e surgeon will evaluate the
References
severity of lesions and will decide the treatment [2,8].
e presence of internal metal rods in patients with
1. Al-Wahibi AM. Impact of diabetic foot care education
gangrene requiring amputation of the thigh is a rare
program on lower limb amputation rate. Vascular
situation that raises particular problems.
e rst
Health and risk Management 2010;6:923-34.
requirement is primarily to establish the presence of
2. Jankovic D. Case study: shock waves treatment of
rods, which is not always easy, especially in patients with
diabetic gangrene. International Wound Journal
memory impairment or loss of lucidity, for example in
2011;8(2):206-9.
patients with Alzheimer’s disease. Such situations are
3. Rosati M, Lisanti M, Baluganti A, Andreani L, Rizzo
very rare but still, the possibility, forces us to a careful
L, Piaggesi A. A multidisciplinary approach and surgical
and properly managed history, including questions
tips in major amputations of diabetic patients.
about possible fractures and femoral osteosynthesis
Musculoskelet Surg 2012;96(3):191-7.
methods. When present, we must take into consideration
4. Johannesson A. Incidence of limb amputation in the
the new operative step, the extraction of metal rods.
diabetic and non-diabetic general population. A 10-years
In this sense it is useful questioning relatives, but
population - based cohort study of initial unilateral,
especially verifying old discharge notes from orthopedic
controlateral and reamputation. Diabetes care
services. Con rmation of the existence of rods is
2009;32:275-80.
achieved by radiological examination that is required in
5. Gray DWR. „Limb Amputation” in Morris PJ, Malt
such situations. Ender rods extraction in patients
RA. (sub red.), Oxford Textbook of Surgery. Oxford
undergoing an amputation of the thigh is done with
University Press, Oxford, 1994
48
Aiordăchioaie et al
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
CASE PRESENTATION
6. Wong K, Nicholson DJ, Gray R. Lower limb
diabetic, Ed. Niculescu, Bucureşti, 2005; pp 84-109.
compartment syndrome arising from fulminant
8. Stoia D, Hulpus R, Kiss I. Complica iile piciorului
streptococcal sepsis. ANZ J Surg 2005,75(8):728-9.
diabetic raportate gradului de ischemie cronică a
7. Patrascu T, Doran H, Catrina E, Buga C, Muntean A,
membrelor inferioare, Acta Medica Transilvanica
Sera nceanu C. Particularită i ale chirurgiei la
2011;2(3)149-50.
Thigh Amputations in Diabetic Patients with a History of Femoral Osteosynthesis. Case Report
49
ISSN 1843-9306
Revista „Medical Connections/Conexiuni Medicale” are o vizibilitate na ională şi interna ională
prin indexarea în Journals Master List a bazei de date interna ionale Index Copernicus®, începând
cu numerele din anul 2009, precum şi datorită includerii în cadrul schimburilor cu Universitatea
Titu Maiorescu, Bucureşti, Facultatea de Medicină şi Medicină Dentară, Sackler School of
Medicine a iată la Universitatea Tel Aviv, Hasharon Hospital, Centrul Medical Rabin din Israel
şi Universitatea de Vest Vasile Goldiş, Arad.
e journal “Medical Connections/Conexiuni Medicale” has a national and international
(ISSN e-serials 2068-8369), and due to the fact that the journal is included in an exchange
program between national and international universities such as Titu Maiorescu University,
Bucharest, Faculty of Medicine ans Dental Medicine, and Hasharon Hospital, Rabin Medical
Center A liated with Sackler School of Medicine, Tel Aviv University, and Vasile Goldiş Western
University of Arad, Romania.
e “Medical Connections/Conexiuni Medicale” is indexed in
Journals Master List of Index Copernicus®, isues since 2009
MEDICINE AND ART
THE DESCRIPTION OF THE SEQUELS OF POLIOMYELITIS IN ART
Bumbulu Călin1, Bumbulu Andrei2, Oprea Andrea2, Koren Rumelia3
1SCM dr Bumbulu -dr Balaj, Satu Mare, România, 2Faculty of Medicine, Iuliu Ha ieganu University of Medicine and
Pharmacy, Cluj Napoca, România, 3Department of Pathology, Hasharon Hospital, Petah Tikva, and Sackler Faculty of
Medicine, Tel-Aviv University, Israel
Address for correspondence:
Bumbulu Călin, MD, FP
Satu Mare, str. Bobocului UK 30-440258
Email: bumbulutcalin@yahoo.com
Received: 15.07.2013
Accepted: 10.08.2013
Med Con October 2013 Vol 8, No 3, 51-54
Abstract
Poliomyelitis comes from three Greek root words:
“Polio” meaning “grey”, referring to the grey matter;
e impact of polio on activity and participation
“Myelon” means
“spinal cord”, and
“Itis” means
can be seen in ancient Egyptian art. e rst modern
“in ammation”.
e disease was given its rst clinical
epidemics were fuelled by the growth of cities after the
description in 1789 by the British physician Michael
industrial revolution.
e artistic representation of
Underwood, and recognised as a condition by Jakob
de ciency and disability has evolved in parallel to the
Heine in 1840. e rst modern epidemics were fuelled
feelings of men and women in each period of history
by the growth of cities after the industrial revolution.
and, at the same time, their social evolution. In
e
e artistic representation of de ciency and disability
Fight Between Carnival and Lent painted by Pieter
has evolved in parallel to the feelings of men and women
Bruegel in 1559, two crippled gures appear; although
in each period of history and, at the same time, their
this artistic testimony is not formal proof of
social evolution. Nowadays, this concept continues to
poliomyelitis, it strongly suggests that both su ered
advance and some artists no longer represent the sick
from the disease. e drawing Studies of Beggars and
person, but instead the illness itself. As the years go by,
Vagrants from the same period, unknown whether is
human beings have evolved and, at the same time, so
by Hieronymus Bosch or Pieter Bruegel the Elder, also
have medicine and art. And therein lies the extraordinary
captures the cruel e ects of the disease. In
1899,
value, from the ontological point of view, of many works
Joaquín Sorolla represented a group of children
of art, which would never have been produced without
probably with sequels of poliomyelitis bathing at
the intervention of disease and the practice of the
Valencia’s beach. One of the best-known images in
medical art [1].
20th-century American art is Andrew Wyeth’s painting,
e impact of polio on activity and participation
Christina’s World, where the woman who su ered
can be seen in ancient Egyptian art. e Figure 1 present
from polio is saw making her slow crawl across the
a priest called Rom
(in other sources, a doorkeeper
yard.
named Roma or Ruma), makes an o ering, with a
Keywords: poliomyelitis, painting, drawing,
walking stick and foot deformities characteristic of polio.
Egyptian art, Pieter Brueghel the Elder, Hieronymus
Some medical scholars have interpreted Rom’s deformity
Bosch, Joaquin Sorolla y Bastida, Andrew Newell Wyeth
to be the result of polio; others believe that it is not polio
The Description of the Sequels of Poliomyelitis in Art
51
MEDICINE AND ART
MEDICAL CONNECTIONS • NUMBER 2 (30) • JUNE 2013
Figure 1. Egyptian stele (an upright stone carving)
dating from 1403-1365 BC
Figure 4. Hieronymus Bosch (?), Studies of Beggars and
Vagrants, pen and brown ink on paper, 1465-1559 (?)
Figure 2. Pieter Bruegel the Elder, e Fight Between Carnival
and Lent, oil-on-panel, 1559, Kunsthistorisches Museum, Vienna
Figure 3. Pieter Bruegel the Elder, e Fight Between Carnival
Figure 5. Hieronymus Bosch (?), Studies of Beggars and
and Lent, oil-on-panel, 1559, Kunsthistorisches Museum,
Vagrants, pen and brown ink on paper, 1465-1559 (?), detail
Vienna, detail
52
Bumbuluț et al
MEDICAL CONNECTIONS • NUMBER 2 (30) • JUNE 2013
MEDICINE AND ART
but a speci c type of clubfoot, with secondary wasting
and shortening of the leg. e mummie of the pharaoh
Siptah had a clubfoot and a withered leg, much like
Rom’s. As a child, Siptah was known to have contracted
a disease that left him with an atrophied leg; he walked
on it for several years before his bones matured.
In the sixteenth century, Renaissance painting
radiated from Italy across Europe. Many artists of
northern Europe responded by merging Italian classical
composition with the nely-detailed realism of Low
Countries painting. Yet the greatest Low Countries
painter of the sixteenth century, Pieter Bruegel the Elder
(c. 1525 - 9 September 1569), chose not to embrace
Italian art. Instead of classically-structured biblical
Figure 6. Joaquín Sorolla, Sad Legacy, oil, 1899
scenes, Bruegel preferred to chronicle the everyday lives
of peasants against realistic interiors and landscapes. e
Fight Between Carnival and Lent (Figure 2) is an work
painted by him in
1559.
is painting depicts a
common festival of the period, as celebrated in the
Southern Netherlands. It presents the contrast between
two sides of contemporary life, as can be seen by the
appearance of the inn on the left side - for enjoyment,
and the church on the right side
- for religious
observance. Two crippled gures appear in the painting,
one gure, who has a maimed leg, walks with a wooden
crutch
(Figure
3).
e other moves forward on his
hands, his shrunken and bent legs strapped to splints
and dragging behind him. e small “trestles” that the
Figure 7. Andrew Newell Wyeth, Christina’s World, 1948,
men are supporting themselves on were called “scabella”,
Museum of Modern Art, New York City
and the men
“scabellarii.” Although this artistic
testimony is not formal proof of poliomyelitis, it
strongly suggests that both su ered from the disease [2].
Andrew Newell Wyeth (July 12, 1917 - January 16,
e drawing Studies of Beggars and Vagrants
2009) was a realist painter. In his art, Wyeth’s favorite
(Figures
4,5), unknown whether is by Hieronymus
subjects were the land and people around him. One of
Bosch (c. 1450 - 9 August 1516) or Pieter Bruegel the
the best-known images in 20th-century American art is
Elder, also captures the cruel e ects of the disease [3,4].
his painting, Christina’s World (Figure 7).
e woman
Joaquin Sorolla y Bastida (February 27, 1863 -
in the painting is Christina Olson (3 May 1893-27
August
10,
1923) was a Spanish painter, born in
January 1968). Wyeth had a summer home in the area
Valencia, who excelled in the painting of portraits,
and was on friendly terms with Olson, using her and her
landscapes, and monumental works of social and
younger brother as the subjects of paintings from 1940
historical themes. His most typical works are
to 1968 [6]. But while the painting is ostensibly about
characterized by a dexterous representation of the people
her, Wyeth did not use Olson as a primary model.
and landscape under the sunlight of his native land. In
Instead, he called upon his wife who was in her mid-
August 1865 he and his sister were orphaned when their
twenties to pose for the scene, recreating the moment he
parents died, possibly from cholera. After completing
looked out the window and saw his neighbor, who
his military service, at twenty-two Sorolla obtained a
su ered from polio, making her slow crawl across the
grant which enabled a four year term to study painting
yard. Olson was 55 at the time Wyeth created the work.
in Rome, Italy. A long sojourn to Paris in 1885 provided
e painting of the young woman in a pink dress
his rst exposure to modern painting.
with wasted limbs has a haunting quality to it.
e
In 1899, Joaquín Sorolla represented, in a large
landscape and the rural house are all painted in great
canvas (Figure 6), a group of children probably with
detail. Each blade of grass and each strand of the
sequels of poliomyelitis bathing at Valencia’s beach [5].
woman’s hair is painted individually.
e style of the
The Description of the Sequels of Poliomyelitis in Art
53
MEDICINE AND ART
MEDICAL CONNECTIONS • NUMBER 2 (30) • JUNE 2013
painting has been termed
“magic realism” which is
2. Bonn, R. Painting Life. e Art of Pieter Bruegel e
de ned as an artistic genre in which meticulously realistic
Elder, Chaucer Press Books, 2006.
painting is combined with surreal elements of fantasy or
3. Friedländer, Max J. Early Netherlandisch Painting.
dreams. Wyeth commenting on his picture said: “ e
Volume V. Geertgen tot Sint Jans and Jerome Bosch,
challenge to me was to do justice to her extraordinary
Leyden: A.W. Slijthof, 1969.
conquest of a life which most people would consider hopeless.”
4. Cohn, V. Sister Kenny. e Woman Who Challenged the
Doctors. Minnesota Archive Editions, USA, 1975.
5. Martínez-Lage JF, Pérez-Espejo MA, Galarza M.
References
Portraying disease: Sorolla’s Sad Legacy. Childs Nerv
Syst
2012 Jul;28(7):959-61. doi: 10.1007/s00381-
1. Cano de la Cuerda R, Collado-Vazquez S. De ciency,
012-1687-y
disability,
neurology and art. Rev Neurol
6. h t t p s : / / w w w. m a i n e . g ov / e d u c a t i o n / l re s / v p a /
2010;51(2):108-16.
documents/CHRISTINAOLSONBIO.pdf
54
Bumbuluț et al
IN MEMORIAM
Professor Dr. Thoma Ionescu
(13th September 1860, Ploieşti - 28th March 1926, Bucureşti)
oma Ionescu is the founder of the romanian school of surgery and topographic anatomy,
honorary member of the Romanian Academy.
After the graduation of the „St. Sava” high school he enrolled at the Faculty of Medicine
in Paris in 1879, in 1892 becoming doctor in medicine and surgery. rough contest, in
1887 he obtained the position of associated anatomy prosector and then full prosector at
Faculty of Medicine Paris. He supports his doctoral thesis in
1892 with „L’evolution
intrauterine du colon pelvien”, obtaining the title of laureate of hospitals in Paris, after
winning in 1890 the title of laureate of Academy of Surgery in France for the work „Les
hernies intraperitoneales.” In 1892, through a contest where he became the rst,
oma
Ionescu got the title of associate professor. He collaborates with professors Poirier and Charpy at
the biggest treaty of anatomy at that time, in 1894, writing the chapter „L’anatomie de tube
digestiv” in which he describes for the rst time the duodeno-jejunal ssures, sigmoidian
ssures, rectal sheath and rectal ns. In 1895, by decree of law, the Faculty of Medicine in
Bucharest established the Department of Topographic Anatomy and Surgical Clinic, where he
is invited as a professor. In 1897, along with his colleagues, he founded the journal “Surgery”,
periodic of Romanian Society of Surgery. During the periods 1906-1912, 1921-1922 and
1925-1926 he is Dean of Faculty of Medicine, and from 1912 to 1915 Rector of University
in Bucharest.
oma Ionescu has published numerous articles about the cervical sympathetic chain
resection in the treatment of angina pectoris - “the Ionescu cure”, about total gastrectomy for
stomach cancer, and he developed original operatory techniques of trepanation, nephropexy,
splenectomy and radical cure of hernia. During visits in England and America in the years
1909-1910, he launched the “high spinal anesthesia” used to surgical intervention performed
on the upper chest and throat, making operatory demonstrations at renowned clinics in
London, New York, Philadelphia, Chicago, and at the famous Mayo brothers’ clinic in
Rochester.
Even today, in the famous Mayo Clinic is found the bust of the Romanian surgeon oma
Ionescu. By his name is linked the spreading of spinal anesthesia by narcosis, rst using a
mixture of stovaine and stricnine, then stovaine and ca eine. Eponymous associated besides
“Ionescu cure”: “Ionescu needle” for total metal wire suture, “Ionescu retractor” - abdominal
autostatic retractor on which can be xed valves of di erent sizes, “Ionescu operation” - total
larged hysterectomy with broad removal of lymph node groups.
He always gave proof of profound national attitude; in World War I, he was gone to Iaşi,
where he continued working as a surgeon, operating thousands of wounded soldiers coming
Professor Dr. Thoma Ionescu
55
IN MEMORIAM
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
from the front. e closure of “peace of Buftea” forced him to leave the country. In 1920 he
returns and resumes the research and teaching. He activates for the cause of union of
Transylvania with Romania ghting in Romanian National Council Unit in Paris, and from
1920 to 1921 he supports the interests of the country as Romania’s rst delegate to the League
of Nations sessions.
oma Ionescu was appointed delegate of Romania to the League of
Nations, and he took part in the rst session of the organization in Geneva. Brother of the
politician Take Ionescu, he was elected for several times as Deputy or Senator. A speech made
in 1906 in the Deputies Chamber reveals - in the extent that a political statement of any time
could be true - the shadows of the man oma Ionescu, on the one hand: challenging the
institution of rural physicians, or the county hospitals, disregarding of midwives and rural sub
surgeons, highlighting only the achievements of the Conservative Party, but on the other hand,
its bright beliefs, outlined also by Ion Cantacuzino “he did not know what it is hate, envy,
revenge, he did not know what it is sel shness”, by defending the interests of peasants saying
about the quality of medical services to the rural population: “what is not good for us it’s not
good either for peasant.”
In 1926 he dies at the age of 66, leaving behind a real school of Romanian surgery. He
was buried in Bellu Orthodox Cemetery, near the grave of Grigore Romniceanu, another
eminent surgeon.
Bumbulu Călin, Koren Rumelia
References
1. Vidu, V. Medalion aniversar: oma Ionescu. Jurnalul de Chirurgie, 2010;6(3):388-93.
3. Angelescu, N. oma Ionescu (1860-1926). Chirurgia, 2005;100(1):9-10.
4. Ciurea, AV, Palade, C. Professor oma Ionescu - founder of modern surgical practice in
Romania. Romanian Neurosurgery 2010,2:137-42.
5. Făgăraşanu, I. Via a şi opera lui Toma Ionescu, Ed Academiei Române, Bucureşti, 1962.
56
Bumbuluț et al
GUIDANCE FOR DRAWING UP
GUIDANCE FOR AUTHORS
Scope
on which patients or other subjects of your experiments
e Medical Connections publishes papers reporting
clearly grant permission for the publication of
original clinical and scienti c research, which contribute
photographs or other material that might identify them.
to the advancement of knowledge in all eld of medicine.
If the consent form for your research does not speci cally
e journal also publishes reviews, editorials and short
include this, please obtain it or remove the identifying
communications on speci c topics. Case reports will be
material. A statement must be included in the ‘Methods’
accepted if of great interest and well investigated. Letters
section of your paper.
to the Editor, especially those mentioning an opinion on
an article previously published, or expressing a new
Ethics Committee approval
nding are welcome. e website address of the Medical
You must state clearly in your submission in the
Connections is http://www.conexiunimedicale.ro.
e
Methods section that you conducted studies on human
journal is published quarterly and papers are accepted
participants with the approval of the Hospital, or
for publication in English language. Papers from
University Ethics Committee etc. Similarly, you must
contributors living abroad and from Romanian authors
con rm that experiments involving animals adhered to
should be addressed to the editorial o ce: dr. Bumbulu
ethical standards.
Călin, assitant editor in chief of Medical Connections,
Eroilor Revolu iei Pl. no.23-440055 Satu Mare,
Copyright assignment
Romania. Tel./Fax:
+40-261-710456,
e-mail:
Papers are accepted for publication on the
bumbulutcalin@yahoo.com.
understanding that exclusive copyright in the paper is
assigned to the Publisher. Authors may use material
Redundant or duplicate publication
from their paper in other works published by themselves.
We ask you to con rm that your paper has not been
published in its current form or a substantially similar
Submissions
form, that it has not been accepted for publication by
All manuscripts submitted to the Medical
another journal, and that it is not under consideration
Connections are made available for online review.
e
by another publication.
journal introduced the electronic submission of
manuscripts in Word format, but also accepts
Con icts of interest
manuscripts submitted as attachments to electronic
We ask authors to state all possible con icts of
mail (text, gures and tables). Do not send them in
interest, including nancial and other relationships. If
PDF format. e word count for electronic submissions
you are sure that there is no con ict of interest, please
is up to 3,500 words for original articles, 2,500 words
state this also.
e sources of funding should be
for case reports, 2,000 for clinical imaging papers, 500
acknowledged in your paper.
words for letters, and 4,500 words for review articles.
Authors should NOT in addition post a hard copy
Permissions to reproduce previously
submission to the editorial o ce, unless they are
published material
supplying artwork, letters or if les that cannot be
Please send us copies of permission to reproduce
submitted electronically, or have been instructed to do
material (such as illustrations) from the copyright holder.
so by the editorial o ce. For those authors who have no
option but to submit by mail please send one copy of
Patient consent forms
the article, plus an electronic version on CD-ROM to
e protection of a patient’s right to privacy is
the Editorial O ce, Conexiuni Medicale/Medical
essential. Please send copies of patient’s consent forms
Connections, Eroilor Revolu iei Pl. no.23-440055 Satu
57
GUIDANCE FOR DRAWING UP
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
Mare, Romania. Double spacing should be used
Review articles and case reports should include an
throughout the manuscript, which should include the
unstructured summary.
following sections, each starting on a separate page: title
Key words
page, abstract and key words, text, acknowledgements,
e abstract should be followed by a list of 3-10
references, individual tables and legend for gures. Pages
keywords or short phrases which will assist the cross-
should be numbered consecutively, beginning with the
indexing of the article and which may be published.
title page, and the Arabic numbers should be placed in
When possible, the terms used should be from the
the top right hand corner of each page.
Medical Subject Headings 262 list of Index Medicus
Presentation of papers
Text
Title page
Full papers of an original study may be divided into
e title page should carry the full title of the paper
sections headed Introduction, Methods (including ethical
and a short title to be used as a short ‘running head’ (and
and statistical information), Results and Discussion
which should be so identi ed and should comprise up to
(including a conclusion).
is so-called
“IMRAD”
45 characters).
e rst name, middle initial and last
structure is not simply an arbitrary publication format,
name of each author should appear. If the work is to be
but rather a direct re ection of the process of scienti c
attributed to a department or institution, its full name
discovery. Long articles may require subheadings within
should be included. Any disclaimers should appear on the
some sections (especially the Results and Discussion
title page, as should the name and address of the author
sections) to clarify their content. Other types of articles,
responsible for correspondence concerning the manuscript
such as case reports, reviews, and editorials, are likely to
and the name, address and e-mail address of the author to
require other formats. Excessive use of abbreviations is
whom requests for reprints should be made (the author
not recommended. Outline statistical methods used.
should mention if he does not want his e-mail address to
Identify drugs and chemicals used by generic name (if
be published). Finally, the title page should include the
trade-marks are mentioned, manufactured name and
sources of any support for the work in the form of grants,
city should be given).
equipment, drugs, or any combination of these.
Acknowledgements
Abstracts
Acknowledgements should be made only to those
e second page should carry a structured abstract
who have made a substantial contribution to the study.
of no less than 200 words. Do not use abbreviations,
Authors are responsible for obtaining written permission
footnotes, or references.
from people acknowledged by name in case readers infer
Background & Aims
their endorsement of data and conclusions.
Describe the importance of the study and the
References
precise research objective(s) or study question(s).
References should be numbered consecutively in
Methods
the order in which they rst appear in the text.
ey
Methods should include information on the following
should be assigned Arabic numerals, which should be
aspects of study design when applicable: Design - describe
given in brackets, e.g. [12]. References should include
the basic study design, e.g. randomized controlled trial,
the names of all authors when six or fewer; when seven
cross sectional study, cohort study, case series, survey etc;
or more, list only the rst three names and add et al.
Setting - specify whether the study was conducted in a
References should also include full title and source
primary or tertiary care setting, in an ambulatory care
information. Journal names should be abbreviated as in
clinic or hospital, in the general community etc;
Index Medicus
Participants - indicate the number of study subjects and
terms_cond.html). No more than 90-100 references
how they were selected, recruited, and assigned to the
will be accepted for reviews. For Letters to the Editor,
intervention; Intervention
- report the method of
5-6 references. Avoid or keep as low as possible the use
administration and duration of the intervention.
of abstracts as references. Personal communications and
Results
unpublished work should not feature in the reference
Provide the main outcomes of the study, including
list but should appear in parentheses in the text.
con dence intervals or p values.
Unpublished work accepted for publication but not yet
Conclusion
released should be included in the reference list with the
State only conclusions that are directly supported
words “in press” in parentheses beside the name of the
by the evidence and the implications of the ndings.
journal concerned.
58
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
GUIDANCE FOR DRAWING UP
a) Article:
in the metric system in terms of the International
[1] Otvos L Jr, Shao WH, Vanniasinghe AS, Amon
System of Units (SI).
MA, Holub MC, Kovalsykz I, et al. Toward understanding
Abbreviations and symbols
the role of leptin and leptin receptor antagonism in
Use only standard abbreviations. Avoid
preclinical models of rheumatoid arthritis. Peptides
abbreviations in the title and abstract.
e full term for
2011;32:1567-74.
which an abbreviation stands should precede its rst use
b) Papers published only with DOI numbers:
in the text unless it is a standard unit of measurement.
[2] Chaldakov GN, Beltowsky J, Ghenev PI, Fiore
M, Panayotov P, Rancic G, et al. Adipoparacrinology -
Reprints
vascular periadventitial adipose tissue (tunica adiposa) as
Ten reprints of the published articles and two copies
an example. Cell Biol Int
2011;doi:
10.1042/
of the Journal will be supplied free of charge. If required
CBI20110422.
in a greater number, they will be available on payment
c) Book:
of the necessary cost.
[3] Gertler A, editor. Leptin and Leptin Antagonists.
Landes Bioscience, Austin, Texas, USA. 2009.
Editorial policy
d) Book chapter:
We welcome all contributions in the eld of
[4] Jeremy L, Abe PD. Treatment Options in
medicine. We invite known personalities with expertise
Super cial (pTa/pT1/CIS) Bladder Cancer. In: Urological
and many published papers in a speci c eld to write
cancers in clinical practice, Springer-Verlag, London
reviews and editorials in our journal. We accept original
Limited, 2007:75-102.
papers and case reports from all countries.
e
Tables
Conexiuni Medicale/Medical Connections o ers
Each table should be assigned a Roman numeral
thorough peer review and immediate publication on
(e.g. Table III) and a brief title. Explanatory matter
acceptance.
e redactor-in-chief or one of the rst
should be placed in footnotes. Explain in footnotes all
reads the manuscripts received and in about 1-3 weeks
non-standard abbreviations that are used in each table.
decide upon their priority level: some are immediately
Identify statistical measures of variations, such as
sent to the reviewers, some are rejected without being
standard deviation and standard error of the mean. Each
sent for review and some are returned to authors with
table should be cited in the text.
suggestions for improvement before submitting them
Illustrations
to reviewers.
All graphs, photographs (on glossy paper), diagrams
will be referred to as gures and should be numbered
Peer-review procedure
consecutively in the text in Arabic numerals. If a gure
e Conexiuni Medicale/Medical Connections
has been published before, the original source must be
promotes evaluation of all the original papers by two or
acknowledged and written permission from the
three independent reviewers, of whom two are
copyright holder for both print and electronic formats
international personalities.
e peer-review process is
should be submitted with the material. Figures may be
essential for ensuring the quality of the scienti c
reduced, cropped or deleted at the discretion of the
information disseminated.
e reviewers are asked to
Editor.
evaluate the manuscript by applying the same standards
Legends for illustrations
as for the international journals.
e reviewers send
Captions should have an Arabic numeral
their comments to the Editor. e Editor will inform
corresponding to the illustration to which it refers with
the authors about the suggestions made by the referee
a title above and explanatory notes below it. Internal
and ask them to answer the questions and make the
scales should be explained and staining methods for
required corrections. is information is provided up to
photomicrographs should be identi ed.
three months from the date they submitted the paper to
Units of measurement
the journal. e revised manuscript should be sent in no
Measurements of length, height, weight, and
more than one month to the Editor. When the Editor
volume should be reported in metric units
(meter,
receives the corrected version with all changes marked,
kilogram, or litre) or their decimal multiples.
accompanied by a letter with a point-by-point reply to
Temperatures should be given in degrees Celsius. Blood
the reviewers’ comments, he sends those back to the
pressures should be given in mmHg. All hematological
same reviewer, who makes the nal recommendation for
and clinical chemistry measurements should be reported
acceptance or rejection of the manuscript.
59
GUIDANCE FOR DRAWING UP
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
Notice to subscribers
inside front or inside back cover: Euro 350 1 issue, 1400
e annual subscription rates for 2013: 80 RON
4 issues. Full colour page ouside back cover: Euro 400 1
individual, 160 RON institutional. Foreing subscribers:
issue, 1600 4 issues. Bank account: Colegiul Medicilor
75
$ individual, 150
$ institutional. Additional postage:
Satu Mare, CUI 9839430, Banca Transilvania, branch
surface mail 20
$, for overseas air mail 40
$. Bank
Agen ia Golescu Satu Mare, IBAN: RO38 BTRL 0310
account: Colegiul Medicilor Satu Mare, CUI 9839430,
1202 K392 62XX (RON) IBAN: RO62 BTRL 0310
Banca Transilvania, branch Agen ia Golescu Satu Mare,
2202 K392 62XX (USD) Swift: BTRLRO22.
IBAN: RO38 BTRL 0310 1202 K392 62XX (RON)
IBAN: RO62 BTRL 0310 2202 K392 62XX (USD)
© Copyright Conexiuni Medicale/Medical
Swift: BTRLRO22. Orders should be sent to the
Connections, Satu Mare, 2013
Editorial O ce, Eroilor Revolu iei Pl. no.23-440055
No part of this publication may be reproduced,
Satu Mare, Romania. Tel./Fax:
+40-261-710456 or
stored in a retrieval system or transmitted in any form or
+40-361-408164, or by e-mail: colmedsm@gmail.com.
by any means without prior permission in writing of
Conexiuni
Medicale/Medical
Connections.
Notice to advertisers
Permission is not however required to copy abstracts of
Applications for advertisement space and for rates
papers or of articles on condition that a full reference to
should be addressed to the Editorial O ce of Conexiuni
the source is shown. Correspondence regarding
Medicale/Medical Connections.
2013 advertising
permission to reprint all or part of any article
rates are Euro 200 full (A4) colour page, 1 issue, and
published in this journal should be addressed to the
Euro 800 full colour page, 4 issues. Full colour page on
Editor, e-mail: colmedsm@gmail.com
60
EDITORIAL
SFÂRŞITUL UNEI ILUZII
Este un paradox remarcabil faptul că în momentul
dorim să mâncăm mai pu in decât o facem în mod
de vârf (comparativ cu tot trecutul nostru) al realizărilor
obișnuit. Pentru prima dată în istorie săracii sunt în
umane materiale și tehnologice ale României, ne trezim
medie mai grași decât boga ii. Creșterea economică, care
copleși i de anxietate, înclina i spre depresie, îngrijora i
a fost până acum motorul progresului, și-a atins limitele
de cum apărem în ochii altora, nesiguri de prieteniile
în ările dezvoltate. Statisticile care măsoară bunăstarea
noastre, tenta i de consum și lipsi i de o via ă
și fericirea indică o plafonare a indicilor în ările
comunitară. În lipsa unor rela ii sociale calme și a
civilizate, în timp ce crește frecven a anxietă ii, depresiei
satisfac iei emo ionale de care cu to ii avem nevoie,
și a problemelor sociale. Printre ările sărace speran a de
căutăm alinarea în mâncatul excesiv, cumpăratul obsesiv,
via ă crește rapid în primele stadii de dezvoltare
sau cădem pradă alcoolului, psihotropelor sau drogurilor.
economică, iar printre ările cu venit mediu rata de
Cum se face că avem parte de atâta suferin ă emo ională
creștere a speran ei de via ă încetinește. Pe măsură ce
și mentală în ciuda nivelului de bunăstare și confort
nivelul de trai crește iar ările devin tot mai bogate,
nemaiîntâlnite în istoria noastră na ională? Ce ne
rela ia dintre creșterea economică și speran a de via ă
lipsește este ceva mai mult decât timpul petrecut în
devine tot mai slabă. Pentru ările bogate acumularea de
compania prietenilor și a familiei. Ne comportăm ca și
noi bogă ii nu mai adaugă nimic la speran a de via ă.
cum via a noastră ar
o bătălie continuă pentru
Motivul pentru aceasta nu este dat de faptul că am atins
supravie uirea psihologică, o luptă împotriva stresului și
limitele biologice ale speran ei de via ă. Chiar și cele mai
a epuizării emo ionale. Unii dintre noi doresc o societate
bogate ări bene ciază de progresul medicinei. Ceea ce
centrată pe valori, comunitate și familie, departe de
s-a schimbat este faptul că creșterea speran ei de via ă a
lăcomia și excesul ultimilor ani. Totuși majoritatea încă
încetat să mai e legată de nivelul material de trai. Cu
nu și-au realizat idealul material, tot mai iluzoriu, și
ecare decadă care trece, speran a de via ă în ările
continuă să se poarte egoist și iresponsabil într-o
bogate crește cu 2-3 ani, dar acest lucru nu mai depinde
societate tot mai fragmentată. Clasa politică nu pare a
de creșterea economică. De aceea cetă enii SUA nu au o
interesată de subiect și a renun at să încerce să ne ofere o
speran ă de via ă mai mare decât grecii, deși sunt de
viziune coerentă capabilă să ne inspire să creeăm o
două ori mai boga i decât ei. Cu cât ara este mai bogată
societate mai bună. Criza economică nu a făcut decât să
cu atât creșterea nivelului material de trai contribuie mai
ne abată aten ia de la societatea bolnavă, la economia
pu in la speran a de via ă și la starea de sănătate în
bolnavă. În loc să ne străduim să avem o societate mai
general.
bună, ecare se străduiește individual să-și întărească
Ce altceva mai este important pentru noi, în afară
pozi ia în societatea existentă. Dacă dorim să ne crescă
de speran a de via ă și starea de sănătate? Desigur
calitatea vie ii trebuie să ne mutăm aten ia și eforturile
căutarea și atingerea fericirii, pe care americanii o
de la standardele materiale la îmbunătă irea stării de
consideră atât de importantă încât au trecut-o și în
bine psihologic și social al întregii societă i. Cum
Constitu ie ca pe un drept fundamental. Economistul
pomenim însă de psihologie, discu ia tinde să se îndrepte
Richard Layard a demonstrat că asemenea speran ei de
spre solu ii individuale. Mașinăria politică este
via ă și sănătă ii, fericirea în ările foarte bogate încetează
împotmolită în noroi! Voi începe prin a spune că
să mai
e corelată cu acumularea de bogă ie
dovezile statistice ne arată că creșterea economică și-a
suplimentară. Fericirea crește în ările sărace propor ional
atins limitele în ceea ce privește furnizarea fericirii
cu creșterea economică, dar de la un anumit nivel al
umane, cel pu in în ările civilizate. Când lupii bântuiau
bogă iei în sus intră
„în platou”. Desigur de ni ia
pe uli ele satului, vremurile bune însemnau pur și
fericirii are multe particularită i culturale locale. În
simplu să ai burta plină și să i la adăpost. Pentru
unele societă i să nu spui că ești fericit înseamnă că
majoritatea dintre noi apa potabilă, casa încălzită și
admi i că ești un ratat; în altele să pretinzi că ești fericit
frigiderul plin sunt lucruri de la sine în elese. Mul i ne
este o dovadă de fudulie. Cu toate acestea studiile lui
61
EDITORIAL
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
Layard arată că la un venit anual de peste 25.000
$ per
de-a lungul istoriei creșterii economice, ările ating un
capita, corela ia dintre creșterea venitului și creșterea
prag al a uen ei de la care bene ciile aduse de creșterea
fericirii este foarte slabă. Studii de durată făcute în
bogă iei scad. Tendin ele privind mortalitatea con rmă
Japonia, SUA și Regatul Unit arată că pe o perioadă
același model. Când ările încep să se îmbogă ească,
su cient de lungă ca să se relizeze dublarea venitului,
primele care scad sunt bolile sărăciei: malnutri ia,
fericirea nu a crescut semni cativ. Același model este
tuberculoza, holera, rujeola. Acestea încetează să mai e
valabil și pentru al i indicatori ai bunăstării precum
principalele cauze de deces. Apar în schimb bolile
„măsura bunăstării economice” și „indicatorul autentic
a uen ei: bolile cardiovasculare, diabetul, cancerul,
al progresului” care calculează bene ciile nete ale
bolile degenerative. În timp ce bolile sărăciei omoară
dezvoltării după ce se scad costurile cu poluarea și
mai ales copiii, bolile a uen ei omoară mai ales adul ii.
ambuteiajele din tra c. În ările sărace creșterea
România nu a atins pragul celor 25.000$ pe an, dar în
economică continuă să e esen ială pentru sănătatea și
mod sigur va ajunge acolo. Discu ia ar putea să vi se
fericirea locuitorilor. Dar odată atins pragul bogă iei,
pară prematură acum, deși semnele suferin elor datorate
creșterea venitului contează din ce în ce mai pu in. Dacă
creșterii haotice le avem deja. Rostul ei este să speculeze
ești ămând, o pâine este esen ială pentru sănătatea și
unul din avantajele relativei înapoieri. Putem să ne
bunăstarea ta. Dar dacă ești sătul, o sută de pâini s-ar
elaborăm un model de dezvoltare socială care să evite
putea chiar să te deranjeze. Mai devreme sau mai târziu,
greșelile făcute de ceilal i. Dar vrem noi acest lucru?
Dr. Sever-Cristian Oană
62
ORIGINAL ARTICLES
CONCENTRAȚII SCĂZUTE ÎN SER ALE VITAMINEI D 25 OH LA
PACIENȚI CU DEBUT DE POLIARTRITĂ REUMATOIDĂ
Cojocaru Manole1, Rusu Elena2, Cojocaru Inimioara Mihaela3, Siloşi Isabela4
1Disciplina de Fiziologie, Facultatea de Medicină, Universitatea „Titu Maiorescu”, Bucureşti, Centrul Clinic de Boli
Reumatismale „Dr Ion Stoia”, Bucureşti, 2Disciplina de Biochimie, Facultatea de Medicină Dentară, Universitatea „Titu
Maiorescu”, Bucureşti,
3Departamentul de Neurologie
„Prof. Gheorghe Marinescu”, Spitalul Clinic Colentina,
Universitatea de Medicină şi Farmacie Carol Davila, Bucureşti, 4Disciplina de Imunologie, Universitatea de Medicină şi
Farmacie, Craiova, România
Adresa pentru coresponden ă:
Cojocaru Manole
Str omas Masaryk Nr 5, Sector 2, Codul Poştal 020983
Bucureşti, România
E-mail: mancojocaru@yahoo.com
Primit: 12.08.2013
Acceptat: 30.08.2013
Med Con October 2013, Vol 8, No 3, 63-65
Rezumat
folosit corela ia Spearman, iar diferen ele între grupuri
au fost calculate cu testul Fisher și testul t par pentru
Introducere: Studiile recente au sugerat rolul
variabile continue.
imunoregulator al vitaminei D. S-a sugerat o asociere
Rezultate: Concentra iile serice de 25(OH)D erau
între de cien a de vitamina D și apari ia poliartritei
scăzute la 46 dintre 74 pacien i cu PR (62%) vs. 80
reumatoide (PR). În prezent nu există studii privind
subiec i normali (p<0,01). Opt dintre cei 46 pacien i au
rolul vitaminei D în activitatea bolii.
prezentat concentra ia de 25(OH)D la limita inferioară.
Obiective: Să evaluăm nivelul
seric
de
Concentra iile serice de 25(OH)D în PR la debut au
25-hidroxivitamina D [25(OH)D] la pacien i cu PR și
indicat corela ie directă cu agravarea bolii
(r=0,61;
să investigăm efectele nivelurilor de vitamina D în ser
p<0,01). Nivelurile de 25(OH)D se corelează cu niveluri
asupra evolu iei clinice a pacien ilor cu PR la debut.
serice crescute de CRP (r=0,59; p<0,01). Concentra ia
Material și metode: Concentra iile serice de
serică medie de 25(OH)D la pacien i cu PR a fost
25(OH)D au fost determinate la 74 pacien i cu PR la
28,34±8,7 nmol/l (limitele între 18,52 și 41,36 nmol/l),
debut (M/F 25/49) cu vârsta medie 35,7±11,4 ani
comparativ cu 52,42±13,4 nmol/l (limitele între 36,17
(limite de la
21,9 ani la 58,4 ani); durata medie a
și 70,31) la subiec ii normali; (p<0,001)
poliartritei 5,1±4,3 luni (limite de la 2 luni la 10,2 luni)
Concluzie: To i pacien ii cu PR la debut au
comparativ cu 80 subiec i normali (M/F 27/53) cu
prezentat de cien ă marcată de 25(OH)D. Concentra ia
vârsta medie 34,2±10,7 ani (limite între 22,4 ani și 47,8
scăzută de
25(OH)D prezintă consecin e negative
ani). Nivelurile serice de 25(OH)D au fost determinate
asupra evolu iei clinice.
folosind
analiza
imunoenzimatică
(ELISA).
Cuvinte cheie: vitamina D, poliartrita reumatoidă,
Concentra iile de
25(OH)D au fost exprimate în
activitatea bolii
nmol/L. Rezultatele au fost analizate statistic folosind
testul t Student; valoarea p<0,05 (95% intervalele de
Vitamina D joacă rol un rol în men inerea
încredere) a fost considerat semni cativ statistic. S-a
homeostaziei imune [1,2]. S-au acumulat dovezi care
The Low Serum Concentrations of 25-Oh Vitamin D in Patients with Early Rheumatoid Arthritis
63
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
sprijină ideea că homeostazia alterată a vitaminei D
pacien i cu PR (62%) vs. subiec ii normali (p<0,01).
contribuie la mecanismele patogene în PR [3]. Poliartrita
Opt dintre 46 pacien i au prezentat 25(OH)D la limita
reumatoidă este o boală autoimună care prezintă
inferioară. Valorile serice de 25(OH)D la pacien i cu PR
poliartrită simetrică și cronică. Patogenia este numai
la debut au indicat o corela ie directă cu activitatea severă
par ial elucidată dar poate să includă factorii de
a bolii (r=0,61; p<0,01). Nivelurile de 25(OH)D s-au
susceptibilitate genetici precum antigenele clasei de
corelat cu nivelurile serice crescute de CRP
(r=0,59;
histocompatibilitate majoră, factorii de mediu
p<0,01). Concentra ia serică medie de
25(OH)D la
declanșează activarea sistemului imun înnăscut și
pacien i cu PR la debut a fost 28,34±8,7 nmol/L (limitele
adaptativ. De cien a de vitamina D ar putea să e
între 18,52 și 41,36 nmol/l), comparativ cu subiec ii
eventual unul dintre factorii declanșatori ai distrugerii
normali
52,42±13,4 nmol/L (limitele între
36,17 și
cartilajului în PR [4,5]. In uen a vitaminei D asupra
70,31 nmol/l); (p<0,001). Serum values of 25(OH)D,
bolilor autoimune nu este complet cunoscută.
titrurile anticorpilor anti-CCP3 IgG și nivelurile serice
crescute de CRP s-au corelat cu activitatea bolii (r=0,61,
Material şi metode
r=0,64, respectiv r=0,73). Nivelurile serice de 25(OH)D
la femei bolnave/femei sănătoase au indicat o corela ie
Concentra iile serice de
25-hidroxivitamină D
(r=0,31); la bărba i bolnavi/bărba i sănătoși (r=0,34); la
[25(OH)D] au fost determinate la 74 pacien i (vârsta
femei bolnave/bărba i bolnavi
(r=0,63); la femei
medie 35,7±11,4 ani, media duratei poliartritei 5,1±4,3
sănătoase/bărba i sănătoși (r=0,84).
luni) și 80 subiec i sănătoși (vârsta medie 34,2±10,7 ani).
Diagnosticul de PR se bazează în special de
Discu ii
manifestările clinice ale bolii și mai pu in pe datele
serologice reduse. Numărul articula iilor afectate este
Autorii au demonstrat că pacien ii cu PR prezintă
variabil la debutul bolii. Boala poate să debuteze cu
risc crescut de de cien ă de vitamina D. Nivelul extrem
afectarea uneia dintre articula ii sau a mai multor, de
de scăzut de 25(OH)D are consecin e negative asupra
asemenea poate să prezinte un debut palindromic.
evolu iei clinice. Nivelurile scăzute de vitamina D sunt
Datele care sunt în continuă creștere indică folosirea
legate de activitatea crescută în PR.
anticorpilor anti-CCP3 IgG ca marker serologic pentru
Se pare că vitamina D, de asemenea, este un reglator
eviden ierea PR la debut.
important al func iei imune. De cien a de vitamina D
Anticorpii în serul pacien ilor fa ă de peptidele
sau aportul redus a fost legat de creșterea susceptibilită ii
ciclice citrulinate au fost testa i folosind kit-ul ELISA
de apari ie a bolilor autoimune. Recent de cien a de
pentru anticorpi anti-CCP3 IgG.
vitamina D a fost implicată ca un poten ial factor de
Concentra ia serică de 25(OH)D a fost determinată
mediu pentru declanșarea de numeroase tulburări
folosind ELISA. Concentra iile de
25(OH)D erau
autoimune, cum ar PR [6-9]. În ultimii ani, s-a
exprimate în nmol/l. Rezultatele au fost analizate
demonstrat rolul posibil al vitaminei D în patogenia
statistic folosind testul t Student și valoarea p<0,05
PR. Nivelurile serice de 25(OH)D s-au corelat invers cu
(95% intervalele de încredere) a fost
semni cativ statistică. Analizele de
corela ie au fost efectuate folosind
corela ia Spearman, și diferen ele între
grupuri au fost calculate cu testul
Fisher și și testul t par pentru variabile
continue.
Rezultate
To i pacien ii cu RA prezentau
anticorpi
anti-CC3
IgG.
Concentra iile serice medii de 25(OH)
D la grupul de pacien i au fost
demni cativ mai scăzute decât cele de
la lotul martor. Concentra ia în ser de
Figura 1. Valoarea medie a concentra iilor serice de vitamina D
25(OH)D a fost scăzută la 46 din 74
la pacien i cu poliartrită reumatoidă la debut comparativ cu lotul martor
64
Cojocaru et al
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
ORIGINAL ARTICLES
severitatea PR [10-12]. Aportul crescut de vitamina D
management of rheumatoid arthritis. Rheumatology
ar putea asociat cu risc scăzut de PR, totuși, această
2008;47:1617-21.
observa ie este o ipoteză. Rolul ziopatologic al
6.
Costenbader KH, Feskanich D, Holmes M Karlson
vitaminei D în in ama ia articulară, rămâne totuși,
EW, Benito-Garcia E. Vitamin D intake and risk of
neclar.
systemic lupus erythematosus and rheumatoid arthritis
in women. Ann Rheum Dis 2008;67:530-5.
7.
Marques C, Dantas A, Fragoso T, et al. e importance
Referin e
of vitamin D levels in autoimmune diseases. Bras J
Rheumatol 2010;50:73-80.
1. Wen H, Baker JF. Vitamin D, immunoregulation, and
8.
Patel S, Farragragher T, Berry J, et al. Association
rheumatoid arthritis. Journal of Clinical Rheumatology
between serum vitamin D metabolite levels and disease
2011;17:102-7.
activity in patients with early in ammatory polyarthritis.
2. Kiran G, Debashish D. Vitamin D and rheumatoid
Arthritis Rheum 2007;56:2143-9.
arthritis: is there a link? Int J Rheum Dis 2008;11:206-
9.
Cutolo M, Otsa K, Ypras M, et al. Vitamin D and
11.
rheumatoid arthritis: comment on the letter by Nielen et
3. Cantorna MT. Vitamin D and autoimmunity: is
al [letter]. Arthritis Rheum 2007;56:1719-20.
vitamin D status an environmental factor a ecting
10.
Haque UJ, Barlett SJ. Relationship among vitamin D,
autoimmune disease prevalence? Proc Soc Exp Biol
disease activity, pain and disability in rheumatoid
Med 2000;223:230-3.
arthritis. Clin Exp Rheumatol 2010;28:745-7.
4. Craig SM, Yu F, Curtis JR, et al. Vitamin D status and
11.
Szodoray P, Nakken B, Gaal J, et al. e complex role
its associations with disease activity and severity in
of vitamin D in autoimmune diseases. ScandJ Immunol
African Americans with recent-onset rheumatoid
2008;68:261-9.
arthritis. J Rheumatol 2010;37:275-81.
12.
Holick MF. Vitamin D de ciency. N Engl J Med
5. Leventis P, Payel S. Clinical aspects of vitamin D in the
2007;357:266-81.
The Low Serum Concentrations of 25-Oh Vitamin D in Patients with Early Rheumatoid Arthritis
65
Medical Connections/Conexiuni Medicale
Declara ia de con ict de interese
Medical Connections/Conexiuni Medicale (Med Con) solicită tuturor autorilor şi recenzorilor să declare
orice con ict de interese care ar putea interveni în contribu iile lor.
Con ictul de interese pentru un anumit manuscris există atunci când un participant în procesul de
recenzie inter pares (peer review) şi de publicare -autor, referent, sau editor- are legături cu activită i care
l-ar putea in uen a necorespunzător pe el sau judecata lui, indiferent dacă aceasta este sau nu afectată.
Rela iile nanciare cu industria medicală, de exemplu prin muncă salarială, consultan ă, de inere de
ac iuni, onorarii, testimoniale ca şi expert, e direct, e prin intermediul familiei, sunt de obicei considerate
a cele mai importante con icte de interese. Cu toate acestea, pot apărea con icte din alte motive, cum ar
rela iile personale, concuren a academică şi implicarea intelectuală.
Încrederea publicului în procesul de revizuire inter pares şi credibilitatea articolelor publicate depinde
în parte de cât de bine este administrat posibilul con ict de interese în timpul redactării, recenziei inter
pares şi a luării deciziilor editoriale. Părtinirea poate de multe ori identi cată şi eliminată prin aten ia
crescută asupra metodelor ştiin i ce şi concluziilor lucrării. Rela iile nanciare şi efectele lor sunt mai uşor
de identi cat decât alte con icte de interese. Participan ii la peer review şi în procesul de publicare trebuie
să-şi dezvăluie posibilele con ictele de interese, iar informa iile trebuie să e puse la dispozi ie, astfel încât
şi al ii să poată aprecia aceste efecte pentru ei înşişi.
Autori: atunci când trimit un manuscris sau o scrisoare, autorii sunt responsabili pentru recunoaşterea
şi divulgarea con ictelor nanciare şi altor con icte de interese care ar putea să le in uen eze activitatea. Ei
trebuie să recunoască în manuscris orice sprijin nanciar pentru activitate, precum şi orice alte legături
nanciare sau personale în munca lor.
Recenzorii: evaluatorii externi inter pares trebuie să dezvăluie editorilor orice con icte de interese care
le-ar putea părtini opiniile asupra manuscrisului şi ar trebui să se recuze de la recenzia anumitor manuscrise
în cazul în care cred că este oportun. Editorii trebuie să e conştien i de posibilele con icte de interese ale
recenzorilor în interpretarea recenziilor şi trebuie să judece pentru ei dacă recenzorul ar trebui să e recuzat.
Recenzorii nu trebuie să utilizeze informa iile în munca lor, înainte de publicare, pentru a-şi promova
propriile interese.
Titlul manuscrisului: ________________________________________________________
Declar că nu există con ict de interese
Declar că există următoarele con icte de interese poten iale:
_________________________________________________________________________
_________________________________________________________________________
_________________________________________________________________________
_________________________________________________________________________
_________________________________
_________________________________
Nume
Semnătura/Data
Vă rugăm trimite i acest formular semnat pe fax sau mail la sediul editorului Med Con.
Fax: +40-261-710456
Email: colmedsm@gmail.com
ORIGINAL ARTICLES
DISCUȚIA DESPRE SEX DINTRE PĂRINȚI ŞI COPIII LOR ÎN
COMUNITATEA ARABĂ DIN ISRAEL
Joubran Samia1, Marcus Ohad2, Rath-Wolfson Lea6,8,Tova Hartman4, Iancu Iulian3,8, Weizman Abraham5,8,
Ram Edward7,8
1Facultatea de Medicină Bruce Rappaport, Institutul Tehnologic Technion şi Centrul Medical Emek, 2Departamentul de
Psihologie, Colegiul Yezreel Valley, 3,8Clinica de Sănătate Mentală Yavne, 4Departamentul de Educa ie şi al Genurilor,
Universitatea Bar-Ilan, Israel, 5,8Centrul de Sănătate Mentală Geha, Petah Tikva, Israel, 6,8Departamentul de Patologie,
Spitalul Hasharon, Centrul Medical Rabin, 7,8Departamentul de Chirurgie Generală, Spitalul Hasharon, Centrul
Medical Rabin, 8Facultatea de Medicină Sackler, Universitatea Tel Aviv
Adresa pentru coresponden ă:
Edward Ram
Division of General Surgery, Rabin Medical Center-Campus Golda
Petach Tiqva, 7 Keren Kaiemet St.
Tel: 972-3-9372323, Fax: 972-3-9372401
E-mail: edwardrm@netvision.net.il
Primit: 10.01.2013
Acceptat: 30.06.2013
Med Con October 2013, Vol 8, No 3, 67-74
Rezumat
studii academice, vorbesc cu copiii lor despre valorile
religioase ale actului sexual, în timp ce creștinii, în
Aproape jumătate din popula ia globului are mai
special cei cu studii academice, vorbesc cu copiii lor
pu in de douăzeci și cinci de ani. Rezultatele negative ale
despre contracep ie. De asemenea, am constatat că to i
sarcinii, infec iile cu transmitere sexuală, violen a și
părin ii, în special musulmanii religioși, vor să știe cu
consumul de alcool amenin ă sănătatea oamenilor în a
cine se întâlnesc copiii lor, unde se întâlnesc și cât de
doua decadă de via ă mai mult decât la orice altă grupă
intime sunt aceste întâlniri. În sfârșit, am constatat că
de vârstă. Adolescen a este o perioadă cu libertate
to i părin ii, în special cei non-religioși (atât musulmani
crescută în a face alegeri, iar capacitatea adolescen ilor
cât și creștini), cred că au primit o educa ie sexuală e
de a se confrunta cu aceste alegeri și să ia decizii sănătoase
de citară, e foarte de citară de la părin ii lor.
este crucială pentru dezvoltarea lor. Părin ii pot avea o
Cuvinte cheie: discurs, părin i, adolescen i,
in uen ă importantă asupra comportamentului copiilor
educa ie sexuală, sectorul arab israelian, musulmani,
lor, rela iile părinte-copil precum și monitorizarea și
creștini
supravegherea parentală ind asociate cu debutul mai
târziu al activită ii sexuale în rândul copiilor. E cacitatea
Introducere
unei astfel de discu ii ar putea depinde de o serie de
factori, incluzând sexul părintelui și al copilului, nivelul
Când tinerii simt că pierd legătura cu familia, casa,
rela iei dintre ei, atitudinea părin ilor fa ă de activitatea
școala, se pot implica în activită i care le pun sănătatea
sexuală a adolescen ilor și de abilitatea părintelui de a
în pericol. Lipsa discu iei dintre copii și părin ii lor
discuta despre sexualitate deschis și fără jenă. Am
afectează comportamentele și atitudinile copiilor. Cei
constatat că musulmanii, în special cei religioși și fără
care au relatat sentimentul de lipsă de căldură, dragoste,
Discourse Between Parents and Their Children about Sex in the Arab Community in Israel
67
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
sau de îngrijiri parentale, sunt cei care au cele mai multe
Cei preocupa i de sexualitatea adolescen ilor și
șanse de a prezenta dezechilibru emo ional, scăderea
sănătatea reproducerii s-au străduit să stimuleze discu ia
stimei de sine, probleme școlare, consum de droguri și
părinte-copil despre sex, din mai multe motive. În
comportamente sexuale riscante [1].
primul rând, ampli carea unei astfel de discu ii este
Părin ii pot avea o in uen ă importantă asupra
importantă în sine. În al doilea rând, în unele
comportamentelor copiilor lor. Studiile au indicat că
comunită i, este mult mai larg acceptat și mai pu in
rela iile de sus inere părinte-copil și monitorizarea și
controversat pentru părin i să-și exprime valorile și
supravegherea parentală sunt asociate cu activitatea
credin ele lor despre sex fa ă de copii lor, decât pentru
sexuală întârziată în rândul copiilor
[2]. Dinamica
profesori sau al i educatori să vorbească despre sex în
rela iilor părinte-copil și a comunicării sunt foarte mult
sala de clasă. În al treilea rând, ampli carea discu iei
in uen ate de cultura și mediul social în care ei trăiesc.
părinte-copil despre valorile sexului și utilizarea de
Comunicarea parinte-copil pe problemele sexuale
contraceptive este asociată, în anumite condi ii, cu o
rămâne o problemă di cilă. Cei mai mul i adolescen i
întârziere a debutului sexual, sau cu o mai mare utilizare
nu par a se sim i confortabil când vorbesc despre
a contracep iei [10]. Discursul poate ajuta la reducerea
sexualitate cu părin¬ ii lor [3].
asumării riscului sexual de către adolescen i, cum ar
E cacitatea unei astfel de discu ii poate depinde de
sarcinile nedorite și a bolilor cu transmitere sexuală.
o serie de factori, incluzând sexul părintelui și al
Într-adevăr, programele educa ionale e ciente cu privire
copilului, nivelul rela iei dintre ei, atitudinea părin ilor
la sex și a bolilor cu transmitere sexuală sau HIV, de
fa ă de sex la adolescen i și de capacitatea părintelui de a
multe ori ampli că discu ia părinte-copil despre sex [4].
discuta despre sexualitate deschis și confortabil
[4].
Israelul este o resursă valoroasă pentru furnizarea
Majoritatea adul ilor tineri doresc să știe despre
unei abordări multi-religioase pentru diverse probleme.
abstinen ă, contraceptive și modul de prevenire a HIV și
El prezintă o varietate de religii, grupuri etnice, culturi
a altor infec ii cu transmitere sexuală (ITS). Cu toate
și tradi ii. Statul Israel are aproape
7,4 milioane de
acestea, părin ii au de multe ori di cultă i în a discuta
locuitori. Caracteristica cea mai importantă a popula iei
despre sex. Studiile au arătat ca adolescen ii care au
Israelului este marea sa diversitate. Pe lângă principala
raportat că simt o conexiune cu părin ii și cu familia lor
împăr ire a locuitorilor ării în evrei
(80%) și arabi
au mai multe șanse decât al ii de a amâna ini ierea
(20%), există mult mai multe subdiviziuni. Evreii, de
actului sexual. Adolescen ii care au spus că familiile lor
exemplu, sunt împăr i i în religioși și laici, în timp ce
sunt calde și grijulii au raportat, de asemenea, o utilizare
aceștia din urmă includ diferite comunită i de imigran i
a marijuanei mai redusă și un stres emo ional mai redus
care își păstrează cultura. Arabii sunt împăr i i în
decât colegii lor
[5]. Într-un studiu care a explorat
musulmani, creștini și druzi. Cea mai mare minoritate
sursele primei discu ii despre sex cu copii [6], Moore și
de non-evrei în Israel este cea arabă, care reprezintă
Davidson au arătat că în rândul femeilor studente
aproximativ o cincime din popula ia ării. Marea
necăsătorite, cele care au vorbit primele despre sex cu
majoritate a arabilor din Israel sunt musulmani suni i,
mama lor au fost mai mult dispuse de a utiliza
doar aproximativ o zecime ind creștini. Diferen ele
contraceptive la primul contact sexual decât cele care au
culturale dintre evrei și arabi în Israel dirijează valorile
învă at despre sex de la colege sau profesori.
de bază ale ecărui sector, datorită apartenen ei culturale
Adolescen a este o perioadă de libertate crescută în a
derivate din patru origini: etnie, limbă, religie și
face alegeri, iar capacitatea adolescentului de a se
na ionalitate [11].
confrunta cu aceste alegeri și să ia decizii sănătoase este
În creștinism, Biserica este educatorul normelor
crucială pentru dezvoltare [7]. O’Sullivan și colab. [8]
morale și etice, ea a primit misiunea specială de pază și
au sugerat că pentru unele fete dezvoltarea sexuală
protec ie a înaltei demnită i a căsătoriei și cea mai
cauzează un con ict, care afectează discu ia cu mamele
importantă responsabilitate a transmiterii vie ii umane.
lor și necesită ob inerea educa iei sexuale din alte surse.
Educa ia sexuală este un drept de bază și o datorie a
Genera ia adolescen ilor de astăzi este cea mai mare
părin ilor și trebuie să e întotdeauna efectuată sub
din istorie. Aproape jumătate din popula ia globului are
îndrumarea lor atentă, e la domiciliu, e în centre
mai pu in de douăzeci și cinci de ani. Rezultatele
educa ionale alese și controlate de ei. Misiunea de a
negative ale sarcinii, infec iilor cu transmitere sexuală,
educa cere ca părin ii creștini să prezinte copiilor lor
violen a și concep ia sub in uen a alcoolului, amenin ă
toate subiectele care sunt necesare pentru maturizarea
starea de sănătate a oamenilor în a doua decadă de via ă
treptată a personalită ii lor, din punct de vedere creștin
mai mult decât la orice altă grupă de vârstă [9].
și ecleziastic [12]. În Islam, sexualitatea este considerată
parte a identită ii ca in e umane: Islamul este explicit
68
Joubran et al
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
ORIGINAL ARTICLES
cu privire la mai multe aspecte ale sexualită ii umane.
(1) Care sunt subiectele sexuale abordate de părin i
De asemenea, pe baza Hadith-ului care arată dorin a
cu copiii lor?
Profetului de a discuta aceste probleme în mod deschis,
(2) Ce cantitate de detalii doresc părin ii să știe
ar trebui să e evident că educa ia cu privire la aspecte
despre persoana cu care se întâlnesc copiii lor? Doresc să
legate de sex este acceptabilă
[13]. Predarea despre
știe unde se întâlnesc? Doresc să știe cât de intime sunt
sexualitate nu este în sine o încălcare a moralei, într-
aceste întâlniri?
adevăr, părin ii sunt îndemna i să nu simtă timiditate
(3) Sunt părin ii mai liberali acum, decât au fost
sau jenă cu privire la furnizarea de informa ii necesare
părin ii lor?
despre sex copiilor lor [13]. Explicarea anatomiei și a
Procedură
modi cărilor corpului experimentate în cursul pubertă ii
Chestionarele au fost furnizate administratorilor
sunt esen iale pentru a permite tinerilor să crească cu o
școlilor din întreaga ară, care le-au trimis părin ilor
imagine de sine sănătoasă. Într-o epocă în care activitatea
selecta i aleatoriu de la școlile lor. Chestionarele
sexuală în multe ări debutează la o vârstă fragedă,
completate anonim au fost trimise înapoi la anchetatori
adolescen ii musulmani trebuie să e informa i, pentru
prin e-mail. Din 1.000 de chestionare, au fost returnate
a permite o mai bună adaptare pentru a face fa ă
797, cu o rată de răspuns de 79,7%, care este mare
presiunii de grup. Educa ia sexuală poate predată într-
pentru comunitatea arabă.
un mod care să informeze tinerii despre sexualitate în
termeni știin i ci și morali [13].
Rezultate
Acest studiu își propune să răspundă la următoarele
întrebări:
Am vrut să examinăm diferen ele dintre musulmani
1. Există o corela ie între religia părin ilor
și creștini în ceea ce privește rela ia dintre părin i și
(musulmană sau creștină) și discu ia cu copiii lor?
copiii lor.
Diferen ele dintre părin ii laici și cei religioși, precum și
Primul lucru pe care am vrut să-l știm este ce
între mediul academic și non-academic ampli că această
subiecte privind sexul abordează părin ii în discu ii cu
corela ie?
copiii. Am constatat că 56,7% dintre părin i au vorbit
2. Există o corela ie între religia părin ilor
cu copiii lor despre valorile religioase ale actului sexual,
(musulmană sau creștină) și cât de liberală este abordarea
49,4% au vorbit despre pubertate, 49,3% au vorbit
lor privind educa ia sexuală? Diferen ele dintre părin ii
despre actul sexual și sarcină, 48,2% au vorbit despre
seculari și cei religioși, precum și între mediul academic
bolile sexuale, 42,3% au vorbit despre amânarea actului
și non-academic ampli că această corela ie?
sexual până la căsătorie și doar 28,7% dintre părin i au
vorbit cu copiii lor despre contracep ie.
Metodologia de cercetare
Am găsit o corela ie medie și semni cativă (Φ=0,20)
între religia părintelui și subiectul privind valorile
Participan ii
religioase ale actului sexual
[χ(1)=28,44, p<0,001],
Participan ii au fost 797 de părin i israeliano-arabi
astfel încât părin ii musulmani au vorbit cu copiii lor cu
din tot Israelul, a căror interval de vârstă a fost între 20
privire la valorile religioase ale actului sexual (65,8%)
și 66 de ani (M=39). Printre ei au fost 371 de creștini și
mai mult decât au făcut-o părin ii creștini (34,8%). În
426 musulmani, 208 bărba i și 589 femei; 533 locuiesc
plus, printre părin ii musulmani, am găsit o corela ie
în orașe și 264 în mediul rural sau sate; 483 cu studii
medie și semni cativă
(Φ=0,11) între gradul de
academice și
314 non-academice. În plus,
545 de
religiozitate și subiectul privind valorile religioase ale
participan i s-au de nit ca seculari sau tradi ionaliști, iar
actului sexual [χ(1)=4,52, p<0,05], astfel încât părin ii
252 s-au de nit ca ind religioși sau foarte religioși.
musulmani religioși au discutat cu copiii lor despre
Chestionare
valorile religioase ale actului sexual (71,7%) mai mult
Studiul s-a bazat pe chestionare elaborate de
decât au făcut-o părin ii musulmani non-religioși
Blendon [15], care au constat din patruzeci și două de
(61,3%). Am constatat, de asemenea, o corela ie slabă și
întrebări cu răspunsuri multiple, care examinează
semni cativă
(Φ=0,15), între gradul de studii și
atitudinea unui părinte fa ă de educa ia sexuală.
subiectul privind valorile religioase ale actului sexual
Chestionarul a fost tradus în limba arabă (traducere în
[χ(1)=8,18, p<0,005], astfel încât părin ii musulmani
ambele sensuri) și a fost certi cat de un specialist de
fără studii academice au vorbit cu copiii lor despre
limbă arabă. Din acest chestionar au fost utilizate trei
valorile religioase ale actului sexual (74,3%) mai mult
întrebări.
decât au făcut părin ii musulmani cu studii academice
Întrebările care au ghidat această cercetare sunt:
(60,2%).
Discourse Between Parents and Their Children about Sex in the Arab Community in Israel
69
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
cantitatea de detalii pe care doresc să o
cunoască despre cine se întâlnește cu
copiii lor [U(768)=67144,5, p<0,05],
astfel
încât părin ii musulmani
(M=400,30) au dorit să știe mai în
detaliu despre cine se întâlnește cu
copiii lor decât părin ii creștini
(M=366,96). În plus, printre
musulmani, am găsit o diferen ă
semni cativă între părin ii religioși și
non-religioși cu privire la cantitatea
Figura 1. Procentul părin ilor care au vorbit cu copiii lor despre
de detalii pe care doresc să o cunoască
diferite subiecte despre sex
despre persoana pe care copiii lor o
întâlnesc [U(404)=16,903, p<0,005],
Am găsit o corela ie slabă și semni cativă (Φ=0,09)
astfel încât părin ii musulmani religioși (M=220,15) au
între religia părin ilor și subiectul contracep iei
vrut să știe în detaliu despre persoana pe care copiii lor o
[χ(1)=4,90, p<0,05], astfel încât părin ii musulmani au
întâlnesc, mai mult decât părin ii musulmani non-
vorbit cu copiii lor despre contracep ie (25,3%) mai
religioși (M=189,55).
pu in decât cei creștini
(32,8%). În plus, în rândul
În plus, am constatat o diferen ă semni cativă între
părin ilor creștini, am găsit o corela ie slabă și
părin ii musulmani și creștini cu privire la cantitatea de
semni cativă
(Φ=0,17) între gradul religiozitate și
detalii pe care doresc să o știe despre locul de întâlnire al
subiectul contracep iei
[χ(1)=8,99, p<0,005], astfel
copiilor lor
[U(752)=64061,5, p<0,05], astfel încât
încât părin ii creștini religioși au vorbit cu copiii lor
părin ii musulmani (M=392,99) au vrut să cunoască
despre contracep ie (17,6%) mai pu in decât au făcut-o
mai în detaliu locul de întâlnire al copiilor lor decât
părin ii creștini non-religioși (36,9%).
părin ii creștini
(M=358,44). Printre musulmani, am
Nu a existat nicio corela ie semni cativă între religie
găsit o diferen ă semni cativă între părin ii religioși și
și oricare dintre celelalte subiecte și nicio corela ie
non-religioși cu privire la cantitatea de detalii pe care
semni cativă între gradul de religiozitate și nivelul
doresc să o cunoască despre locul de întâlnire al copiilor
academic pentru oricare dintre celelalte subiecte, în
lor
[U(393)=15597,5, p<0,001], astfel încât părin ii
rândul musulmanilor sau creștinilor. Figura 1 reprezintă
musulmani religioși (M=216,47) au vrut să știe mai
rezultatele de mai sus.
multe detalii despre locul de întâlnire al copiilor lor
Al doilea lucru pe care am vrut să-l știm este procentul
decât au vrut părin ii musulmani non-religioși
părin ilor care vor să cunoască în detaliu cu cine se
(M=182,91). De asemenea, printre musulmani, am
întâlnesc copiii lor, unde se întâlnesc și cât de intime sunt
găsit o diferen ă semni cativă între părin ii cu studii
aceste întâlniri. Am constatat că 64,8% dintre părin i
academice și non-academice cu privire la cantitatea de
doresc să cunoască în detaliu cu cine se întâlnesc copiii
detalii pe care doresc să o știe despre locul de întâlnire al
lor, 26,3% doresc doar să știe cu cine se întâlnesc copiii
copiilor lor
[U(393)=16,132, p<0,05], astfel încât
lor, 8,2% doresc să știe doar o parte despre cei care se
părin ii musulmani cu studii academice (M=187,28) au
întâlnesc cu copiii lor, iar 0,7% nu doresc să știe cu cine
vrut să știe mai pu ine detalii despre locul de întâlnire al
se întâlnesc copiii lor. În plus,
64,8% dintre părin i
copiilor lor, decât au vrut părin ii musulmani fără studii
doresc să cunoască în detaliu unde se întâlnesc copiii lor,
academice (M=211,92).
24,9% doresc doar să știe unde se întâlnesc copiii lor,
În sfârșit, am găsit o diferen ă semni cativă între
9,3% doresc să știe doar o parte despre unde se întâlnesc
părin ii musulmani și creștini cu privire la cantitatea de
copiii lor, iar 1,1% nu doresc să știe unde se întâlnesc
detalii pe care doresc să o știe despre cât de intime sunt
copiii lor. În sfârșit,
62,6% dintre părin i doresc să
întâlnirile copiilor lor [U(754)=69,221, p<0,005], astfel
cunoască în detaliu cât de intime sunt întâlnirile copiilor
încât părin ii musulmani (M=397,43) au vrut să știe în
lor, 25,2% doresc doar să știe cât de intime sunt întâlnirile
detaliu despre cât de intime sunt întâlnirile copiilor lor,
copiilor lor, 9,8% doresc să știe doar par ial cât de intime
fa ă de cât au vrut părin ii creștini (M=355,45). În plus,
sunt întâlnirile copiilor lor, iar 2,4% nu doresc să știe cât
printre musulmani, am găsit o diferen ă semni cativă
de intime sunt întâlnirile copiilor lor.
între părin ii religioși și non-religioși cu privire la
Am găsit, de asemenea, o diferen ă semni cativă
cantitatea de detalii pe care doresc să o știe despre cât de
între părin ii musulmani și creștini cu privire la
intime sunt întâlnirile copiilor lor
[U(396)=16,258,
70
Joubran et al
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
ORIGINAL ARTICLES
p<0,005], astfel că părin ii musulmani
religioși (M=215,73) au vrut să știe în
detaliu despre cât de intime sunt
întâlnirile copiilor lor, fa ă de cât au
vrut părin ii musulmani non-religioși
(M=185,81). Figura
2 reprezintă
rezultatele de mai sus.
A treia întrebare pusă părin ilor a
fost dacă ei sunt mai liberali decât au
fost părin ii lor. Am constatat că
39,5% dintre părin i cred că sunt mai
Figura 2. Cantitatea de detalii (în procente) pe care părin ii doresc să o ştie
liberali decât au fost părin ii lor, 52%
despre cine se întâlneşte cu copiii lor, unde se întâlnesc şi cât de intime sunt
cred că ei sunt par ial mai liberali
aceste întâlniri
decât au fost părin ii lor, iar
8,5%
cred că ei și părin ii lor sunt la fel de
liberali. Am găsit, de asemenea, o
diferen ă semni cativă între părin ii
musulmani și creștini despre părerea
lor dacă ei sunt mai liberali decât au
fost părin ii lor
[U(709)=57,387,
p<0,05],
astfel
încât
părin ii
musulmani (M=340,44) au crezut că
sunt mai pu in liberali decât au fost
părin ii lor, fa ă de cât au crezut
părin ii creștini (M=370,71). Figura 3
Figura 3. Procentul părin ilor care cred că sunt mai mult, par ial mai mult,
reprezintă rezultatele de mai sus.
sau la fel de liberali decât au fost părin ii lor, în general şi în func ie de religie
Ultimul lucru pe care l-am
întrebat a fost ce fel de educa ie
sexuală au primit de la părin ii lor.
Am constatat ca 45,6% dintre părin i
cred că au primit o educa ie sexuală
foarte de citară de la părin ii lor,
30,2% cred că au primit o educa ie
sexuală de citară de la părin ii lor,
16,7% cred că au primit o educa ie
sexuală bună de la părin ii lor și doar
7,6% cred că au primit o educa ie
Figura 4. Procentul părin ilor care cred că au primit o educa ie sexuală de la
sexuală foarte bună de la părin ii lor.
părin ii lor foarte bună, bună, slabă sau foarte slabă, în general şi în func ie
În plus, cu toate că nu am găsit
de religie şi de gradul de religiozitate
diferen e semni cative între religii cu
privire la ce fel de educa ie sexuală au
primit de la părin ii lor [U(713)=61434,5, ns], am găsit
fa ă de ce cred părin ii creștini non-religioși (M=163,67).
o diferen ă semni cativă între gradul de religiozitate cu
Figura 4 reprezintă rezultatele de mai sus.
privire la ce fel de educa ie sexuală au primit de la
părin ii lor, atât pentru părin ii musulmani
Discu ie
[U(375)=15085,5, p<0,05], cât și pentru părin ii
creștini
[U(338)=7712, p<0,05], astfel încât părin ii
Educa ia este un proces inten ional structurat
religioși musulmani (M=201,30) cred că au primit o
pentru a împărtăși cunoștin e și abilită i și pentru a
educa ie sexuală mai bună de la părin ii lor, fa ă de ce
in uen a procesul de dezvoltare al unui individ [14].
cred părin ii musulmani non-religioși (M=177.99), iar
Educa ia sexuală permite oamenilor să dobândească
părin ii creștini religioși (M=192,23) cred că au primit o
cunoștin e și să dezvolte abilită i pe care le pot folosi
formă mai bună de educa ie sexuală de la părin ii lor,
pentru a se proteja pe ei înșiși și pe al ii [7].
Discourse Between Parents and Their Children about Sex in the Arab Community in Israel
71
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
Studiul nostru a avut două scopuri. Primul a fost de
majoritatea părin ilor au vrut să știe totul despre copiii
a găsi o corela ie între religia părin ilor (musulmană sau
lor și rela ia cu partenerul lor, 65% din ambele religii,
creștină) și discu ia cu copiii lor, precum și pentru a a a
musulmană și creștină, au vrut să știe cu cine și unde
dacă diferen ele dintre mediul academic și cel non
adolescentul se întâlnește și cât de intime sunt întâlnirile
academic și dintre părin ii laici și cei religioși ampli că
lui. Musulmanii au vrut să știe despre copiii lor, mai
această corela ie. Al doilea a fost de a găsi o corela ie
mult decât creștinii.
între religia părin ilor
(musulmană sau creștină) și
Gândirea religioasă are o in uen ă enormă asupra
abordarea lor liberală fa ă de educa ia sexuală, precum și
punctelor de vedere și opiniilor credincioșilor cu privire
pentru a a a dacă diferen ele dintre mediul academic și
la sexualitate. Sexualitatea în Islam nu se limitează la
cel non academic și dintre părin ii laici și cei religioși
procreere, de altfel ca și în majoritatea celorlalte religii
ampli că această corela ie.
monoteiste. Islamul face diferen a între sexualitate
În studiul de fa ă doar jumătate din părin i au
„legitimă” și
„nelegitimă”, pe baza stării civile
[18].
raportat că stau de vorbă cu copiii lor despre probleme
Sexualitatea în cadrul căsătoriei este permisă și acceptată
legate de sex, iar mai mult de jumătate dintre ei vorbesc
de societate. Sexualitatea în afara căsătoriei este interzisă
despre valorile religioase și etice ale educa iei sexuale.
și inacceptabilă social [19]. Ca o consecin ă, sexualitatea
Creștinii discută despre contracep ie cu copiii lor mai
nu este numai obiectul unor norme religioase, dar are,
mult decât musulmanii. Creștinii seculari discută despre
de asemenea, efecte asupra statutului social, economic și
controlul nașterii mai mult decât majoritatea părin ilor
public al oamenilor [18].
creștini religioși. Musulmanii laici și religioși au solicitat
Sectorul arab israelian este compus în mare parte
valori educa ionale și morale ale educa iei sexuale,
din creștini și musulmani, ambele religii având o cultură
printre ei, musulmanii cu studii academice au cerut
mediteraneană. Mernissi [20] a descris această cultură ca
aceste învă ături mai mult decât părin ii musulmani fără
una în care subordonarea oamenilor for elor naturale
studii academice. Ini ierea discu iei despre problemele
capricioase și imprevizibile este egalată doar de
sexuale poate di cilă pentru părin ii din comunită ile
subordonarea femeilor bărba ilor. Conform acestei
similare celei arabe din Israel, deoarece aceștia pot
abordări, fetele trebuie să e virgine până la căsătorie. O
nesiguri cu privire la modul de abordare a acestor
fată care nu este fecioară ar aduce rușine pentru familia
probleme. În 1979, Fox a raportat că mai pu in de
sa, iar so ul ei o va trimite înapoi părin ilor. În unele ări
jumătate din adolescen i au vorbit de fapt cu părin ii lor
musulmane fundamentaliste, chiar poate executată.
despre probleme sexuale de bază, cum ar rolul tatălui
Mernissi explică această situa ie cu acurate e:
în reproducere și o pătrime nu au vorbit niciodată cu
„Bărba ii vor acces la femei pentru scurte întâlniri
părin ii lor, nici măcar despre menstrua ie
[15].
sexuale înainte de căsătorie, dar odată ce au decis să se
Constatarea cea mai importantă în cercetarea privind
căsătorească, se lansează într-o căutare frenetică pentru o
educa ia sexuală din ultimul sfert de secol con rmă ceea
fecioară pe care niciun alt bărbat nu a „de orat-o”. Prin
ce ar trebui să e evident intuitiv: copiii care cresc în
urmare, îngrijorările părin ilor arabi israelieni rezultă
familii în care sexualitatea este discutată deschis cresc
din teama că copiii lor vor face lucruri care le vor afecta
sănătoși, au o copilarie mai lungă și sunt mult mai
viitorul, cum ar
pierderea virginită ii și sarcini
responsabili [16].
nedorite.
Un aspect important în discu ia părinte-adolescent
Supravegherea și reglementarea parentală este, de
este de a stabili motivul pentru care părin ii nu reușesc
asemenea, legată de riscul mai redus de sarcină la
să se angajeze în discu ii semni cative cu copiii lor.
adolescen i.
Cercetarea a sugerat cinci clase de îngrijorări pe care
Adolescen ii ai căror părin i îi supraveghează
părin ii le exprimă cu privire la angajarea unor astfel de
îndeaproape sunt mult mai susceptibili de a avea o vârstă
discu ii: nu au cunoștin ele și aptitudinile necesare
mai mare la primul contact sexual, să aibă mai pu ini
pentru a explica lucrurile, îngrijorarea că adolescentul
parteneri și de a folosi contracep ia. Cu toate acestea,
nu își va lua părintele în serios, îngrijorarea dacă discu ia
unele studii indică faptul că monitorizarea foarte strictă
va face o diferen ă, di cultă i în a găsi momentul și locul
de către părin i este asociată cu un risc mai mare de
potrivit și teama de a încuraja activitatea sexuală [17].
sarcini la adolescente, sugerând că supravegherea mai
Unele studii au examinat impactul independent al
pu in invazivă ar putea mai e cientă [1].
surselor, cum ar părin ii, colegii și mass-media. De
Părin ii din studiul nostru au fost întreba i dacă
exemplu, atitudinile sexuale și comportamentul
sunt mai liberali decât părin ii lor. Jumătate au răspuns
adolescen ilor s-au dovedit a
legate mai mult de
că sunt par ial mai liberali și aproximativ 39,5% au spus
discu ia cu părin ii lor
[10,17]. În studiul nostru,
ca sunt mai liberali decât părin ii lor. Și aici, creștinii au
72
Joubran et al
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
ORIGINAL ARTICLES
fost mai liberali decât musulmanii. Atitudinile liberale
Concluzie
sexuale au varia ii de la o persoană la alta. Sunt la fel de
multe diferite atitudini liberale sexuale, după câ i
Scopul acestei cercetări a fost de a investiga discu ia
oameni există în lume. Unele dintre principalele
dintre părin i și copiii lor și pentru a găsi corela ia dintre
in uen e ale atitudinilor liberale sexuale sunt mediul
această discu ie și religia părintelui
(musulmană sau
socio-economic, psiho-intelectual și educa ia, credin ele
creștină), educa ie
(universitară sau nu) și gradul de
religioase și spirituale, precum și dimensiunea familiei.
religiozitate
(laici sau religioși). Am arătat că doar
Copii crescu i în familii mici bene ciază de o aten ie
jumătate dintre părin i vorbesc cu copiii lor despre
individualizată de la părin ii lor. În plus, există mai
problemele legate de sex și, dacă vorbesc despre sex,
multe resurse nanciare, economice și materiale alocate
această discu ie este în cea mai mare parte cu privire la
în familiile mici [21].
valorile religioase și etice. În plus, majoritatea părin ilor
În Israel, rata fertilită ii în rândul femeilor arabe
au vrut să știe totul despre copiii lor și rela ia cu partenerul
musulmane este foarte mare în compara ie cu rata de
lor, inclusiv cu cine și unde se întâlnesc și cât de intime
fertilitate în rândul femeilor creștine arabe (2,9% vs.
sunt întâlnirile lor. Paradoxal, cei mai mul i dintre acești
1,2%). În ultimii ani, există o tendin ă de scădere a ratei
părin i cred că sunt par ial, sau mai liberali decât părin ii
de creștere a popula iei musulmane din Israel. Acest
lor (care nu le-au dat nicio educa ie sexuală).
declin al ratei de creștere poate atribuit în mare parte
Deși există diferen e minore între părin ii creștini și
nivelului de educa ie [11].
musulmani, credem că principalul factor pentru care
Multe dintre aspectele psihosociale ale sexualită ii,
părin ii nu sunt su cient de liberali este comunitatea
cum ar atitudinile sexuale, au fost relativ neexplorate
arabă. Ini ierea discu iei despre problemele sexuale
în diverse grupuri etnice. Există motive să credem că
poate di cilă pentru părin ii din comunitatea arabă
grupurile etnice diferă în ceea ce privește valorile sexuale,
din Israel, deoarece aceștia pot nesiguri cu privire la
luând în considerare factorii separa i culturali, politici,
modul de abordare a acestor probleme.
istorici și socio-economici care in uen ează sexualitatea
Cercetarea noastră este printre pu inele studii
în ecare grup [22].
efectuate privind educa ia sexuală în general și în
În ultima întrebare, părin ii au fost întreba i despre
societatea arabă, în special. Acesta este primul studiu
educa ia sexuală pe care au primit-o de la părin ii lor.
care analizează diferen ele dintre creștini și musulmani și
Majoritatea au declarat că nu au primit nicio educa ie
primul care examinează în profunzime subiectul
sexuală. Nu au existat diferen e între creștini și
discu iei între părin i și copiii lor la aceste două
musulmani.
popula ii. Studiul nostru a contribuit în mod
În Orientul Mijlociu, tabuurile culturale sunt
semni cativ la educa ia sexuală în societatea arabă în
obstacole majore în discu iile informate despre
general, iar în particular, eviden iază asemănările care
problemele de sănătate sexuală și reproductivă, în special
există în această societate.
cu privire la adolescen i. Rela iile sexuale premaritale
Mul umiri: Societă ii pentru Dezvoltarea Cercetării
sunt interzise, iar tăcerea provine în parte din valoarea
Academice Abhath pentru sprijinul și ajutorul în
mare pe care societatea o pune pe virginitatea unei fete
desfășurarea acestui studiu.
înainte de căsătorie și din credin a că a vorbi deschis
despre sănătatea sexuală și reproductivă ar putea încuraja
tinerii necăsători i să facă sex premarital [4].
Referin e
Părin ii care au participat la acest studiu erau
adolescen i acum treizeci de ani, neprimind nicio
1. Resnick MD, Bearman P S, Blum R W, Bauman KE,
educa ie sexuală, pentru că în acele timpuri educa ia
Harris KM, Jones J, Udry JR. Protecting adolescents
sexuală nu era su cient de dezvoltată. În ciuda faptului
from harm: Findings from the National Longitudinal
că în ultimele cinci decenii a existat o liberalizare a
Study on Adolescent Health.
e Journal of the
atitudinilor sexuale și a educa iei sexuale, iar educa ia în
American Medical Association 1997;278,823-32.
sine nu aduce atingere moralei, doar jumatate din părin i
2. Miller BC, Benson B, Galbraith D. Family
au raportat că stau de vorbă cu copiii lor despre probleme
relationships and adolescent pregnancy risk: A research
legate de sex; dintre ei, mai mult de jumătate au vorbit
synthesis. Developmental Review 2001;21,1-38.
despre valorile religioase și etice ale educa iei sexuale.
3. Carrera MA. Parents and their children learning about
Opinia publică din comunitatea arabă în sondajele
sexuality. New York:
e Children’s Aid Society.
israeliene sugerează un sprijin puternic pentru abstinen ă
Retrieved on
ca un obiectiv comportamental pentru adolescen ă.
advocatesforyouth.org/parents/experts/carerra.htm.
Discourse Between Parents and Their Children about Sex in the Arab Community in Israel
73
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
4.
Kirby D, Lepore G. Sexual risk and protective factors:
13.
Muslim Women’s League. An Islamic perspective on
Factors a ecting teen sexual behavior, pregnancy,
childbearing and sexually transmitted disease.
mwlusa.org/topics/sexuality/sexuality_pos.html
Washington, DC: National Campaign to Prevent
14.
Noibi D. An Islamic perspective, in: omason R. (Ed.),
Teen and Unplanned Pregnancy, 2007.
Religion, ethnicity and sex education: Exploring the issues.
5.
Karofsky PS, Zeng L, Korosok MR. Relationship
London: National Children’s Bureau 1993, pp. 41-57.
between adolescent parental communication and
15.
Blendon R. Sex education in America: General public/
initiation of rst intercourse by adolescents. Journal of
parent’s survey. Cambridge; Harvard University, 2004.
Adolescent Health, 2000;28,41-5.
16.
Schneewind KA. Socialization and education:
6.
Moore NB, Davidson JK. Parents as rst information
eoretical perspective, in: Smelser NJ, Baltes PB.
sources: Do they make a di erence in daughters’ sexual
(Eds.), International encyclopedia of social and
attitudes and behavior? Journal of Sex Education and
behavioral sciences
(14507-14513) Amsterdam:
erapy 1999;24(3),155-63.
Elsvier, 2001.
7.
Beyth-Marom R, Fischho B. Adolescents’ decisions
17.
Fox GL. e family’s in uence on adolescent sexual
about risks: A cognitive perspective. In Schulenberg T,
behavior. Children Today, 1979;8,21-5, 36.
Maggs J, Hurrelmann K, (Eds.), Health risks and
18.
Ro man D. Sex and sensibility: e thinking parent’s
developmental
transition
during
adolescence,
guide to talking sense about sex. Cambridge,
Cambridge: Cambridge University Press 1997, pp.
Massachusetts: Perseus Publishing, 2000.
110-135
19.
Jaccard J, Dittus P. Parent-adolescent communication
8.
O’Sullivan LF, Meyer B, Heino FL, Watkins B.
about premarital pregnancy. Families in Society
Mother-daughter communication about sex among
1993;74,329-43.
urban African-American and Latino families. Journal
20.
Musso S, Fanget D, Cherabi K. An Arab-Muslim
of Adolescent Research 2001;16(3),269-92.
view. Prospect 2002;32,207-15.
9.
United Nations Population Fund. e state of the
21.
Gerholm L. Overcoming temptation: On masculinity
world population: Making one billion count investing in
and sexuality among Muslims in Stockholm. Global
adolescents’ health rights. New York: UNFPA, 2006.
Networks 2003;3,401-16.
10.
Miller BC. Families matter: A research synthesis of
22.
Mernissi F. Virginity and patriarchy. Women’s Studies
family in uences on adolescent pregnancy. Washington,
International Forum 1982;5(2),183-91.
DC: National Campaign to Prevent Teen Pregnancy,
23.
Darwin LT. e Religion and Family Connection:
1998.
Social Science Perspectives. Deseret book company, Salt
11.
Israel Central Bureau of Statistics. Press Release -
Lake City: Utah, 1988.
Publication Statistical Abstract of Israel 2007 - No. 58,
24.
Amaro H, Navarro A, Conron K, Raj A, On C.
10/09/2007.
Cultural in uences on women’s sexual health. In
aspx?itemID=7398
DiClemente RJ, Wingood GM,
(Eds.), Women’s
12.
Pope Paul VI. Gravissimum educations 3. e Vatican,
sexual and reproductive health. New York: Plenum,
1965.
2002, pp. 71-92.
Traducere: dr Bumbulu Călin
74
Joubran et al
ORIGINAL ARTICLES
ASPECTE EPIDEMIOLOGICE ALE CANCERULUI GASTRIC ÎN
JUDEȚUL ARAD
Răducan Ionu Daniel, Ciobanu Gheorghe
Departamentul Ştiin ele Vie ii, Universitatea de Vest „Vasile Goldiş” Arad, România
Adresa pentru coresponden ă:
Dr. Răducan Ionu Daniel
Tel: 0740159500
E-mail: dani_raducan@yahoo.com
Primit: 04.08.2013
Acceptat: 10.09.2013
Med Con October 2013 Vol 8, No 3, 75-78
Rezumat
Obiectivul studiului este de a identi ca principalele
aspecte epidemiologice ale cancerului gastric din jude ul
Neoplasmul gastric este unul dintre cele mai
Arad în perioada 2005-2011.
frecvente cancere ale tractului digestiv, responsabil de o
mortalitate încă ridicată. Deși prevalen a, inciden a și
Material şi metode
mortalitatea cancerului gastric au scăzut în ultimii 60 de
ani la nivel mondial, se estimează că în România
În acest studiu realizat am urmărit inciden a prin
conform datelor oferite de Globocan, se înregistrează
tumori maligne ale stomacului la nivelul jude ului Arad
peste 5000 cazuri noi pe an și 4000 decese pe an. Zonele
în perioada
2005-2011. În evaluarea statistică a
cu mortalitate crescută sunt estul Transilvaniei (Covasna,
pacien ilor diagnostica i cu cancer gastric în perioada
Harghita), vestul Transilvaniei
(Timiș, Arad, Bihor),
studiată am urmărit elemente epidemiologice, cum ar
București și jude ul Teleorman.
sexul, vârsta sau mediul de provenien ă, dar și aprecierea
Cuvinte cheie: cancer gastric, epidemiologie
extinderii procesului
tumoral conform clasi cării
interna ionale TNM
(a
7-a stadializare TNM a
Introducere în temă şi scopuri
International Union Against Cancer a cancerului
gastric) [3].
Cancerul reprezintă în lume o problemă majoră de
Datele studiului au fost ob inute de la Direc ia de
sănătate publică, prin dimensiunea implica iilor umane,
Sănătate Publică Arad și reprezintă numărul total de
medicale, economice și sociale.
pacien i diagnostica i cu cancer gastric în Jude ul Arad
Conform studiilor oferite de către World Health
în perioada studiată. Conform datelor ob inute,
Organization și e Globocan Project peste 12 milioane
diagnosticul a fost con rmat prin metode radio-
de oameni a ă în ecare an că suferă de cancer și pu ini
imagistice și histologice, iar cazurile au fost raportate la
sunt cei care reușesc să învingă boala. Se estimează că
Direc ia de Sănătate Publică Arad.
până în 2030, numărul bolnavilor se va dubla.
Conform datelor oferite de World Health
Rezultate
Organization și
e Globocan Project în România
mortalitatea prin cancer gastric ocupă locul patru după
Tabelele I, II și III, sintetizează principalele date
cancerul pulmonar, colorectal și sân [1,2].
demogra ce. În perioada studiată s-au diagnosticat 479 de
Epidemiological Aspects of Gastric Cancer in Arad County
75
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
cazuri noi de cancer gastric. În anul 2005, numărul cazurilor
diagnosticate a fost de 61; în anul 2006 - 78 de cazuri; în
2007 - 79 de cazuri, în 2008 - 81cazuri, în 2009 - 48 cazuri,
în 2010 - 87 cazuri și în 2011 - 45 de cazuri (Figura 1).
În grupa de vârstă 61-70 ani au fost diagnostica i 166
de pacien i, iar în grupa de vârstă 71-80 ani 128 pacien i.
Analiza distribu iei cazurilor de cancer gastric în
func ie de sexul pacien ilor în perioada studiată a arătat că
predomină la sexul masculin 294 (61,378% din cazuri) în
compara ie cu sexul feminin
185 (39% din cazuri),
diferen a având o valoare semni cativ statistică p=0,1424.
Figura 1. Inciden a prin tumori maligne ale stomacului
În distribu ia cazurilor diagnosticate cu cancer gastric
la nivelul Jude ului Arad în perioada 2005-2011
în Jude ul Arad am observat o inciden ă
mai crescută a cazurilor la pacien ii din
mediu rural 249 (52% dintre cazuri), în
compara ie cu pacien ii din mediu
urban 230 (48% din cazuri) (p=0,0252).
În func ie de vârsta pacien ilor și
mediul de provenien ă, în distribu ia
cazurilor de cancer gastric se observă
că persoanele diagnosticate cu cancer
gastric au fost mai numeroase după
vârsta de
60 ani (315 cazuri) și în
această categorie de vârstă cazurile din
mediu rural au fost în număr de 183,
în compara ie cu 132 de cazuri din
mediu urban. În grupa de vârstă 30-
Figura 2. Clasi carea Interna ională TNM a cazurilor diagnosticate
60 ani au fost diagnostica i
164
cu cancer gastric la nivelul Jude ului Arad în perioada 2005-2011
pacien i cu cancer gastric, dintre care
65 cazuri au fost din mediu rural și 98
Tabelul I. Date statistice privind epidemiologia
cazuri din mediu urban.
cancerului gastric în Jude ul Arad, în mediul urban
Clasi carea Interna ională TNM (a
7-a stadializare TNM a International
Date Generale
Urban
Union Against Cancer
-UICC a
Nr.
31-40
41-50
51-60
61-70
71-80
81-90
Anul Sex
cancerului
gastric)
a
cazurilor
total
ani
ani
ani
ani
ani
ani
diagnosticate cu cancer gastric în această
M
38
0
2
5
6
4
2
2005
perioadă eviden iază doar
24 cazuri
F
23
0
1
3
4
0
0
diagnosticate în stadiul I,
154 cazuri
M
53
1
3
3
8
5
3
2006
diagnosticate în stadiul II,
176 cazuri
F
25
0
3
1
3
3
1
diagnosticate în stadiul III,
95 cazuri
M
47
3
5
6
9
2
2
diagnosticate în stadiul IV, iar la 30 cazuri
2007
F
32
1
0
0
10
4
1
stadiul nu a putut precizat (Figura 2)
M
49
1
5
4
3
3
0
2008
F
32
2
4
3
6
2
0
Discu ii
M
29
0
4
5
2
2
0
2009
În jude ul Arad principala
F
19
1
1
2
3
1
0
problemă observată din studiul
M
51
1
5
7
8
7
1
2010
statistic efectuat este diagnosticul
F
36
1
2
5
12
3
1
cancerului gastric într-o fază avansată.
M
27
1
2
4
4
1
0
2011
Prevalen a cancerului gastric a fost mai
F
18
0
1
0
5
1
0
mare la sexul masculin și la persoanele
Total
479
12
38
48
83
38
11
din mediu rural. Inciden a cea mai
76
Răducan et al
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
ORIGINAL ARTICLES
crescută a cazurilor diagnosticate cu
Tabelul II. Date statistice privind epidemiologia cancerului gastric
cancer gastric în jude ul Arad s-a
în Jude ul Arad, în mediu rural
întâlnit la persoanele de peste 60 ani.
Date Generale
Rural
Cele mai multe cazuri diagnosticate cu
Nr.
31-40
41-50
51-60
61-70
71-80
81-90
Anul Sex
cancer gastric în această perioadă au
total
ani
ani
ani
ani
ani
ani
fost descoperite în stadiul III
M
38
0
2
3
7
6
1
(Aprecierea extinderii
procesului
2005
F
23
0
0
1
8
5
1
tumoral conform stadiilor TNM).
Comparând datele statistice
M
53
0
1
4
9
14
2
2006
ob inute cu cele din literatură, am
F
25
0
2
3
3
6
0
observat că grupele de vârstă cele mai
M
47
1
2
2
7
7
1
frecvent afectate sunt cele peste
60
2007
ani, dar în analiza efectuată am
F
32
0
0
2
5
9
0
observat că neoplasmul gastric a fost
M
49
1
4
6
9
10
3
diagnosticat la 164 cazuri, cu vârsta
2008
F
32
0
2
1
5
7
0
până în
60 ani. În literatura de
M
29
1
1
2
5
7
0
specialitate se precizează un număr
2009
redus de cazuri diagnosticate înainte
F
19
0
3
3
4
1
0
de 60 ani în compara ie cu cazurile
M
51
1
2
3
6
9
1
diagnosticate în Arad în această grupă
2010
F
36
0
3
2
5
2
0
de vârstă. Diferen a de inciden ă între
mediul
urban/rural
este
M
27
0
1
2
7
5
0
2011
nesemni cativă, dar este mai ridicată
F
18
0
2
3
3
2
1
la categoriile sociale defavorizate și în
Total
479
4
25
37
83
90
10
special în mediu rural [2,3,4,5].
În urma studiului statistic efectuat
am observat o prevalen ă a cancerului
Tabelul III. Date statistice privind aprecierea
gastric mai mare la sexul masculin
(61%) fa ă de cel feminin
(39%).
extinderii procesului tumoral, conform stadializării TNM
Inciden a cea mai crescută a cancerului
Date Generale
Stadiul
gastric s-a întâlnit la persoanele de
Total
NE-
Anul
Sex
I
II
III
IV
peste
60 ani, atât la pacien ii din
pacien i
PRECIZABIL
mediu urban, cât și la pacien ii din
M
38
0
8
17
13
0
mediu rural. Se observă o inciden ă
2005
F
23
1
6
9
7
0
crescută a bolii în mediul rural (52%),
fa ă de mediul urban (48%).
M
53
1
15
18
14
5
2006
La nivel mondial, cancerul gastric
F
25
0
4
13
6
2
reprezintă aproximativ
930.000 de
M
47
3
13
18
8
5
cazuri noi și determină mai mult de
2007
700.000 de decese. Vârsta medie la
F
32
3
9
13
7
0
diagnostic este de 71 ani în SUA și o
M
49
1
13
20
12
3
2008
decadă mai devreme în Japonia [6].
F
32
3
13
12
3
1
Studiul de fa ă, este după datele pe
M
29
3
6
12
7
1
care le de inem, primul de acest gen.
2009
Urmează ca în cercetări viitoare să se
F
19
1
6
9
2
1
caute cauzele diferen elor epidemiologice
M
51
3
27
9
9
3
din diverse zone geogra ce.
2010
F
36
1
15
11
2
7
Mul umiri: Această lucrare a fost
co nan ată din Fondul Social
M
27
3
10
10
3
1
2011
European, prin Programul Opera ional
F
18
1
9
5
2
1
Sectorial Dezvoltarea Resurselor Umane
TOTAL
479
24
154
176
95
30
2007-2013,
contract
Epidemiological Aspects of Gastric Cancer in Arad County
77
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
POSDRU/107/1.5/S/77082 - „Burse doctorale de pregătire
4. Crew KD, Neugat AI. Epidemiology of Gastric Cancer.
ecoeconomică și bioeconomică complexă pentru siguran a și
World J Gastroenterol.2006 ;12(3):354-62.
securitatea alimentelor și furajelor din ecosisteme antropice”.
5. Ries L, Melbert D, Krapcho M, et al. Editori. SEER Cancer
Statistics Review, National Cancer Institute, Bethesda;
2007:1975-2004.
Referin e
6. Anderson W, Camargo C, Fraumeni J, Correa P,
Rosenberg P, Rabkin C. Age-Specific Trends in Incidence
1.
of Noncardia Gastric Cancer in US Adults. JAMA
2010;303(17):1723-8.
78
Răducan et al
ORIGINAL ARTICLES
INFLUENȚELE MEDIULUI ÎN COMPORTAMENTUL ADICTIV AL
PERSOANELOR DIN JUDEȚUL CLUJ
Kelemen Alexander, Podea Delia, Puşchi ă Maria
Facultatea de Medicină,Universitatea de Vest „Vasile Goldiş”, Arad, România
Adresa pentru coresponden ă:
Kelemen Alexander
Spitalul Clinic Minicipal Cluj, Psihiatrie Cr. II
Str. Decebal, nr. 126, Cluj-Napoca, România
Email: Phd.alexander.kelemen@gmail.com
Primit: 23.04.2013
Acceptat: 20.08.2013
Med Con October 2013 Vol 8, No 3, 79-82
Rezumat
exemplu pu ine festivită i se desfășoară în absen a
consumului de alcool și de tutun, etc.).
Obiectivele studiului sunt ob inerea datelor privind
Unul din factorii redutabili în apari ia
prevalen a consumului diferitelor substan e psihoactive,
comportamentului adictiv îl reprezintă presiunea
identi carea unor atitudini, în ceea ce privește consumul
socială. Se referă nu numai la ocaziile familiale,
de droguri, identi carea modelelor de consum, a
profesionale, la toleran a socială, dar și la interesele
factorilor de risc și de protec ie ale acestora.
economice ce impun vânzarea drogului [1].
Materiale și metode: Metoda de cercetare utilizată
Totodată, există și foarte multe prejudecă i sociale
a fost interviul psihologic anamnestic cantitativ, iar
asupra adic iei. Drogul forti că, favorizează în anumite
instrumentul de cercetare aplicat a fost un chestionar
contexte integrarea socială, joacă un rol ini iatic în
structurat cu 40 de întrebări care se referă la obiectivele
statutul adultului și intră în rezonan ă cu unele
cercetării.
di cultă i proprii ale individului, suferind deja de o
Rezultate: Dependen ii de droguri apar in unor
inhibi ie rela ională, de incertitudine asupra propriei
pături sociale diverse, iar unele categorii sociale par a
valori. În plus, abstinen a, surprinzător poate să ducă la
avea o predispozi ie în acest sens. Există corela ii
marginalizarea individului, mai ales în mediile unde
importante statistic între comportamentul adictiv de-a
consumul este o practică frecventă, chiar și fără a exista
lungul vie ii și caracteristici sociodemogra ce.
riscul de dependen ă [2,3].
Cuvinte
cheie:
adic ie,
comportamente
Pe plan epidemiologic rolul factorilor socio-culturali
dezadaptative, background anamnestic
este demonstrat de propor iile diferite de consumatori
integra i în grupele sociale, profesionale sau într-un
Introducere
anumit grup de societate. Comportamentul adictiv îl
regăsim mai frecvent în profesiile care impun o muncă
Consumul de droguri este un fenomen care se
mai di cilă, pu in cali cată, în profesiile care impun un
regăsește în aproape toate socită ile studiate din
contact cu publicul (chelneri, comis-voiajori, etc) [4].
antichitate până în zilele noastre. Drogul este asociat
Un nivel modest educativ, condi iile precare de via ă,
ritualurilor religioase și această conduită o întâlnim și
par de asemenea a
factori favorizan i în alegerea
sub forma micilor ritualuri ale societă ilor moderne (de
consumului.
Environmental Influences on Addictive Behavior of the People in Cluj County
79
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
Anumite comportamente adictive sunt mai ușor
Analiza statistică
repetate în clasele sociale defavorizate decât în mediile
înalte, unde sunt mai mascate.
S-a făcut în programul SPSS și a urmărit stabilirea
Studiile sociologice descriu o prelevan ă ridicată a
prevalen ei consumului de droguri în func ie de diverse
consumului în raport cu unele norme culturale. În
variabile socio-demogra ce (clasă, vârstă, sex, forma de
particular, consumul excesiv de drog ar apărea
învă ământ, mediu familial, anturaj), modele de
preferen ial într-un context în care sunt prezente
consum, riscuri percepute, etc. Pentru ecare dintre
normele asociate consumului și în care nu există norme
aceste corela ii au fost calculate teste de semni ca ie
prescriptive [5,6]. Așa se întâmplă în societă ile numite
statistică.
anxiogene, în societă ile nomade, în comunită ile
dezorganizate, în mediile sociale defavorizate, în mod
Rezultate
special în unele subculturi din cadrul marilor metropole,
în care consumul de alcool, tutun și alte droguri sunt
Date generale
mai frecvente [7].
Lotul de cercetat este constituit din 50 de persoane,
32 (64%) de gen masculin și 18 (36%) de gen feminin.
Materiale şi metode
Distribu ia pe vârste este următoarea: 6 responden i cu
vârsta sub 18 ani, 36 de subiec i pâna în 30 de ani și 8
Studiul este reprezentativ pentru popula ia formată
subiec i cu vârsta de peste 30 de ani.
din persoanele cu probleme de adic ie din jude ul Cluj.
Din punct de vedere educativ
57,3% din cei
Baza de date pentru eșantionare a fost furnizată de
intervieva i au urmat cel pu in cursuri profesionale,
ARAS Cluj și Spitalul Clinic Municipal Cluj, Sec ia de
27,9% înva ă într-o unitate de învă ământ superior,
Psihiatrie. Metoda de eșantionare a fost cea aleatoare
14,8% au cunoscut abandonul școlar. Mediul de
simplă, astfel oricare subiect care făcea parte din
provenien ă al responden ilor era
76% din mediul
categoria vizată avea șanse egale să e parte din studiu,
urban, 20% locuiseră până la vârsta majoratului doar în
fără niciun criteriu de discriminare. Lotul a fost format
mediu rural și 4% din responden i proveneau din rural
din 50 de responden i, to i pacien i cunoscu i centrului
(contactul cu orașul ind ocazional și ritmat de
psihiatric de substitu ie cu metadonă. Metoda de
evenimente sociale extracurriculare).
cercetare utilizată a fost interviul clinic cantitativ, iar
Date anamnestice heredo-colaterale
instrumentul de cercetare aplicat a fost un chestionar
Majoritatea celor intervieva i au fost născu i și
structurat cu 40 de întrebări care se referă la cunoștin ele,
crescu i în familie de muncitori, cu un nivel educativ
atitudinile, practicile de consum ale liceenilor, precum și
satisfăcător: părin ii a
8% absolviseră maxim 8 clase
la factorii de risc și de protec ie în ceea ce privește
elementare,
20,4% erau absolven i ai unei școli
consumul de tutun, alcool și droguri ilegale.
profesionale,
36,6% (53,2% dintre mame, respectiv
Tehnica de anchetă utilizată pentru acest studiu a
43,5% dintre ta i) aveau studii medii și 9,6% studii
fost chestionarul autoaplicat. Pentru realizarea acestei
universitare. Cei proveni i din familii dezorganizate, cu
cercetări s-a urmărit asigurarea con den ialită ii prin
părin i care au abandonat căminul familial și care nu
păstrarea anonimatului persoanelor intervievate.
pot men iona nivelul de școlarizare, au constituit
Designul chestionarelor-interviul structurat a fost
14,2%.
împăr it strategic pe întrebări care acopereau toate ariile
Legăturile afective în familie erau descrise ca ind
precum cunoașterea
opiniilor
și
atitudinea
par ial armonice, modelele de adaptare ind construite pe
responden ilor fa ă de consum și consumatori, tipurile
constela ii cu prevalen ă în oralitate, modul de rela ionare
de droguri care fac obiectul consumului, vârsta de debut
cu lumea și cu familia alternau între dependen ă și
în consumul de droguri, motiva ia pentru consum,
agresivitate, nu exista ascensiune către o dezvoltare
disponibilitatea drogurilor pe pia ă și al i factori de risc
psihologică autonomă. Existau comportamente de
și de protec ie în cazul consumului de droguri (stima de
autoagresivitate și lentă adaptare a imaginii de sine și
sine, implicarea în activită ile școlare, modul de petrecere
automatismul de repeti ie (teoretic ar exista un eveniment
a timpului, in uen a anturajului în luarea deciziilor,
traumatic, niciodată integrat în via a psihică). Nu s-a
autoritatea părin ilor și implicarea acestora în educa ia
putut stabili o corela ie din punct de vedere socio-
copiilor, rela ia cu grupul de prieteni). Interviul s-a făcut
economic cu mediul social de origine, în schimb se
pe un numar semni cativ de responden i, pacien i ai
constată o frecven ă sporită la cei ai căror părin i sunt
Clinicii de Psihiatrie Cluj, având diagnostic de consum
consumatori, dependen i de diverse medicamente
cronic de alcool.
psihotrope și la care există familii dezorganizate.
80
Kelemen et al
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
ORIGINAL ARTICLES
Prevalen a consumului
consumul din curiozitate, 15% prin imita ie, 8% o
Mai mult de o treime din subiec i au declarat consum
alternativă la stres, iar 6% au inten ionat să depășească
de droguri ușoare (tutun, alcool, etnobotanice, etc.) cel
cu ajutorul lui o puternică stare depresivă), iar 16% au
pu in cu o ocazie, peste 60% dintre responden i au dorit
atribuit cauze internalizate (10% neîncredere în sine,
și repetat experien a, iar mai mult de unul din 5 subiec i
6% timiditate).
au răspuns pozitiv privitor la un consum în ultimele 30
În ceea ce privesc evenimentele și antecedentele
de zile. Din lotul de 50 subiec i, 32 erau de gen masculin,
personale din copilărie se remarcă: frecven a sporită a
iar dintre aceștia
29 aveau diagnostic de consum de
tratamentelor cu psihotrope în mica copilărie,
droguri, altele decât tranchilizante sau sedative. Din 18
plasamente sociale precoce, studii școlare inferioare
subiec i de gen feminin, 14 consumau benzodiazepine și
standardelor, abandon de cămin, tulburări de somn,
alte tranchilizante. În general bărba ii preferă marijuana
crize nervoase și manifestări psiho-somatice.
sau hașiș, iar femeile tranchilizante sau sedative. În plus,
Asocierea dintre prevalen a consumului de droguri
adic ia are prevalen ă în rândul bărba ilor.
la responden i și modul în care aceștia se rela ionează cu
Referitor la loca iile preferate și posibilită ile
cei din jur, își percep propria persoană și iau decizii, este
manifestărilor adic iei, există date semni cative statistic
semni cativă statistic. Astfel, subiec ii care au declarat
care arată corela ii strânse între mediul de reziden ă,
că au consumat cel pu in o dată în via ă droguri,
disponibilitatea drogului și modelul utilizat. Analiza
comparativ cu cei care nu au background de consum, au
disponibilită ii și accesibilită ii drogului pentru
di cultă i în a cere ajutorul atunci când au probleme
persoanele din jude ul Cluj indică faptul că 33% din cei
(63,6%) și consideră într-o mai mare măsură că
intervieva i nu au probleme în procurarea unor droguri
„singurul mod de a face fa ă agresiunilor este să îi lași pe
oricând doresc,
41% au declarat că acest lucru este
al i să în eleagă cine este șeful”. De asemeni, au încredere
di cil, dar nu imposibil, 6% apreciază că acest lucru este
mai mică în for ele proprii: „câteodată mă gândesc că nu
imposibil fără ajutorul cuiva, iar 20% au optat pentru
sunt bun de nimic” (60,7%).
varianta de răspuns „nu știu/nu răspund” (Figura 1).
Motiva ia consumului de droguri indicată de
Discu ii
toxicomanii investiga i este în principal curiozitatea
(75%), sus inută de o puternică dorin ă de a rmare
În studiul nostru am constatat că frecven a
personală și de integrare în microgrup. Curiozitatea este
comportamentului adictiv se intensi că odată cu vârsta
înso ită de lipsa unei informări corecte și complete
majoră, cu toate că persoanele tinere sunt mai tentate de
asupra drogurilor și a efectelor acestora (75%). Există
consumul de droguri mai mult decât persoanele
însă și cazuri (25%) în care deși responden ii a rmativ
vârstnice. Din lotul de 50 responden i doar 6 subiec i
erau pe deplin conștien i asupra efectelor drogurilor și
erau minori. Există o corela ie directă între nivelul de
riscului existent, au optat pentru drog ca o solu ie
școlarizare și model adictiv, situa ia familială
-
ocazională.
background-ul familial negativ împinge subiec ii spre
Conștiin a stării psihice și modul de prelucrare
comportamente dezadaptative
(părin i consumatori,
Locusul de control atribuit (Figura 2) a fost external
antecedente heredo-colaterale anxiogene și depresive,
la
84% din cazuri (55% din responden i au motivat
familii dezorganizate). Locuitorii orașelor mari sunt mai
Figura 1. Analiza disponibilită ii şi accesibilită ii
Figura 2. Distribu ia locusului de control
drogului în jude ul Cluj
în consumul de droguri privind popula ia din Cluj
Environmental Influences on Addictive Behavior of the People in Cluj County
81
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
expuși la acest agel în compara ie cu persoanele din
individului, mai ales în mediile unde consumul este o
mediul rural.
practică frecventă, chiar și fără a exista riscul de
În studiul de fa ă am pornit de la o realitate bazată
dependen ă.
pe considerentul că dependen a este rezultatul unei
triple întâlniri între produs, personalitate și momentul
socio-cultural.
Referin e
Produsele pot face obiectul unei utilizări
toxicomanice în anumite societă i, dar în alte societă i
1. Mitrofan, I. Terapia toxicodependen ei - posibilită i şi
sunt utilizate și acceptate social într-un alt cadru cultural.
limite [ erapy drugs dependencies - possibilities and
Drogul este asociat ritualurilor religioase și această
limitations], Ed. Sper, 2003.
conduită o întâlnim și sub forma micilor ritualuri ale
2. Ades J, et al. Le classi cations de l’alcoolisme, Ed.
societă ilor moderne (de exemplu pu ine festivită i se
Masson, 1997.
desfășoară în absen a consumului de alcool și de tutun,
3. Biro, MA, Prolegomene clinice [Clinical Prolegomena],
etc.).
Editura Dacia, 2001.
Unul din factorii redutabili în apari ia
4. Magura, S. e role of work în substance dependency
comportamentului addictiv îl reprezintă presiunea
treatment: a preliminary overview. Substance Use and
socială. Se referă nu numai la ocaziile familiale,
Misuse, 2003.
profesionale, la toleran a socială, dar și la interesele
5. Planul de Ac iune pentru Implementarea Strategiei
economice ce impun vânzarea drogului.
Na ionale Antidrog
[Action Plan for the
Drogul forti că, favorizează în anumite contexte
Implementation of the National Drug Strategy]
integrarea socială, joacă un rol ini iatic în statutul
2005-2008.
adultului și intră în rezonan ă cu unele di cultă i proprii
6. Strategia Europeană privind Drogurile
[European
ale individului, suferind deja de o inhibi ie rela ională,
Strategy on Drugs] 2005-2012.
de incertitudine asupra propriei valori. În plus,
7. Winnicott W, et al. Procesuss de Maturation chez
abstinen a, surprinzător poate să ducă la marginalizarea
l’Enfant, Ed. Payot, 1978.
82
Kelemen et al
GENERAL REVIEW
MANIFESTĂRI BUCALE LA PACIENȚII CU AFECȚIUNI ALE SERIEI
ROŞII SANGUINE ŞI TULBURĂRI DE COAGULARE. O REVISTĂ A
LITERATURII
Pop Diana-Ioana, ovaru Şerban
Catedra de Patologie Orală, Facultatea de Medicină Dentară, Universitatea de Medicină şi Farmacie „Carol Davila”
Bucureşti, România
Adresa pentru coresponden ă:
Dr. Pop Diana-Ioana
Bd. Mărăşeşti Nr. 42, Bl. 1, Ap 121, Sector 4, 040255, Bucureşti
Tel: 0742377610
E-mail: popdianaioana@yahoo.com
Primit: 08.07.2013
Acceptat: 15.08.2013
Med Con October 2013 Vol 8, No 3, 83-88
Rezumat
căror afec iuni interesează mai multe specialită i
medicale. Patologia bucală din hemopatii a fost îndelung
Articolul descrie leziunile elementare observate în
neglijată de medicii dentiști, iar pacien ii au fost trata i
cavitatea bucală în cazul sindroamelor hemoragice și în
pentru boala de fond în clinicile de hematologie,
afec iunile seriei eritroide sanguine. Au fost identi cate și
manifestările intraorale ale afec iunii nereprezentând o
descrise afec iunile seriei roșii
(anemii, poliglobulii) și
prioritate. Este absolut esen ial ca medicul dentist să
tulburările de coagulare (ce implică atât trombocitul cât și
cunoască tipurile de sindroame hemoragice și
factorii plasmatici ai coagulării) care pot determina
manifestările orale care pot să apară în ecare dintre ele.
manifestări la nivelul cavită ii bucale și au fost descrise pe
Pot astfel prevenite complica iile și pot tratate din
scurt aceste manifestări. Paloarea mucoaselor, xerostomia,
timp afec iunile, pentru a preîntâmpina eventualele
glosita atro că, cheilita angulară, ulcera iile, gingivoragiile,
neplăceri. Manopere dentare ca extrac iile și chirurgia
peteșiile, echimozele sau edemele sunt manifestări orale
parodontală sunt proceduri invazive care se asociază în
comune, unele nespeci ce, ale tulburărilor de coagulare și
mod obișnuit cu sângerări posttratament care, în cele
ale afec iunilor seriei eritroide sanguine. Fie că apar
mai multe cazuri, se opresc de la sine, dacă pacientul nu
precoce, tardiv, în cursul evolu iei bolii sau ca efect în
suferă de sindroame hemoragice. Un număr mic, dar
urma tratamentului, manifestările bucale din hemopatii
semni cativ din popula ie prezintă probleme de
nu au un caracter patognomonic și trebuie luate în
coagulare, la care chiar și interven iile minim invazive
considerare în contextul clinic și biologic. Tratamentul
pot să determine risc de sângerare crescut.
stomatologic al pacien ilor trebuie adaptat în func ie de
Sângerarea excesivă nu reprezintă numai un
boala hematologică de fond, pentru ecare caz în parte.
disconfort pentru pacient, dar poate interfera cu alte
Cuvinte cheie: afec iune hemoragică, anemie,
proceduri medicale (de exemplu sutura plăgii) și poate
manifestări orale
uneori chiar compromite starea generală de sănătate a
pacientului.
Introducere
În ultimul timp tot mai multe persoane suferă de
afec iuni hematologice congenitale sau dobândite ca
În ultimii 10 ani o tot mai mare aten ie a fost
urmare a medica iei, afec iunilor altor organe, sau a
acordată terapiilor interdisciplinare și pacien ilor ale
consumului de alcool
[1]. Managementul dentar al
Oral Manifestations in Patients with Red Blood Series Pathology and Coagulation Disorders. Review of Literature
83
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
acestor pacien i trebuie să cuprindă o cunoaștere cât mai
creștere a sensibilită ii la alimente acide, condimentate
exactă a afec iunilor de către medicul dentist și
etc, pacien ii acuzând senza ie de usturime. Anemia
colaborarea acestuia cu medicul hematolog.
feriprivă se asociază frecvent și cu glosită atro că și cheilita
Manifestările bucale ale hemopatiilor au fost în elese
angulară și ragade comisurale [2,7]. Cheilita angulară se
în diferite moduri de stomatologi și de hematologi, în
poate suprainfecta cu Candida albicans și/ sau al i germeni
conformitate cu evolu ia bolii, a metodelor de diagnostic
și poate apărea deshidratarea mucoasei [8].
și cu progresele terapeutice.
Sindromul Plummer-Vinson se mai numește
Diagnosticarea manifestărilor orale în cadrul
sindromul Kelly-Paterson. Este un sindrom complex,
tulburărilor de coagulare și în afec iunile seriei roșii este
cauzat de de citul cronic de er [9]. Se manifestă prin
foarte importantă pentru medicului stomatolog și
glosită atro că și ocazional prin apari ia de leziuni
pentru practica de zi cu zi. Medicul dentist trebuie să
keratozice pe mucoasa orală. Se mai pot asocia și disfagie
recunoască leziunile elementare ce apar la nivelul
și atro a mucoasei orofaringiene [3,10].
cavită ii orale la pacien ii cu boală hematologică de
Talasemia este o anemie constitu ională care
fond; să facă diagnosticul diferen ial al acestor leziuni cu
presupune defecte în sinteza lan urilor α sau β
cele care apar în cadrul altor boli și sindroame la nivel
polipeptidice ale hemoglobinei. În func ie de lan ul de
intraoral; să realizeze un plan de tratament care să ia în
globină care prezintă defectul cantitativ de sinteză,
calcul eventualele complica ii care se pot asocia cu
talasemiile sunt divizate în două grupuri principale: α
tulburarea de coagulare sau cu anemia [1,2].
talasemii și β talasemii
[7]. Aspectul oro-facial al
Pentru diagnosticarea unui sindrom hemoragic
pacien ilor cu talasemie este cunoscut sub numele de
izolat pot
utile revizuirea și recunoașterea formelor
facies Cooley: boselarea oaselor frontale și parietale,
elementare ale diferitelor leziuni bucale, în asociere cu
mărirea oaselor maxilare care datermină anomalii de
modi carea hemoleucogramei: hemoragii în caz de
implantare ale din ilor, uneori cu aspecte monstruoase și
trombopenie, paloare sau glosite în caz de anemie,
ocluzie modi cată (ocluzie deschisă, inocluzie sagitală
hiperplazii gingivale în poliglobulii, glosită Hunter în
marcată sau alte forme de malocluzie) [11]. Mucoasa
anemia Biermer, etc [3]. Studiile din ultimii ani nu
orală este palidă de cele mai multe ori [11,12]. În cazul
con in o abordare su cientă a acestui subiect, doar în
α talasemiilor pacien ii sunt asimptomatici, dar pot
ultima decadă existând un interes interdisciplinar între
prezenta uneori o anemie ușoară, exprimată la nivel oral
medicina dentară și hematologie, rezultatele ind însă
prin paloarea mucoasei [12,13].
pu ine.
Anemia pernicioasă
Biermer
(anemie
Această trecere în revistă a literaturii prezintă
megaloblastică) apare în cazul unei de cien e de
principalele afec iuni ale seriei roșii sanguine și
vitamina B12. Intraoral semnul patognomonic este
tulburările de coagulare, manifestările lor intraorale și
glosita Hunter, care reprezintă atro a progresivă a
particularită ile
terapeutice
pentru principalele
papilelor liforme și fungiforme [14,15]. Acestea dau
proceduri dentare.
un aspect roșu lucios și neted al fe ei dorsale a limbii
[15]. Atro a limbii se instalează progresiv și se poate
Manifestări bucale în afec iunile seriei
complica uneori cu suri și/ sau leziuni ulcerative sau
roşii
vezicule dureroase și sensibile la contactul cu alimentele
[2,15,16]. Depapilarea pe toată suprafa a limbii permite
Hemopatiile seriei roșii (eritrocitelor) sunt împăr ite
diferen ierea de alte tipuri de glosită [6]. Glosita Hunter
în func ie de creșterea sau scăderea numărului acestora
constituie un semn important în anemia Biermer,
în anemii, respectiv eritremii
(policitemie sau
putând apărea oricând în timpul evolu iei bolii [17]. În
eritroblastoze).
cazul în care precede anemia este un semn sugestiv
Anemia prin de cit de er este cel mai comun tip
pentru diagnosticarea anemiei Biermer și permite
de anemie [4]. În sfera orală manifestările sunt frecvente,
instituirea unui tratament precoce [14,18].
observându-se paloarea mucoaselor, xerostomie, leziuni
Anemia aplastică este o afec iune caracterizată prin
aftoase, glosită atro că, zone de in ama ie de culoare
pancitopenie determinată de reducerea cantită ii de
roșie- violacee, cu gingii adiacente palide
[5]. Glosita
esut hematopoietic din măduva osoasă. Severitatea
atro că se manifestă printr-o limbă depapilată și
simptomelor depinde de gradul citopeniei [19]. La nivel
eritematoasă
[4], care poate
confundată cu glosita
bucal se observă mai ales gingivoragii și peteșii. Mucoasa
migratorie (în acest caz zonele depapilate și eritematoase
este palidă, uscată și atro că; fa a dorsală a limbii este
sunt înconjurate de un halou keratozic) [6]. În anumite
netedă, nă și dureroasă; cheilita angulară poate
cazuri de anemie feriprivă limba poate avea o ușoară
prezentă [20]; uneori se observă ulcera ii ale mucoasei,
84
Pop et al
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
GENERAL REVIEW
suprainfectări cu Candida albicans sau infec ii virale,
perfectă: etapa vasculară, etapa trombocitară, etapa de
acestea din urmă
ind datorate imunosupresiei
activare a factorilor de coagulare (coagularea propriu-
(neutropenie, limfopenie) [8,20].
zisă), etapa de brinoliză ziologică. Dacă apar defecte
Sicklemia este o anemie hemolitică cronică legată de
la una sau mai multe dintre aceste etape, cu înclinarea
fenomenul de siclizare al hematiilor (hematiile își pierd
balan ei spre brinoliză, atunci apar fenomene de
forma normală, căpătând aspect de
„seceră) în cursul
sângerare. Tulburările de coagulare
(dobândite sau
deoxigenării [1]. În această variantă de hemoglobină, acidul
moștenite) pot produce o serie de manifestări orale care
glutamic din pozi ia 6 a lan ului β normal este înlocuit
includ: peteșii, hematoame ale limbii [36], sângerare
printr-o moleculă de valină [21]. Anemia din sicklemie
gingivală spontană sau prelungită postinterven ie
prezintă câteva modi cări oro-faciale: hipomineralizarea
chirurgicală [37]. Traume minime cum ar periajul
smal ului și prezen a diastemei
[22,23,24], scăderea
dentar sau mastica ia pot cauza hemoragii gingivale
densită ii osoase la nivel apical [25], anestezia sau parestezia
prelungite în timp, chiar dacă profunzimea plăgii nu
nervului mentonier [26,27], necroză pulpară asimptomatică
este semni cativă [37].
[28]. Osteomielita mandibulei este o complica ie frecventă
Etapa vasculară a hemostazei constă într-un proces
observată la pacien ii cu sicklemie, care rareori este înso ită
de vasoconstric ie locală care reduce dimensiunea breșei
de alte complica ii, facilitând diagnosticul și tratamentul
vasculare. În cazul în care etapa vasculară este alterată
[29]. Durerile la nivelul mandibulei pot preceda neuropatia
(cel mai frecvent printr-o anomalie a peretelui vasului
nervului alveolar inferior și parestezia buzei inferioare.
de sânge), apare mai frecvent sângerarea la nivelul pielii,
Biopsia gingivală poate releva prezen a eritrocitelor
manifestată prin peteșii, echimoze sau ambele. Defectul
modi cate în vasele de sânge ale epiteliului [30]. Saint Clair
vascular care cauzează hemoragia poate moștenit sau
de Velasquez a raportat într-un studiu efectuat pe popula ia
dobândit [3,36].
din Venezuela că cea mai comună manifestare intraorală la
Etapa trombocitară cuprinde următoarele
pacien ii cu anemie cu sicklemie este paloarea mucoasei, iar
momente: adeziunea, agregarea și secre ia trombocitară.
malocluzia la acești pacien i este deseori prezentă și poate
Sângerările anormale se asociază cu trombocitopenie
explicată prin modi carea echilibrului muscular perioral
(număr scăzut de plachete sanguine) sau trombocitopatie
[31].
(alterarea func iei plachetelor) și includ: hemoragii
Eritremia este o afec iune caracterizată prin
gingivale și ale mucoasei bucale, sângerări prelungite
creșterea numărului de globule roșii din sânge
postinterven ie chirurgicală [38].
(poliglobulie) și printr-o hiperplazie a măduvei osoase.
Trombastenia Glanzmann este o anomalie extrem
Se clasi că în policitemie și eritroblastoză [3].
de rară care se manifestă intraoral prin hemoragii
Policitemia desemnează creșterea hematocritului, a
gingivale, purpură și peteșii ale mucoasei [39].
valorilor hemoglobinei și a numărului total de eritrocite
Coagularea propriu-zisă se realizează pe două căi
[32]. Intraoral se pot observa: gingia congestionată,
distincte, care interac ionează: calea intrinsecă și calea
edema iată, ulcera ii roșu-violacee sau purpurii,
extrinsecă. Calea extrinsecă este activată prin
gingivoragii, peteșii, echimoze, manifestările hemoragice
traumatisme externe care provoacă sângerare. Această
ind accentuate și de sindroamele de hipervâscozitate
cale este mai rapidă decât calea intrinsecă. Implică
[33,34].
factorul VII al coagulării. Calea intrinsecă este activată
Eritroblastoza se caracterizează prin apari ia în
de traume din interiorul sistemului vascular și este
sânge a eritroblaștilor și se observă după splenectomie,
activată de trombocite, endoteliul expus, substan e
după o hemoragie acută și în cursul oricărei hemolize
chimice sau colagen. Această cale este mai lentă decât
importante, în special în boala hemolitică a nou-
cea extrinsecă, dar mult mai importantă. Implică factorii
născutului. Exprimă o manifestare reactivă, o stimulare a
XII, XI, IX, VIII ai coagulării. Ambele căi se unesc și
eritropoezei, declanșată de pierderea sau distrugerea
încheie formarea cheagului în ceea ce este cunoscut sub
globulelor roșii. Ea poate uneori să traducă și o afectare
numele de calea comună a coagulării. Aceasta implică
primitivă a măduvei osoase [7]. Intraoral s-au raportat
factorii I, II, V și X [40].
ulcera ii pe fond roșu-violaceu și congestia gingiilor [35].
Defectele în etapa coagulării pot
conven ional
împăr ite în două categorii: prima cu pacien i cu defecte
Manifestări bucale ale sindroamelor
dobândite ale anumitor factori (protrombină, factorul
hemoragice
VII, IX, X), care apar în urma tratamentului cu
medicamente anticoagulante, prin de cien e ale
În condi ii normale, hemostaza se desfășoară în
vitaminei K și ca rezultat al bolilor hepatice (tulburări
patru etape care se succed într-o armonie func ională
de sinteză). A doua categorie, pacien i cu defecte
Oral Manifestations in Patients with Red Blood Series Pathology and Coagulation Disorders. Review of Literature
85
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
congenitale ale unuia sau mai multor factori ai
gingivoragii. Parodontita poate determina mobilitate
coagulării. La aceste grupe de pacien i se observă
dentară și poate impune necesitatea unei extrac ii, greu
intraoral purpură la nivelul limbii și palatului, hematom
de realizat la acești pacien i [47].
intraoral, echimoze la nivelul buzelor, limbii și mucoasei
Tratament endodontic și restaurativ. Procedurile
orale, sângerări gingivale spontane sau postraumatice,
restaurative nu ridică problema sângerării la pacien ii cu
hemoragie prelungită în urma extrac iilor. Pot să mai
coagulopatii. Trebuie avut totuși în vedere să nu se lezeze
apară (cel mai adesea în cazul pacien ilor cu hemo lie)
gingia prin diferite proceduri: aplicarea clemei pt digă,
hemartroză și artropatie la nivelul articula iei temporo-
șlefuiri subgingivale, etc. Tratamentul endodontic este
mandibulare [35,36,37].
de preferat în locul extrac iei la acești pacien i, ori de
Etapa de brinoliză: sângerări gingivale.
câte ori este posibil [37].
Tratamentul protetic. Acest tip de tratament nu ar
Managementul stomatologic al
trebui să prezinte risc crescut de sângerare, trauma ind
pacien ilor cu tulburări de coagulare
minimă dacă fazele de tratament se respectă și se
efectuează cu o aten ie sporită.
Conduita terapeutică a pacien ilor cu tulburări de
Alegerea terapiei medicamentoase. Multe
coagulare depinde în mare măsură de mecanismul
medicamente prescrise în practica dentară interferă cu
etiopatogenic al bolii, gravitatea acesteia și tipul de
procesul hemostazei. În plus, alte medicamente ca
interven ie stomatologică ce urmează a
efectuată.
antii amatoarele nesteroidiene pot poten a efectul
Dacă procedura stomatologică este minim invazivă, iar
anticoagulantelor orale prin afectarea func iei plachetare,
hemopatia este compensată, se pot realiza, fără a avea un
crescând riscul sângerării [48]. Penicilina, Eritromicina
risc crescut manoperele dentare.
și Miconazolul poten ează și ele efectul Trombostopului
Dacă pacientul prezintă o tulburare de coagulare
[49]. Medicul dentist trebuie să aibă în vedere medica ia
severă este necesar ca mai întâi să e tratată pe cât posibil
curentă a pacientului și să se consulte cu medicul său
boala hematologică de fond și să se asigure ulterior o
hematolog pentru prescrierea acestor medicamente.
hemostază locală cât mai riguroasă [41].
În concluzie, manifestările orale ale hemopatiilor
Controlul durerii. La pacien ii cu coagulopatii
îmbracă diverse aspecte, în func ie de boala hematologică
anestezia tronculară periferică este contraindicată,
de fond și de complica iile asociate. Medicii stomatologi
deoarece există un risc foarte mare de dezvoltare a unui
și hematologi ar trebui să își canalizeze aten ia și pe
hematom [42]. Anestezia plexală și cea intraligamentară
leziunile orale atunci când întâlnesc un pacient cu
sunt de preferat în cazul în care tratamentul nu se poate
hemopatii, acest fapt ind folositor pentru depistarea
efectua fără anestezie. Dacă este posibil, e indicat să se
precoce și tratarea leziunilor. Medicul dentist trebuie să
folosească anestezic cu vasoconstrictor. Pacien ii care sunt
e familiarizat cu diversele tipuri de hemopatii și
sub tratament intensiv în clinicile de hematologie trebuie
manifestările orale ale acestora, pentru a putea face fa ă
anestezia i complet, iar interven ia se va face intraoperator.
unei sângerări intraoperatorii, pentru a realiza o
Chirurgia orală. Procedurile chirurgicale implică
hemostază e cientă și un tratament postinterven ional
un mare risc de sângerare, iar măsurile suplimentare
corect, iar tratamentul dentar al acestor pacien i ar
pentru realizarea hemostazei trebuie obligatoriu folosite:
trebui adaptat la afec iunea hematologică de fond
sutura plăgii, utilizarea unui hemostatic local, presiune
pentru ecare caz în parte.
la nivelul plăgii, utilizarea de trombină locală, lipici
topic cu brină [43] sau vasoconstrictor; pot folosite
individual sau împreună
[44,45,46]. Tratamentul
Bibliogra e
trebuie amânat până în momentul în care pacientul
prezintă limite normale ale valorilor sanguine, iar
1. Schlosser BJ, Pirigyi M, Mirowski GW. Oral
medicul hematolog își dă acceptul cu privire la
manifestations of hematologic and nutritional diseases.
interven ie [46]. În cazul în care afec iunea hematologică
Otolaryngol Clin North Am 2011;44(1):183-203.
de fond persistă se poate realiza o echilibrare
2. Long RG, Hlousek L, Doyle JL. Oral manifestations of
preinterven ională, folosind tratament substitutiv cu
systemic diseases. Mt Sinai J Med 1998;65(5-6):309-
concentrat trombocitar, plasmă proaspătă, concentra ii
15.
de factori ai coagulării [45].
3. Adeyemo TA, Adeyemo WL, Adediran A, Akinbami
Proceduri parodontale. Sănătatea parodontală are
AJ, Akanmu AS. Orofacial manifestations of
o importan ă critică la pacien i cu afec iuni ale
hematological disorders: anemia and hemostatic
coagulării, la care pot să apară hiperemie gingivală și
disorders. Indian J Dent Res 2011;22(3):454-61.
86
Pop et al
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
GENERAL REVIEW
4.
McFarlane DB, Pinkerton PH, Dagg JH, Goldberg
21.
Embury SH, Matsui NM, Ramanujam S, Mayadas
A. Incidence of iron de ciency, with and without
TN, Noguchi CT, Diwan BA, Mohandas N, Cheung
anaemia, in women in general practice. Br J Haematol
AT. e contribution of endothelial cell P-selectin to the
1967;13(5):790-6.
microvascular ow of mouse sickle erythrocytes in vivo.
5.
Brunner C, Wuillemin WA. Iron de ciency and iron
Blood 2004;104(10):3378-85.
de ciency anemia -symptoms and therapy. er Umsch
22.
Kelleher M, Bishop K, Briggs P. Oral complications
2010;67(5):219-23.
associated with sickle cell anemia: a review and case
6.
Şerban ovaru. Oral Medicine and Pathology. 2nd ed.
report. Oral Surg Oral Med Oral Pathol Oral Radiol
Ed. Quintessence. Bucharest, 2012.
Endod 1996;82(2):225-8.
7.
Delia Popescu Mut. Clinical Hematology. Ed.
23.
Okafor LA, Nonnoo DC, Ojehanon PI, Aikhionbare
Medicală, Bucharest, 2001.
O. Oral and dental complications of sickle cell disease in
8.
Zegarelli DJ. Fungal infections of the oral cavity.
Nigerians. Angiology 1986;37(9):672-5.
Otolaryngol Clin North Am 1993;26(6):1069-89.
24.
Taylor LB, Nowak AJ, Giller RH, Casamassimo PS.
9.
Ho man RM, Ja e PE. Plummer-Vinson syndrome. A
Sickle cell anemia: a review of the dental concerns and a
case report and literature review. Arch Intern Med
retrospective study of dental and bony changes. Spec
1995;155(18):2008-11.
Care Dentist 1995;15(1):38-42.
10.
Demirci F, Savaş MC, Kepkep N, et al. Plummer-
25.
Brown DL, Sebes JI. Sickle cell gnathopathy: radiologic
Vinson syndrome and dilation therapy: a report of two
assessment. Oral Surg Oral Med Oral Pathol
cases. Turk J Gastroenterol 2005;16(4):224-7.
1986;61(6):653-6.
11.
Cannell H. e development of oral and facial signs in
26.
Friedlander AH, Genser L, Swerdlo M. Mental nerve
beta-thalassaemia major. Br Dent J 1988;164(2):50-1
neuropathy: a complication of sickle-cell crisis. Oral
12.
Weatherall JD, Clegg JB. e thalassaemia syndromes.
Surg Oral Med Oral Pathol 1980;49(1):15-7.
3rd ed, Oxford: Blackwell Scienti c, 1981: pp. 132-74.
27.
Gregory G, Olujohungbe A. Mandibular nerve
13.
Van Dis ML, Langlais RP. e thalassemias: oral
neuropathy in sickle cell disease. Local factors. Oral Surg
manifestations and complications. Oral Surg Oral Med
Oral Med Oral Pathol 1994;77(1):66-9.
Oral Pathol 1986;62(2):229-33.
28.
Andrews CH, England MC Jr, Kemp WB. Sickle cell
14.
Graells J, Ojeda RM, Muniesa C, Gonzalez J,
anemia: an etiological factor in pulpal necrosis. J Endod
Saavedra J. Glossitis with linear lesions: an early sign of
1983;9(6):249-52.
vitamin B12 de ciency. J Am Acad Dermatol
29.
Michaelson J, Bhola M. Oral lesions of sickle cell
2009;60(3):498-500.
anemia: case report and review of the literature. J Mich
15.
Field EA, Speechley JA, Rugman FR, Varga E,
Dent Assoc 2004;86(9):32-5.
Tyldesley WR. Oral signs and symptoms in patients
30.
Mendes PH, Fonseca NG, Martelli DR, Bonan PR,
with undiagnosed vitamin B12 de ciency. J Oral Pathol
de Almeida LK, de Melo LA, Martelli H Jr. Orofacial
Med 1995;24(10):468-70.
manifestations in patients with sickle cell anemia.
16.
Greenberg MS. Clinical and histologic changes of the
Quintessence Int 2011;42(8):701-9.
oral mucosa in pernicious anemia. Oral Surg Oral Med
31.
Saint Clair de Velasquez Y, Rivera H. Sickle cell
Oral Pathol 1981;52(1):38-42.
anemia oral manifestations in a Venezuelan population.
17.
Pontes HA, Neto NC, Ferreira KB, Fonseca FP,
Acta Odontol Latinoam 1997;10(2):101-10.
Vallinoto GM, Pontes FS, Pinto Ddos S Jr. Oral
32.
Lengfelder E. Diagnosis and therapy of polycythemia
manifestations of vitamin B12 de ciency: a case report. J
Vera in the era of JAK2. Dtsch Med Wochenschr
Can Dent Assoc 2009;75(7):533-7.
2013;138(7):331-6.
18.
Lu SY, Wu HC. Initial diagnosis of anemia from sore
33.
Carlson ER, Chewning LC. Polycythemia Vera in an
mouth and improved classi cation of anemias by MCV
oral surgical patient. A case report. Oral Surg Oral Med
and RDW in 30 patients. Oral Surg Oral Med Oral
Oral Pathol 1989;67(6):673-5.
Pathol Oral Radiol Endod 2004;98(6):679-85.
34.
Cao M, Olsen RJ, Zu Y. Polycythemia vera: new
19.
Brennan MT, Sankar V, Baccaglini L, et al. Oral
clinicopathologic perspectives. Arch Pathol Lab Med
manifestations in patients with aplastic anemia. Oral
2006;130(8):1126-32.
Surg Oral Med Oral Pathol Oral Radiol Endod
35.
Sambandan T. Review on Oral Manifestations of Blood
2001;92(5):503-8.
Diseases. JIADS 2010;1:41-3.
20.
Sepúlveda E, Brethauer U, Rojas J, Le Fort P. Oral
36.
Malfait F, De Paepe A. Bleeding in the heritable
manifestations of aplastic anemia in children. J Am
connective tissue disorders: mechanisms, diagnosis and
Dent Assoc 2006;137(4):474-8.
treatment. Blood Rev 2009;23(5):191-7.
Oral Manifestations in Patients with Red Blood Series Pathology and Coagulation Disorders. Review of Literature
87
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
37.
Gupta A, Epstein JB, Cabay RJ. Bleeding disorders of
44. Adornato MC, Penna KJ. Hemostatic technique. Using
importance in dental care and related patient
a splint in oral bleeding. N Y State Dent J
management. J Can Dent Assoc 2007;73(1):77-83.
2001;67(6):24-5.
38.
Girolami A, Luzzatto G, Varvarikis C, Pellati D,
45. Piot B, Sigaud-Fiks M, Huet P, Fressinaud E, Trossaërt
Sartori R, Girolami B. Main clinical manifestations of
M, Mercier J. Management of dental extractions in
a bleeding diathesis: an often disregarded aspect of
patients with bleeding disorders. Oral Surg Oral Med
medical and surgical history taking. Haemophilia
Oral Pathol Oral Radiol Endod 2002;93(3):247-50.
2005;11(3):193-202.
46. Rayen R, Hariharan VS, Elavazhagan N, Kamalendran
39.
Toygar HU, Guzeldemir E. Excessive gingival bleeding
N, Varadarajan R. Dental management of hemophiliac
in two patients with Glanzmann thrombasthenia. J
child under general anesthesia. J Indian Soc Pedod Prev
Periodontol 2007;78(6):1154-8.
Dent 2011 ;29(1):74-9.
40.
Kasper DL, Fauci AS, Longo DL, Braunwald E, Hauser
47. Agnihotri R, Bhat KM, Bhat GS, Pandurang P.
SL, Jameson JL. Harrison’s Principles of Internal Medicine.
Periodontal management of a patient with severe aplastic
14th ed. Bucharest, Ed. Teora, 2002, pp 372-9
anemia: a case report. Spec Care Dentist
41.
Gómez-Moreno G, Cutando-Soriano A, Arana C, Scully
2009;29(3):141-4.
C. Hereditary blood coagulation disorders: management
48. Brennan MT, Wynn RL, Miller CS. Aspirin and
and dental treatment. J Dent Res 2005;84(11):978-85.
bleeding in dentistry: an update and recommendations.
42.
Behrman, R. E. et al. Nelson Textbook of Pediatrics.
Oral Surg Oral Med Oral Pathol Oral Radiol Endod
17th ed. China: Saunders, 2004.
2007;04(3):316-23.
43.
Chabbat J, Tellier M, Porte P, Steinbuch M. Properties
49. Terezhalmy GT, Lichtin AE. Antithrombotic,
of a new brin glue stable in liquid state.
romb Res
anticoagulant, and thrombolytic agents. Dent Clin
1994;76(6):525-33.
North Am 1996;40(3):649-64.
88
Pop et al
GENERAL REVIEW
O REVISTĂ A LITERATURII ÎN TRATAMENTUL CANCERULUI DE
PROSTATĂ PRIN DEPRIVARE ANDROGENICĂ INTERMITENTĂ
Mureşanu Horia, Ioiart Ioan
Clinica de Urologie, Universitatea de Vest „Vasile Goldiş” Arad, România
Adresa pentru coresponden ă:
Mureşanu Horia
Spitalul Clinic Jude ean de Urgen ă Arad
E-mail: hmuresanu@gmail.com
Primit: 29.07.2013
Acceptat: 17.08.2013
Med Con October 2013 Vol 8, No 3, 89-92
Rezumat
deprivare androgenică a CaP și dacă există pacien i la
care crește durata de supravie uire prin re-expunerea la
Ghidurile
acceptă
deprivarea
androgenică
androgeni.
intermitentă
(DAI) în tratamentul unor stadii ale
Cuvinte cheie: deprivare androgenică intermitentă,
cancerului de prostată
(CaP). Studiile de fază II au
calitatea vie ii, efecte secundare, supravie uire cu cancer
demonstrat că prin reducerea efectelor secundare în
de prostată
perioadele fără tratament s-a îmbunătă it calitatea vie ii
pacien ilor. Studiile clinice de fază II/III au ajutat la
Introducere
identi carea pacientului ideal pentru DAI
(tumoră
mică, scădere marcată a PSA după ini iere) dar nu au
În
1978, conceptul de privare de androgeni
demonstrat echivalen a sau superioritatea acestui tip de
intermitentă (IAD) a fost sugerată pentru prima oară de
tratament în ceea ce privește progresia bolii spre
dr. Willett Withmore la Memorial Sloan Kettering
rezisten ă la castra ie și supravie uire.
Cancer Centre (MSKCC), care a administrat un astfel
DAI prezintă patru bene cii: îmbunătă irea calită ii
de tratament unui pacient jucător de tenis de competi ie.
vie ii, reducerea efectelor adverse, scăderea costului și
Pacientul tratat cu dietilstilbestrol (DES) pentru CaP
creșterea poten ială a duratei de răspuns a bolii la
metastatic a devenit asimptomatic. Capacitatea de a juca
supresia androgenică. Datele actuale sugerează că nu
tenis în circuitul profesionist a scăzut semni cativ, din
există o scădere a supravie uirii la bolnavii cu CaP a a i
cauza tratamentului hormonal. Dr. Withmore a
pe tratament intermitent antiandrogenic. Durata
întrerupt tratamentul și în perioadele fără tratament
perioadei fără tratament poate prelungită prin folosirea
randamentul jocătorului de tenis s-a îmbunătă it
inhibitorilor de 5α-reductază. Există totuși încă multe
sim itor. Când au reapărut durerile datorate metastazelor
întrebări, cum ar
: durata optimă a tratamentului
osoase, tratamentul a fost reluat și simptomele au
ini ial de deprivare androgenică, parametrul optim
încetat.
pentru reînceperea tratamentului, importan a blocadei
După această experien ă, a fost ini iat primul studiu
androgenice complete
(BAC) versus monoterapie în
pe 20 de pacien i cu cancer de prostată avansat la
perioada de induc ie, impactul inhibitorilor de
MSKCC. Pacien ii au fost trata i în mod similar [1].
5α-reductază în prelungirea perioadei de răspuns la
Studiul s-a desfășurat în perioada pre-PSA și înaintea
Intermittent Androgen Deprivation in Treatment of Prostate Cancer. Review of Literature
89
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
descoperirii agoniștilor LH-RH. Odată cu apari ia
Rezultatele studiului comparativ între deprivarea
progresiei sau a simptomelor clinice tratamentul cu
androgenică continuă și intermitentă efectuat de
DES se relua. Perioada medie de progresie a bolii a fost
Hussain și colab. au fost raportate în 2013 [10]. Au fost
de 8 luni. Activitatea sexuală s-a reluat la
9 din 10
trata i cu analog LHRH și antiandrogen o perioadă de 7
pacien i care au fost impoten i în perioada de tratament.
luni bărba i cu CaP metastatic, nou diagnosticat,
Răspunsul clinic a fost rapid la reluarea tratamentului la
hormonosensibil, cu status de performan ă între 0 și 2,
to i pacien ii.
antigen speci c prostatic (PSA) peste 5 ng/ml. Pacien ii
La începutul anilor
70, Bruchovsky a descris
la care PSA a scăzut sub 4 ng/ml au fost randomiza i pe
moartea celulelor prostatice după îndepărtarea
tratament de deprivare androgenică continuă sau
androgenilor. Acest proces activ denumit
„liză
intermitentă în func ie de statusul de performan ă și
autofagică” este cunoscut astăzi sub numele de apoptoză.
extensia bolii (localizată sau metastazată). Obiectivele
În anii 90 Bruchovsky a lansat ipoteza că re-expunerea
primare au fost să se stabilească dacă tratamentul DAI
celulei stem din CaP la androgen ar reface fenotipul
este inferior sau nu tratamentului continuu în ceea ce
dependent androgenic [2,3].
privește supravie uirea și dacă la cele două grupuri
Înlocuirea in vivo a mai mult de o treime din celulele
calitatea vie ii este diferită începând cu
3 luni de la
stem tumorale cu celule stem androgen independente
randomizare [10,11].
reprezintă o condi ie su cientă pentru instalarea stării
Într-un alt studiu au fost înrola i 3040 pacien i din
de rezisten ă la castra ie. Pentru întârzierea progresiei
care
1535 au fost incluși în studiu:
765 urmând
bolii la starea de independen ă androgenică, s-a emis
tratamentul continuu și 770 pe DAI. Perioada medie de
ipoteza că reexpunerea celulei maligne care
urmărire a fost de 9,8 ani. Durata medie de supravie uire
supravie uiește supresiei androgenice la androgeni ar
a fost de 5,8 ani la tratamentul continuu și 5,1 ani la
readuce celula în starea normală de diferen iere în care
tratamentul intermitent (factor de hazard pentru deces
revine poten ialul apoptoic și apare din nou răspunsul la
cu tratament intermitent de
1,10;
90% interval de
deprivarea androgenică. Teoria aceasta a fost con rmată
con den ă,
0,99-1,23). Pacien ii cu tratamentul
prin inducerea de mai multe ori a apoptozei la modelul
intermitent au avut func ie erectilă și cognitivă mai
tumoral Shionogi prin cicluri repetate de deprivare și re-
bună (p<0,001 și respectiv p=0,003) la 3 luni, dar nu și
expunere la androgeni [4,5]. Această metodă nouă de
după aceea. Nu au fost diferen e semni cative legate de
tratament a fost denumită tratament de supresie
evenimentele adverse serioase datorate tratamentului la
androgenică intermitentă, bolnavilor cu CaP indu-le
cele două grupuri [10,11].
aplicat același protocol de tratament [2-4].
Datele studiilor clinice pot
rezumate astfel: în
Acest concept care permite revenirea nivelului
perioada fără tratament calitatea vie ii bolnavilor revine la
androgenic pentru a prelungi durata dependen ei
nivelul ini ial [9,10,12,13]; PSA nadir scade cu 95% fa ă
androdenice a generat cercetări preclinice și clinice
de nivelul ini ial; durata primului interval fără tratament
substan iale pentru DAI [2-7].
la pacien ii cu PSA<10, 10-20 și >20 ng/ml a fost de 91,
DAI oferă bene cii cvadruple: îmbunătă irea
65 și respectiv 39 de săptămâni; nivelul PSA la început și
calită ii vie ii în perioadele fără tratament prin scăderea
PSA ”nadir” sunt predictori importan i în durata ciclului
morbidită ii datorită reducerii evenimentelor cardio-
fără tratament [14,15,16]. Durata ciclului fără tratament
vasculare și osteoporozei, poten ialul prelungirii duratei
s-a scurtat continuu cu ecare ciclu și semni că progresia
de răspuns la deprivare androgenică a bolii și scăderea
graduală spre independen a androgenică. La ciclul
4
costurilor. Pu ine modi cări terapeutice pot induce
intervalul fără tratament a fost între 23-29 săptămâni,
atâtea bene cii
[7,8]. Întrebarea principală este dacă
indferent de nivelul PSA de început. Nivelul
tratamentul intermitent oferă durată de supravie uire
testosteronului seric a revenit la întreruperea
CaP speci că echivalentă (sau chiar crescută) în raport
tratamentului, dar și această revenire a scăzut cu ecare
cu tratamentul de deprivare androgenică continuă.
ciclu de tratament la
75%, 50%, 40%, și 30% din
Cel mai mare studiu de fază II a fost realizat în
pacien i între ciclurile 1-4 de tratament. Hemoglobina a
Canada pe 110 pacien i cu recidivă biochimică după
scăzut în medie la 11 g/L în timpul tratamentului și a
radioterapie cu inten ie curativă. Rezultatele studiului
revenit la valoarea de început în perioada de oprire a
au fost publicate în trei articole prezentând rezultatele
tratamentului. PSA ini ial,
”nadir” PSA ob inut prin
nale complete [7], rezultate privind calitatea vie ii și
tratament și perioada fără tratament prezic timpul până la
morbiditatea [9] și rezultatele biochimice [8]. Pacien ii
progresia androgen independentă [8-11].
au fost trata i 9 luni cu agonist LHRH și cyproteron
Avantajele tratamentul de deprivare androgenică cu
acetat (CPA) și retrata i când PSA ajungea la 10 ng/ml.
agonist sau antagonist LHRH sunt reversibilitatea,
90
Mureşanu et al
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
GENERAL REVIEW
scăderea evenimentelor adverse tromboembolice și
impoten ei, a urgen ei mic ionale și nocturiei și creșterea
absen a ginecomastiei. În timp apare sindromul de
activită ii zice și a performan ei sexuale.
deprivare androgenică cu bufeuri de căldură, scăderea
libidoului și impoten ă sexuală, oboseală, scăderea for ei
Care sunt pacien ii care bene ciază de
și a masei musculare, scăderea densită ii minerale osoase
tratament intermitent de deprivare
[17], alterarea func iei cognitive și instalarea sindromului
androgenică şi cum trebuie ea folosită?
metabolic (MetS) [13]. MetS este asociat cu creșterea
efectelor secundare cardio-vasculare și scăderea
Majoritatea pacien ilor pot
candida i la
supravie uirii. Osteoporoza și scăderea densită ii osoase
tratamentul intermitent. În următoarele situa ii IAD
prezentă la această gupă de vârstă asociată cu abuzul de
trebuie folosit cu precau ie:
alcool și hipogonadismul indus de tratamentul de
Pacien i cu metastaze osoase care au perspectivă
deprivare androgenică îndelungat, cresc riscul de
limitată de via ă pot bene cia de tratament intermitent
fractură de șold. Acest risc poate evaluat cu ajutorul
numai dacă ajung rapid la un PSA ”nadir” foarte mic
calculatorului FRAXX [18].
după ini ierea tratamentului [11,20,21].
Pacien ii incluși în studiile clinice cu DAI sunt
Pacien ii fără creșterea PSA timp de 3 ani și timp de
diferi i de cei incluși pentru tratamentul continuu.
dedublare a PSA peste un an au șanse de supavie uire la
Randomizarea pentru DAI este condi ionată de
10 ani de 90-97%. Studiul EORTC 300902 sugerează
răspunsul favorabil la
3-9 luni de tratament
ADT întârziată la pacien i cu vârstă <70 ani, PSA >20
antiandrogenic.
ng/ml, sau PSA >50 ng/ml și vârstă >70 de ani cu
Strategia DAI favorizează tratamentul cu antagonist
rezultate similare tratamentului imediat [22,23].
GNRH datorită instalării rapide a supresiei androgenice
Pot bene cia de IAD to i pacien ii care nu au avut
în compara ie cu analogul LHRH.
rezultat bun după tratament local și au CaP cu risc
mediu. Indica ia de tratament este când PSA este în jur
Deprivarea androgenică şi sindromul
de 10 ng/ml.
metabolic
Pacien ii cu metastaze ganglionare au nevoie de
tratament imediat care poate prelungi supravie uirea.
Un studiu observa ional efectuat de Keating și
DAI reprezintă o posibilitate de tratament pentru acești
colab. [19] a eviden iat creșterea riscului de inciden ă a
pacien i [4,24].
bolii pentru diabet zaharat, boală coronariană, infarct
miocardic și moarte subită cardiacă. La in ierea
Concluzie
tratamentului cu agoniști LHRH s-a constatat creșterea
nivelului plasmatic preprandial de insulină.
DAI îmbunătă ește calitatea vie ii, reduce inciden a
Caracteristicile MetS din ADT sunt: grăsimea
efectelor secundare, scade costul și poate crește durata
abdominală este predominant viscerală și nu
de dependen ă androgenică a bolii. Toate eviden ele
subcutanată, greutatea pacientului și indicele de masă
arată că nu există o scădere a supravie uirii cu CaP prin
corporală IMC au crescut între
2,4-9% și HDL
tratamentul intermitent.
colesterolul nu este scăzut.
Efectul ADT asupra efectelor secundare şi
Bibliogra e
calită ii vie ii
1. Klotz LH, Herr HW, Morse MJ, Whitmore WF Jr.
Îmbunătă irea calită ii vie ii prin tratament
Intermittent endocrine therapy for advanced prostate
hormonal intermitent se datorează
creșterii
cancer. Cancer 1986; 58(11):2546-50.
testosteronului în perioadele fără tratament. Bruchovsky
2. Bruchovsky N, Rennie PS, Coldman AJ, Goldenberg
și colab.
[7,9] au raportat că inciden a efectelor
SL, To M, Lawson D. E ects of androgen withdrawal
secundare este mai mare în perioadele de tratament.
on the stem cell composition of the Shionogi carcinoma.
Oboseala, dispeea și hematuria sunt simptomele cele
Cancer Res 1990; 50(8):2275-82.
mai frecvente
(50,5%,
24,8% și
17,4%). Infarctul
3. Bruchovsky N, Craven S. Prostatic involution: E ect on
miocardic (7,3%) accidentul vascular cerebral (6,4%) și
androgen receptors and intracellular androgen transport.
tromboza venoasă profundă (5,5%) au fost de asemenea
Biochem Biophys Res Comm 1975; 62(4):837-43.
frecvente. În perioadele fără tratament s-a îmbunătă it
4. Akakura K, Bruchovsky N, Coldenberg SL, Rennie
calitatea vie ii prin scăderea bufeurilor de căldură, a
PS, Buckley AR, Sullivan LD. E ects of intermittent
Intermittent Androgen Deprivation in Treatment of Prostate Cancer. Review of Literature
91
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
androgen suppression on androgen-dependent tumors.
14.
Goldenberg SL, Bruchovsky N, Gleave ME, Sullivan
Apoptosis and serum prostate-speci c antigen. Cancer
LD, Akakura K. Intermittent androgen suppression in
1993; 71(9):2782-90.
the treatment of prostate cancer: a preliminary report.
5.
Gleave ME, Hsieh JT, Wu HC, von Eschenbach AC,
Urology. 1995; 45(5):839-44; discussion 844-5.
Chung LW. Serum prostate speci c antigen levels in
15.
Oliver RT, Williams G, Paris AM, Blandy JP.
mice bearing human prostate LNCaP tumors are
Intermittent androgen deprivation after PSA- complete
determined by tumor volume and endocrine and growth
response as a strategy to reduce induction of hormone-
factors. Cancer Res 1992; 52(6):1598-605.
resistant prostate cancer. Urology 1997; 49(1):79-82.
6.
Mottet N, Lucas C, Sene E, Avances C, Maubach L,
16.
De la Taille A, Zerbib M, Conquy S, et al. Intermittent
Wol JM. Intermittent androgen castration: a biological
androgen suppression in patients with prostate cancer.
reality during intermittent treatment in metastatic
BJU Int 2003; 91(1):18-22.
prostate cancer? Urol Int 2005; 75(3):204-8.
17.
Higano C, Shields A, Wood N, Brown J, Tangen C.
7.
Bruchovsky N, Klotz L, Crook J, Phillips N,
Bone mineral density in patients with prostate cancer
Abersbach J, Goldenberg SL. Quality of life, morbidity,
without bone metastases treated with intermittent
and mortality results of a prospective phase II study of
androgen suppression. Urology 2004; 64(6):1182-6.
intermittent androgen suppression for men with evidence
18.
of prostate-speci c antigen relapse after radiation therapy
19.
Keating NL, O’Malley AJ, Smith MR. Diabetes and
for locally advanced prostate cancer. Clin Genitourin
cardiovascular disease during androgen deprivation
Cancer. 2008; 6(1):46-52.
therapy for prostate cancer. J Clin Oncol
2006;
8.
Bruchovsky N, Klotz L, Crook J, Goldenberg SL.
24(27):4448-56.
Locally advanced prostate cancer-biochemical results
20.
Sato N, Akakura K, Isaka S, e tal. Intermittent
from a prospective phase II study of intermittent
androgen suppression for locally advanced and metastatic
androgen suppression for men with evidence of prostate
prostate cancer: preliminary report of a prospective
speci c antigen recurrence after radiotherapy. Cancer
multicenter study. Urology 2004; 64(2):341-5.
2007;109(5):858-67.
21.
Calais Da Silva F.Goncalbes F, Santos A, et al. Phase 3
9.
Bruchovsky N, Klotz L, Crook J, et al. Final results of
study of intermittent monotherapy versus combined
the Canadian prospective phase II trial of intermittent
androgen deprivation. J Urol 2006; 175(4):315 (abs.
androgen suppression for men in biochemical recurrence
974).
after radiotherapy for locally ad-vanced prostate cancer:
22.
Albrecht W, Collette L, Fava C, et al. Intermittent
clinical parameters. Cancer 2006; 107 (2):389-95.
maximal androgen blockade in patients with metastatic
10.
Hussain M, Tangen CM, Berry DL et al. Intermittent
prostate cancer: an EORTC feasibility study. Eur Urol
versus Con-tinuous Androgen Deprivation in Prostate
2003; 44(5):505-11.
Cancer. N Engl J Med 2013; 368 (14):1314-25.
23.
Studer UE, Whelan P, Albrecht W, et al. Immediate or
11.
Hussain M, Tangen CM, Higano C, et al. Absolute
deferred androgen deprivation for patients with prostate
prostate-speci c antigen value after androgen deprivation is
cancer not suitable for local treatment with curative
a strong independent predictor of survival in new metastatic
intent: European Organization for Research and
prostate cancer: data from Southwest Oncology Group Trial
Treatment of Cancer (EORTC) Trial 30891. J Clin
9346 (INT-0162). J Clin Oncol 2006; 24(24):3984-90.
Oncol 2006; 24(12):1868-76.
12.
Higano CS, Ellis W, Russell K, Lange PH. Intermittent
24.
Messing EM, Manola J, Yao J et al. Immediate versus
androgen suppression with leuprolide and utamide for
deferred androgen deprivation treatment in patients
prostate cancer: a pilot study. Urology 1996; 48(5):800-4.
with node-positive prostate cancer after radical
13.
Tunn U. Can intermittent hormone therapy ful ll its
prostatectomy and pelvic lymphadenectomy. Lancet
promise? Eur Urol Suppl 2008; 7:752-7.
Oncol 2006; 7(6):472-9.
92
Mureşanu et al
GENERAL REVIEW
ABORDAREA TERAPEUTICĂ A LEUCOPLAZIEI ORALE. TRECERE ÎN
REVISTĂ A DATELOR DIN LITERATURĂ
Părlătescu Ioanina1, ovaru Şerban1, Mihai Lelia2
1Catedra de Patologie Orală, Facultatea de Medicină Dentară, Universitatea de Medicină şi Farmacie „Carol Davila”,
Bucureşti, 2Catedra de Patologie Orală, Universitatea de Medicină Dentară, Universitatea „Titu Maiorescu”, Bucureşti
Adresa pentru coresponden ă:
Dr. Ioanina Părlătescu
Facultatea de Medicină Dentară, Catedra de Patologie Orală
Str. Eforiei, nr.4-6, Bucureşti
E-mail: ioaninap@yahoo.com
Received: 08.07.2013
Accepted: 10.08.2013
Med Con October 2013 Vol 8, No 3, 93-97
Rezumat
histologic în orice altă boală și nu este asociată cu un
agent cauzal zic sau chimic, cu excep ia fumatului [2].
Leucoplazia este cea mai frecventă leziune orală cu
Leucoplazia este un termen clinic și nu are conota ii
poten ial de malignizare. Diagnosticul se stabilește pe
histologice speci ce. La examenul anatomo-patologic
criterii clinice și histologice. Scopul tratamentului
leucoplazia prezintă hiperkeratoză, atro e, acantoză și
leucoplaziei orale este evitarea transformării maligne.
diferite grade de displazie epitelială. Nu are o evolu ie
Astfel, există mai multe op iuni terapeutice. Acestea
predictibilă, dar are o tendin ă de transformare malignă.
variază de la îndepărtarea chirurgicală în totalitate a
Displazia epitelială nu are un aspect clinic speci c, poate
leziunii, până la o atitudine de expectativă („wait and
să apară în orice leziune albă clinic aparent benignă.
see”). La nivel mondial nu există un consens legat de cea
Există două forme clinice de leucoplazie: omogenă și
mai bună posibilitate de tratament. Decizia depinde de
neomogenă. Tipul omogen are o suprafa ă plană, sub ire
specialist și este adaptată ecărui pacient în func ie de
și netedă (Figura 1).
aspectul clinic și trăsăturile histologice.
Forma neomogenă poate pătată (zone albe cu
Cuvinte cheie: leucoplazie, displazie, tratament
zone roșii, dar predominant albe), verucoasă (suprafa ă
reliefată) (Figura 2) sau nodular (cu mici noduli albi pe
Introducere
suprafa ă).
Leucoplazia poate unică leziune, sau pot să apară
Leucoplazia orală este de nită ca o pată albă mai
mai multe zone având un aspect multifocal (Figura 3),
mare de 5 mm2, care nu se îndepărtează prin ștergere și
ceea ce se consideră un semn de agresivitate al leziunii.
are o etiologie necunoscută sau tabagică. În
1978
Leucoplazia verucoasă proliferativă este o formă
Centrul de Colaborare pentru Leziuni
Orale
agresivă care progresează în timp. Debutează ca un
Precanceroase coordonat de OMS a de nit leucoplazia
placard omogen, apoi crește și are tendin a de a deveni
orală ca o pată albă care are risc de transformare malignă
multifocală [3]. Evoluează cu multe focare de leucoplazie
[1]. Ulterior, în 2007, Grupul de Specialiști de Medicină
care sunt exo tice și con uează. Acest tip de leucoplazie
Orală organizat cu scopul de a integra progresele în
este rezistentă la orice tratament, are o rată mare de
biologia precancerului oral, a rede nit leucoplazia ca o
recidivă și de obicei evoluează în carcinom verucos sau
pată sau placă albă care nu poate încadrată clinic sau
spinocelular în procente cuprinse între 40-100% [4].
Treatment Approach of Oral Leukoplakia. Review of Literature
93
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
raportează că pacien ii cu leucoplazie con rmată
histologic nu prezintă malignizare în procent de 86,6%
la
3 ani și
82,5% la
5 ani
[2]. Pe perioada de
dispensarizare de 5 ani transformarea malignă raportată
este de 41% pentru leziunile displazice și 9% pentru
cele fără displazie [2].
În ciuda progreselor din biologia celulară, nu există
markeri de certitudine pentru a anticipa transformarea
malignă a leucoplaziei orale [6]. Markerii Ki-67(Mib-1)
și p53 sunt considera i predictivi pentru transformarea
Figura 1. Leucoplazie omogenă pe mucoasa
malignă, dar nu sunt în general adopta i în practica
retrocomisurală, la un pacient fumător
clinică [6].
Op iunile terapeutice pentru leucoplazia orală sunt
chirurgicale și nechirurgicale, dar nu există un consens
despre care este mai bună. Decizia este adaptată ecărui
pacient în func ie de aspectul clinic - dimensiune și
localizare și în func ie de caracterele histologice.
Tratamentul chirurgical
Majoritatea specialiștilor în medicină orală
consideră că tratamentul chirurgical este prima op iune
în abordarea leucoplaziei orale [7], dar nu s-a demonstrat
Figura 2. Leucoplazie verucoasă pe gingie
că îndepărtarea totală a leziunii va exclude transformarea
malignă. Un studiu randomizat care a evaluat
tratamentul chirurgical al leucoplaziei nu a indicat
e cien a tratamentului chirurgical pentru reducerea
malignizării [8], dar aceasta nu înseamnă că îndepărtarea
chirurgicală ar trebui abandonată, mai ales pentru că
permite diagnosticul histologic
[7]. Tratamentul
chirurgical este o metodă de diagnostic care se folosește
și în evolu ia leucoplaziei orale ca parte integrantă a
dispensarizării active.
Se utilizează mai multe tehnici chirurgicale: laser,
chirurgia clasică cu bisturiul, electrocoagularea și
Figura 3. Leucoplazie multifocală la nivelul planşeului
criochirurgia.
bucal: zone reduse omogene şi o arie uşor proliferativă
Chirurgia laser este considerată cea mai abilă
tehnică în ultimii 30 de ani [7]. Are două bene cii
importante: efectul hemostatic și reducerea cicatricilor
De obicei termenul de leucoplazie este folosit ca un
apărute postoperator. Poate utilizată pentru leziuni
diagnostic provizoriu când la examinarea clinică se
extinse. De asemenea, disconfortul postoperator este
observă o leziune albă a mucoasei orale care nu poate
redus, dar dezavantajul major al acestei tehnici este
încadrată în nicio altă afec iune. Biopsia este necesară
lipsa diagnosticului histopatologic. Mai mult,
pentru stabilirea diagnosticului. Diagnosticul de nitiv
comparându-se diferite tipuri de laser: cu dioxid de
de leucoplazie orală este stabilit ulterior, când s-au
carbon, cu neodymium: yttrium aluminum garnet
eliminat orice factori etiologici (cu excep ia fumatului)
(NdYAG) și cel cu potasiu-titan-fosfat
(KTP), s-au
și examenul histopatologic nu a fost speci c pentru altă
găsit diferen e ale ratelor de recuren ă (34,2%, 28,9%
afec iune [2].
și 17%) [7,9].
Displazia epitelială este considerată cel mai
Chirurgia conven ională se referă la excizia
important indicator pentru transformarea malignă.
clasică a leziunii cu bisturiul. Această tehnică este
Leucoplazia orală displazică are un risc de malignizare
urmată de vindecare secundară în cazul leziunilor
de 5 ori mai mare decât cea fără displazie
[5]. Se
reduse, sau de traspozi ia unor grefe de mucoasă orală,
94
Părlătescu et al
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
GENERAL REVIEW
sau chiar grefe tegumentare în cazul unor defecte
antioxidant [14]. Un studiu [18] care a evaluat licopenul
mucozale extinse.
în tratamentul leucoplaziei orale pentru o perioadă de
Electrocoagularea poate folosită singură sau ca
trei luni, folosind dozele de 4mg/zi și 8mg/zi, raportează
adjuvant în tehnica chirurgicală clasică. Aceasta induce
remiterea clinică în propor ie de 25% și respectiv de
distrugerea
termincă
inclusiv
a
esuturilor
55% [14].
înconjurătoare, producând dureri post-operatorii, edem
Acidul retinoic (Vitamina A)
și cicatrici retractile.
Acidul retinoic include toate componentele
Crioterapia este o metodă care permite distrugerea
naturale și sintetice care au activitate similară cu
esutului lezional prin înghe are in situ. Se folosește în
vitamina A [14]. Această posibilitate terapeutică nu este
sistem „deschis” sau „închis” [10]. Sistemul deschis al
larg
acceptată datorită
efectelor
adverse
-
crioterapiei presupune aplicarea directă a unui criogen
hipervitaminoză, toxicitate, efecte teratogene și alterări
pe leziune folosind un tampon de bumbac [11], sau un
ale diverselor organe [14].
spray [10]. Sistemul închis are un grad mai mare de
Totuși folosirea locală a acidului 13-cis retinoic s-a
control folosind un aparat complex [10,11]. Principale
demonstrat a e cientă în remiterea leucoplaziei orale
avantaje ale crioterapiei sunt înterven ia nesângerândă,
[15,19], dar există limitări, deoarece recidivele apar la
riscul redus de infec ie postoperator și lipsa cicatricilor
scurt timp după întreruperea tratamentului [14,15].
[12]. Unele studii au indicat crioterapia ca alternativă în
Folosirea pe cale generală a dozelor de 300.000 UI
tratamentul leucoplaziei orale
[12]. În timpul
de acid retinoic a fost urmată de remiterea clinică a
crioterapiei se formează cristale de ghea ă în lichidele
leziunilor în 50% din cazuri [14].
extracelulare și intracelulare ceea ce duce la deshidratarea
Într-un studiu recent privind leucoplazia
celulei, creșterea concentra iei de electroli i toxici
proliferativ-verucoasă s-a demonstrat că rezultatele
intracelulari, inhibi ie enzimatică și distrugerea
folosirii locale a retinoizilor
(sub forma unui gel de
proteinelor. Aceste mecanisme asociate cu șocul termic
tretinoin sau izotretinoin 0,05-0,1%) sunt în general
induc vacuolizarea celulelor, expansiunea, urmată de
similare cu cele ale retinoizilor sistemici [20].
ruperea acestora
[12,13]. Modi cările vasculare sunt
Bleomicina
urmate de necroză ischemică a esutului tratat și de
Bleomicina, un antibiotic citotoxic, este un
răspuns imunologic care va produce distrugerea
tratament alternativ al leucoplaziei orale. Este folosit în
esutului prin mecanisme citotoxice [13].
tratamentul carcinoamelor spinocelulare ale capului și
regiunii gâtului, esofagului și pentru cele tegumentare
Tratamentul medicamentos
[14]. Utilizarea topică a bleomicinei 1% o dată pe zi a
dus la remiterea leucoplaziei în 14 zile [21], dar datorită
Carotenoizii
efectele sale adverse (reac ii cutaneo-mucoase precum
Betacarotenul este un precursor al vitaminei A.
stomatită, alopecie, eritem pruriginos și vezicule
Carotenodermia
(starea în care tegumentul devine
tegumentare) bleomicina nu este frecvent folosită în
galben) este efectul aportului excesiv de betacaroten și
practică [14].
dispare în câteva săptamâni de la reducerea consumului
Terapia fotodinamică
[14]. Func ia betacarotenului se realizează prin legare de
Terapia fotodinamică este o metodă noninvazivă
oxigen, astfel apar celule instabile reactive care vor
pentru tratamentul tumorilor din regiunea capului și
reduce efectul distrugător al radicalilor liberi [15].
gâtului [22]. Se bazează pe reac ia fotochimică ini iată
Unele studii indică că remiterea clinică a leziunilor
de activarea cu lumină a unor substan e fotosensibile,
leucoplazice orale variază între 4% până la 54%, cu doze
reac ie care induce distrugerea celulară. Aceasta necesită
variabile între 20 - 90mg/zi de betacaroten pe perioade
prezen a simultană a substan ei fotosensibile, a
cuprinse între 3 și 12 luni [14,16].
oxigenului și a luminii vizibile. Este o reac ie non-
Licopenul
termică
[23].
Substan a fotosensibilă
(acidul
Licopenul este un carotenoid lipsit de ac iunea
aminolevulinic - ALA) este administrată sistemic prin
provitaminei A [14]. Este un pigment roșu liposolubil
injectare intravenoasă, sau poate aplicată topic. După
care se găsește în unele fructe și legume. Există o rela ie
un scurt timp, aceasta se localizează în esutul intă și
pozitivă între consumul de licopen și reducerea riscului
este activată prin expunere la lumină vizibilă cu putere
de dezvoltare a bolilor degenerative cauzate de radicalii
mică cu o lungime de undă speci că substan ei
liberi, cum ar cancerul și bolile cardiovasculare [17].
fotosensibile. Rezultatul va
apari ia unor specii de
Licopenul se leagă chimic de substan e care reac ionează
oxigen reactiv care vor produce modi cări la nivelul
cu oxigenul, astfel ind cel mai e cient agent biologic
componentelor celulare (proteinele structurale, enzime,
Treatment Approach of Oral Leukoplakia. Review of Literature
95
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
ADN și fosfolipide). Structurile importante ale
Bibliogra e
organelor nu sunt afectate, iar rezultatele func ionale și
cosmetice sunt bune [23]. De-a lungul timpului s-au
1.
Kramer IR, Lucas RB, Pindborg JJ, Sobin LH.
folosit mai multe substan e fotosensibile: (1) fotofrin a
De nition of leukoplakia and related lesions: an aid to
fost aprobat în mai multe ări pentru tratamentul
studies on oral precancer. Oral Surg Oral Med Oral
cancerului esofagian și pulmonar;
(2)
acidul
Pathol 1978;46(4):518-39.
5-aminolevulinic este aprobat și folosit pentru
2.
Warnakulasuriya S, Johnson NW, van der Waal I.
tratamentul cancerul tegumentar; (3) vertepor n pentru
Nomenclature and classi cation of potentially malignant
tratamentul maculelor degenerative;
(4) foscan este
disorders of the oral mucosa. J Oral Pathol Med
unica substan ă fosensibilă care este aprobată pentru
2007;36(10):575-80.
tratamentul carcinoamelor spinocelulare de la nivelul
3.
Cerero-Lapiedra R, Balade-Martinez D, Moreno-
capului și gâtului în Europa în anul 2001 [23]. Există
Lopez LA, Esparza-Gomez G, Bagan JV. Proliferative
câteva studii
[14,24,25] care au raportat folosirea
verrucous leukoplakia: a proposal for diagnostic criteria.
acidului
5-aminolevulinic în tratamentul leucoplaziei
Med Oral Patol Oral Cir Bucal 2010;15(6):e839-45.
orale cu rezultate bune și fără recidivă pe o perioadă de 9
4.
Bagan JV, Jimenez-Soriano Y, Diaz-Fernandez JM,et
luni de dispensarizare.
al. Malignant transformation of proliferative verrucous
Eliminarea factorilor de risc
leukoplakia to oral squamous cell carcinoma: a series of
Oprirea fumatului este o prioritate în leucoplaziile
55 cases. Oral Oncol 2011;47(8):732-5.
tabagice, dar nu există studii pe grupe de fumători care
5.
van der Waal I, Schepman KP, van der Meij EH,
să evalueze transformarea malignă. În mod sigur
Smeele LE. Oral leukoplakia: a clinicopathological
încurajarea pacientul de a opri fumatul va reduce
review. Oral Oncol 1997;33(5):291-301.
inciden a leucoplaziei și va face ca un număr mare de
6.
Smith J, Rattay T, McConkey C, Helliwell T,
leziuni să remită [5,26].
Mehanna H. Biomarkers in dysplasia of the oral cavity:
Atitudinea de urmărire (wait and see)
a systematic review. Oral Oncol 2009;45(8):647-53.
O posibilitate de tratament este urmărirea clinică și
7.
Lodi G, Porter S. Management of potentially malignant
histologică a leziunii. Aceasta presupune controale
disorders: evidence and critique. J Oral Pathol Med
frecvente și biopsii dacă leziunile devin suspecte, dar
2008;37(2):63-9.
fără o altă interven ie activă. Această metodă urmărește
8.
Schwarz F, Maraki D, Yalcinkaya S, Bieling K,
un diagnostic rapid al unei eventuale transformări
Bocking A, Becker J. Cytologic and DNA-cytometric
maligne, oferind astfel cel mai bun prognostic [7]. În
follow-up of oral leukoplakia after CO2 - and Er:YAG-
prezent există studii care sugerează că evolu ia naturală a
laser assisted ablation: a pilot study. Lasers Surg Med
leucoplaziei orale poate independentă de tratament și
2005;37(1):29-36.
anumite leziuni sunt destinate să se malignizeze
9.
Ishii J, Fujita K, Munemoto S, Komori T. Management
indiferent de terapia aplicată [7].
of oral leukoplakia by laser surgery: relation between
recurrence and malignant transformation and
Concluzii
clinicopathological features. J Clin Laser Med Surg
2004;22(1):27-33.
Cunoașterea displaziei epiteliale este obligatorie
10.
Leopard PJ. Cryosurgery, and its application to oral
pentru alegerea celei mai bune variante de tratament.
surgery. Br J Oral Surg 1975;13(2):128-52.
Prezen a displaziei moderate sau severe impune
11.
Yeh CJ. Simple cryosurgical treatment for oral lesions.
necesitatea tratamentului chirurgical
[7]. Displazia
Int J Oral Maxillofac Surg 2000;29(3):212-6.
ușoară sau absen a displaziei nu necesită obligatoriu
12.
Yu CH, Chen HM, Chang CC, Hung HY, Hsiao
extirparea leziunii. În aceste situa ii decizia se ia inând
CK, Chiang CP. Cotton-swab cryotherapy for oral
cont de factorii clinici
- localizare, dimensiune și
leukoplakia. Head Neck 2009;31(8):983-8.
angajamentul pacientului legat de renun area la fumat
13.
Reade PC. Cryosurgery in clinical dental practice. Int
[27].
Dent J 1979;29(1):1-11.
Mul umiri: Această lucrare este efectuată în cadrul
14.
Ribeiro AS, Salles PR, da Silva TA, Mesquita RA. A
Programului Opera ional Sectorial pentru Dezvoltarea
review of the nonsurgical treatment of oral leukoplakia. Int
Resurselor Umane (POSDRU) 2007-2013, nan at din
J Dent 2010;2010:186018, doi: 10.1155/2010/186018.
Fondul Social European și Guvernul României prin
15.
Kaugars GE, Silverman S Jr., Lovas JG, ompson
contractul nr. POSDRU/107/1.5/S/82839
JS, Brandt RB, Singh VN. Use of antioxidant
supplements in the treatment of human oral leukoplakia.
96
Părlătescu et al
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
GENERAL REVIEW
Oral Surg Oral Med Oral Pathol Oral Radiol Endod
22.
Kubler A, Niziol C, Sidhu M, Dunne A, Werner JA.
1996;81(1):5-14.
Analysis of cost e ectiveness of photodynamic therapy
16.
Sankaranarayanan R, Mathew B, Varghese C, et al.
with Foscan
(Foscan-PDT) in comparison with
Chemoprevention of oral leukoplakia with vitamin A and
palliative chemotherapy in patients with advanced head-
beta carotene: an assessment. Oral Oncol 1997;33(4):231-6.
neck tumors in Germany. Laryngorhinootologie
17.
Riccioni G, Mancini B, Di Ilio E, Bucciarelli T,
2005;84(10):725-32.
D’Orazio N. Protective e ect of lycopene in
23.
Kubler AC. Photodynamic therapy. Medical Laser
cardiovascular disease. Eur Rev Med Pharmacol Sci
Application 2005;20(1):37-45.
2008;12(3):183-90.
24.
Zakrzewska JM, Lopes V, Speight P, Hopper C.
18.
Nagao T, Ikeda N, Warnakulasuriya S, et al. Serum
Proliferative verrucous leukoplakia: a report of ten cases.
antioxidant micronutrients and the risk of oral leukoplakia
Oral Surg Oral Med Oral Pathol Oral Radiol Endod
among Japanese. Oral Oncol 2000;36(5):466-70.
1996;82(4):396-401.
19.
Kaugars GE, Silverman S, Jr., Lovas JG, et al. A
25.
Chen HM, Yu CH, Tu PC, Yeh CY, Tsai T, Chiang
clinical trial of antioxidant supplements in the treatment
CP. Successful treatment of oral verrucous hyperplasia
of oral leukoplakia. Oral Surg Oral Med Oral Pathol
and oral leukoplakia with topical
5-aminolevulinic
1994;78(4):462-8.
acid-mediated photodynamic therapy. Lasers Surg Med
20.
Poveda-Roda R, Bagan JV, Jimenez-Soriano Y, Diaz-
2005;37(2):114-22.
Fernandez JM, Gavalda-Esteve C. Retinoids and
26.
Roed-Petersen B. E ect on oral leukoplakia of reducing
proliferative verrucous leukoplakia (PVL). A preliminary
or ceasing tobacco smoking. Acta Derm Venereol
study. Med Oral Patol Oral Cir Bucal 2010;15(1):e3-
1982;62(2):164-7.
9.
27.
Warnakulasuriya S, Reibel J, Bouquot J, Dabelsteen
21.
Epstein JB, Gorsky M, Wong FL, Millner A. Topical
E. Oral epithelial dysplasia classi cation systems:
bleomycin for the treatment of dysplastic oral leukoplakia.
predictive value, utility, weaknesses and scope for
Cancer 1998;83(4):629-34.
improvement. J Oral Pathol Med 2008;37(3):127-33.
Treatment Approach of Oral Leukoplakia. Review of Literature
97
Scrisoare de informare
Având în vedere activită ile revistei Medical Connections/Conexiuni Medicale privind recenzia şi
editarea articolului mai jos numit, efective odată cu acceptarea acestuia de către Medical Connections/
Conexiuni Medicale (la care se face referin ă în continuare ca Med Con), autorul (autorii) atribuie prin
prezenta către Med Con, reprezentan ilor legali, succesorilor şi mandata ilor ei, toate drepturile de
publicare şi ecare şi oricare drept privind articolul în întreaga lume, în orice limbă şi în orice mediu, chiar
şi ca lucrare audiovizuală, colectivă, compila ie, lucrare derivată, lucrare în comun, operă literară,
înregistrare audio, în imagini, gra că, operă de artă vizuală, program de calculator, sau orice alt mediu
existent acum sau care va deveni ulterior uzual, inclusiv drepturile de autor şi dreptul de a înregistra
dreptul de autor, precum şi dreptul de a asigura orice reînnoire, reeditare şi extinderea unor astfel de
drepturi de autor în România sau în orice ară străină. Autorul (Autorii) pot solicita permisiunea de a
reutiliza manuscrisul sau por iuni din acesta. Astfel de cereri trebuie să e în scris, iar permisiunea dată de
Med Con nu va refuzată în mod nejusti cat. Autorul (Autorii) desemnează Med Con ca reprezentant
legal al acestuia (acestora) pentru a întocmi orice documente pe care Med Con le consideră necesare
pentru a înregistra oricare dintre aceste garan ii la o ciul de copyright românesc sau din alte ări. Autorul
(Autorii) garantează de asemenea către Med Con că articolul este lucrarea originală a autorului (autorilor),
cu excep ia materialelor provenite din domeniul public, iar fragmente din alte lucrări pot incluse doar cu
acordul prealabil scris al titularilor drepturilor de autor, că articolul nu a fost publicat anterior, nu a fost
prezentat, sau acceptat pentru publicare în altă parte, că autorul (autorii) nu au nicio rela ie, nanciară sau
de altă natură, cu orice producător sau distribuitor de produse evaluate în această lucrare, sau, dimpotrivă,
orice astfel de rela ie a fost dezvăluită într-o notă de subsol la articol, sau că această cerin ă este irelevantă
pentru lucrare.
Titlul manuscrisului: ________________________________________________________
Nume:
Semnătură/Data:
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Vă rugăm trimite i pe fax +40-261-710456 această scrisoare la sediul editorului Med Con.
CASE PRESENTATION
AMPUTAȚIILE DE COAPSĂ LA PACIENȚII DIABETICI CU OSTEOSINTEZĂ
FEMURALĂ ÎN ANTECEDENTE. PREZENTARE DE CAZ
Aiordăchioaie Gigi Adrian1, Pop Alexandru2, Dumnici Alexandru1, Fruja Dan2, Papiu Hora iu Sabin1,
Korodi Andrei1, Hărăguş Horia3
1Departamentul de Chirurgie, Universitatea de Vest „Vasile Goldiş” Arad, România, 2Departamentul de Ortopedie şi
Traumatologie, Universitatea de Vest „Vasile Goldiş” Arad, România, 3Universitatea de Medicină şi Farmacie „Victor
Babeş” Timişoara, România
Adresa pentru coresponden ă:
Dr. Gigi Adrian Aiordăchioae
Departamentul de Chirurgie, Universitatea de Vest „Vasile Goldiş” Arad, România
Str. Henri Coanda nr. 31, Arad, 310429, România
Telefon: 0040722166895
E-mail: gigi_aiordachioaie@yahoo.com
Primit: 27.06.2013
Acceptat: 12.08.2013
Med Con October 2013 Vol 8, No 3, 99-103
cele două cazuri, în celălalt ind for a i să facem incizia
Rezumat
în treimea medie datorită progresiei înalte a procesului
infec ios, consecin ă a prezentării tardive la medic a
Amputa ia de coapsă la pacientul diabetic reprezintă,
bolnavului. În ambele situa ii di cultatea interven iei a
adesea o solu ie nedorită dar salvatoare pentru via a
fost mărită de prezen a tijelor metalice Ender, a căror
acestuia, în situa ia în care procesul gangrenos are o
extragere s-a realizat mai greu în cazul sec ionării
ascensiune rapidă. Această interven ie mutilantă trebuie
femurului în treimea medie.
rezervată numai pentru cazurile în care au fost epuizate
Amputa iile de coapsă la pacien ii diabetici cu
celelalte mijloace terapeutice, respectiv chirurgia vasculară
osteosinteză femurală ridică probleme particulare de
și amputa iile de nivele inferioare. Prezen a în femur a
diagnostic și tratament. Anamneza atentă și examenul
tijelor de osteosinteză consecutive unor fracturi vechi
radiologic eviden iază tijele centromedulare. În aceste
ridică probleme suplimentare legate îndeosebi de extrac ia
situa ii nivelul de elec ie al sec ionării copasei este în
acestora. Subliniem faptul că lăsarea unui bont lung
treimea distală, fapt care asigură atât extrac ia facilă a
permite protezarea în condi ii destul de bune, permi ând
tijelor cât și prezervarea unui bont cât mai lung, cu
reinser ia socială a pacientului și atenuarea semni cativă a
ușurarea semni cativă a protezării ulterioare.
handicapului major postoperator al acestuia.
Cuvinte cheie: diabet zaharat, infec ie, amputa ie
Sunt discutate 2 cazuri de pacien i diabetici cu tije
de coapsă, osteosinteză femurală
femurale Ender care au necesitat amputa ia de coapsă,
unul în treimea distală, celălalt în cea medie.
Introducere
Particularitatea cazurilor este dată de prezen a acestor
tije centromedulare care îngreunează actul operator.
Macroangiopatia obliterantă a membrelor inferioare
Amputa iile de coapsă se fac, de regulă, cât mai
reprezintă o complica ie frecventă a diabetului zaharat,
distal cu putin ă pentru a prezerva un bont cât mai lung.
adesea la pacien i vârstnici cu o patologie asociată
Acest deziderat a putut respectat doar în unul dintre
încărcată, având o evolu ie dramatică, ce ridică serioase
Thigh Amputations in Diabetic Patients with a History of Femoral Osteosynthesis. Case Report
99
CASE PRESENTATION
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
di cultă i terapeutice [1,2]. În situ ia în care chirurgia
Din antecedente remarcăm diabetul zaharat tip II
vasculară de dezobstruc ie și/sau reconstruc ie este
diagnosticat în urmă cu 5 ani, în tratament cu metformin
depășită, când apare gangrena diabetică, devine necesară
de 1000 mg, 2/zi; HTA stadiu II în tratament cu reserpină
amputa ia diferitelor segmente ale membrului inferior.
0,1 mg și dihidralazină 10 mg, 2 tablete/zi și propranolol
Un prim obiectiv al acestei chirurgii ablative este
40 mg (1/2 tabletă/zi), cardiopatie ischemică cronică. În
reprezentat de îndepărtarea segmentului neviabil gangrenos
urmă cu 10 ani pacientul a suferit o fractură de epi za
și stoparea procesului septic ascendent, cu salvarea vie ii
distală femur stâng, care a fost tratată chirurgical prin
bolnavului. Un al doilea scop, de asemenea esen ial, este
osteosinteză centromedulara cu tije Ender.
ob inerea unui bont de amputa ie sănătos și cât mai lung cu
Analizele de laborator au relevat un sindrom
putin ă, care ulterior să poată sus ine o proteză, astfel încât
in amator important cu leucocitoză
21800/mm³,
să permită o reintegrare socială cât mai bună a bolnavului.
hemoglobina
-
9,8 g/dl și glicemia
-
215mg/dl.
Prezen a materialului de osteosinteză de tipul tijelor
Radiogra a de bazin și coapsă ne relevă prezen a
Ender la pacien ii cu indica ie de amputa ie este o situa ie
materialului de osteosinteză (tije Ender).
rară care ridică probleme suplimentare, legate îndeosebi
Se instituie tratament antibiotic (ceftriaxonă 1g/8h și
de extragerea acestora. De regulă, aceasta se realizează
metronidazol 200ml/8h) și pacientul este trecut pe insulina
printr-o incizie în
1/3 inferioară a coapsei, deasupra
cu ac iune rapidă, frac ionată în 4 prize (0,5U/kgC/zi).
genunchiului, nivel indicat și pentru amputa ia de coapsă
deoarece realizează prezervarea unui bont lung.
Prezentarea cazurilor
Cazul nr. 1
Bolnavul de sex masculin în vârstă de 60 ani, din
mediu rural, s-a internat de urgen ă în clinica noastră
prezentând o leziune ulcerativ-necrotică la nivel plantar
și gleznă stângă cu semne de celulită prezente până în
Figura 1. Aspect preoperator al membrului inferior
1/3 medie a gambei, în evolu ie de 7 zile (Figura 1).
(necroză extensivă tegumentară fa ă laterală gamba
Starea generală a pacientului era alterată, acesta ind
stângă extinsă în profunzime la planul muscular;
adinamic, cu respira ii super ciale, oliguric și hipotensiv.
leziune ulcerativ-necrotică plantară stângă)
A
C
B
D
Figura 2. A: Incizie tegumentară în” bot de ra ă” în treimea inferioară coapsa stângă, B: Incizia
esutului celular subcutanat, C: Sec ionarea planului muscular; sângerare minimă, D: Sec ionarea
femurului în treimea inferioară coapsa stângă, cu eviden ierea tijelor centromedulare (săgeata)
100
Aiordăchioaie et al
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
CASE PRESENTATION
interven ie cu un bont viabil ce a fost ulterior protezat
(Figura 3,4).
Cazul nr. 2
Pacient în vârstă de 68 de ani, din mediu rural, se
internează de urgen ă în serviciul nostru prezentând la
nivelul gambei drepte în treimea medie o leziune
ulcerativă cu zone necrotice de 10/15 cm, edem gambier
extensiv și celulită prezentă inclusiv la nivelul
genunchiului.
Din antecedentele personale patologice re inem că
pacientul este fumător și cunoscut cu diabet zaharat tip
II de 10 ani în tratament cu metformin 500mgx2/zi și
glimepiridum 2mg 1/zi seara. Bolnavul a suferit în urmă
cu 15 ani o fractură trohanteriană femurală dreaptă
pentru care s-a practicat osteosinteza cu tijă
centromedulară de tip Ender.
Boala actuală a debutat brusc în urmă cu 10 zile
Figura 3. Bontul de
Figura 4. Protezarea
când, în urma unui traumatism cu un obiect contondent,
amputa ie la 1 an este de aspect
bontului
a rezultat o plagă gambieră de 2/3 cm. Plaga gambieră a
normal, cu cicatrice suplă
fost neglijată, evoluând pe fondul diabetului spre
gangrenă.
Având in vedere aspectul leziunilor și starea generală
Bioumoral s-au înregistrat următoarele modi cări
alterată, se stabilește indica ia de interven ie chirurgicală de
patologice: leucocite
25000/mm³, Hb
9,2 g/dl și
urgen ă ablativă. Tehnica operatorie aleasă a fost amputa ia
glicemie
253 mg/dl. Radiogra a de bazin și coapsă
coapsei deasupra genunchiului, supracondilian, de tip Gritti-
eviden iază prezen a tijelor femurale centromedulare,
Stokes (Figura 2-A,B,C,D). Acest abord a permis extragerea
ușor migrate inferior.
relativ facilă a tijelor centromedulare și crearea unui bont lung.
Se instituie tratament de urgen ă cu antibioterapie
Evolu ia postoperatorie a fost favorabilă, cu
(ceftriaxonă
1g/8h, gentamicină
40mg/12h și
vindecare lentă, pacientul ind externat la 30 zile după
metronidazol
200ml/12h) și echilibrare a diabetului
A
C
B
D
Figura 5. A: Incizie tegumentară eliptică în 1/3 inferioară coapsa dreaptă, B: Prelungirea inciziei
tegumentare la nivelul articula iei genunchiului şi reperarea capătului distal al unei tije Ender, C:
Extragerea uneia din cele 3 tije Ender, D: Sec ionarea femurului în 1/3 inferioară cu extragerea
celorlalte 2 tije restante împreună cu segmentul amputat
Thigh Amputations in Diabetic Patients with a History of Femoral Osteosynthesis. Case Report
101
CASE PRESENTATION
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
zaharat cu insulină cu ac iune rapidă frac ionată în 4
instruirea pacientului pentru prezentarea cât mai
prize (0,5U/kgC/zi).
precoce la medic în cazul apari iei leziunilor cu poten ial
Se decide amputarea de urgen ă a membrului
necrotic [1,7]. Practic, bolnavii diabetici, aterosclerotici
inferior la nivelul coapsei. Alegerea ideală a nivelului de
și cu trombangeită obliterantă trebuie să-și examineze
amputa ie ar trebuit să e în 1/3 inferioară a coapsei.
zilnic picioarele și să se prezinte la chirurg pentru orice
Datorită prezentării tardive a pacientului procesul
leziune constatată, urmând ca acesta să evalueze
infec ios a ascensionat până deasupra genunchiului, fapt
gravitatea acesteia și conduita de urmat [2,8].
care ne-a obligat la realizarea amputa iei în1/3 medie a
Prezen a tijelor
metalice
de osteosinteză
coapsei.
centromedulară la pacien ii cu gangrenă care necesită
Tehnica operatorie aleasă a fost procedeul eliptic
amputa ii de coapsă este o situa ie rară, care ridică o serie
Marcellin-Duval (Figura 5). Femurul a fost sec ionat
de probleme particulare. O primă necesitate este, în
circular și prin mișcări ușoare de rota ie s-a reușit
primul rând, stabilirea prezen ei tijelor, care nu vine
îndepărtarea segmentului distal al membrului inferior.
întotdeauna de la sine, mai ales la pacien ii cu de cit de
Am întâmpinat di cultă i suplimentare fa ă de primul
memorie sau cu pierdere a lucidită ii, de exemplu la
caz, legate de extragerea tijelor Ender, dar în nal s-a
bolnavii cu maladie Alzheimer. Asemenea situa ii nu sunt
reușit îndepărtarea acestora prin trac ionarea lor
foarte rare și posibilitatea acestora ne obligă la o anamneză
progresivă.
atentă și bine condusă, care să includă și întrebări
Evolu ia postoperatorie a fost lent favorabilă, ind
privitoare la eventualele fracturi femurale, modalitatea de
grevată de apari ia unei supura ii de plagă, tratată
osteosinteză. Astfel, vom lua în considerare un nou timp
conservator cu succes. Pacientul a fost externat la 35 zile
operator de extragere a tijelor. În această direc ie este utilă
cu bontul vindecat, urmând a protezat.
și chestionarea apar inătorilor dar, mai ales, consultarea
biletelor de ieșire din serviciile de ortopedie. Con rmarea
Discu ii
prezen ei tijelor este realizată prin examenul radiologic
care devine obligatoriu în asemenea situa ii.
În ciuda caracterului profund mutilant al amputa iei
Extragerea tijelor Ender la pacien ii la care se
de coapsă, prognosticul acestor pacien i poate
efectuează o amputa ie de coapsă se realizează cu relativă
semni cativ
îmbunătă it
datorită
dezvoltării
ușurin ă dacă se adoptă incizia standard în treimea
posibilită ilor de protezare și reeducare func ională. Se
inferioară a coapsei, prin trac ionarea de capătul distal al
știe faptul că acestea sunt dependente de viabilitatea și
tijei.
dimensiunile bontului, astfel, cu cât lungimea acestuia
După vindecarea plăgii postoperatorii trebuie
este mai mare, cu atât recuperarea este mai bună [3].
implementată o strategie de protezare și reeducare
Alegerea nivelului optim de amputa ie are un rol
func ională, stabilindu-se premisele pentru o reintegrare
hotărâtor, ind una din problemele cele mai delicate cu
socială cât mai bună. Succesul tuturor acestor demersuri
care se confruntă chirurgul în situa ia în care progresia
depinde în primul rând de determinarea pacientului dar
ascendentă a procesului infec ios este avansată. Regula
și de sprijinul moral al familiei, acesta ind de asemenea
de bază este realizarea amputa iei în treimea distală a
esen ial [3].
coapsei, ca în cazul nr. 1, situa ie ideală inclusiv pentru
pacien ii cu tije Ender deoarece oferă condi ii optime
Concluzii
pentru extragerea acestora, constatare în acord cu
rezultatele raportate și de al i autori [4,5]. În cazurile
Amputa iile de coapsă la pacien ii diabetici cu
neglijate, cu celulită deasupra genunchiului, devine
osteosinteză centromedulară femurală cu tije Ender
necesară realizarea inciziei la un nivel superior, în 1/3
ridică probleme particulare de diagnostic și tratament.
medie a coapsei, cum a fost cazul nr. 2. Desigur, această
Stabilirea prezen ei tijelor se face printr-o anamneza
op iune a lăsat un bont ceva mai scurt și implicit, mai
atentă coroborată cu consultarea biletelor de ieșire și cu
di cil de protezat, respectiv a creat di cultă i
examenul radiologic obligatoriu în aceste situa ii.
suplimentare intraoperatorii legate de extragerea tijelor.
La acești bolnavi indica ia de elec ie a nivelului
Pe de altă parte, o amputa ie în esuturile infectate din
sec ionării coapsei este în treimea distală, fapt care
treimea distală a coapsei ar implicat riscul major de
asigură atât extrac ia facilă a tijelor, cât și prezervarea
gangrenă de bont, cu consecin ele sumbre previzibile,
unui bont cât mai lung, cu ușurarea semni cativă a
poate chiar fatale
[6]. De aceea, pentru scăderea
protezării ulterioare.
numărului de amputa ii înalte, cu un grad ridicat de
Complexul terapeutic de care bene ciază acești
invaliditate și o protezare mai di cilă, este necesară
pacien i nu trebuie să se încheie cu vindecarea plăgii, ci
102
Aiordăchioaie et al
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
CASE PRESENTATION
trebuie continuat prin eforturi perseverente legate de
tips in major amputations of diabetic patients.
protezare și reeducare func ională.
Musculoskelet Surg 2012;96(3):191-7.
Mul umiri: Această lucrare a fost nan ată prin
4. Johannesson A. Incidence of limb amputation in the diabetic
Fondurile
Structurale
POSDRU/CPP107/DMI
and non-diabetic general population. A 10-years population
1.5/S/77082 „Burse doctorale de pregătire ecoeconomică
- based cohort study of initial unilateral, controlateral and
și bioeconomică complexă pentru siguran a și securitatea
reamputation. Diabetes care 2009;32:275-80.
alimentelor și furajelor din ecosisteme antropice”
5. Gray DWR. „Limb Amputation” in Morris PJ, Malt
RA. (sub red.), Oxford Textbook of Surgery. Oxford
University Press, Oxford, 1994
Referin e
6. Wong K, Nicholson DJ, Gray R. Lower limb
compartment syndrome arising from fulminant
1. Al-Wahibi AM. Impact of diabetic foot care education
streptococcal sepsis. ANZ J Surg 2005,75(8):728-9.
program on lower limb amputation rate. Vascular
7. Patrascu T, Doran H, Catrina E, Buga C, Muntean A,
Health and risk Management 2010;6:923-34.
Sera nceanu C. Particularită i ale chirurgiei la
2. Jankovic D. Case study: shock waves treatment of
diabetic, Ed. Niculescu, Bucureşti, 2005; pp 84-109.
diabetic gangrene. International Wound Journal
8. Stoia D, Hulpus R, Kiss I. Complica iile piciorului
2011;8(2):206-9.
diabetic raportate gradului de ischemie cronică a
3. Rosati M, Lisanti M, Baluganti A, Andreani L, Rizzo
membrelor inferioare, Acta Medica Transilvanica
L, Piaggesi A. A multidisciplinary approach and surgical
2011;2(3)149-50.
Thigh Amputations in Diabetic Patients with a History of Femoral Osteosynthesis. Case Report
103
CENTER FOR DOCUMENTATION AND
CONTINUOUS MEDICAL EDUCATION
SATU MARE
The need to continue and enhance medical programs for the medical personnel from
the primary and secondary care network, as well as the social and comunity staff from the
health care centers in the county of Satu Mare, is a problem whose solution is the
development of the Documentation and Continuous Medical Education Center Satu
Mare. Satu Mare College of Physicians in partnership with the Association of Family
Physicians Satu Mare, the Dental College Satu Mare, wishes within this project to
continue the health educational programs in order to improve health services for
vulnerable social groups: disabled, social cases as well as for the population of Satu Mare
county.
Necesitatea continuării şi perfecţionării programelor de educaţie medicală a
personalului medical din reţeaua de asistenţă primară şi secundară, precum şi a
personalului de asistenţă socială şi comunitară din centrele de îngrijire ale judeţului Satu
Mare este o problemă a cărei soluţie este dezvoltarea Centrului de Documentare şi
Educaţie Medicală Continuă Satu Mare. Colegiul Medicilor Satu Mare în parteneriat cu
Asociaţia Medicilor de Familie Satu Mare, Colegiul Medicilor Dentişti Satu Mare,
doreşte în cadrul acestui proiect continuarea programelor educaţionale în domeniul
sănătăţii în vederea ameliorării serviciiilor de sănătate pentru grupurile sociale
vulnerabile: dizabilităţi, cazuri sociale, precum şi pentru populaţia judeţului Satu Mare.
MEDICINE AND ART
REPREZENTAREA SECHELELOR POLIOMIELITEI ÎN ARTĂ
Bumbulu Călin1, Bumbulu Andrei2, Oprea Andrea2, Koren Rumelia3
1SCM dr Bumbulu -dr Balaj, Satu Mare, România, 2Facultatea de Medicină, Universitatea de Medicină şi Farmacie Iuliu
Ha ieganu, Cluj Napoca, România, 3Departmentul de Patologie, Spitalul Hasharon, Petah Tikva şi Facultatea de Medicină
Sackler, Universitatea Tel-Aviv, Israel
Adresa pentru coresponden ă:
Dr. Bumbulu Călin
Satu Mare, str. Bobocului UK 30-440258
Email: bumbulutcalin@yahoo.com
Primit: 15.07.2013
Acceptat: 10.08.2013
Med Con October 2013 Vol 8, No 3, 105-108
Rezumat
Cuvântul poliomielită are ca rădăcină trei cuvinte
grecești: „Polio” înseamnă „gri”, referindu-se la materia
Impactul poliomielitei asupra activită ii și
cenușie,
„Myelon” înseamnă „coloană vertebrală”, iar
participării sociale poate văzut în arta egipteană antică.
„Itis” înseamnă „in ama ie”. Prima descriere clinică a
Primele epidemii moderne au fost alimentate de
bolii a fost făcută în 1789 de către medicul britanic
creșterea
orașelor
după revolu ia industrială.
Michael Underwood, ind recunoscută ca și condi ie
Reprezentarea artistică a de cien elor și dizabilită ilor a
medicală de către Jakob Heine în
1840. Primele
evoluat în paralel cu sentimentele oamenilor fa ă de ele
epidemii moderne au fost alimentate de creșterea
în ecare perioadă istorică și, în același timp, cu evolu ia
orașelor după revolu ia industrială. Reprezentarea
socială. În „Lupta dintre Carnaval și Postul Mare” pictat
artistică a de cien elor și dizabilită ilor a evoluat în
de Pieter Bruegel în 1559, apar două guri de in rmi;
paralel cu sentimentele oamenilor fa ă de ele în ecare
deși această mărturie artistică nu este o dovadă o cială a
perioadă istorică și, în același timp, cu evolu ia socială.
poliomielitei, există indicii puternice că ambii au suferit
În zilele noastre, acest concept continuă să avanseze, iar
de pe urma bolii. Desenul „Studii despre cerșetori și
unii artiști nu mai reprezintă persoana bolnavă, ci boala
vagabonzi”, din aceeași perioadă, despre care nu știm
în sine. Pe măsura trecerii timpului, oamenii au evoluat
dacă apar ine lui Hieronymus Bosch sau lui Pieter
și totodată și medicina și arta. În aceasta constă valoarea
Bruegel cel Bătrân, surprinde, de asemenea, crudele
extraordinară, din punct de vedere ontologic, a multor
consecin e ale bolii. În 1899, Joaquín Sorolla a pictat un
opere de artă, care nu ar fost create fără interven ia
grup de copii, având probabil sechele ale poliomielitei,
bolii și a practicii artei medicale [1].
făcând baie pe plaja din Valencia. Una dintre cele mai
Impactul poliomielitei asupra activită ii și
cunoscute imagini din arta americană a secolului XX
participării sociale poate văzut în arta egipteană antică.
este pictura lui Andrew Wyeth, Lumea Christinei, în
Figura 1 prezintă un preot numit Rom (în alte surse, un
care femeia care a suferit de poliomielită este descrisă
portar numit Roma sau Ruma), care face o ofrandă,
târându-se chinuitor prin curte.
având un baston și deformări ale piciorului caracteristice
Cuvinte cheie: poliomielită, pictură, desen, artă
poliomielitei. Unii cercetători medicali au interpretat
egipteană, Pieter Bruegel cel Bătrân, Hieronymus
deformitatea lui Rom ca nd rezultatul poliomielitei,
Bosch, Joaquin Sorolla y Bastida, Andrew Wyeth Newell
al ii cred că nu este poliomielită, ci un anumit tip de
The Description of the Sequels of Poliomyelitis in Art
105
MEDICINE AND ART
MEDICAL CONNECTIONS • NUMBER 2 (30) • JUNE 2013
Figura 1. Stelă egipteană datând din 1403-1365 ÎH
Figura 4. Hieronymus Bosch (?), „Studii despre cerşetori şi
vagabonzi”, peni ă şi cerneală maro pe hârtie, 1465-1559 (?)
Figura 2. Pieter Bruegel cel Bătrân, „Lupta dintre
Carnaval şi Postul Mare”, ulei pe panou, 1559,
Kunsthistorisches Museum, Viena
Figura 3. Pieter Bruegel cel Bătrân, „Lupta dintre
Figura 5. Hieronymus Bosch (?), „Studii despre cerşetori
Carnaval şi Postul Mare”, ulei pe panou, 1559,
şi vagabonzi”, peni ă şi cerneală maro pe hârtie,
Kunsthistorisches Museum, Viena, detaliu
1465-1559 (?), detaliu
106
Bumbuluț et al
MEDICAL CONNECTIONS • NUMBER 2 (30) • JUNE 2013
MEDICINE AND ART
picior strâmb congenital, cu afectare secundară și
scurtarea piciorului. Mumia faraonului Siptah are un
picior stramb și atro at, la fel ca a lui Rom. Ca și copil,
Siptah a contractat o boală care l-a lăsat cu un picior
atro at, umblând pe el mai mul i ani înainte de
maturizarea oaselor.
În secolul al XVI-lea, pictura renascentistă radiază
din Italia în toată Europa. Mul i artiști din nordul
Europei au răspuns la aceasta prin fuziunea compozi iei
clasice italiene, cu realismul foarte detaliat din pictura
ărilor de Jos. Totuși, cel mai mare pictor al ărilor de
Jos din secolului al XVI-lea, Pieter Bruegel cel Bătrân (c.
1525 - 9 septembrie 1569), a ales să nu să îmbră ișeze
arta italiană. În locul scenelor biblice clasic-structurate,
Figura 6. Joaquín Sorolla, „Trista moştenire”, ulei, 1899
Bruegel a preferat să descrie cronica vie ii zilnice a
ăranilor, decât a interioarelor realiste și a peisajelor.
„Lupta dintre Carnaval și Postul Mare” (Figura 2) este o
lucrare pictată de acesta în 1559. Tabloul descrie un
festival obișnuit în acea perioadă, așa cum era celebrat în
ările de Jos. El prezintă contrastul dintre cele două
laturi ale vie ii contemporane pictorului, gurate prin
reprezentarea hanului pe partea stângă
- pentru
distrac ie și a bisericii pe partea dreaptă
- pentru
respectarea religiei. În pictură apar și două guri de
in rmi, unul are un picior mutilat, mergând cu o cârjă
de lemn (Figura 3). Celălalt avansează pe mâini, cu
picioarele atro ate și îndoite, legate de atele, atârnând în
spatele lui. Micile „capre” pe care omul se sprijină erau
Figura 7. Andrew Newell Wyeth, Lumea Christinei , 1948,
numite
„scabella”, iar oamenii care le utilizau
Muzeul de Artă Modernă, New York
„scabellarii”. Deși această mărturie artistică nu este o
dovadă o cială a poliomielitei, există indicii puternice
că ambii au suferit de pe urma bolii [2].
Andrew Wyeth Newell (12 iulie 1917 - 16 ianuarie
Desenul „Studii despre cerșetori și vagabonzi”, din
2009) a fost un pictor realist. În arta sa, subiectele
aceeași perioadă, despre care nu știm dacă apar ine lui
preferate de Wyeth au fost pământul, precum și oamenii
Hieronymus Bosch (c. 1450 - 9 august 1516) sau lui
din jurul lui. Una dintre cele mai cunoscute imagini din
Pieter Bruegel cel Bătrân, surprinde, de asemenea,
arta americană a secolului XX este pictura lui, „Lumea
crudele consecin e ale bolii [3,4].
Christinei” (Figura 7). Femeia din tablou este Christina
Joaquin Sorolla y Bastida (27 februarie 1863 - 10
Olson (3 mai 1893 -27 ianuarie 1968). Wyeth avea o casă
august 1923) a fost un pictor spaniol, născut în Valencia,
de vară în zonă și a fost în rela ii de prietenie cu Olson,
care a excelat în portrete, peisaje și lucrări monumentale
atât ea, cât și fratele ei mai mic, ind subiectele unor
pe teme sociale și istorice. Lucrarile sale tipice sunt
tablouri între
1940-1968 [6]. Totuși, deși pictura era
caracterizate de o reprezentare cu măiestrie a oamenilor
aparent despre ea, Wyeth nu a folosit-o pe Olson ca
și a peisajului, sub lumina soarelui ării sale natale. În
model. În schimb, a chemat-o pe so ia lui, care avea în jur
august 1865, el și sora sa rămân orfani, părin ii lor
de 25 de ani, pentru a poza, recreând momentul în care
murind probabil din cauza holerei. După terminarea
s-a uitat pe fereastră și a văzut-o pe vecina sa, care suferea
serviciului militar, la douăzeci și doi de ani Sorolla
de poliomielită, târându-se chinuitor prin curte. Olson
ob ine o bursă, care îi permite studiul picturii la Roma,
avea 55 de ani la momentul în care Wyeth a creat opera.
timp de patru ani. O ședere prelungită la Paris în 1885 îl
Pictura despre femeia tânără într-o rochie roz, cu
expune pentru prima dată picturii moderne. În 1899,
membrele inerte, are o calitate care te bântuie. Peisajul și
Joaquín Sorolla prezintă, pe o mare pânză (Figura 6), un
casa rurală sunt pictate în detaliu. Fiecare r de iarbă și
grup de copii, probabil cu sechele de poliomielită,
ecare r de păr al femeii sunt pictate individual. Stilul
făcând baie pe plaja din Valencia [5].
picturii a fost numit „realism magic”, de nit ca un gen
The Description of the Sequels of Poliomyelitis in Art
107
MEDICINE AND ART
MEDICAL CONNECTIONS • NUMBER 2 (30) • JUNE 2013
artistic în care pictura realizată meticulos și realist, este
2. Bonn, R. Painting Life. e Art of Pieter Bruegel e
combinată cu elemente suprarealiste de fantezie sau din
Elder, Chaucer Press Books, 2006.
vise. Wyeth comentând despre pictura lui spunea:
3. Friedländer, Max J. Early Netherlandisch Painting.
„Provocarea pentru mine a fost de a face dreptate luptei ei
Volume V. Geertgen tot Sint Jans and Jerome Bosch,
extraordinare pentru o via ă pe care majoritatea oamenilor
Leyden: A.W. Slijthof, 1969.
ar considera-o fără speran ă.”
4. Cohn, V. Sister Kenny. e Woman Who Challenged the
Doctors. Minnesota Archive Editions, USA, 1975.
5. Martínez-Lage JF, Pérez-Espejo MA, Galarza M.
Referin e
Portraying disease: Sorolla’s Sad Legacy. Childs Nerv
Syst
2012 Jul;28(7):959-61. doi: 10.1007/s00381-
1. Cano de la Cuerda R, Collado-Vazquez S. De ciency,
012-1687-y
disability,
neurology and art. Rev Neurol
6. h t t p s : / / w w w. m a i n e . g ov / e d u c a t i o n / l re s / v p a /
2010;51(2):108-16.
documents/CHRISTINAOLSONBIO.pdf
108
Bumbuluț et al
IN MEMORIAM
Profesor Dr. Thoma Ionescu
(13 septembrie 1860, Ploieşti - 28 martie 1926, Bucureşti)
oma Ionescu este întemeietorul şcolii româneşti de chirurgie şi de anatomie topogra că,
membru de onoare al Academiei Române.
După terminarea liceului „Sf. Sava” oma Ionescu se înscrie la Facultatea de Medicină
din Paris în 1879, devenind în 1892 doctor în medicină şi chirurgie. În 1887 ob ine prin
concurs locul de prosector asociat de anatomie şi mai apoi prosector de nitiv la Facultatea de
Medicină din Paris. Îşi sustine teza de doctorat în 1892, cu lucrarea „L’evolution intrauterine
du colon pelvien” obtinând titlul de laureat al spitalelor din Paris, după ce în 1890 ob ine
titlul de laureat al Academiei de chirurgie din Fran a pentru lucrarea
„Les hernies
intraperitoneales”. În anul 1892, în urma unui concurs la care se clasi că primul, oma
Ionesu ob ine titlul de profesor agregat. Colaborează cu profesorii Poirier şi Charpy la cel mai
mare tratat de anatomie al vremii, în 1894, scriind capitolul „L’anatomie de tube digestiv” în
care descrie pentru prima dată fosetele duodeno-jejunale, fosetele sigmoidiene, teaca rectului şi
aripioarele rectale. În 1895, prin decret de lege se în in ează la Facultatea de Medicină din
Bucureşti catedra de anatomie topogra că şi clinică chirurgicală la care este chemat ca profesor.
În 1897, împreună cu colaboratorii săi fondează revista „Chirurgia”, periodic al Societă ii
Române de Chirurgie. În perioadele 1906-1912, 1921-1922 şi 1925-1926 este Decan al
Facultă ii de Medicină, iar între 1912 şi 1915 Rector al Universită ii din Bucureşti.
oma Ionescu a publicat numeroase articole despre rezec ia simpaticului cervical în
tratamentul anginei pectorale,
„cura Ionescu”, despre gastrectomia totală în cancerul de
stomac, a imaginat şi dezvoltat tehnici operatorii originale de trepana ie, nefropexie,
splenectomie şi în cura radicală a herniilor. În timpul unor vizite în Anglia şi America în anii
1909-1910, a lansat „rahianestezia înaltă”, utilizabilă şi la interven ii chirurgicale efectuate
pe toracele superior şi gât, făcând demonstra ii operatorii în clinici de renume din Londra,
New York, Philadelphia, Chicago, precum şi la vestita clinică a fra ilor Mayo din Rochester.
Chiar şi astazi, în vestita clinică Mayo se a ă bustul chirurgului român oma Ionescu.
De numele său se leagă răspândirea narcozei prin rahianestezie, utilizând mai întâi un
amestec de stovaina şi stricnina, apoi de stovaină şi cofeină. Eponime asociate pe lângă „cura
Ionescu”: „acul Ionescu” pentru sutura totală cu r de metal, „depărtătorul Ionescu”, depărtător
autostatic abdominal de care se pot xa valve de diferite mărimi,
„opera ia Ionescu”,
histerectomie totală largită cu extirparea grupelor ganglionare limfatice.
A dat întotdeauna dovadă de o atitudine profund na ională; la izbucnirea primului
război mondial, pleacă la Iaşi, unde continuă munca de chirurg, operând mii de solda i
răni i, veni i de pe front. Încheierea „păcii de la Buftea” l-a obligat să părăsească ara. În anul
1920 se întoarce şi reia cercetările şi activitatea didactică. Activează pentru cauza Unirii
Professor Dr. Thoma Ionescu
109
IN MEMORIAM
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
Transilvaniei cu România în cadrul Consiliului National al Unită ii Române de la Paris, iar
în 1920-1921 sus ine interesele ării ca prim delegat al României la sesiunile Ligii Na iunilor.
Toma Ionescu a fost numit delegat al României la Societatea Na iunilor, calitate în care a luat
parte la cele dintâi sesiuni ale organiza iei de la Geneva. Frate cu omul politic Take Ionescu,
a fost în mai multe rânduri ales deputat şi senator. O cuvântare inută în 1906 în Camera
Deputa ilor dezvăluie - în măsura în care o declara ie politică a oricărei vremi poate re ecta
realitatea - umbrele omului oma Ionescu, pe de-o parte: contestarea meritelor institu iei
medicilor de plasă, sau celei a spitalelor jude ene, desconsiderarea moaşelor şi subchirurgilor
rurali, eviden ierea doar a realizărilor Partidului Conservator, dar pe de altă parte,
convingerile sale luminoase, subliniate şi de Ion Cantacuzino: „nu a ştiut ce este ura, invidia,
răzbunarea, nu a ştiut ce este egoismul”, prin apărarea intereselor ărănimii spunând despre
calitatea presta iilor medicale acordate popula iei rurale: „ceea ce nu este bun pentru noi nu
trebuie să e bun nici pentru ăran”.
În 1926, moare la vârsta de 66 de ani, lăsând în urmă o şcoală adevărată de chirurgie
românească. A fost înmormântat la Cimitirul Bellu Ortodox, lângă mormântul lui Grigore
Romniceanu un alt eminent chirurg.
Bumbulu Călin, Koren Rumelia
Referin e
1. Vidu, V. Medalion aniversar: oma Ionescu. Jurnalul de Chirurgie, 2010;6(3):388-93.
3. Angelescu, N. oma Ionescu (1860-1926). Chirurgia, 2005;100(1):9-10.
4. Ciurea, AV, Palade, C. Professor oma Ionescu - founder of modern surgical practice in
Romania. Romanian Neurosurgery 2010,2:137-42.
5. Făgăraşanu, I. Via a şi opera lui Toma Ionescu, Ed Academiei Române, Bucureşti, 1962.
110
Bumbuluț et al
STANDARDE DE REDACTARE
Scop
materiale care ar putea să îi identi ce. Dacă formularele
Revista Conexiuni Medicale publică lucrări de
de accept nu prevăd acest lucru vă rugăm să rugăm
cercetare care contribuie la progresul din toate domeniile
ob ine i acordul, sau îndepărta i posibilitatea de
medicinei. Revista publică de asemenea reviste generale,
identi care. O declara ie în acest sens trebuie inclusă în
editoriale și scurte comunicări pe domenii speci ce.
sec iunea „Metode” a lucrării.
Prezentările de caz sunt acceptate dacă prezintă interes
crescut și sunt bine investigate. Scrisorile către editor, în
Aprobarea Comitetului de Etică
special cele care prezintă o opinie privind un articol
Preciza i la sec iunea „Metode” faptul că desfășura i
publicat anterior sau care prezintă noi date, sunt de
studii asupra subiec ilor umani cu aprobarea Spitalului,
asemenea binevenite. Adresa web a revistei este http://
Comitetului de Etică al Universită ii, etc. În mod
similar, con rma i dacă experimentele asupra animalelor
trimestrial, articolele sunt acceptate în limba engleză sau
corespund standardelor etice.
română, având cel pu in traducerea în limba engleză a
rezumatului și cuvintelor cheie. Lucrările pot trimise
Asumarea dreptului de copyright
pe adresa: dr. Bumbulu Călin, editor șef adjunct,
Lucrările acceptate pentru publicare au implicit
Conexiuni Medicale, P- a. Eroilor Revolu iei nr. 23,
drepturile de copyright cedate către editor. Autorii pot
cod 440055, Satu Mare, România. Tel./Fax: +40-261-
utiliza materiale din lucrările lor în alte articole proprii,
710456, e-mail: bumbulutcalin@yahoo.com.
după ob inerea acceeptului editorului.
Republicarea articolelor
Propunerea pentru publicare
Vă rugăm să con rma i că lucrarea dumneavoastră
Toate manuscrisele propuse pentru publicare în
nu a mai fost publicată în forma prezentată sau într-o
Conexiuni Medicale vor în format compatibil pentru
formă asemănătoare, sau că nu a fost acceptată pentru
efectuarea recenziei online. Revista acceptă manuscrise
publicare într-o altă revistă.
propuse în formă electronică, în format Word (text,
guri și tabele). Nu trimite i lucrări în format PDF.
Con icte de interese
Acceptăm lucrări care nu depășesc 3.500 de cuvinte
Rugăm autorii să declare posibilele con icte de
pentru articole originale, 2.500 pentru prezentări de
interese, inclusiv cele de natură nanciară. Dacă nu
caz, 2.000 pentru prezentări de imagini clinice, 500
există con icte de interese, vă rugăm să preciza i acest
pentru scrisori către editor și 4.500 de cuvinte pentru
lucru. Sursele de nan are trebuie precizate în lucrarea
reviste generale. Autorii NU vor trimite prin poștă sub
dumneavoastră.
formă de hârtie propunerea pentru publicare, decât
dacă este vorba de scrisori sau dacă se solicită astfel din
Permiterea de a reproduce materiale
partea redac iei. Dacă nu există altă op iune decât
publicate anterior
trimiterea prin poștă, vă rugăm să expedia i și versiunea
Vă rugăm să ne trimite i o copie a acceptului de
electronică CD-ROM pe adresa redac iei: Conexiuni
reproducere (de exemplu al ilustra iilor) de la de inătorul
Medicale, P- a. Eroilor Revolu iei nr. 23, cod 440055,
dreptului de copyright.
Satu Mare, România. Utiliza i text la două rânduri și
include i următoarele sec iuni: pagina de titlu,
Formularele de accept ale pacien ilor
rezumatul și cuvintele cheie, textul, mul umiri,
Protec ia drepturilor pacien ilor este esen ială; vă
referin e, tabele și guri. Paginile vor
numerotate
rugăm să ne trimite i formularele de accept ale
consecutiv, începând cu pagina de titlu, numerele
pacien ilor sau subiec ilor studiului dumneavoastră,
arabe ind plasate în col ul din dreapta sus al ecărei
prin care aceștia permit publicarea fotogra ilor sau altor
pagini.
111
GUIDANCE FOR DRAWING UP
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
Prezentarea lucrării
Nu recomandăm utilizarea excesivă a abrevierilor. Folosi i
Pagina de titlu
metode de calcul statistic standardizate. Nominaliza i
Cuprinde titlul întreg și titlul scurt format din
medicamentele și substan ele chimice utilizând numele
maxim 45 de caractere, numele și prenumele ecărui
generic
(dacă sunt men ionate mărcile înregistrate, se
autor; dacă lucrarea apar ine unui departament sau unei
furnizează numele producătorului și orașul).
institu ii, va men ionat numele acestuia în întregime.
Mul umiri
De asemenea numele, e-mail-ul și adresa autorului
Vor
adresate celor care au adus contribu ii
împuternicit pentru coresponden ă, sursele de nan are
importante la studiu.
sau suport utilizate sub forma burselor, echipamentelor,
Referin e
medicamentelor, sau orice combina ie a acestora.
Vor
numerotate între paranteze drepte cu
Rezumatul
numerale arabe, succesiv în ordinea în care sunt
Pagina a doua va cuprinde rezumatul cu minim 200
men ionate în text. Referin ele vor include numele
de cuvinte; nu utiliza i abrevieri, note de subsol, sau
autorilor până la al șaselea autor, dacă sunt mai mul i,
referin e.
enumera i primii trei și apoi adăuga i „et al”. Referin ele
Introducere în temă și scopuri
vor include titlul complet și sursa informa iei; numele
Descrie i importan a studiului și obiectivul
revistelor va abreviat conform Index Medicus (http://
(obiectivele) precise ale cercetării sau întrebarea
(întrebările) pe care le ridică studiul.
acceptă mai mult de 90-100 referin e; pentru scrisori
Metode
către redac ie se acceptă
5-6 referin e. Folosi i ca și
Include i informa ii privind următoarele aspecte ale
referin e cât mai pu ine rezumate. Comunicările
studiului dacă sunt utilizate: proiectul
- descrie i
personale și lucrările nepublicate nu vor men ionate la
elementele de bază ale studiului, de exemplu studiu
referin e și vor apare în text între paranteze. Lucrările
controlat randomizat, studiu cross-sec ional, de cohortă,
nepublicate dar a ate în curs de publicare vor incluse
de urmărire, serii de cazuri, etc; procedura - speci ca i
în referin e cu men iunea „in press” între paranteze,
dacă a fost desfășurat în sistem de îngrijire primar sau
lângă numele revistei implicate.
ter iar, în ambulator sau spital, în comunitate, etc;
a) Articole:
participan i - indica i numărul subiec ilor și cum au
[1] Otvos L Jr, Shao WH, Vanniasinghe AS, Amon
fost selecta i, recruta i și desemna i pentru interven ie;
MA, Holub MC, Kovalsykz I, et al. Toward understanding
interven ia
- metoda de administrare și durata
the role of leptin and leptin receptor antagonism in
interven iei.
preclinical models of rheumatoid arthritis. Peptides
Rezultate
2011;32:1567-74.
Prezenta i principalele rezultate ale studiului,
b) Lucrări publicate numai cu numerele DOI:
inclusiv intervalurile de con den ă sau valorile p.
[2] Chaldakov GN, Beltowsky J, Ghenev PI, Fiore
Concluzii
M, Panayotov P, Rancic G, et al. Adipoparacrinology -
Enun a i doar concluziile sus inute direct de dovezi,
vascular periadventitial adipose tissue (tunica adiposa) as
precum și importan a descoperirilor. Revistele generale
an example. Cell Biol Int
2011;doi:
10.1042/
și prezentările de caz vor include un rezumat
CBI20110422.
nestructurat.
c) Căr i sau manuale:
Cuvinte cheie
[3] Gertler A, editor. Leptin and Leptin Antagonists.
Rezumatul va urmat de o listă de 3-10 cuvinte
Landes Bioscience, Austin, Texas, USA. 2009.
cheie sau fraze scurte care vor ajuta la indexare. Dacă
d) Capitole de căr i sau de manuale:
este posibil, utiliza i termeni proveni i din lista Index
[4] Jeremy L, Abe PD. Treatment Options in
Medicus cu
262 subiecte medicale/Medical Subject
Super cial (pTa/pT1/CIS) Bladder Cancer. In: Urological
Headings
262
cancers in clinical practice, Springer-Verlag, London
meshhome.html).
Limited, 2007:75-102.
Textul
Tabele
Un studiu original va divizat în sec iuni denumite
Fiecare tabel va numerotat cu numerale romane,
Introducere, Metode, Rezultate și Discu ii
(incluzând
cu un titlu scurt deasupra, la subsolul lor vor trecute
concluziile), după formula „IMRAD”. Articolele lungi
notele
explicative,
men ionându-se abrevierele
pot necesita subsec iuni (în special la Rezultate și Discu ii)
nestandardizate utilizate; nominaliza i valorile statistice
pentru clari care. Alte tipuri de articole precum prezentări
care variază precum devia ia standard și eroarea standard
de caz, reviste generale, editoriale, pot urma alt format.
a medianei. Fiecare tabel va citat în text.
112
MEDICAL CONNECTIONS • NUMBER 3 (31) • OCTOBER 2013
GUIDANCE FOR DRAWING UP
Figuri
acestor sugestii, rugându-i să răspundă la întrebări și să
Toate gra cele, fotogra ile, diagramele vor
facă necesarele corec ii. Aceste informări sunt făcute în
considerate ca guri și vor numerotate succesiv în text
cel mult trei luni de la propunerea de publicare.
cu numerale arabe. Dacă o gură a fost publicată
Manuscrisul revizuit de autori va reexpediat editorului
anterior, sursa va citată cu mul umiri, men ionându-
în cel mult o lună. La primirea de către editor a versiunii
se permisiunea de inătorului de copyright. Figurile pot
corectate, înso ită de o scrisoare de răspuns punctuală la
reduse, grupate sau șterse la dorin a editorului.
comentariile recenzorilor, se retrimite manuscrisul
Legenda gurii va plasată la subsolul ei; va explicată
acelorași recenzori, care vor face recomandarea nală
scala utilizată, respectiv metodele de colorare
pentru acceptarea sau respingerea acestuia.
microscopică.
Unită i de măsură
Abonamente
Măsurătorile lungimii, înăl imii, greută ii și
Pre ul unui abonament anual pentru 2013 este: 80
volumului vor făcute în sistem metric sau multipli
RON individual, 160 RON pentru institu ii, plăti i în
decimali. Temperaturile vor
exprimate în grade
contul Colegiului Medicilor Satu Mare RO38 BTRL
Celsius. Tensiunea va
măsurată în mmHg. Toate
0310
1202 K392
62XX, cod scal
9839430, cu
măsurătorile hematologice vor exprimate în Sistemul
men iunea
„pentru abonament Conexiuni Medicale”.
Interna ional de Unită i (SI).
Solicitarea abonării poate
trimisă prin poștă: P- a.
Abrevieri și simboluri
Eroilor Revolu iei nr.
23, cod
440055, Satu Mare,
Utiliza i doar abrevieri standard. Evita i abrevierile
România. Tel./Fax: 0261-710456, 0361-408164, sau
în titlu și rezumat. Cuvântul va preceda abrevierea la
prin e-mail: colmedsm@gmail.com.
prima utilizare în text, cu excep ia unită ilor de măsură
standard.
Publicitate
Cererile pentru spa iu publicitar vor
adresate
Retipăriri
redac iei Conexiuni Medicale. Pre urile (plătite în lei la
Sunt oferite gratuit zece copii ale articolului publicat
cursul BNR) pentru publicitate pe 2013 sunt 200 euro
și două ale revistei. Dacă sunt necesare mai multe copii,
pagina (A4) color, un număr și 800 euro patru numere;
sunt disponibile contra cost.
coperta interioară fa ă sau spate: 350 euro un număr,
1400 euro patru numere; coperta exterioară spate: 400
Politica editorială
euro un număr, 1600 euro patru numere. Cont bancar:
Apreciem toate contribu iile în domeniul medicinei.
Colegiul Medicilor Satu Mare, CUI 9839430, Banca
Invităm personalită i recunoscute cu expertiză și articole
Transilvania, agen ia Golescu Satu Mare, IBAN: RO38
din diverse domenii să publice reviste generale și
BTRL 0310 1202 K392 62XX.
editoriale în revista noastră. Acceptăm de asemenea
lucrări originale și prezentări de caz din toate ările.
© Copyright Conexiuni Medicale/Medical
Conexiuni Medicale vă oferă o recenzie atentă și publicarea
Connections, Satu Mare, 2013
imediată după acceptare. Redactorii vor citi primii
Nicio parte a acestei publica ii nu poate reprodusă,
lucrarea, decizând în decurs de 1-3 săptămâni în func ie
stocată sau transmisă sub orice formă sau prin orice
de nivelul de prioritate: unele sunt trimise imediat
mijloace, fără permisiunea prealabilă în scris a revistei
recenzorilor, unele pot
respinse, iar unele sunt
Conexiuni Medicale. Permisiunea nu este necesară
returnate autorilor cu sugestii de îmbunătă ire înainte
pentru a copia rezumate sau articole dacă este indicată
de expedierea spre recenzori.
sursa, cu citarea completă a referin ei. Solicitarea
privind permisiunea de a retipări toată revista sau o
Procedura peer-review
parte a ei, va
adresată editorului prin e-mail:
Conexiuni Medicale practică o evaluare a tuturor
colmedsm@gmail.com
lucrărilor originale de către doi sau trei recenzori
independen i, din care doi sunt personalită i
Revista Conexiuni Medicale apare trimestrial prin
interna ionale. Procesul peer-review este esen ial pentru
efortul logistic și nanciar al Colegiului Medicilor
asigurarea calită ii informa iei știin i ce. Recenzorii
Satu Mare și Asocia iei Medicilor de Familie Satu
sunt ruga i să evalueze manuscrisul aplicând aceleași
Mare, în cadrul proiectului comun al Centrului de
standarde ca și pentru reviste interna ionale; comentariile
Documentare și Educa ie Medicală Continuă Satu
sunt trimise editorului, care va informa autorii asupra
Mare.
113