MEDICAL CONNECTIONS | CONEXIUNI MEDICALE
ASSISTANT EDITORS
EDITOR IN CHIEF
Blaga Vasile (electronic version)
Koren Rumelia
Andó Ottó (print version)
ASSISTANT EDITOR IN CHIEF
Oană Cristian Sever (editorialist)
Bumbuluţ Călin
Tudor Stăncioiu (Dental Medicine)
EDITORIAL BOARD
Bauer Adalbert (SCM Satu Mare, România)
Lup Liliana (Synevo Satu Mare, România)
Bidilean Nicolae (Emergency County Hospital,
Kesler Gavriel (Israel)
Satu Mare, România)
Kiss Ladislau (Emergency County Hospital,
Boros Melinda (Bucureşti, România)
Satu Mare, România)
Borcean Gheorghe (Caransebeş Hospital, România)
Mihalca Man Sorina (Emergency County Hospital,
Brândeu Ioan (Emergency County Hospital,
Satu Mare, România)
Satu Mare, România)
Neumann Gad (Hasharon Hospital, Tel Aviv, Israel)
Cârstea Constantin (CMI Braşov, România)
Negru Alina (Centro de Salud Caspe, Zaragoza, Spain)
Cojocaru Manole (Titu Maiorescu University,
Rath-Wolfson Lea (Hasharon Hospital, Tel Aviv, Israel)
Bucureşti, România)
Rădulescu Viorel (CMI Olt, România)
Comăneanu Raluca Monica (Titu Maiorescu University,
Roatiş Marius Dinu (Emergency County Hospital,
Bucureşti, România)
Satu Mare, România)
Cornean-Santa Corina (Emergency County Hospital,
Rusu Cristian Bogdan (Emergency County Hospital,
Satu Mare, România)
Satu Mare, România)
Feciche Bogdan (Emergency County Hospital,
Shvero Kesler Dana (Hadassa University, Jerusalem, Israel)
Satu Mare, România)
Trip Gheorghe (Emergency County Hospital,
Grosz Gyula (SCM West Satu Mare, România)
Satu Mare, România)
Gruzman Carlos (Hasharon Hospital,
Zilahi Karoly (SCM Praxis, Bixad, România)
Tel Aviv, Israel)
Zeidman Aliza (Hasharon Hospital, Tel Aviv, Israel)
Horber Orsolya (SCM Praxis Bixad, România)
Virag Tiberiu (CMI Satu Mare, România)
EDITOR
ASSOCIATED EDITOR
College of Physicians Satu Mare
Satu Mare Association of Family Physicians
Satu Mare, 23 Eroilor Revoluţiei Pl.
Affiliated with National Society of
Family Medicine/General Medicine
email: colmedsm@gmail.com
Satu Mare, UK 30 Bobocului St.
PARTNERSHIP
EXTERNAL PARTNERSHIP
Titu Maiorescu University, Bucharest
Hasharon Hospital, Rabin Medical Center
Faculty of Medicine and Dental Medicine
Affiliated with Sackler School of Medicine, Tel Aviv University,
67A Gheorghe Petraşcu St.
7 Keren Kayemet St., Petah Tikva 49372, Israel
EDITORIAL OFFICE
23 Eroilor Revoluţiei Pl., 440055, Satu Mare, Romania, Tel/Fax: 0040261-710456, 0040361-408164, http://
ISSN online 2068 - 8369
ISSN 1843 - 9306
Journal included in Te Schedule of Medical Publications of CMR, 5 credits CMR for subscribers
Indexed in Index Copernicus®, CNCSIS B+ Category, Code 944
Medical Connections/Conexiuni Medicale® is a trademark of College of Physicians Satu Mare and Satu Mare Association of Family Physicians
Printed at TIPOOFFSET, Fabricii str, No. 93-103, Cluj Napoca, Tel./Fax: 0040264-456071
SCIENTIFIC AND PEER REVIEW BOARD | COLECTIV ŞTIINŢIFIC ŞI DE RECENZIE
Acad. Prof. Univ. as. Dr. Virgil Enătescu
Prof. Univ. Dr. Tuvia Hadar
(Emergency County Hospital, Satu Mare,
(Beilinson Hospital, Rabin Medical Center, Sackler
Romania)
Faculty of Medicine, Tel Aviv University, Israel)
Acad. Prof. Univ. Dr. Doina Onicescu
Prof. Univ. Dr. Gheorghe Manole
(Titu Maiorescu University, Faculty of Medicine
(Titu Maiorescu University, Faculty of Medicine
and Dental Medicine, Bucharest, Romania)
and Dental Medicine, Bucharest, Romania)
Acad. Senior Scientific Researcher Dr. Sorin Riga
Prof. Univ. Dr. Dorel Augustin Manu
(Prof. Dr. Al. Obregia Clinic Hospital of Psychiatry,
(Titu Maiorescu University, Faculty of Medicine
Bucharest, Romania)
and Dental Medicine, Bucharest, Romania)
Acad. Senior Scientific Researcher Dr. Dan Riga
Prof. Univ. Dr. Dan Mănăstireanu
(Prof. Dr. Al. Obregia Clinic Hospital of Psychiatry,
(Titu Maiorescu University, Faculty of Medicine
Bucharest, Romania)
and Dental Medicine, Bucharest, Romania)
Prof. Univ. Dr. Vasile Astărăstoae
Prof. Univ. Dr. Elena Moldoveanu
(Gr. T. Popa University of Medicine and Pharmacy,
(Titu Maiorescu University, Faculty of Medicine
Iaşi, Romania)
and Dental Medicine, Bucharest, Romania)
Prof. Univ. Dr. Rumelia Koren
Prof. Univ. Dr. Adriana Stănilă
(Hasharon Hospital, Rabin Medical Center, Sackler
(Victor Papilian Faculty of Medicine, Lucian Blaga
School of Medicine, Tel Aviv University, Israel)
University, Sibiu, Romania)
Prof. Univ. Dr. Petru Armeanu
Prof. Univ. Dr. Maria Lidia Nica Udangiu
(Titu Maiorescu University, Faculty of Medicine
(Titu Maiorescu University, Faculty of Medicine
and Dental Medicine, Bucharest, Romania)
and Dental Medicine, Bucharest, Romania)
Prof. Univ. Dr. Ilie Constantin
Prof. Univ. Dr. Dan Florin Ungureanu
(Victor Babeş University, Faculty of Medicine,
(Titu Maiorescu University, Faculty of Medicine
Timişoara, Romania)
and Dental Medicine, Bucharest, Romania)
Prof. Univ. Dr. Gheorghe Ionel Comşa
Conf. Univ. Dr. Ghinescu Minerva
(Ovidius University, Constanţa, Romania)
(Titu Maiorescu University, Bucureşti, Romania)
Prof. Univ. Dr. Constantin Dumitru
Conf. Univ. Dr. Mircea Sorin Sabău
(Titu Maiorescu University, Faculty of Medicine
(University of Medicine and Pharmacy Târgu
and Dental Medicine, Bucharest, Romania)
Mureş, Romania)
Prof. Univ. Dr. Rivka Gal
Ş. L. Dr. Anca Ciurea
(Hasharon Hospital, Rabin Medical Center, Sackler
(Iuliu Haţieganu University, Faculty of Medicine,
School of Medicine, Tel Aviv University, Israel)
Cluj Napoca, Romania)
Prof. Univ. Dr. Doina Lucia Ghergic
As. Univ. Dr. Virgil Radu Enătescu
(Titu Maiorescu University, Faculty of Medicine
(Eduard Pamfil Universitary Clinic of Psychiatry,
and Dental Medicine, Bucharest, Romania)
Timişoara, Romania)
Te Medical Connections/Conexiuni Medicale® is indexed in Journals Master List of Index Copernicus®
B+ Category, Code 944
© Copyright Medical Connections/Conexiuni Medicale, Satu Mare, 2012
No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form or by
any means without prior permission in writing of Medical Connections/Conexiuni Medicale®. Permission is not
however required to copy abstracts of papers or of articles on condition that a full reference to the source is
shown. Correspondence regarding permission to reprint all or part of any article published in this journal
should be addressed to the Editor, e-mail: colmedsm@gmail.com
MEDICAL CONNECTIONS | CONEXIUNI MEDICALE
EDITORI ADJUNCŢI
EDITOR ŞEF
Blaga Vasile (versiunea electronică)
Koren Rumelia
Andó Ottó (versiunea tipărită)
EDITOR ŞEF ADJUNCT
Oană Cristian Sever (editorialist)
Bumbuluţ Călin
Tudor Stăncioiu (Medicina Dentară)
COMITET EDITORIAL
Bauer Adalbert (SCM West Satu Mare, România)
Kesler Gavriel (Israel)
Bidilean Nicolae (Spital Judeţean de Urgenţă, Satu Mare,
Kiss Ladislau (Spital Judeţean de Urgenţă, Satu Mare,
România)
România)
Boros Melinda (Bucureşti, România)
Mihalca Man Sorina (Spital Judeţean de Urgenţă,
Borcean Gheorghe (Spital Municipal Caransebeş, România)
Satu Mare, România)
Brândeu Ioan (Spital Judeţean de Urgenţă, Satu Mare,
Neumann Gad (Spital Hasharon, Tel Aviv, Israel)
România)
Negru Alina (SCM Satu Mare, România)
Cârstea Constantin (CMI Braşov, România)
Rath-Wolfson Lea (Spital Hasharon, Tel Aviv, Israel)
Cojocaru Manole (Universitatea Titu Maiorescu,
Rădulescu Viorel (CMI Olt, România)
Bucureşti, România)
Roatiş Marius Dinu (Spital Judeţean de Urgenţă,
Comăneanu Raluca Monica (Universitatea
Satu Mare, România)
Titu Maiorescu, Bucureşti, România)
Rusu Cristian Bogdan (Spital Judeţean de Urgenţă,
Cornean-Santa Corina (Spital Judeţean de Urgenţă,
Satu Mare, România)
Satu Mare, România)
Shvero Kesler Dana (Universitatea Hadassa,
Feciche Bogdan (Spital Judeţean de Urgenţă,
Ierusalim, Israel)
Satu Mare, România)
Trip Gheorghe (Spital Judeţean de Urgenţă,
Grosz Gyula (SCM West Satu Mare, România)
Satu Mare, România)
Gruzman Carlos (Hasharon Hospital, Tel Aviv, Israel)
Zilahi Karoly (SCM Praxis, Bixad, România)
Horber Orsolya (SCM Praxis Bixad, România)
Zeidman Aliza (Spital Hasharon, Tel Aviv, Israel)
Lup Liliana (Synevo Satu Mare, România)
Virag Tiberiu (CMI Satu Mare, România)
EDITOR
EDITOR ASOCIAT
Colegiul Medicilor Satu Mare
Asociaţia Medicilor de Familie Satu Mare
Satu Mare, P-ţa Eroilor Revoluţiei nr.23
Afiliată la Societatea Naţională de Medicina
Familiei/Medicină Generală
email: colmedsm@gmail.com
Satu Mare, str. Bobocului UK 30
PPARTENER
PARTENER EXTERN
Universitatea Titu Maiorescu Bucureşti
Hasharon Hospital, Rabin Medical Center
Facultatea de Medicină şi Medicină Dentară
Afiliat la Sackler School of Medicine, Universitatea Tel Aviv
str. Gheorghe Petraşcu 67A
7 Keren Kayemet St., Petah Tikva 49372, Israel
REDACŢIA
P-ţa Eroilor Revoluţiei nr 23, 440055, Satu Mare, Romania, Tel/Fax: 0261-710456, 0361-408164
ISSN online 2068 - 8369
ISSN 1843 - 9306
Revistă inclusă în Nomenclatorul Publicaţiilor Medicale ale CMR, 5 credite CMR pentru abonaţi
Indexare în Index Copernicus®, CNCSIS categoria B+, cod 944
Medical Connections/Conexiuni Medicale® este marcă înregistrată a Colegiului Medicilor Satu Mare şi a Asociaţiei Medicilor de Familie Satu Mare
Tipărit la TIPOOFFSET, str. Fabricii, Nr. 93-103, Cluj Napoca, Tel./Fax: 0264-456071
Contents
Editorial
6
Original Articles
Te Terapeutic Approach in Febrile Lithiasic Renal Colic-Single Center Experience
Lăpuşan Carmen, Crişan Nicolae, Cucu Vlad, Coman Ioan
9
Parent’s Attitude toward the Effectiveness of Sexual Education in Schools in the Arab Society
in Israel
Joubran Samia, Marcus Ohad, Iancu Iulian,Tova Hartman, Abraham Weizman, Rath-Wolfson Lea,
Ram Edward
15
Depressive Symptoms and Memory Disorder in Elderly
Popescu Cristina Maria, Ghiuru Rodica, Spiru Luiza, Stroe Felicia
23
Atherogenic Risk Quantification by Using the Atherogenic Index of Plasma (AIP) and
Cardiovascular Risk Calculator on Hypertensive Patients
Popa Călin, Puşchiţă Maria
29
Changes of Serum Pentosidine Levels in Patients with Rheumatoid Arthristis Stage I-II
Before Treatment
Cojocaru Manole, Ghinescu Minerva Claudia, Rusu Elena, Bălăeţ Constantin, Cojocaru Inimioara Mihaela
37
Te Sanogenic Role of Terapeutic Intervention for Firefighters
Popa Gabriela Sorina, Podea Delia, Puşchiţă Maria
41
General Review
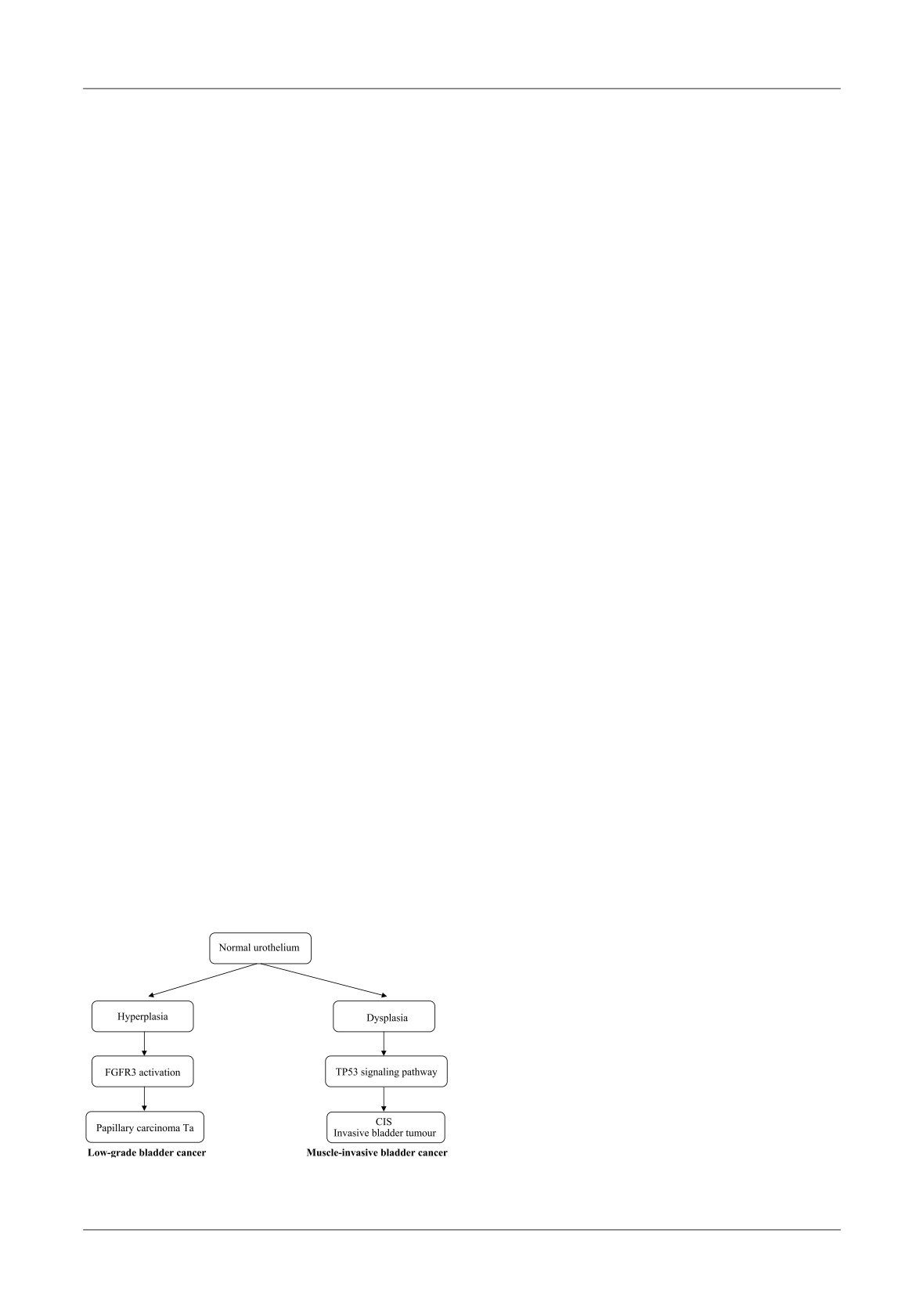
Relationship Between TP53 and FGFR3 Mutations in Superficial Bladder Cancer
Prunduş Paul, Stanca Vasile Dan, Nicolescu Sergiu, Coman Ioan
47
Etiology of Postoperative Astigmatism After Cataract Surgery
Pop Rodica, Pop Radu
53
News in Study of Optic Nerve Vascularization
Măgureanu Marineta, Stănilă Adriana, Stănilă Dan Mircea
59
Case Presentation
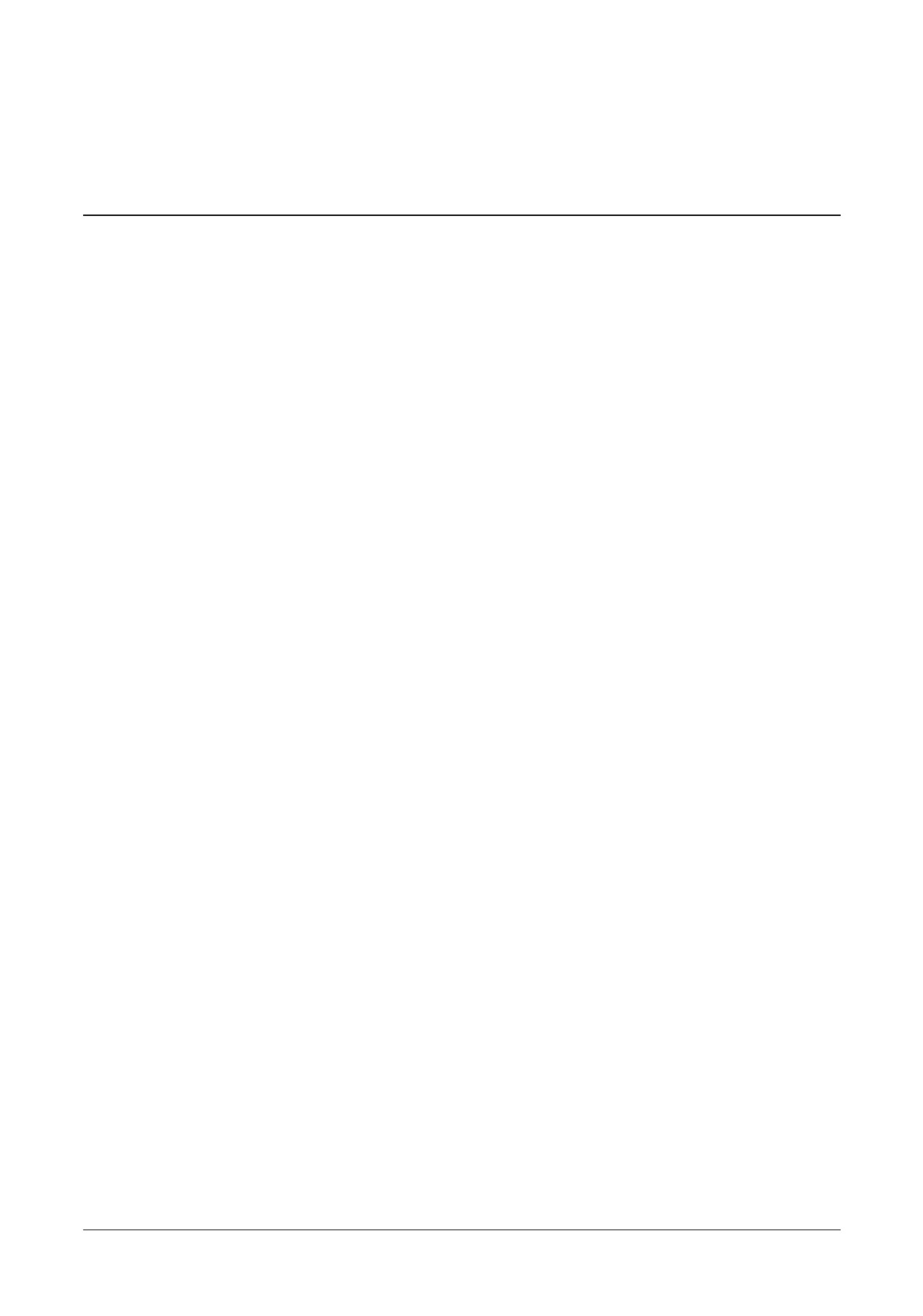
Desmoid Tumor Masquerading as Fibroadenoma. Case Report and Review of Literature
Hermann Naama, Fridel Ludmila, Grubstein Ahuva, Sharon Eran
67
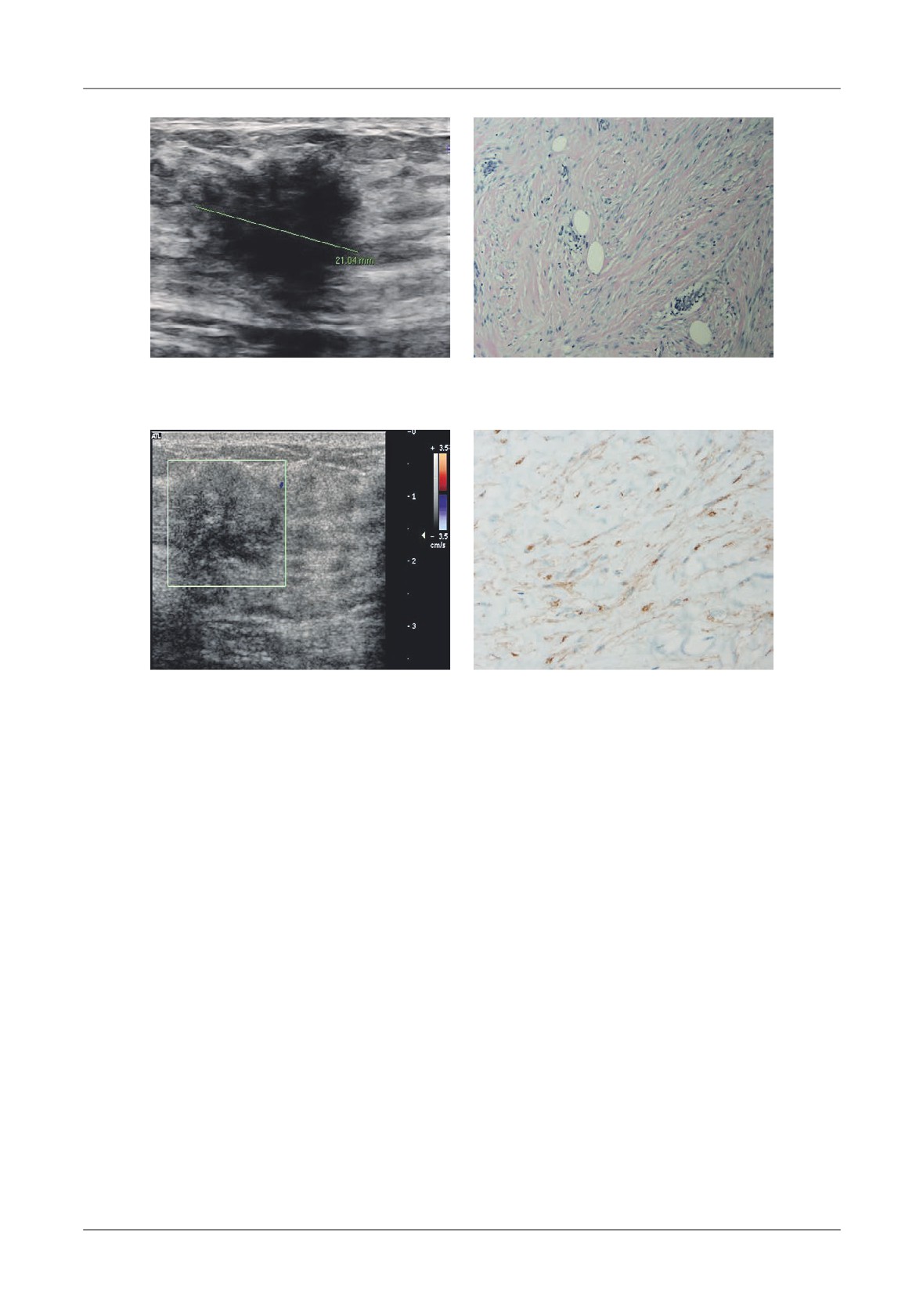
Metal Stents of the Ureter are they Innocent?
Stein Avi, Freifeld Yuval, Klein Ilan, May Tal, Muhad Yichie, Mecz Yoel, Goldin Dmitri, Faris Gazi,
Kaploun Alexander, Dekel Yoram
71
Editorial Appearance
Encyclopedia of Crisis Management
73
Guidance for Authors
75
Cuprins
Editorial
79
Articole originale
Rolul parametrilor bioumorali în stabilirea conduitei terapeutice la pacientul cu colică renală
febrilă litiazică
Lăpuşan Carmen, Crişan Nicolae, Cucu Vlad, Coman Ioan
81
Atitudinea părinţilor faţă de eficacitatea educaţiei sexuale în şcoli, în societatea arabă din Israel
Joubran Samia, Marcus Ohad, Iancu Iulian,Tova Hartman, Abraham Weizman, Rath-Wolfson Lea,
Ram Edward
87
Simptomele depresive şi tulburările memoriei la pacienţii vârstnici
Popescu Cristina Maria, Ghiuru Rodica, Spiru Luiza, Stroe Felicia
95
Cuantificarea riscului aterogenic folosind indexul aterogenic al plasmei (AIP) şi al riscului de boli
cardiovasculare la pacienţii hipertensivi
Popa Călin, Puşchiţă Maria
101
Variaţii ale nivelurilor de Pentozidină la pacienţi cu poliartrită reumatoidă în stadiul I-II înaintea
tratamentului
Cojocaru Manole, Ghinescu Minerva Claudia, Rusu Elena, Bălăeţ Constantin, Cojocaru Inimioara Mihaela
109
Rolul sanogenetic al intervenţiei terapeutice în cazul pompierilor salvatori
Popa Gabriela Sorina, Podea Delia, Puşchiţă Maria
113
Revistă generală
Relaţia dintre mutaţiile TP53 şi FGFR3 în cancerul vezical superficial
Prunduş Paul, Stanca Vasile Dan, Nicolescu Sergiu, Coman Ioan
119
Etiologia astigmatismului postoperator apărut după chirurgia cataractei
Pop Rodica, Pop Radu
125
Actualităţi în studiul vascularizaţiei nervului optic
Măgureanu Marineta, Stănilă Adriana, Stănilă Dan Mircea
131
Prezentare de caz
Tumoră desmoidă mascată ca fibroadenom. Prezentare de caz şi o revistă a literaturii
Hermann Naama, Fridel Ludmila, Grubstein Ahuva, Sharon Eran
139
Stenturile metalice ale ureterului au inocuitate?
Stein Avi, Freifeld Yuval, Klein Ilan, May Tal, Muhad Yichie, Mecz Yoel, Goldin Dmitri, Faris Gazi,
Kaploun Alexander, Dekel Yoram
143
Apariţie editorială
Enciclopedia managementului de criză
145
Eveniment medical
Invitaţie la Zilele Medicale Sătmărene ediţia a X-a, 4-6 octombrie 2013
147
Standarde de publicare
148
EDITORIAL
Drugged with food
Man digs his grave with his teeth
(Hindu Proverb)
In 1487, Giovanni II Bentivoglio, Bologna leader,
Greeks word leptos meaning weak. At the genetically
held a great banquet on the occasion of the wedding of
modified mice to which the leptin do not work became
his son Hannibal with Lucretia d’Este. Te feast lasted
quickly obese. A major health problem, obesity, seemed
seven hours, from 8 PM until 3 AM, during which they
to hold on to a simple defective feedback mechanism.
served: appetizers and cakes of soft paste with butter and
Unfortunately things started to get complicated at the
sweet wine, roasted pigeon, liver, thrushes, partridges
moment when it was discovered that leptin plays a role
with marinated olives and grapes, a sugar castle with
in addictive behavior. Heroin addict laboratory animals
battlements and towers full of live birds who have taken
suffer harder during withdrawal if they are also starved.
a flight when serving, a roast deer and ostrich surrounded
Probably satiety hormone suppresses not only the desire
by various pastries, veal loaf, boiled capons, chests and
for food but also for certain drugs. Anyone who has held
legs of calf, kids, sausages, pigeon with sauce, roasted
a diet knows how hard it is to give up old habits. Is
peacock adorned with their feathers in a wheel way,
obesity also a form of addiction? At first glance, no! A
mortadela (thick sausage baked and flavored with dill),
person who eats too much does not develop food
rabbits and deer served in baked sauce and dressed in
tolerance and those who are put on a diet do not
their skin that they seemed alive, doves and pheasants
experience withdrawal symptoms. At a closer look, we
from whose beak came out flames; citrus juices and
see that the obese have some signs of addiction: a strong
various sauces. Afterwards followed sugar cakes with
desire to eat and loss of self-control by neglecting other
almonds shaped in palaces from where have come out
needs. From neurobiological point of view the two
live rabbits, cheese and biscuits. Continued with whole
disorders are similar. Nerve fibers that go from trunk to
fried milk piglets and wild duck roasted. Finally they
accumbens nucleus secrete by abundance dopamine
brought milk and jelly sweets, pears, pasta, sweets,
whenever we live a surprise or pleasure, like an excellent
marzipan and other delicacies. All were accompanied by
meal. Similarly, cocaine and amphetamine increase
precious wines. As chronicler Cherubino Ghirardacci
dopamine levels in the accumbens nucleus ten times
told “before being put in front of banqueting guests,
triggering a wave of pleasure. Tis reward system
pieces were worn in the market with great honor around
controls the hypothalamus which in turn regulates
the palace ... to be shown to the people to see so much
eating behavior. Genetically modified mice that do not
greatness”.
produce dopamine simply have no desire to eat
Te first question you ask yourself, reading this
something and die by starvation. If they are injected
story, is who can eat so much? Italian Renaissance
with dopamine the appetite comes back.
portraits show some fit nobles who, like ordinary people
In 2001, Gene-Jack Wang of Brookhaven National
probably watched more than they ate. Even an obese
Laboratory and Nora Volkow from the National
would declare defeat by such a feast. Despite the enticing
Laboratory on Drug Abuse, confirmed the role of
images the body has control mechanisms that can block
dopamine in eating behavior. Using Positron Emission
the brain’s commands. Physiological mechanisms work
Tomography they measured the amount of dopamine
equally well in reverse: despite the decision to diet,
receptors in the striatum of overweight volunteers and
hunger can push us to the foolish gestures.
found that this correlates closely with body mass index.
In
1994, Jeffrey M. Friedman of Rockefeller
Like drug addicts, obese suffers from a relative lack of
University found that adipocytes secrete a protein that
dopamine, which forces them to search new satisfaction
cross the blood-brain barrier and reach the hypothalamus
in food. Excess dopamine, which so appears, reduce the
which suppresses hunger. He named it leptin from the
number of receptors as in cocaine case.
6
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
EDITORIAL
Kevin LaBar from Duke University studied
eating their favorite chocolate. Te brain activity
amygdala which is involved in arousal and emotional
increased both in the area associated with taste sensations,
response using Nuclear Magnetic Resonance. Nine
but especially in orbitofrontal region. Subjects continued
healthy subjects were asked to watch a series of pictures
to eat chocolate until they reached nausea. At that time
of food and cars and tools after starvation for 8 hours or
the center of activity in orbitofrontal area went in “OFF”,
respectively after a good meal. Amygdala of hungry
after that reappeared in side parts of the same area.
subjects immediately became active when they looked
All these experiments demonstrate that brain
to something edible. After lunch it no longer responded
processes stimuli related to food in the same way as
to images of food. Similar studies made on cocaine
other addictive stimuli. Control of feeding behavior
addicts at Emory University gave similar results. It seems
seems therefore to be considerable in obesity. Because it
that the amygdala acts as a buzzer alarm which sounds
can not be about will, it turned to drugs used for drug
whenever reveals something important for the survival
addicts. For example, naltrexone, an opioid antagonist,
of the organism, either a dangerous wolf or a rich meal.
led to the stop of weight gain. Rimonabant, an
Another brain region involved in addictive behavior
endogenous cannabinoid receptor blocker, helps to lose
is orbitofrontal cortex. Patients with lesions in this area
weight but only within certain limits. Drugs are not yet
can not control themselves, act impulsively and have
a solution, especially since we have no idea of their long-
some addictive behavior. Dana M. Small of Yale
term effect. For now we are limited to treating the
University showed that the orbitofrontal region processes
consequences of obesity such diabetes type 2, although
pleasure and aversion related to food. She studied
even here there are problems. Terefore I believe that
tomographic images from Positron Emission of
the best way to curb our appetite is to remember that
orbitofrontal cortex in nine subjects while they were
eating is the most primitive way to console us.
Sever Cristian Oană, MD
7
CENTER FOR DOCUMENTATION AND
CONTINUOUS MEDICAL EDUCATION
SATU MARE
The need to continue and enhance medical programs for the medical personnel from
the primary and secondary care network, as well as the social and comunity staff from the
health care centers in the county of Satu Mare, is a problem whose solution is the
development of the Documentation and Continuous Medical Education Center Satu
Mare. Satu Mare College of Physicians in partnership with the Association of Family
Physicians Satu Mare, the Dental College Satu Mare, wishes within this project to
continue the health educational programs in order to improve health services for
vulnerable social groups: disabled, social cases as well as for the population of Satu Mare
county.
Necesitatea continuării şi perfecţionării programelor de educaţie medicală a
personalului medical din reţeaua de asistenţă primară şi secundară, precum şi a
personalului de asistenţă socială şi comunitară din centrele de îngrijire ale judeţului Satu
Mare este o problemă a cărei soluţie este dezvoltarea Centrului de Documentare şi
Educaţie Medicală Continuă Satu Mare. Colegiul Medicilor Satu Mare în parteneriat cu
Asociaţia Medicilor de Familie Satu Mare, Colegiul Medicilor Dentişti Satu Mare,
doreşte în cadrul acestui proiect continuarea programelor educaţionale în domeniul
sănătăţii în vederea ameliorării serviciiilor de sănătate pentru grupurile sociale
vulnerabile: dizabilităţi, cazuri sociale, precum şi pentru populaţia judeţului Satu Mare.
Original articles
THE THERAPEUTIC APPROACH IN FEBRILE LITHIASIC RENAL
COLIC-SINGLE CENTER EXPERIENCE
Lăpuşan Carmen, Crişan Nicolae, Cucu Vlad, Coman Ioan
Department of Urology, Cluj-Napoca Clinical Hospital, “Iuliu Haţieganu”University of Medicine and Pharmacy,
Cluj-Napoca
Address for correspondence:
Lăpuşan Carmen, MD
11 Tăbăcarilor St., PO 400139, Cluj-Napoca, Cluj
Tel: 0745-316717
Email: carmenlapusan@yahoo.com
Received: 10.12.2012
Accepted: 15.02.2013
Med Con March 2013, Vol 8, No 1, 9-14
Abstract
Conclusions: Te febrile colic remains a urological
emergency. Te remission of the septic phenomena
Introduction: One of the most frequent urologic
during the first hours from the initiation of the
pathologies is represented by the febrile renal colic with
resuscitation therapy could be followed by the
an evolutionary potential to sepsis, in which case,
spontaneous passage of the calculus, particularly if it is
concurrently with the specific therapy of resuscitation,
located distally and has small size.
urinary diversion is considered to be obligatory.
Keywords: infected ureteral lithiasis, febrile renal
Objective: Te aim of this study is to evaluate the
colic, urinary diversion
clinical and bioumoral parameters, in order to establish
possible predictive values for the necessity of the urinary
Introduction
diversion in patients with febrile renal colic of lithiasic
origin.
Te high incidence of urosepsis is encountered both
Materials and Methods: Te present trial is a
in the urology departments and intensive care units,
prospective one and it includes all of the patients with
knowing that evolution and prognosis of septic patient
renoureteral lithiasis and febrile colic (above 38°C) who have
depend on early diagnosis and rapid treatment setting
come at the ED of the Municipal Hospital in Cluj, between
[1-3]. Te urosepsis diagnosis is based on clinical,
2010 and 2012. Te diagnosis and treatment protocols are
laboratory and imagistic criteria, but optimal time for
standardized. Te clinical parameters considered for the
the urologic intervention is still only relatively defined
evaluation are the following: age, sex, urosepsis stage,
[1,2,4]. One of the most common urologic pathology is
diabetes, active neoplasia, size and location of the renal
the febrile renal colic, potentially evolving to sepsis,
calculus, degree of hydronephrosis, urinary diversion.
situation where specific therapy of resuscitation is
Results: 142 patients were admitted for febrile renal
considered mandatory, concomitant with emergency
colic (above 38°C) through lithiasic obstruction between
diversion of the urinary tract [1,4,5]. Recent studies
2010-2012. Te decision to perform urinary drainage
have indicated a continuing increase in the incidence of
was significantly associated with the location and size of
the infected urolithiasis; practically, its value has doubled
the calculus (p<0.0001), the degree of hydronephrosis
in the past ten years. Te same upward trend has been
(p<0.0001) and the severity of urosepsis (p<0.0001).
observed in the association of urolithiasis with sepsis,
The Therapeutic Approach in Febrile Lithiasic Renal Colic-Single Center Experience
9
Original articles
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
but mortality rate has remained unchanged (0.2 to
as well as, the type of the germs responsible for the
0.25%) [6]. Currently, there is a set of nonspecific
septic condition and their sensibility towards antibiotics.
criteria that determines indication for urinary drainage
Te decision of performing the urinary diversion
in patients with renal colic: fever over 38°C, leukocytosis
was taken in conformity with the recommendations
with neutrophilia and persistent pain despite adequate
featured in the current EAU guidelines: fever above
analgesia. Tere are specific situations in which the
38°C, leukocytosis with neutrophilia and the persistence
positive evolution of the patient with febrile lithiasic
of pain for more than 24 hours in the context of using
colic was demonstrated, also in the absence of invasive
the adequate analgosedation. Te antibiotherapy and
procedures involving the diversion of the superior
the complementary therapy were both applied in a
urinary tract [2,7,8].
standardized way, pursuant to the current guidelines,
depending on the urosepsis stage, the type of suspected
Objectives
infection
(community acquired or nosocomial) and
previous antibiotic treatments. Te method of choice
Te aim of this study is to evaluate the clinical and
for urinary drainage in the context of infected
bioumoral parameters, both independently and in
renoureteral lithiasis, used in our clinic is the internal
association, in order to establish possible predictive
ureteral drainage in analgosedation and in case of failure,
values for the necessity of the urinary diversion in
the ultrasound-guided percutaneous nephrostomy in
patients with febrile renal colic of lithiasic origin. We
local anesthesia.
also offer comparative evaluation of the isolated
Te patients for whom the standard protocol of
pathogens and their susceptibility to antibiotics.
diagnosis and treatment was not pursued for different
reasons were excluded from the study; so were those
Materials and Methods
found in the situation in which the lithiasic origin of the
episode was not established.
Te present trial is a prospective one and it includes
Numerical data were either continuous or discrete.
all of the patients with renoureteral lithiasis and febrile
Discrete variables were characterized through frequencies
colic
(above
38°C) who have come at the First
(number and percent). Continuous values were
Emergency Department of the Municipal Hospital in
presented as means
± standard deviation
(SD).
Cluj-Napoca, between the 1st of April 2010 and the 31st
Comparison between groups was performed using the
of December
2012. Te diagnosis protocol is
Student’s t-test for continuous variables with normal
standardized and it includes the following steps: medical
distribution and the χ2 test for categorical variables. Te
history, objective examination, ultrasound exam, simple
differences between categories, in case of more than two
renovesical radiography and/or computed tomography,
categories, were tested using Kruskal-Wallis or ANOVA
laboratory tests (glycemia, renal and hepatic function,
method. P values < 0.05 were considered statistically
hemoleucogram, coagulogram, urinalysis, and urine
significant. Te MedCalc® 9.3.9.0.software was used for
culture). Te biologic samples were collected by
the analysis of statistical data.
qualified personnel and then analyzed in the accredited
laboratory of the hospital.
Results
Te clinical parameters considered for the evaluation
are the following: age, sex, urosepsis stage, diabetes,
142 patients were hospitalized for febrile renal colic
active neoplasia, size and location of the renal calculus,
(above
38°C) through lithiasic obstruction between
degree of hydronephrosis, urologic procedures
2010-2012, 99 (66.9%) of them being women and the
concerning the urinary tract.
other 47 (33.1%) men. Te age median was 51. Te
Te clinical and bioumoral parameters were
characteristics of the patients at the time of
dynamically analyzed (on arrival, after 12h, 24h and
hospitalization are summarized in Table I.
48h) but also in correlation with the time of urinary
A number of 56 patients (40%) presented a calculus
diversion, if this ever occurred. Tese parameters are:
under 4 mm and for 84 patients (60%) the dimension
body temperature, pulse, blood pressure, the number of
was over 4 mm. Approximately a third of the patients
leukocytes and the percent of neutrophils, urine analysis
(32.4%) eliminated the lithiasic fragment spontaneously,
and culture, renal function and last but not least, the
as for the rest of them a urinary diversion procedure was
urosepsis stage.
necessary, as it follows: in 82 of the cases (57.7 %) a
Moreover, the urinary drainage method was noted
ureteral stent JJ was insert endoscopic and in 14 of the
(spontaneous passage, ureteral stent JJ or nephrostomy)
cases (9.9%) a percutaneous nephrostomy was performed.
10
Lăpuşan et al
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
Original articles
Table I. Characteristics of the patients
at the time of hospitalization
Average,
Variable
SD, %
Age
51.16±16.17
Sex: F (nr, %)
95 (66.9)
M (nr, %)
47 (33.1)
Creatinine:
<1.4 (nr, %)
106 (74.6)
>1.4 (nr, %)
36 (25.1)
Te sepsis stage: SIRS
111 (78.1)
Sepsis
29 (20.4)
Severe sepsis
2 (1.4)
Leukocyturia: Absent
43 (30.3)
Present
99 (69.7)
Nitrites: Absent
106 (74.7)
Present
36 (25.3)
Hematuria: Absent
34 (23.9)
Figure 1. Location of calculi and procedure
Present
108 (76.1)
Urine culture: negative
78 (54.9)
simple germs
41 (28.9)
multiresistant germs
13 (9.1)
ESBL
10 (7.1)
Urinary pH
5.59±1.17
Leukocytes:
<4000
5 (3.5)
4000-10000
51 (35,9)
10000-20000
69 (48.5)
20000
17 (12.1)
Trombocytes:
<100000
9 (6.5)
100000-400000
118 (83.0)
>400000
15 (10.5)
Calculus location: Pyelic
30 (21.4)
Lumbar
45 (32.1)
Iliac
34 (23.3)
Juxtavesical
31 (22.1)
Calculus size:
<0.4mm
56 (40)
>0.4mm
84 (60)
Figure 2. Location of calculi and degree of hydronephrosis
Performed procedure: Spontaneous passage
46 (32.4)
Stent
82 (57.7)
Nephrostomy
14 (9.9)
Hospitalization days
4.13±2.7
Considering the stage of urosepsis, the majority of
Associated diabetes: No
98 (69)
the patients presented SIRS, only 31 patients (21.83%)
Yes
44 (31)
presented urosepsis out of which 2 cases featured severe
Associated neoplasia: No
130 (91.5)
urosepsis. Te persistence of fever, leukocytosis and
Yes
12 (8.5)
hydronephrosis after
12 hours of hospitalization
represented the criteria for the decision of performing
the emergency urinary diversion in most of the cases.
Te decision to perform urinary
drainage was
Te urinary diversion was performed in the first 6 hours
significantly associated with the location and size of the
of arrival for the patients admitted with clinical
calculus
(p<0.0001), the degree of hydronephrosis
symptoms of urosepsis and severe urosepsis. For the
(p<0.0001), the severity of urosepsis
(p<0.0001), the
patients with SIRS the urinary drainage was performed
value of seric creatinine (p=0.0037) and with the positive
at an average of 24 hours (12-48 hours) since admission.
results of the urine culture
(p=0.0087).
46 cases of
Tere were no cases of decease registered.
spontaneous passage of the calculus were registered, the
Two patients required ureterolithotomy open
majority of them presenting small size (41 cases - 89.13%)
surgery and pyelolithotomy respectively, performed in
and distal location (40 cases - 86.95%), Figure 1.
emergency due to complications arising after a failed
The Therapeutic Approach in Febrile Lithiasic Renal Colic-Single Center Experience
11
Original articles
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
Table II. Bacteriologic results, urine culture
Year/germ
2010 (37 pac/16 inf.)
2011 (44 pac/17 inf)
2012 (61 pac/31 inf)
Gram neg. total
11
15
23
G- multiresistent
-
2
6
G- ESBL
1
4
5
Gram poz. total
5
2
8
G+ multiresistent
1
-
4
attempt of ureteral stenting. Te curative surgery was
colic represents a urologic emergency but the optimal
scheduled and performed 14-21 days after the remission
time and the type of urinary deviation have not been
of the septic process for the 94 cases which underwent
defined yet [1,2,4]. Te urinary drainage for the septic
ureteral stent or nephrostomy diversion.
patient should be performed in the least invasive manner
Te location of calculi was significantly associated
[1,2,4]. Recently, in patients with renoureteral lithiasis
with the degree of hydronephrosis
(p=0.0001). Te
and infection, Sammon et al evaluated the 28.5% patients
degree of pyelocalicial dilatation was of major
who need a urinary diversion on the first day of
importance for the lumbar calculi, then for the iliac,
hospitalization and the fact that 70.1% out of them were
juxtavezical and pyelic ones, Figure 2.
women [6]. Te results recently published by Yamamoto
In cases of calculi with a diameter greater than 4
et al, on a group of 98 patients with obstructive PNA for
mm, their size were significantly associated with the
whom a urinary drainage was performed, indicate an
presence of leukocytes in urine (p=0.02) and positive
average of
3 days (0-38) from the beginning of the
urine culture (p=0.04), but also with the presence of
condition until the time of the urologic surgery [10]. Te
hydronephrosis degree II (p=0.001).
choice regarding urinary drainage (stent or nephrostomy)
Although by the time of admission, infection was
is still controversial; the ureteral JJ drainage is preferred in
suspected in
99 patients
(69.7%), objectification
the USA and EAU
[9,11] while in the U.K the
through the urine culture of the germs involved in the
percutaneous nephrostomy is performed in case of
occurrence of the septic process was done in 64 of the
ureteral obstruction accompanied by urosepsis [12].
cases
(45.07%). Out of those, in
49 of the cases
Sammon et al have recently emphasized the fact
(76.56%) Gram negative germs were involved the most
that the incidence of urinary lithiasis is higher in men
frequent was E.Coli in 35 of the cases (71.42%). Within
but lithiasis associated with infection is more frequent
the analyzed group, there were 10 cases of extended-
in women considering that its value has doubled
spectrum
beta-lactamase
(ESBL)
producing
between 1999-2009. Te same study indicates the fact
Enterobacteriaceae and 13 cases of multiresistant germs.
that emergency diversion is more frequent in women
Te ascending trend of these infections during those
who are more prone to develop urosepsis than men; the
three years can be observed. Te bacteriologic results
mortality was similar [6].
which were obtained are presented in Table II.
Regarding the treatment methods of the ureteral
Tere was no statistically significant correlation
calculi depending on location and size, several studies
between procedure and sex or age within the analyzed
show an increased rate (up to 80%) of the spontaneous
group.
passage for the calculi under 4 mm located in the distal
Te duration of hospitalization was significantly
ureter while the spontaneous elimination of the
correlated with the size of the calculus (p<0.001), the
proximal ureteral calculi with the same size occurs in
location of the calculus (p=0.001) but also with the
maximum 50% of the cases without specifying the time
degree of hydronephrosis (p<0.001) and the type of
until expulsion. Tough, these percentages decrease
procedure (p<0.0001).
with the increasing dimension of the ureteral calculi
[11-15]. In the context of associated urosepsis, in most
Discussion
cases, drainage of the urinary tract, by performing
invasive procedures with all the risks that they imply,
In the absence of a real marker, the diagnosis of
can’t be delayed by waiting for the spontaneous passage
urosepsis can only be done by considering nonspecific
of the calculus, even if its dimensions are small. Within
clinical criteria, some of these being caused either by
the analyzed group, there were 14 cases in which a stent
urosepsis or the acute pain felt in renal colic. Te febrile
was fixed for calculi under 4mm.
12
Lăpuşan et al
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
Original articles
Angulo et al, in their prospective study on 110
microbes requires the review of local protocols for
patients with renal colic secondary to upper urinary
antibiotherapy in concordance with the susceptibility of
calculi concluded that determination of CRP in patients
isolated microbes.
with renal colic due to urolithiasis provides an objective
and useful parameter for deciding placement of urinary
stent, which is even more valuable than leukocytosis or
seric creatinine level [16].
References
In terms of bacteriological results, emphasizing the
pathogenic agent in urine culture was possible only in
1.
European Association of Urology, Sepsis Syndrome in
45.07% of the cases, a lower percentage than the one for
Urology
(Urosepsis), Guidelines edition
2012.
urosepsis in general [1,3]. One of the explanations is the
existence of a complete urinary obstruction, as the
pdf/17_Urological%20infections_LR%20II.pdf
overlying purulent stasis could not be objectified after
2.
Wagenlehner FM, Pilatz A, Weidner W. Urosepsis-
the drainage since the patient was already taking
from the view of the urologist. Int J Antimicrob Agents
antibiotics [4].
2011;38 Suppl:51-7.
Schmudermaier M et al in their 6 years study
3.
Calandra T, Cohen J. International Sepsis Forum
concluded that there is a significant increase in resistance
Definition of Infection in the ICU Consensus Conference.
development for standard antibiotics in E. Coli urinary
Te international sepsis forum consensus conference
tract infections but no increase in ESBL resistance [17].
on definitions of infection in the intensive care unit.
In 2010, Hoban et al. find that the increasing resistance
Crit Care Med 2005;33:1538-48.
in Gram-negative bacilli isolated from hospital-acquired
4.
Coman I, Secasan I, Feciche B, et al. Infectiile tractului
infections worldwide has complicated empirical
urinar în Sinescu I, Gluck G, et al. Tratat de Urologie,
antimicrobial selection for these infections [18,19]. In
ediţia I, Editura Medicală, Bucureşti, 2008:875-932.
2008, Souli et al. in 2008 find that there is an increasing
5.
Naber KG, Schaeffer AJ, Heyns CF, Matsumoto T,
isolation of organisms with resistance to beta-lactam/
Shoskes DA, Bjerklund Johansen TE. International
beta-lactamase inhibitor combinations as well as
Consultation on Urogenital Infections. Stockholm,
carbapenem-resistant Enterobacteriaceae [19,20].
Sweden, March 2009 Urogenital Infections, EAU,
Te limitations of this study are drawn by the
edition 2010.
establishment of the threshold of 4mm for the calculi
6.
Sammon JD, Ghani KR, Karakiewicz PI. Temporal
for which a spontaneous passage is expected, although
Trends, Practice Patterns, and Treatment Outcomes for
in the medical literature, spontaneous eliminations for
Infected Upper Urinary Tract Stones in the United
the 5-7 mm up to 1 cm calculi are quoted. Within the
States. Eur Urol 2012;25. Available from URL: http://
analyzed group, there were 6 patients with calculi of
over 4 mm that were spontaneously eliminated. Another
S0302283812011037.
limitation of the study is the fact that the data obtained
7.
Angulo JC, Gaspar MJ, Rodríguez N, García-Tello A,
from patients with febrile colic is not compared with the
Torres G, Núñez C. Te value of C-reactive protein
data obtained from patients with renal colic and
determination in patients with renal colic to decide
infection, but without the clinical signs of sepsis.
urgent urinary diversion. Urology 2010;76:301-6.
8.
Matlaga BR. How Do We Manage Infected, Obstructed
Conclusions
Hydronephrosis? Eur Urol 2012;16. Available from
In the absence of a real marker for the urosepsis, the
pii/S0302283812012316.
febrile colic remains a urological emergency in the
9.
Ghani KR, Sammon JD, Trinh QD. Reply from
context of which alongside the resuscitation procedure a
Authors re: Brian R. Matlaga. How Do We Manage
drainage of the urinary tract is required. Te remission
Infected, Obstructed Hydronephrosis? Eur Urol. 2012 In
of the septic phenomena during the first hours from the
initiation of the resuscitation therapy could be followed
com/science/article/pii/S0302283812013309.
by the spontaneous passage of the calculus, particularly
10.
Yamamoto Y, Fujita K, Nakazawa S. Clinical
if it is localized distally and has small size. Tese
characteristics and risk factors for septic shock in patients
situations require careful monitoring and urinary
receiving emergency drainage for acute pyelonephritis
drainage if the clinical and bioumoral parameters urge
with upper urinary tract calculi. BMC Urol
for it. Te increasing incidence of the multiresistant
2012;13:12:4.
The Therapeutic Approach in Febrile Lithiasic Renal Colic-Single Center Experience
13
Original articles
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
11.
Türk C, Knoll T, Petrik A, Sarica K, Straub M, Seitz
17. Schmudermaier M, Lunacek A, Koenig U, et al.
C. Guidelines on urolithiasis. European Association of
Trends of Increasing Resistance of E. Coli and Non-
Significant Changes in Extended Spectrum Beta-
org/gls/pdf/20_Urolithiasis_LR%20March%20
Lactamase (ESBL) E. Coli in Urinary Tract Infections.
13%202012.pdf.
Urology 2011:S225.
12.
Lynch M, Anson K, Patel U. Percutaneous nephrostomy
18. Hoban DJ, Bouchillon SK, Hawser SP, Badal RE.
and ureteric stent insertion for acute renal deobstruction.
Trends in the frequency of multiple drug-resistant
Consensus based guidelines. Br J Med Surg Urol
Enterobacteriaceae and their susceptibility to ertapenem,
2008;1:120-5.
imipenem, and other antimicrobial agents: data from
13.
Preminger GM, Tiselius HG, Assimos DG,et al.
the Study for Monitoring Antimicrobial Resistance
EAU/AUA Nephrolithiasis Guideline Panel.
2007
Trends 2002 to 2007. Diagn Microbiol Infect Dis
guideline for the management of ureteral calculi. J Urol
2010;66:78-86.
2007;178:2418-34.
19. Hoban DJ, Nicolle LE, Hawser S, Bouchillon S,
14.
Tseng TY, Stoller ML. Medical and medical/urologic
Badal R. Antimicrobial susceptibility of global inpatient
approaches in acute and chronic urologic stone disease.
urinary tract isolates of Escherichia coli: results from the
Med Clin North Am 2011;95:169-77.
Study for Monitoring Antimicrobial Resistance Trends
15.
Graham A, Luber S, Wolfson AB. Urolithiasis in the
(SMART) program:
2009-2010. Diagn Microbiol
emergency department. Emerg Med Clin North Am
Infect Dis 2011;70:507-11.
2011;29:519-38.
20. Souli M, Galani I, Giamarellou H. Emergence of
16.
Angulo JC, Gaspar MJ, Rodríguez N, García-Tello A,
extensively drug-resistant and pandrug-resistant Gram-
Torres G, Núñez C. Te value of C-reactive protein
negative bacilli in Europe. Euro Surveill
2008;13.
determination in patients with renal colic to decide
urgent urinary diversion. Urology 2010;76:301-6.
org/ViewArticle.aspx?ArticleId=19045.
14
Lăpuşan et al
Original articles
PARENT’S ATTITUDE TOWARD THE EFFECTIVENESS OF SEXUAL
EDUCATION IN SCHOOLS IN THE ARAB SOCIETY IN ISRAEL
Joubran Samia1, Marcus Ohad2, Iancu Iulian3,8,Tova Hartman4, Abraham Weizman5,8, Rath-Wolfson Lea6,8,
Ram Edward7,8
1Te Bruce Rappaport Faculty of Medicine Technion-Institute of Technology and Emek Medical Center, 2Department of
Psychology, Te Yezreel Valley College, 3,8Te Yavne Mental Health Clinic, 4Department of Education and Gender Bar-
Ilan university Israel, 5,8Geha Mental Health Center, Petah Tikva, Israel, 6,8Department of Pathology, Hasharon Hospital,
Rabin Medical Center, 7,8Division of General Surgery, Hasharon Hospital, Rabin Medical Center, 8Sackler Faculty of
Medicine, Tel Aviv University
Address for correspondence:
Edward Ram
Division of General Surgery, Rabin Medical Center- Campus Golda
Petach Tiqva Keren Kaiemet St.7
Tel: 972-3-9372323, Fax: 972-3-9372401
E-mail: edwardrm@netvision.net.il
Received: 13.12.2012
Accepted: 15.02.2013
Med Con March 2013, Vol 8, No 1, 15-28
Abstract
today sexual education is better than in the past
(especially among the Christians parents).
Sexual education in Israel in general, and in the
We believe that the Arab community and
Arab sector in particular, has received almost no study.
Mediterranean culture, in which sexual intercourse and
Tis study aim was to find what do Israeli-Arab parents
sexual education are not trivial issues, has a great
think about the sexual education that their children get
influence on the parents, spite their will to become more
in school, in general and separately among Muslims and
modern. We also concluded that Christian Arabs lean
Christian parents.
more toward modernization and toward the
In order to address that question, 797 participants
individualistic end of the continuum than do Muslim
were asked five questions from a survey previously
Arabs, who are generally more strictly collectivist.
utilized by Blendon et al. Our results showed that most
Key word: parent’s attitudes, sexual intercourse,
parents (from both faiths, but mostly Christians) believe
Arab sector in Israel, Muslim and Christians
sexual education is very important, and that it greatly
influence avoiding sexual transmitted diseases, avoiding
Introduction
unwanted pregnancy, postponing sexual intercourse till
marriage and having good decision making about sexual
We are sexual human beings. From birth but during
intercourse and it has only partial influence on engaging
adolescence, sexual feelings change and intensify. Tose
sexual intercourse. In addition, we found that most
sexual feeling can add a vital dimension to the lives of
parents believe that sexual education teachers do not
adolescents. A dimension that has may positive
have sufficient preparation, that the sexual education
elements. Tere can be those wonderful and intense
only partial compatible to their values (especially among
feeling of being attracted to someone else, there can be
the Muslims parents) and that most parents believe
the opportunity for growth that comes from an intimate
Parent’s Attitude Toward the Effectiveness of Sexual Education in Schools in the Arab Society in Israel
15
Original articles
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
relationship with another person. Tese positive
Israel is a valuable resource for providing a multi
elements should not be forgotten or ignored [1].
religious approach to diverse issues. It represents a
Sexual health education is a controversial topic,
variety of religions, ethnic groups, cultures and
with perhaps no other subject sparking as much debate.
traditions. Te state of Israel has some
7.4 million
School administrators have identified fear of parental or
inhabitants. Te most prominent characteristic of
community opposition as major barriers to the provision
Israel’s population is its high diversity. Besides the main
of sexual health education [2,3].
division of the country’s inhabitants into Jews (80%)
Te school is the only institution in regular contact
and Arabs (20%), there are many more subdivisions
with a sizable proportion of the teenage population [4],
(Israel Central Bureau of Statistics, 2009). Statistics are
with virtually all youth attending it before they initiate
noteworthy considering that Muslims comprise about
sexual risk-taking behavior [5].
15% of the Israeli population, whereas Christians
Tere seems to be a growing consensus that school
comprise about 2% [17]. Cultural differences between
can play an important role in providing youth with a
Jews and Arabs in Israel drive the basic values of each
knowledge base which may allow them to make
sector due to the cultural affiliation derived from four
informed decision and help them shape a healthy
origins: ethnicity, language, religion, and nationality,
lifestyle [6].
Israeli
Christian and Muslim population are
Parents can have an important influence on their
characterized by substantial differences in values, beliefs,
children’s sexual behaviors. Studies indicate that
family formation, and sexual behavior patterns (Israel
supportive parent-child relationships and parental
Central Bureau of Statistics, 2009).
monitoring and supervision are associated with delayed
Subcultural differences exist within the Arab culture
sexual activity among children [7], in fact Parents are
between Christian and Muslim Arabs. Christian Arabs
not much involved in talking about sex-related issues,
lean more toward modernization and toward the
adolescents strongly express the wish that their parents
individualistic end of the continuum than do Muslim
could be the guide to sex knowledge [8,9]. Tey do
Arabs, who are generally more strictly collectivist. Te
understand this situation, and are aware of their
former generally have higher academic achievements
limitations, so they hope to obtain assistance from the
than do their Muslim Arab counterparts; more Christian
professionals in order to possess the ability to engage in
women study in higher education than do Muslim
parental sexuality education [10].
women; and the Christian schools are considered to be
Discussion of sexuality in the home is an important
among the best [18]. Differences are also apparent
component of students’ overall, sexual health education
within the Arab population itself, in line with gender
and school-based sexual health education can make it
differences and subcultural variation. Te education of
easier for parents to discuss sexuality with their child
daughters is stricter than that of sons, who are allowed
[11,12].
more exposure to the influences of modernization
Most parents believe that parents and schools
outside the home and who receive more autonomy from
should share responsibility for sexual health education.
their parents [19].
For example, McKay and coll. [13] found that most
Te Arab culture in Israel is distinguished by its
parents identified parents (88%), health professionals
traditional, homogeneous, and collectivist orientation,
(88%), and teachers (77%) as appropriate people to
despite undergoing a process of modernization
provide sexual health education in the school and
[20,21,22].
community.
People in a collectivist society tend to behave
Many authorities have long agreed that the most
according to the preferred collective common goals.
important factor in successful sexuality education
Tey tend to exhibit intimate relations among
program implementation is a well qualified and willing
themselves and remoteness from strangers and outsiders.
classroom teacher [14].
Collective harmony is valued above all [23].
Teacher characteristics, attitude, conception of self
Tis norm results in educating children to develop
and intellectual and interpersonal dispositions can
an external locus of control and conformity to an
influence both the explicit and the hidden curriculum
accepted image, while minimizing self-criticism
in the classroom [15].
(Barakat, 1993). For example, family status and honor
Teachers in New Brunswick have identified
led American Arab students to ignore their school
anticipated reactions from parents to the inclusion of
counselor (Courtland, 1997).
specific topics as the greatest barrier to their willingness
Arab society is still considered collectivist, and its
to teach sexual health education [16].
adolescents continue to emphasize their belonging to
16
Joubran et al
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
Original articles
the larger collective, while planning their individual
language specialist. From this questionnaire 3 questions
future [6,24].
were utilized
Te Israeli educational milieu, containing two
Te questions that guided this research are:
different cultures with separate educational systems,
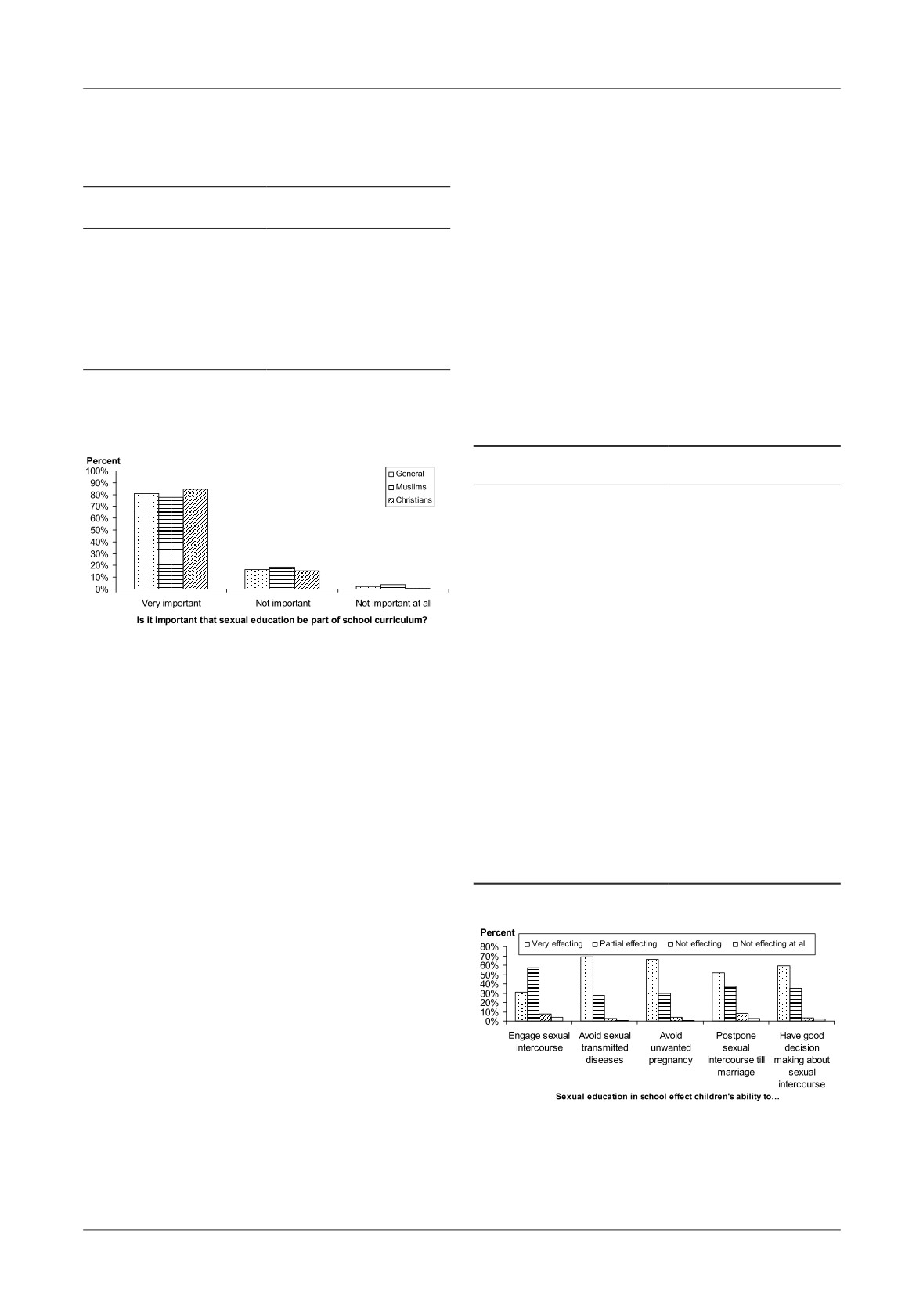
(1) Is it important that sexual education be part of
Arab teacher receive their primary through secondary
school curriculum?
education in the collectivist context of the Arab
(2) How does sexual education in school effect
educational sector, which includes Muslims and
children’s Ability to…
Christians, Tey study in their mother tongue, gain
A. Engage sexual intercourse?
some prior experiences with Western Israeli culture
B. Avoid sexual transmitted diseases?
[25].
C. Avoid unwanted pregnancy?
Te Ministry of Education in Israel is responsible
D. Postpone sexual intercourse till marriage?
for sex education in schools, so the ministry has
E. Have good decision making about sexual
numerous sex education curricula for each population
intercourse?
sector in Israel.
(3) Do sexual education teachers have sufficient
In 1996 the Ministry of Education published the
preparation?
first sex education program for Arab citizens. Tis
(4) How much the sexual education in school
program discussed family life education and sex
compatible to your values?
education aimed at imparting knowledge, skills, and
(5) How good is today sexual education in school
understanding of how to address the subject of sex. Te
compared with past sexual education?
program has 12 chapters of theoretical subjects and
Procedure
activities that include these topics: sex education and
Te questionnaires were provided to school
education for good family life, adolescence, the
administrators across the country, which sent them to
relationship between parents and adolescents, one’s
randomly selected parents from their schools. Te
body, decision making, friendship, prejudice, education
anonymously completed questionnaires were sent back
and assertiveness, peer pressure, tradition and habits,
to the investigators by mail. Out of 1,000 questionnaires
AIDS and sexually transmitted disease [26].
797 were returned, for a response rate of 79.7%, which
Te above program is designed to start in
is a high response rate for Arab community.
kindergarten and end in high school, but in reality
pupils learn only 45 minutes at the elementary school
Results
level.
Tis study aim is to find what do Israeli-Arab
First we wanted to know is it important that sexual
parents think about the sexual education that their
education be part of school curriculum?
children get in school, in general and separately among
We found that 81.1% of the parents believe it is
Muslims and Christian parents.
very important that sexual education be a part of the
school curriculum, 16.6% believe it is not important
Research Methodology
that sexual education be a part of the school curriculum
and only 2.3% believe it is not important at all that
Participants
sexual education be a part of the school curriculum.
Participants were 797 Israeli-Arab parents from all
Tere was also a significant difference between
over Israel whose age range was between 20 and 66
Muslim and Christian parents in the importance of
(M=39). Among them were 371 Christians and 426
sexual education as part of the school curriculum
Muslims, 208 males and 589 females; 533 live in cities
[U(787)=71311.5, p<0.01], so that Muslim parents
and 264 in rural areas or villages; 483 academics and
believe that sexual education be part of school
314 non-academics. In addition, 545 of the participants
curriculum (M=380.10) is less important than Christian
defined themselves as secular or traditional and 252
parents believe (M=409.74).
defined themselves as religious or very religious.
Table I and Figure 1 summarize the above results.
Questionnaires
We wanted to know how does sexual education in
Te study drew on questionnaires developed by
school effect children’s ability to engage sexual
Blendon (2004) that consisted of 42 multiple-choice
intercourse, to avoid sexual transmitted diseases, to
questions that examine a parent’s attitude toward sex
avoid unwanted pregnancy, to postpone sexual
education. Te questionnaire was translated into Arabic
intercourse till marriage and to have good decision
(two-way translation) and was proofed by an Arab
making about sexual intercourse.
Parent’s Attitude Toward the Effectiveness of Sexual Education in Schools in the Arab Society in Israel
17
Original articles
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
Table I. Percents of parents believe it is important that
Tere was no differences between Muslim and
sexual education be part of school curriculum,
Christian parents in the effecting of sexual education in
in general and divided into religion
school on children’s ability to engage sexual intercourse
[U(593)=43652.5, n.s.], to avoid sexual transmitted diseases
General percent
[U(773)=71308, n.s.], to avoid unwanted pregnancy
Muslim
Christian
[U(758)=70864, n.s.], to postpone sexual intercourse till
Very important - 81.1%
marriage [U(766)=68142, n.s.] and to have good decision
Not important - 16.6%
Not important at all - 2.3%
making about sexual intercourse [U(753)=68042.5, n.s.].
Very important - 77.8%
Very important - 84.8%
Tables II and Figure 2 summarize the above results.
Not important - 18.4%
Not important - 14.6%
Not important at all - 3.8% Not important at all - 0.5%
Table II. Percents of parents believe sexual education in
***U(787)=71311.5
school effect children’s ability to engage sexual intercourse,
to avoid sexual transmitted diseases, to avoid unwanted
****p<0.05
***p<0.01
**p<0.005
*p<0.001
pregnancy, to postpone sexual intercourse till marriage and
to have good decision making about sexual intercourse
Sexual education in school
effect children’s ability to…
Engage sexual intercourse
Very effecting - 31.0%
Partial effecting - 57.3%
Not effecting - 7.4%
Not effecting at all - 4.2%
Avoid sexual transmitted
Very effecting - 69.2%
diseases
Partial effecting - 27.7%
Not effecting - 2.6%
Not effecting at all - 0.5%
Figure 1. Percents of parents believe it is important that
Avoid unwanted pregnancy
Very effecting - 66.1%
sexual education be part of school curriculum, in general
Partial effecting - 29.7%
and divided into religion
Not effecting - 3.8%
Not effecting at all - 0.4%
Postpone sexual intercourse
Very effecting - 51.7%
till marriage
Partial effecting - 37.5%
We found that 31% of the parents believe sexual
Not effecting - 8.1%
education in school very effecting on children’s ability to
Not effecting at all - 2.7%
engage sexual intercourse,
57% believe it is partial
Have good decision making
Very effecting - 59.4%
effecting, 7.4% believe it is not effecting and 4.3% believe
about sexual intercourse
Partial effecting - 35.1%
it is not effecting at all; 69.2% of the parents believe sexual
Not effecting - 3.7%
education in school very effecting on children’s ability to
Not effecting at all - 1.9%
avoid sexual transmitted diseases,
27.7% believe it is
partial effecting, 2.6% believe it is not effecting and 0.5%
believe it is not effecting at all; 66.1% of the parents
believe sexual education in school very effecting on
children’s ability to avoid unwanted pregnancy, 29.7%
believe it is partial effecting, 3.8% believe it is not effecting
and 0.4% believe it is not effecting at all; 51.7% of the
parents believe sexual education in school very effecting
on children’s ability to postpone sexual intercourse till
marriage, 37.5% believe it is partial effecting, 8.1% believe
it is not effecting and 2.7% believe it is not effecting at all;
and finally 59.4% of the parents believe sexual education
Figure 2. Percents of parents believe sexual education in
in school very effecting on children’s ability to have good
school effect children’s ability to engage sexual intercourse, to
decision making about sexual intercourse, 35.1% believe
avoid sexual transmitted diseases, to avoid unwanted
it is partial effecting, 3.7% believe it is not effecting and
pregnancy, to postpone sexual intercourse till marriage and to
1.9% believe it is not effecting at all.
have good decision making about sexual intercourse
18
Joubran et al
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
Original articles
We asked the parents do sexual education teachers
Finally, we asked the how good is today sexual
have sufficient preparation?
education in school compared with past sexual
We found that while 28.5% of the parents do
education?
believe sexual education teachers have sufficient
We found that 70.9% of the parents believe today
preparation 71.5% of them believe sexual education
sexual education is better than in the past, 18.7% of the
teachers do not have sufficient preparation.
parents believe today sexual education is the same as in
Tere was no significant correlation between parents
the past and only 10.4% of the parents believe today
religion and their believe about the sexual education
sexual education is worse than in the past.
teachers sufficient preparation [2χ(1)=1.45, n.s.].
Tere was also a significant difference between
We asked the parents how much the sexual
Muslim and Christian parents in the compatible of
education in school compatible with their values?
sexual education in school to their values [U(635)=48928,
We found that 28.2% of the parents believe sexual
p<0.05], so that Muslim parents believe that today
education in school very compatible to their values, 58.7%
sexual education is better than in the past (M=338.59)
believe it is partial compatible, 9.6% believe it is not
less than Christian parents believe (M=313.92).
compatible and 3.5% believe it is not compatible at all.
Table IV and Figure 4 summarize the above results.
Tere was also a significant difference between
Muslim and Christian parents in the compatible of
Discussion
sexual education in school to their values
[U(635)=44650.5, p<0.01], so that Muslim parents
Education is an intentional structured process to
believe that sexual education in school is less compatible
impart knowledge and skills and to influence an
to their values
(M=302.18) than Christian parents
individual’s developmental course [27]. Sex education
believe (M=336.59).
enables people to acquire knowledge and develop skills
Table III and Figure 3 summarize the above results.
that they can use to protect themselves and others [28].
Table III. Percents of parents believe sexual education
Table IV. Percents of parents believe about today sexual
in school compatible to their values, in general
education in school compared with past sexual education,
and divided into religion
in general and divided into religion
General percent
General percent
Muslim
Christian
Muslim
Christian
Very compatible - 28.2%
Today better than in the past - 70.9%
Partial compatible - 58.7%
Te same - 18.7%
Not compatible - 9.6%
Today worse than in the past - 10.4%
Not compatible at all - 3.5%
Today better than in the
Today better than in the
Very compatible - 24.8%
Very compatible - 32.2%
past - 66.9%
past - 75.9%
Partial compatible - 59.5%
Partial compatible - 57.9%
Te same - 23.3%
Te same - 12.9%
Not compatible - 10.8%
Not compatible - 8.2%
Today worse than in the
Today worse than in the
Not compatible at all - 5.0% Not compatible at all - 1.7%
past - 9.7%
past - 11.2%
*** U(635)=44650.5
****U(635)=48928
****p<0.05
***p<0.01
**p<0.005
*p<0.001
****p<0.05
***p<0.01
**p<0.005
*p<0.001
Figure 3. Percents of parents believe sexual education in school
Figure 4. Percents of parents believe about today sexual
compatible to their values, in general and divided into religion
education in school compared with past sexual education,
in general and divided into religion
Parent’s Attitude Toward the Effectiveness of Sexual Education in Schools in the Arab Society in Israel
19
Original articles
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
In our study most of the parents believes that it is
their values, Muslim parents believe that sexual
very important for sexual education to become a part of
education in school is less compatible to their values
school curriculum, there was also a significant difference
than Christian parents believe.
between Muslim and Christian parents, for the
Many Arabs Muslims, parents and even young
Christians the inclusion of sexual education in the
people, are very concerned both about current methods
curricula is more important than for Muslims.
of sex education and about values which laid behind
Many of the psychosocial aspects of sexuality, such
them, some of the opposition is based on a
as sexual attitudes, have been relatively unexplored in
misunderstanding or misrepresentation of current
diverse ethnic groups. Tere is much reason to believe
practice in sex education [18]. Ashraf [35] claimed that
that ethnic groups differ in sexual values, considering
the basis for sex education in schools in the secular
the disparate cultural, political, historical, and
system of education is purely physical without any
socioeconomic factors that influence sexuality in each
spiritual and moral dimensions. Christian Arabs lean
group [29]. Among the 69% of public schools that
more toward modernization and toward the
provide district-wide sexuality education,
14% treat
individualistic end of the continuum than do Muslim
abstinence as an option for adolescents,
51% teach
Arabs, who are generally more strictly collectivist [18].
abstinence as the preferred option for adolescents but
About 71% of the parents in our study believe that
permit discussion about contraception as an effective
sexual education today is much better than in the past,
means of protection against unintended pregnancy and
the Muslims believe that today sexual education is less
STDs and more than 1 in 3 (35%) teach abstinence
good than in the past, in contrast the Christian parents
only, with discussion of contraception prohibited or
believe that today is much better.
limited to discussion of its lack of effectiveness [30].
Arab teacher receive their primary through secondary
Religion play an important role in socialization by
education in the collectivist context of the Arab
inculcating in children the norms, values of the society
educational sector, which includes Muslims and
and provides guides about what is right and what is
Christians. Tey study in their mother tongue, gain
wrong in the society [31].
some prior experiences with Western Israeli culture [25].
All the parents that participated in this study from
Because of teachers in the Arab community received
both faiths believe that sexual education in school
their education in the collectivist context, the majority of
partially affect the children’s ability to engage in sexual
participated parents in our study believe that sexual
intercourse, most of the parents believe that sexual
education teachers do not have appropriate preparation.
education in school is very affecting children’s ability to
avoid sexual transmitted diseases, unwanted pregnancy,
Conclusion
good decision making about sexual intercourse and
postpone sexual intercourse till marriage.
Te aim of this study was to find what do Israeli-
Abstinence-only programs have not demonstrated
Arab parents think about the sexual education that their
successful outcomes with regard to delayed initiation of
children get in school, in general and separately among
sexual activity or use of safer sex practices. Effective
Muslims and Christian parents.
programs tend to provide practical skills, such as
We found that most parents (from both faiths, but
exercising control and increasing communication and
mostly Christians) believe sexual education is very
negotiation skills through role playing or interactive
important, and that it greatly influence avoiding sexual
discussion [32]. Programs that encourage abstinence as
transmitted diseases, avoiding unwanted pregnancy,
the best option for adolescents, but offer a discussion of
postponing sexual intercourse till marriage and having
HIV prevention and contraception as the best approach
good decision making about sexual intercourse and it
for adolescents who are sexually active, have been shown
has only partial influence on engaging sexual intercourse.
to delay the initiation of sexual activity and increase the
In addition, we found that most parents believe that
proportion of sexually active adolescents who reported
sexual education teachers do not have sufficient
using birth control
[33]. Programs that have linked
preparation, that the sexual education only partial
educational curricula with access to reproductive health
compatible to their values
(especially among the
services
and comprehensive community-based
Muslims parents) and that most parents believe today
interventions have also documented reductions in
sexual education is better than in the past (especially
pregnancy rates [34].
among the Christians parents).
Most of the parents in current study believe that
We believe that the Arab community and
sexual education in school partially compatible with
Mediterranean culture, in which sexual intercourse and
20
Joubran et al
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
Original articles
sexual education are not trivial issues, has a great
9.
Warren C, Neer M. Family sex communication
influence on the parents, spite their will to become more
orientation. Journal of Applied Communication
modern. We also concluded that Christian Arabs lean
Research, 1986;14:86-107.
more toward modernization and toward the
10.
Alter JS, Baxter S, Cook AT, Kirby D., Wilson P.
individualistic end of the continuum than do Muslim
Teaching Parents to be the Primary Sex Educators of
Arabs, who are generally more strictly collectivist.
Teir Children. Bethesda, Md: Mathtech, 1982.
Our research is among the few studies conducted
11.
Berne LA, Patton W, Milton J, Hunt LYA, Wright S,
on sex education in general and Arab society in
Peppard J, Dodd J. A qualitative essessment of
particular. Tis is among the first studies that examines
Australian parents’ perceptions of sexuality education
the differences between Christians and Muslims, and
and communication. Journal of Sex Education and
among the first to examine in-depth the subject of
Terapy, 2000;25:161-8.
sexual education in the Israeli-Arab society. Our study
12.
Parcel GS, Coreil J. Parental evaluations of a sex
has contributed significantly to sex education in Arab
education course for young adults. Journal of School
society in general, and in particular, it highlights the
Health, 1985;55:9-12.
similarities that exist within this society.
13.
McKay A, Pietrusiak M, Holowaty P. Parents’opinions
Acknowledgment: to Abhath
- Te Society for
and attitudes toward sexuality education in the schools.
Developing Academic Research for her support and help
Te Canadian Journal of Human Sexuality,
caring out this study.
1998;7:139-45.
14.
Ryan IJ, Dunn PC. Sex education from prospective
teachers’ view poses a dilemma. Journal of School
Health,
1979;49(10),573-5.20. Al-Haj M. Te
References
changing Arab kinship structure: Te effect of
modernization in an urban community. Economic
1.
Kirby D, Short L, Collins J, Rugg D, Kolbe L,
Developmental Cultural Change, 1988;36(2):237-58.
Howard M, Miller B, Sonenstein F, Zabin L. School-
15.
Wenzlaff TL. Dispositions and portfolio development: Is
based programs to reduce sexual risk behaviors: a review
there a connection? Education, 1998;118(4):564-9.
of effectiveness. Public Health Rep, 1994;109(3):339-
16.
Cohen JN, Byers ES, Sears HA, Weaver AD. New
60.
Brunswick Teachers’ Ideas About Sexual Health
2.
Reis J, Seidl A. School administrators, parents, and sex
Education.
2001, Fredericton, New Brunswick:
education: A resolvable paradox? Adolescence,
University of New Brunswick, Department of
1989;24:639-45.
Psychology.
3.
Scales P, Kirby D. Perceived barriers to sex education: A
17.
Trumbull CP. (Ed.) Britannica Book of the Year.
survey of professionals. Journal of Sex Research,
Chicago, 2001, Encyclopaedia Britanica.
1983:19:309-26.
18.
Swirski S. Education in Israel: Schooling for Inequality.
4.
Zabin L, Hirsch M.
(). Evaluation of Pregnancy
1990,Tel-Aviv, Israel: Breirot.
Prevention Programs in the School Context.
1988,
19.
Jarrous-Absawy G. Relationships Between Parents and
Lexington, MA: Lexington Books.
Adolescents as a Function of Culture and Values.
5.
Kirby D, Coyle K. School-based programs to reduce
Unpublished master’s thesis, University of Haifa,
sexual risk-taking behavior. Children and Youth
Israel, 1999.
Services Review, 1997;19,415-39. 24. Al-Haj M. Te
20.
Lehrer EL. Religion as a Determinant of Economic and
Arab Teacher in Israel: Status, Questions, Expectations.
Demographic Behavior in the USA. Population
Haifa, Israel: University of Haifa, Center for
Development Review, 2004;30(4):707-26.
Multiculturalism and Educational Research 1995.
21.
Al-Haj M. Social research on family life styles among
6.
Seginer R. Adolescents facing the future: Cultural and
Arabs in Israel. Journal of Comparative Family
socio-political perspectives. Youth and Society,
Studies, 1989;20(2):175-95.
1988;19:314-33.
22.
Florian V, Mikulincer M, Weller A. Does culture affect
7.
Miller BC, Benson B, Galbraith D. Family
perceived family dynamics? A comparison between Arab
relationships and adolescent pregnancy risk: A research
and Jewish adolescents in Israel. Journal of Comparative
synthesis. Developmental Review, 2001;21:1-38.
Family Studies, 1993;24(2):189-201.
8.
Fisher TD. Parent-child communication about sex and
23.
Triandis HC, McCusker C, Hui CH. Multimethod
young adolescents sexual knowledge and attitudes.
probes of individualism and collectivism. Journal of
Adolescence 1986;2(83):517-28.
Personality and Social Psychology, 1990;59:1006-20.
Parent’s Attitude Toward the Effectiveness of Sexual Education in Schools in the Arab Society in Israel
21
Original articles
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
24.
St Leger L. Te opportunities and effectiveness of the
Sexual and Reproductive Health, New York: Plenum,
health promoting primary school in improving child
2002,pp. 71-92.
health - a review of the claims and evidence. Health
30. Landry DJ, Kaeser L, Richards CL. Abstinence
Education Research, 1999:14,51-69.
promotion and the provision of information about
25.
Eilam B. Passing Trough a Western-Democratic
contraception in public school district sexuality education
Teacher Education: Te Case of Israeli Arab Teachers.
policies. Family Plann Perspect, 1999;31:280-6.
Teachers College Record, 2002;104:1656-701.
31. Tornton A, Camburn D. Religious Commitment and
26.
Israel Ministry of Education, 1996.
Adolescent Sexual Behavior and Attitudes. Journal of
27.
Schneewind KA, Socialization and Education:
Marriege Family, 1994;51(3):641-53.
Teoretical perspective, in: Smelser NJ, Baltes PB
32. Frost JJ, Forrest JD. Understanding the impact of
(eds.), International Encyclopedia of Social and
effective teenage pregnancy prevention programs. Family
Behavioral Sciences, Amsterdam: Elsvier
2001,pp
Plann Perspect, 1995;27:188-95.
14507-13.
33. Zabin LS, Hirsch MB, Streett R, et al. Te Baltimore
28.
Beyth-Marom R, Fischhoff B. Adolescents’ Decisions
pregnancy prevention program for urban teenagers. How
about Risks: A cognitive perspective, in: T. Schulenberg,
did it work? Family Plann Perspect, 1988;20,182-
J. Maggs & K. Hurrelmann (eds.), Health Risks and
7.35. Ashraf SA. Editorial: the Islamic concept of sex as
Developmental Transition During Adolescence,
the basis of sex education, Muslim Education Quarterly,
Cambridge: University press, 1997,pp 110-35.
1996;13:1-3.
29.
Amaro H, Navarro A, Conron K, Raj A, On C.
34. Vincent ML, Clearie AF, Schluchter MD. Reducing
Cultural influences on women’s sexual health, in R. J.
adolescent pregnancy through school and community-
DiClemente & G. M. Wingood (Eds.), Women’s
based education. JAMA, 1987;257:3382-6.
22
Joubran et al
Original articles
DEPRESSIVE SYMPTOMS AND MEMORY DISORDER IN ELDERLY
Popescu Cristina Maria1, Ghiuru Rodica2, Spiru Luiza3, Stroe Felicia4
1C.M.I. at Tudor Vladimirescu Monastery, Galaţi county, 2Te fifth Medical Clinic of Geriatrics and Gerontology, C.F.R.
Hospital, Iaşi, “Gr. T. Popa” University of Medicine and Pharmacy, Iaşi, Romania, 3“Carol Davila” University of Medicine
and Pharmacy, Bucharest, Romania, 4National Institute of Public Health, Bucharest, Romania
Address for correspondence:
Cristina Maria Popescu, MD
1300, C.M.I. Tudor Vladimirescu Monastery, 807295, Galati county, Romania
Phone 0040766774026
E-mail: popescucristinamaria@yahoo.com
Received: 05.01.2013
Accepted: 15.02.2013
Med Con March 2013, Vol 8, No 1, 23-28
Abstract
Conclusions: Findings suggest that elderly with
dysthymia or severe depression, especially of early onset
Background: Growing evidence suggests depression
need to be monitored closely for adverse outcomes, such
as an important risk factor for developing
as development of dementia and worsening symptoms.
neurodegenerative disease later in life.
Future studies should determine whether treatment of
Objective: Correlation of untreated depressive
depressive spectrum disorders may reduce the risk of
symptoms with risk of developing dementia in a
these outcomes.
retrospective study and a group of elderly patients.
Keywords: depressive symptoms, age-related
Methods: Te history of depression was ascertained
memory disorder, dementia of Alzheimer type, elderly
from the personal files of a number of 73 women aged
patients
between 70 and 90 years, registered in the general
practice. Baseline depressive symptoms were assessed
Introduction
with the Geriatric Depression Scale. Alzheimer disease
and mild cognitive impairment were diagnosed
Depression is encountered in 30% [1] up to 50% or
according to Diagnostic and Statistical Manual of
more [2] from the patients with Alzheimer’s disease
Mental Disorders criteria.
(AD), and is commonly reported in people with Mild
Results: A total of 17 women had a history of
Cognitive Impairment (MCI), which is the early, but
depression (9 with an onset<60 years and 8 with a late-
abnormal, state of cognitive impairment [3]. People
onset>60 years). Depression incidence of any type was
who experienced depressive episodes at an earlier age
significantly higher in patients with AD than in those
would be more likely to develop AD than those who
free of this impairment
(85.71% face to
16.67%,
never faced them
[4]. Usually associated with the
p=0.0001,
95%CI:
3.1336-9.5204, RR=5.462).
reduction of physical activity and social interaction,
Dementia incidence was: 23.53% in people with severe
depression is a risk factor for altered health, altered life
depression, 14.29% in those with less severe depression
quality and death. It is not clear if depression is a
(dysthymia) and 5.36% in those with neither 12.33%
symptom of AD or a cause for it [5,6]. Several studies
in those with early onset, i.e. <60 years, and 10.96% in
pointed out that a history of major depression may
those with late onset, i.e. >60 years.
nearly double the risk of developing dementia later in
Depressive Symptoms and Memory Disorder in Elderly
23
Original articles
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
life
[5,6] and that people with more depressive
Measures
symptoms at baseline show an increased incidence of
Depressive Symptoms
MCI and AD with the lapse of time. It is not known,
History of depressive symptoms was taken from the
whether depression is as an early sign of dementia,
personal files of participating people present depressive
demonstrated by a higher incidence of depression prior
symptoms were investigated. Depressive symptoms were
to diagnosis or changes of depressive symptoms during
assessed with the 30-item Geriatric Depression Scale
disease progression. Te results are non-significant [5,6].
Yesavage [8] at baseline. Respondents indicated whether
However, depression should not be viewed as an
or not they had specific depressive symptoms
(e.g.
inevitable part of AD, but depressive symptoms may be
decreased activity/interest, hopelessness) or conditions
associated with specific brain changes that may reduce
that suggest the absence of depression (ex. extra energy,
the neuronal reserve, so that depression must be carefully
thought that life is wonderful), type the answers YES/
treated
[5,6]. Antidepressant therapy improves AD
NO. Respondents indicate whether or not they have
symptoms and patients’ quality of life, but does not slow
experienced particular depressive symptoms
(e.g.
AD progression, if both diseases are present. In
dropping activities/interests, feeling hopeless) or states
pseudodementia
(i.e. impaired cognition as clinical
suggesting an absence of depression
(e.g. feeling
expression of depression) where memory impairment is
energetic, thinking that being alive is wonderful) using a
caused by depression, the antidepressive treatment may
yes/no format. Responses suggesting depression were
improve cognitive functioning
[7]. Terefore, a
summed, and scores of 11 or more were considered for
physician should always search for depression when
suggesting probable depression. Severe depression was
treating the elderly with cognitive disorders, including
considered starting with a score of 21, between 11 and
cognitive impairments developed over a short period of
21, patients were considered to have rather light
time and mild cognitive impairment. A better
depression or dysthymia.
understanding of depression may lead to the discovery
Depression and dysthymia were identified by using
of new pathways in preventing Alzheimer’s disease [5,6].
the International Classification of Diseases, Tenth
Te objective of the study was to determine whether
Revision (ICD-10) [9]. A three-level categorical variable
dysthymia and severe depression were associated with an
of dysthymia, depression, and no dysthymia/depression
increased risk of being diagnosed with dementia and
diagnosis was created from these ICD-10-CM codes. In
MCI among persons with early onset of depressive
case when a person had both a depression and a dysthymia
symptoms face to those with late onset. We have
diagnosis during the baseline period, they were considered
investigated the impact of early onset of depressive
to have met the criteria for depression [10].
symptoms in midlife (<60 years) and late onset (>60
Cognition and functional capacity
years) on the onset of age related memory disorders.
Participants completed a cognitive battery that
Persons aged between 70 and 90 years, who were under
included: the Mini-Mental State Examination test
the supervision of a general medicine practitioner,
(MMSE) of Folstein [11], that measures orientation,
participated to the study. Tis study aims to highlight
registering of information, attention and calculation,
the importance of assessing depressive symptoms and
recalling of information and speech; the clock drawing
depression in general, and in elderly patients in
test of Brodaty [12] in which the patient was invited to
particular, given the major risks of these diseases and the
draw the face of a round clock with the numbers in it
morbid associations that characterize elderly patients
and the arms denoting time 2:45; the SIB test (Severe
and that influence the clinical course.
impairment battery) was used in the case when MMSE
was <9 and the verbal fluency tests.
Methods
Activities of daily living and the functional capacity
of independently living, was measured with: (a) the
Participants
Scale of basic activities of daily living (BADL) which
Data for this retrospective cohort study were
explores the six basic activities of daily living as: walking,
obtained from the personal files registered in the general
eating, bathing, dressing, toileting and continence; (b)
practice in the Moldova region of Romania. 73 women
the Scale of activities of daily living (ADL) with the 17
aged 70 years and over agreed to participate. Te average
items related to walking, dressing, washing, toileting,
age was 78.5±4.83 years and the average schooling was
continence, personal care, preparing meals, using
6th grade.
objects, feeding; and
(c) the Scale of instrumental
All were tested by medical examination in during
activities of daily living (IADL) which explores eight
year 2011.
instrumental activities as: using the telephone, managing
24
Popescu et al
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
Original articles
money/shopping, preparing a tea/meals, taking care of
the disease was calculated by dividing the events of that
his own home, doing laundry, using vehicles/visiting the
age group to the number of people in the specific group.
home of friends and taking medications.
Decision of Clinical Cognitive Status
Results
Clinical cognitive decision was conducted upon
participants’ performance on the cognitive tests, medical
Te overall prevalence of dysthymia was 19.18%
history, medications, and functional status, recorded at
and
4.11% of severe depression.
23.29% were
baseline and at the one-year follow-up visit, when the
considered as having depression. Te highest prevalence
progressive memory decline could be recorded.
of depression was found for participants aged 85-89
According to the Diagnostic and Statistical Manual of
years,
7.14% for severe depression and 42.57% for
Mental Disorders, Fourth Edition criteria [13], National
dysthymia (Figure 1). According to DSM IV, the age
Institute of Neurological and Communicative Disorders
specific prevalence for AD and MCI was calculated, the
and Stroke-Alzheimer’s Disease and Related Disorders
remaining participants were considered to be normal for
Association criteria
[14] and the International
age or having
“benign forgetfulness”.
9.59% were
Classification of the Diseases, tenth revision [9], there
diagnosed with AD, 34.25% with MCI and 56.16%
was determined whether the participants were
were considered normal for age
(Figure
2). It was
cognitively normal, or had MCI or dementia. After 12
observed that the prevalence for AD and MCI increases
months, the progression of cognitive decline was
with age, as “benign forgetfulness” decreases.
assessed by comparing the results of the tests made at 1
Average MMSE frequency distribution shows a
month, 3 months, 6 months.
Gaussian curve with a score between 15 and 30 for the
GDS Reisberg scale was used [15] to assess the state
MMSE (Figure 3 and 4). From both graphs it is
of impairment, with a threshold for dementia at
Reisberg stage four. Only patients functional dependent
in at least one functional scale assessing activities of
daily living, and with cognitive decline in
neuropsychological tests, were considered as screening
positive for possible or probable dementia.
Other measurements
Women’s demographic data included age,
educational attainment, presence of depression and
other
co-morbidities.
Routine
blood
tests,
electrocardiography in resting state and TC-scan were
performed.
Procedure
Te voluntary consent of the patients was recorded
Figure 1. Te age specific prevalence for depression spectrum
after they received the entire information about the
disorders (no depression, dysthymia, severe depression)
study’s goal and protocol. Te team contacted and
informed the nearest relative of the patient to give the
written consent to the study, in case of a frail patient
who couldn’t express her own decision.
Statistical analysis
All statistical procedures were performed using
EpiInfo (TM) software (CDC Atlanta), version 3.5.3.
Results were expressed as mean
± SD for numeric
variables. For qualitative variables total frequency and
percentages were used. Assessment of the differences
between groups was performed using “Student t” test
for continuous variables and χ2 for categorical variables.
Statistical significance was defined as p
<0.05, for a
confidence interval (CI) of 95%. Te prevalence rate
Figure 2. Te age specific prevalence for dementia (AD),
was calculated as a percentage of cases in the total group
mild cognitive impairment (MCI) and benign forgetfulness
at baseline. Age group specific probability of developing
(normal for age)
Depressive Symptoms and Memory Disorder in Elderly
25
Original articles
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
significant difference, p=0.42 (>0.05), 95% CI 0.43-
7.24.
A two-level variable was definite according to the
presence of DAT. By the criteria of developing DAT, the
demographic characteristics of the investigated patients
and their co-morbidities are summarized in Table I. It is
seen that depression (severe depression) and less severe
depression (dysthimia) show statistical significance in
the group with DAT, p=0.0001
(<0.05),
95% CI:
3.1336-9.5204, with a risk 5 times higher for people
diagnosed with AD, RR
(relative risk)
=
5.4620.
Correlation was positive for both severe depression and
especially for dysthymia. Tus for severe depression: p =
0.0112 (<0.05), 95% CI: 1.94-182.62 and RR: 18, and
for dysthymia: p=0.0020 (<0.05), 95% CI: 1.62-8.86,
Figure 3. Distribution of MMSE values
RR: 3.8.
Yesavage Geriatric Depression Score had a mean of
12.94 for those with AD and 8.68 for those without
AD, considering a score between 0-10 as no depression,
11-20 as mild depression and 21-30 as severe depression.
Table I. Characteristics of participants at
baseline according to the presence
of AD (dementia of Alzheimer type)
n=73
ADa
No AD
n=7b
n=66
Age (years), mean ± SD
82.14±2.32
78.5±4.75
Figure 4. Variation of MMSE in age groups
Gender (women), n (%)
7 (9.59)
66 (90.41)
Education (years), mean ± SD
6.1±1.45
6.03±2.03
Scorul de depresie Yesavage,
12.94±2.8
8.68±5.33
media ± SD
observed that the average values indicate the presence of
GDSc, mean ± SD
4.0±0***
2.35±0.55
moderate cognitive impairment, which corresponds to
Depression+Dysthymia
6 (85.71)***
11 (16.67)
stage 4 on Reisberg scale, or early stage dementia of
(presence), n (%)
Alzheimer type (DAT), according to DSM IV. Tese
Severe Depression (presence),
2 (28.57)*
1 (1.52)
patients had moderate cognitive impairment (MMSE =
n (%)
10 to 20), associated with a slight functional impairment
Dysthymia (presence), n (%)
4 (57.14)**
10 (15.15)
as measured by ADL, IADL, objectified only by the
Depression, early onset, < 60
closest people. Only 8% of patients had MMSE values
4 (57.14)***
5 (7.58)
years, n (%)
between 10 and 15 points. Tese patients had TC-scan
Depression, late onset, > 60
changes showing various degrees of cortical atrophy and
2 (28.57)
6 (9.09)
years n (%)
ventricular enlargement. Age distribution of MCI and
AD is shown in Figure 4.
a Diagnostic for Alzheimer disease (AD) and no AD was made
according to the DSM IV criteria.
Depending on the time of the onset of depression,
b χ2 tests for categorical variables and t-tests for continuous
we calculated the risk of AD for the two categories:
variables showed differences in baseline characteristics by AD/no
onset below 60 years and over 60 years, observing that
AD in the studied group at *p<0.05, **p<0.01, and ***p<0.001.
the first case was accompanied by a 2-fold higher risk of
c GDS (global deterioration scale Reisberg) assessed the stage of
developing AD (RR=2.00), without showing statistically
the impairment.
26
Popescu et al
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
Original articles
Discussions
Alzheimer type, late-onset depression may be an early
sign of AD.
Te present study examined the longitudinal
Te presence of depressive symptoms, particularly
relationship between prevalence of age related memory
of early onset, should be carefully monitored for adverse
disorders and presence of depressive symptoms in
outcomes, such as memory degenerative disease or
connection with the time of occurrence before or after
death.
60 years. It was also shown that severe depression and
Future studies should determine whether treatment
dysthymia, are positively correlated with the presence of
of depression spectrum disorders may reduce the risk of
dementia of the Alzheimer type.
these outcomes. A healthy lifestyle, community life and
In the absence of antidepressant treatment,
positive thinking could also be taken into account when
depression should be monitored for adverse outcomes
treating memory disorders.
such as occurrence of AD or death.
None of the authors declared any conflict of interest.
Te results of the paper are similar to those of
Te present study had no other external support.
previous studies that show a positive relationship
between depression and depressive symptoms during
midlife and age-related memory disorders.
References
Despite long-lasting debate around the outcomes of
diverse studies, the causal relationship between
1.
Alexopoulos G S, Abrams R C. Depression in
depression and dementia is far to be clarified [16]. Te
Alzheimer’s disease. Psychiatric Clinics of Nord
two illnesses share certain motor, cognitive and
America 1991;14(2):327-40.
behavioral dysfunctions. A recent paper reporting the
2.
Tune L E, Depression and Alzheimer’s disese. Depress.
outcomes of 17 years of follow up [17] points out that
Anxiety 1998;8(Suppl.1):91-5.
21.6% of their subjects with depression at baseline
3.
Devanand D P, Sano M, Tang Ming-Xin, et al.
developed dementia, face to 16.6% of those without
Depressed Mood and the Incidence of Alzheimer’s disease
this illness at baseline. Ge Li et al. [16] studied the
in Elderly Living in the Community. Arch Gen
temporality of the association between depression and
Psychiatry 1996;53(2):175-82.
dementia and inferred that late-life depression would
4.
Geerlings M I, den Heijer T, Koudstaal P J, Hofman
rather be an early manifestation of the illness.
A, Breteler M M B. History of depression, depressive
Severe depression was present in 28.57% of patients
symptoms, and medial temporal lobe atrophy and the
with DAT and only 1.52% of those without DAT.
risk of Alzheimer disease, Neurology 2008;70:1258.
It is estimated that the risk of developing depression
5.
Wilson RS, Hoganson G M, Rajan KB, Barnes LL,
for people with memory impairment is approximately 5
Mendes de Leon CF, Evans DA. Temporal course of
times higher than for those who do not suffer from these
depressive symptoms during the development of
disorders: 2.77<(RR=5.46) <9.54.
Alzheimer disease: Blowing hot and cold over depression
In reference to the influence of depression on age-
and cognitive impairment. American Academy of
related memory disorders, MCI and DAT, 50% of the
Neurology 2011;76:1531-2.
patients who were more depressed, older and with lower
6.
Wilson RS, Arnold SE, Todd L, Beck MS, Bienias JL,
MMSE scores developed memory disease.
Bennett DA. Changes in Depressive Symptoms During
the Prodromal Phase of Alzheimer’s Disease. Arch Gen
Conclusions
Psychiatry 2008;65(4):439-46.
7.
Lantz MS, Buchalter EN. Pseudodementia. Cognitive
Depression of any type is often associated with age-
decline caused by untreated depression may be reversed
related memory impairment. Te association is statistically
with treatment. Geriatrics 2001;56(10):42-3.
significant for severe depression and dysthymia, p=0.0001
8.
Yesavage JA, Brink TL, Rose TL, et al. Development
(<0.05), 95% CI: 3.13-9.52. Risk of depression for a
and Validation of a Geriatric Depression Screening
person with AD is about 5 times higher (RR=5.46), and a
Scale: A Preliminary Report. J Psych Research
person’s risk of developing AD when depression is present
1983;17(1):37-49.
is 2 times higher (RR=2.00). Te risk is higher for severe
9.
World Health Organisation, Tenth revision of the
depression, RR=18, p=0.0112 (<0.05), and smaller, but
international classification of the disease. Geneva:
still present, for dysthymia, RR=3.8, p=0.0020 (<0.05).
World Health Organisation, 1993;46-7.
While depression with an onset under the age of
10.
Castilla-Puentes RC, Habeych ME. Subtypes of
60 years may be a risk factor for dementia of the
Depression among Patients with Alzheimer’s Disease and
Depressive Symptoms and Memory Disorder in Elderly
27
Original articles
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
Other Dementias. Alzheimer’s & Dementia
disease:report of the NINCDS-ADRDA Work Group
2010;6(1):63-9.
under the auspices of the Department of Health and
11. Folstein MF, Folstein SE, McHugh PR. “Mini-mental
Human Services Task Force on Alzheimer’s disease.
state”. A practical method for granding the cognitive
Neurol 1984,34:939-44.
state of oatients for the clinician. Journal of Psychiatric
15. Reisberg B, Ferris SH, de Leon MJ, Crook T. Te Global
Resourses 1975;12(3):189-98.
Deterioration Scale for assessment of primary degenerative
12. Brodaty H, Moore C M. Te Clock Drawing Test for
dementia. Am J Psychiatry 1982;139(9):1136-9.
dementia of the Alzheimer type: a comparison of three
16. Li G, Wang LY, Shofer GB, et al. Temporal Relationship
scoring methods in a memory disorders clinic. Int J of
Between Depression and Dementia. Findings From a
Geriatric Psychiatr 1997;12:619-27.
Large Community-Based
15-Year Follow-up Study.
13.
***, Diagnostic and Statistical Manual of Mental
Arch Gen Psychiatry 2011;68(9):970-7.
Disorders, 4th edn., American Psychiatric Association,
17. Saczynski JS, Beiser A, Seshadri S, Auerbach S, Wolf
Washington, 1994;21-5.
PA, Au R. Depressive symptoms and risk of dementia.
14. McKhann G, Drachman D, Folstein M, Katzman R,
Te Framingham Heart Study. Neurology 2010; 75(1):
Price D, Stadian E. Clinical diagnosis of Alzheimer’
35-41.
28
Popescu et al
Original articles
ATHEROGENIC RISK QUANTIFICATION BY USING THE ATHEROGENIC
INDEX OF PLASMA (AIP) AND CARDIOVASCULAR RISK CALCULATOR
ON HYPERTENSIVE PATIENTS
Popa Călin1, Puşchiţă Maria2
1Histology Department, Faculty of General Medicine, Pharmacy and Dental Medicine from „Vasile Goldiş” Western
University of Arad, Emergency County Hospital of Timişoara; 2Internal Medicine Department, Faculty of General
Medicine, Pharmacy and Dental Medicine from „Vasile Goldiş” Western University of Arad, Emergency County Hospital
of Arad
Address for correspondence:
Dr. Calin Popa
„Vasile Goldiş” Western University of Arad
Faculty of General Medicine, Pharmacy and Dental Medicine
1 Feleacului Street, Arad
Email: calinpopa@msn.com.
Received: 10.01.2013
Accepted: 20.02.2013
Med Con March 2013, Vol 8, No 1, 29-36
Abstract
cardiac arrest, or any other cardiac diseases) without
tobacco or alcohol consumption. Te method used was
Te aim of this study was to find a protocol for
that of the comparison of several formulas of
quantifying the risk of atherogenesis and the risk of
atherogenesis and cardiovascular disease scores.
major cardiovascular events in hypertensive patients
Results: From our study we obtained high values of
with or without associated chronic diseases.
lipid fractions and a significant decrease of HDL-c values
Methods: Te study included
80 hypertensive
in all groups of study in relation to the control group. In
patients grouped as follows: the first group
(H1)
the H1-H4 study groups, we noticed a significant difference
included 20 hypertensive patients newly discovered 1st
in the risk of future cardiovascular events for male patients
grade hypertension (according to the European Society
compared to female patients. Also we noticed a significant
of Cardiology and the European Society of Hypertension
increase of LDL-c in H2 group compared to H1 group and
guidelines) without antihypertensive treatment; the
the atherogenic index of plasma values
(AIP) were
second group (H2) with 20 patients with metabolic
0.604±0.23 compared to 0.136±0.19 with a p<0.0001
syndrome X; the third group (H3) 20 hypertensive
(extremely significant statistically); for the H1 group the
patients with 2nd grade hypertension associated with
atherogenic and cardiovascular risk was moderate, while
diabetes mellitus type 2; the fourth group (H4) with 20
for groups H2, H3 and H4 were very high compared with
hypertensive patients with
2nd grade hypertension
the control group with a p<0.001.
associated with diabetes mellitus and chronic kidney
Conclusions: Correlating obtained data with recent
disease and a control group (C) with 20 healthy subjects.
studies from the medical literature, we concluded that
Inclusion criteria was age above 35 years and under 60
the atherogenic index of plasma (AIP) and cardiovascular
years (the average age for female patients was 44.5±3.9
risk prediction score (QRISK) are much higher in terms
and for male patients was
45.5±3.2) without
of statistics and diagnosis of atherogenesis and serious
cardiovascular diseases (history of stenting or bypass,
CV events.
Atherogenic Risk Quantification by Using the Atherogenic Index of Plasma (Aip) and Cardiovascular Risk
29
Calculator on Hypertensive Patients
Original articles
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
Keywords:
hypertension,
atherogenesis,
developing coronary heart disease is increased in patients
cardiovascular risk, HDL-c, LDL-c, TC
with elevated levels of TG and mutations of HL gene
which influence the structure and synthesis of HDL-c
Introduction
and raise the levels of TG [9]. Hipertrigliceridemia will
increase the activity of hepatic lipase HL and
Hypertension and atherosclerosis are two main
consecutively will alter the HDL-c, every
1 mg of
causes of cardiovascular morbidity and mortality. Tey
HDL-c degradation will cause an increase of 2% in the
often can coexist in the patient and both can cause and/
risk of coronary heart disease [10,11].
or exacerbate the other. In recent years the widespread
Te main objective of this study was to find a
application of molecular biology techniques led to the
protocol for quantifying the risk of atherogenesis and
identification of genetic polymorphisms associated with
the risk of major cardiovascular events in hypertensive
hypertension and cardiovascular events. Several clinical
patients with or without chronic diseases associated.
studies have begun to reveal physiological diversity in
hypertensive and cardiovascular disease heterogenetic
Material and method
character [1]. A number of peptide growth factors have
been identified through paracrine and autocrine
It was evaluated 80 patients (45 males, females 35)
mechanisms, which may be involved in vascular
suffering from hypertension and have been grouped as
remodeling and atherogenesis at the vascular
follows: first group (H1) included 20 patients (9 male,
endothelium level in hypertensive patients [2]. Due to
11 female) with hypertension
1st degree without
its strategic location, the vascular endothelium functions
treatment, the second group (H2) with 20 patients (12
as a sensor for the blood pressure which mediates
male,
8 female) with X metabolic syndrome
humoral and hemodynamic changes [3].
(hypertension grade I/II, decreased glucose tolerance,
Epidemiological studies have shown that several
obesity, sedentary), third group (H3-11 male, 9 female)
factors contribute to the onset and progression of
included 20 hypertensive patients with diabetes mellitus
atherosclerosis, from these factors age, gender and
type 2, the fourth group (H4-13 male, 7 female) includes
genetic predisposition are non-changeable parameters.
20 hypertensive patients with grade 2 associated with
Although the male sex is a major risk factor,
type 2 diabetes and chronic kidney disease. Te fifth
atherosclerosis becomes a major problem for women
group, control group had 20 healthy individuals (10
who are taking oral contraceptives and that increases the
male, 10 female).
risk even more when used after menopause and usually
Inclusion criteria for the study was people over 35
the symptoms began to appear about 10 years later [4].
years of age and under 60 years of age (the average age
Increased levels of serum cholesterol are the main risk
for female patients was 44.5±3.9 and for male patients
factor for atherosclerosis, especially LDL-c fraction, and
was 45.5±3.2) without cardiovascular disease (history of
other risk factors for atherosclerosis: smoking, decreased
bypass, stenting or other cardiovascular diseases),
glucose tolerance, obesity and sedentary lifestyle [5].
without tobacco, alcohol
consumption and
Prevalence of metabolic syndrome in developing
antihyperlipidemic drugs.
countries is rising due to the increase of obesity’s
Clinical data of hypertensive patients and control
incidence. Central obesity plays a key role in the
group were selected from anamnestic, clinical and
pathogenesis of the metabolic syndrome: promotes
paraclinical exams made to each patient at the moment
inflammation, hypertension, dyslipidaemia and it leads
of inclusion in our study. Blood pressure measurements
to the development of type 2 diabetes and atherosclerosis.
were performed according to the guidelines of the
Correcting and controlling these means less risk of
European Society of hypertension (ESH), in some cases,
increase or progression of atherosclerosis [6].
the patients in the Group H3 and H4 (5 patients)
For estimating the atherogenesis risk there are many
required an blood pressure monitoring apparatus, also
methods at the present time, depending of the study
known as Holter monitor, for 24 hours, in order to
that these are based on, for example the comparison of
determine the correct degree of high blood pressure
total cholesterol (TC), HDL-c/LDL-c ratio, calculators
(grade 2/3) as they had fluctuating hypertension [12].
that use either the Friedewald formula or Iranian
Consecutively the anamnesis and clinical
formula, TC/HDL-c ratio and more. Atherogenic index
examination, the laboratory examination included
of plasma (AIP) is an atherogenetic risk assessment tool,
determination from venous blood of total cholesterol
it is based on a formula that uses the TG and HDL-c
(CT), triglycerides
(TGR), LDL-cholesterol, HDL-
expressed either in mmol/l or mg/dl [7,8]. Te risk of
cholesterol, creatinine
(specifically for the estimated
30
Popa et al
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
Original articles
calculation of glomerular filtration rate-GFR). It was
ratio and AIP
(atherogenic index of plasma) values
investigated the albumin/creatinine ratio, using the
between each group of hypertensive patients and control
urinary dipsticks (for the evaluation of albuminuria as
group. For the comparison of the efficiency we’ve used
marker of renal damage by hypertension or diabetes
QRiskR2-2012 medical software licensed and authorized
mellitus cause) [13].
for predicting risk of major cardiac events for the next 5
Because stress is an important risk factor, we
or 10 years (a computer program that uses multiple data
included a psychological questionnaire for evaluating
from anamnesis, clinical exam and laboratory tests -
stress. Te test consisted of 25 questions, each question
especially those from the lipid profile), also useful to
can be marked with 1 point for a positive answer and
diagnose patients who haven’t been yet diagnosed [14].
with 0 for negative response. Te results obtained were
All results were expressed as mean±standard
classified into one of three categories of possible
deviation (SD). Te data were analysed for statistical
outcomes of the test as follows: under
4 points
-
significance using the computer program Statistica 7.
minimum stress; 5-13 points indicated that the subject
For values of p<0.05 was considered significant, for
experiences stress encountered by health problems,
values of p<0.01 it was considered distinctive statistically
whether physical or mental, or both; and more than 14
significant, for values of p<0.001 was considered very
points indicates a critical level of stress.
significant statistically and for p values
>0.05 were
For quantification of atherogenic risk and
considered non-significant.
cardiovascular disease risk, our goal was to create a
protocol for the most accurate method of estimation for
Results
these two important issues at the present time:
atherogenesis and major cardiovascular events
In Table
1
(data from anamnesis and clinical
(myocardial infarction and stroke). So, we included the
examination) it can be seen that the age of the subjects
determination of the TC/HDL-c ratio, LDL-c/HDL-c
in the study groups is significant close, also the BMI
Table I. Clinical data of hypertensive patients and control group
Parameters*
Group
Age1
BMI1
BP1
SC1
♂
♀
♂
♀
♂
♀
♂
♀
Control
38.5±2.3
37±4.2
24.3±3.2
20.4±1.6
124±2.1
118±1.2
4.75±1.2
6±2.3
/78±1.7
/74±1.7
H1
42±5.7
39±4.5
25.9±2.3
25.1±1.2
148±1.7
146±1.9
10.75±3.4
10.89±4.2
/96±1.8
/94±2.4
p (H1 vs. C)2
0.00026
0.01492
0.26054
0.00155
0.00355
0.00213
0.00086
0.00897
***
**
***
**
***
**
H2
46.5±3.6
44.5±4.8
31.5±4.6
29.5±5.3
150±3.2
148±2.8
13±1.9
12±1.6
/92±2.4
/98±2.3
p (H2 vs. C)2
0.00012
0.00123
0.01801
0,00256 **
0,00082
0,00188
0,00048
0,00064
***
**
***
**
***
***
H3
47±5.1
46±7.2
25.8±1.7
24.9±1.4
168±2.2
156±2.6
12±2.8
11±2.4
/106±2.4
/104±2.8
p (H3 vs. C)2
0.00018
0.00025
0.01901
0.00158 **
0.00142
0.00186
0.00036
0.00054
***
***
**
**
***
***
H4
49±4.2
52±3.1
25.3±3.8
25.5±4.7
176±2.8
172±3.5
14±1.89
13±1.67
/104±2.9
/108±4.1
p (H4 vs C)2
0.00102
0.01811
0.03902
0.00118
0.00024
0.00048
0.00022
0.00028
**
**
***
***
***
***
Legend: 1= average (mean) and standard deviation; BMI = body mass index, BP = blood pressure; SC = stress questionnaire; 2= p values
for each hypertensive group compared with control group, p<0.05* statistically significant, p<0.01** highly statistically significant and
p<0.001*** highly statistically significant.
Atherogenic Risk Quantification by Using the Atherogenic Index of Plasma (Aip) and Cardiovascular Risk
31
Calculator on Hypertensive Patients
Original articles
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
(body mass index) isn’t very different in hypertensive
patients, which indicates a glomerular damage due to
groups H1-H4
(value of p=0.26054 for group H1
hypertension and blood glucose increased levels. We
compared to the control group), but the level of
noticed significant differences for values of TC, TG and
hypertension in the same groups is significantly different
HDL-c, especially in male patients, the rest have the
from the control group, indicated by the values of p<
values for these parameters near the upper limits but
0.05 (p=0.0082 for male subjects and p=0.0018 for
within the normal range (Table II).
female subjects from group H2).
In the H2 Group (table III) biochemical parameters
Regarding the distribution by gender, the female
were significantly modified for these patients with
patients had lower values of measured parameters
higher values. Anamnesis data shows that this group has
compared to those of the male, and the stress index
obese patients with highly modified lipid profile,
shows that in groups with associated diseases, the stress
hypertension for more than 1 year, with a vicious and
is much higher than those in the control group, for
sedentary life style, with low glucose tolerance,
example, the value of p=0.00028 for female patients and
microalbuminuria and high values of GFR indicating
p=0.00022 for male patients in group H4.
impairment of renal function, and p values are
For patients in Group H1
(newly-discovered
significant in comparison with control group.
hypertensive
patients
without antihypertensive
For patients from groups H3 and H4 the resulting
treatment) it can be noticed that is a modification of the
data indicates a significant intermission in comparison
lipid profile and a slightly deviated value of the albumin/
with the control group and the H1 group for
creatinine ratio towards microalbuminuria in male
biochemical values taking into consideration that these
Table II. Biochemical data to study group H1 compared to the control group
Control group
H1
p
Parameters
♀
♂
♀
♂
♀
♂
TC (mg/dl)*
186.1±11.2
188.1±10.2
202.2±25.8
206.5±26.8
0.0125
0.0118
TG (mg/dl)*
122.8±9.8
138.3±9.6
144.3±22.4
182.6±18.6
0.0228
0.0214
LDL cholesterol (mg/dl)*
126.4±7.5
124.2±8.4
154.2±26.8
158.5±24.5
0.0345
0.0278
HDL cholesterol (mg/dl)*
58.1±2.8
52.1±4.4
46.7±32.3
44.8±12.26
0.0159
0.0147
Blood sugar (mg/dl)*
88.3±1.68
92.3±2.4
98.7±17.6
98.7±18.45
0.0445
0.0356
Serum creatinine (mg/dl)
0.84±0.18
0.92±0.12
1±0.68
1.2±0.88
0.0562
0.0511
Albumine/creatinine ratio (mg/g)
18±1.5-N
20±2.4-N
22±2.8-N
24±3.2-M
0.0126
0.0118
GFR (ml/min/1.73m2)
118±2.2
120±3.4
102±7.5
108±5.7
0.0044
0.0024
Legend: * = mean+DS, the value of p<0.05 considered significant (S), p>0.05 considered non-significant (NS); Albumin-creatinine
ratio: N-normal values, M-presence of miroalbuminuria, A-clinical proteinuria; GFR-glomerular filtration rate.
Table III. Biochemical data to study group H2, compared to the control group
Control group
H2
p
Parameters
♀
♂
♀
♂
♀
♂
TC (mg/dl)*
186.1±11.2
188.1±10.2
386.1±54.6
424.3±58.5
0.0036
0.0028
TG (mg/dl)*
122.8±9.8
138.3±9.6
368.1±25.7
452.4±56.2
0.0068
0.0015
LDL cholesterol (mg/dl)*
126.4±7.5
124.2±8.4
192.3±25.5
202.4±44.3
0.0145
0.0122
HDL cholesterol (mg/dl)*
58.1±2.8
52.1±4.4
40.5±34.5
38.8±38.5
0.0224
0.0189
Blood sugar (mg/dl)*
88.3±1.68
92.3±2.4
102.2±23.6
110.7±46.8
0.0388
0.0259
Serum creatinine (mg/dl)*
0.84±0.18
0.92±0.12
1.4±0.89
1.6±0.46
0.0148
0.0125
Albumine/creatinine ratio (mg/g)
18±1.5-N
20±2.4-N
44±12.5-M
68±8.9-M
0.0065
0.0089
GFR (ml/min/1.73m2)
118±2.2
120±3.4
96±12.5
92±7.8
0.0188
0.0145
Legend: * = mean+DS, the value of p<0.05 considered significant (S), p>0.05 considered non-significant (NS); Albumin-creatinine
ratio: N-normal values, M-presence of miroalbuminuria, A-clinical proteinuria; GFR-glomerular filtration rate.
32
Popa et al
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
Original articles
patients’ pathology is more diversified and their
(p>0.05) being close to the control group’s values and
average age is higher. Te differences between the
within the normal range (mean and SD 1.2±0.88).
control group and every other group are obvious, so
For the estimative calculation of glomerular
for the H2 Group (with metabolic syndrome) has the
filtration rate (GFR) we used an online free calculator
highest values of lipid fractions and the same group H2
based on MDRD formula (Modification of Diet in
and for H3 and H4 groups (patients with diabetes
Renal Disease) developed by the International Society
mellitus type 2) we observed the highest levels of blood
of Nephrology (ISN) whit anamnesis data and serum
sugar. Correlated with the hypertension values and
creatinine level we managed to determine the
blood sugar
values
we discovered mild
estimated value of the GFR (ml/min/1.73m2) and to
microalbuminuria even from H1 group
(newly-
classify the functional state of the kidneys’ function
discovered hypertensive patients) with values for male
for all the study groups (Table VI). H2 and H3 groups
patients (average value 20 mg/g), next in the H2 and
were in the stage I chronic kidney disease
H3 group was elevated microalbuminuria values
(microalbuminuria on set) and H4 group was in stage
(averages between 40-180 mg/g), while the H4 group
II chronic kidney disease
(albumin/creatinine ratio
(Table V) we found clinical proteinuria
(average
indicating clinical proteinuria) with the presence of
statistical values >240 mg/g). Values of p have shown
renal dysfunction.
significant differences between the control group and
In table VII we presented resulting data by
H1 for all measured parameters, only the value of
calculating the ratio of LDL-c/HDL-c and TC/HDL-c,
serum creatinine was non-significant to this group
these were reported to AIP values.
Table IV. Biochemical data to study group H3, compared to the control group
Control group
H3
p
Parameters
♀
♂
♀
♂
♀
♂
TC (mg/dl)*
186.1±11.2
188.1±10.2
212.2±34.5
234.7±25.8
0.0098
0.0122
TG (mg/dl)*
122.8±9.8
138.3±9.6
256.1±38.4
260.7±33.7
0.0144
0.0147
LDL cholesterol (mg/dl)*
126.4±7.5
124.2±8.4
166.2±42.1
168.5±34.6
0.0159
0.0135
HDL cholesterol (mg/dl)
58.1±2.8
52.1±4.4
46.3±44.8
38.4±27.4
0.0115
0.0215
Blood sugar (mg/dl)*
88.3±1.68
92.3±2.4
262.2±31.3
324.3±28.4
0.0025
0.0012
Serum creatinine (mg/dl)*
0.84±0.18
0.92±0.12
2.2±0.25
2.4±0.26
0.0059
0.0156
Albumine/creatinine ratio (mg/g)
18±1.5-N
20±2.4-N
162±11.5-M 180±12.5-M
0.0012
0.0256
GFR (ml/min/1.73m2)
118±2.2
120±3.4
88±4.8
86±11.8
0.0278
0.0125
Legend: * = mean+ DS, the value of p<0.05 considered significant (S), p>0.05 considered non-significant (NS); Albumin-creatinine
ratio: N-normal values, M-presence of miroalbuminuria, A-clinical proteinuria; GFR-glomerular filtration rate.
Table V. Biochemical data to study group H4, compared to the control group
Control group
H4
p
Parameters
♀
♂
♀
♂
♀
♂
TC (mg/dl)*
186.1±11.2
188.1±10.2
244.8±46.2
252.9±51.1
0.0147
0.0125
TG (mg/dl)*
122.8±9.8
138.3±9.6
262.2±31.7
281.5±46.5
0.0255
0.0261
LDL cholesterol (mg/dl)*
126.4±7.5
124.2±8.4
172.1±28.5
174.2±11.8
0.0169
0.0256
HDL cholesterol (mg/dl)
58.1±2.8
52,1±4.4
42.4±48.2
36.3±12.3
0.0259
0.0169
Blood sugar (mg/dl)*
88.3±1.68
92,3±2.4
298.6±22.1
286.1±28.4
0.0048
0.0158
Serum creatinine (mg/dl)*
0.84±0.18
0,92±0.12
5.2±0.73
5.8±0.86
0.0011
0.0098
Albumine/creatinine ratio (mg/g)
18±1.5-N
20±2.4-N
242±11.7-A
260±10.2-A
0.0059
0.0185
GFR (ml/min/1.73m2)
118±2.2
120±3.4
66±4.8
58±8.2
0.0198
0.0194
Legend: * = mean+DS, the value of p<0.05 considered significant (S), p>0.05 considered non-significant (NS); Albumin-creatinine
ratio: N-normal values, M-presence of miroalbuminuria, A-clinical proteinuria, GFR-glomerular filtration rate.
Atherogenic Risk Quantification by Using the Atherogenic Index of Plasma (Aip) and Cardiovascular Risk
33
Calculator on Hypertensive Patients
Original articles
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
Table VI. Staging of renal dysfunction according to FRG
Stage** GFR*
Description
I
90+ Normal renal function (urine analysis, structural malformations or genetic factors indicate kidney disease)
II
60-89
Mild renal dysfunction (GFR correlate with urine analysis, structural malformations or genetic factors)
III a
45-59
Moderate kidney dysfunction (with or without other evidence of kidney damage)
III b
30-44
Moderate kidney dysfunction
IV
15-29
Severe renal dysfunction
V
<15
Severe renal insufficiency
Legend: * = GFR glomerular filtration rate in ml/min/1.73 m 2, the estimated values obtained with the MDRD formula GFR
computer; ** = staging ISN (International Society of Nephrology) concerning the classification of kidney disorders.
Table VII. Atherogenesis formulas (values and standard deviation)
C
H1
p(H1-C)
H2
p(H2-C)
I*
♀
♂
♀
♂
♀
♂
♀
♂
♀
♂
0.046±
0.136±
0.257±
0.604±
0.688±
AIP
0.064±0.23
***
***
***
***
0.8
1.2
1.45
1.87
1.75
LDLc/
2.17±
3.59±
5.31±
2.38±0.27
3.34±1.1
**
**
4.8±2.32
**
**
HDLc
1.2
1.67
1.98
TC/
3.20±
4.68±
11.15±
3.61±0.56
4.39±1.12
**
**
9.68±2.31
**
**
HDLc
0.75
1.24
2.06
C
H3
p(H3-C)
H4
p(H4-C)
II*
♀
♂
♀
♂
♀
♂
♀
♂
♀
♂
0.046±
0.475±
0.435±
0.532±
AIP
0.064±0.67
0.385±1.98
***
***
***
***
0.97
2.11
2.31
2.33
LDLc/
2.17±
4.42±
4.09±
4.83±
2.38±1.11
3.60±1.55
**
**
**
**
HDLc
0.67
1.67
1.99
3.11
TC/
3.20±
6.15±
5.80±
7.02±
3.61±1.76
4.60±1.65
**
**
**
**
HDLc
0.12
1.98
1.75
2.34
Legend: * mean±SD; **the value of p<0.001 (very significant statistically); *** the value of p<0.0001 (extremely significant statistically.
Table VIII. Cardiovascular risk scores (average calculations)
Parameters1
AIP
QRISK score
Groups
♀
♂
♀
♂
Control
0.046±0.8
0.064±0.23
0.4%±1.71
0.5%±1.52
H1
0.136±1.2
0.257±1.45
4.2%±2.52
4.6%±2.45
p (H1 vs. C)2
***
***
***
***
H2
0.604±1.87
0.688±1.75
30.4%±1.95
31.8%±2.75
p (H2 vs. C)2
***
***
***
***
H3
0.385±1,98
0.475±2.11
20.2%±2.14
21.3%±3.24
p (H3 vs. C)2
***
***
***
***
H4
0.435±2.31
0.532±2.33
42.5%±2.06
44.2%±2.48
p (H4 vs. C)2
***
***
***
***
Legend: 1 = mean±SD; AIP (atherogenic index of plasma), QRisck score (score indicating the estimate risk of developing
cardiovascular disease over the next 10 years) obtained with software licensed under QRISCKR2012; 2=values of p resulted
by comparing each hypertensive group with the control group, p<0.0001 *** (extreme significant statistically).
34
Popa et al
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
Original articles
In Table VIII the AIP was compared for each group
index of plasma (AIP) can estimate the cardiovascular risk,
by gender with QRISCK score using computer program
this index is also sensitive to pharmacological treatment
QRISKR2-2012 (licensed by ClinRisk Ltd UK). Tis
being a barometer of therapeutic success. Te normal values
program uses anamnesis data (most important: age,
for AIP must be less than
0.11, for this values the
gender, BMI, lifestyle, associated diseases), the blood
cardiovascular events risk is reduced; range from 0.11 to
pressure values and the TC/HDL-c to estimate the risk
0.21 indicates intermediate risk of CV disease and values
of developing major cardiovascular diseases (myocardial
>0.24 shows a high cardiovascular risk [18].
infarction or stroke) over the next 10 years.
In our study, significant differences in the
It can be seen that the values of p are very small
hypertensive patient groups were between male and
(<0.0001), which indicates a very important statistical
female subjects. Te AIP for female patients in the
meaning, in front of p values of atherogenesis indexes:
control group was 0.046 and for female patients in H2
TC/HDL-c ratio and LDL-c/LDL-c ratio.
group was
0.604
(13 times bigger) with values of
p<0.0001 (extremely significant statistically), while the
Discussion
atherogenic index of LDL-c/HDL-c ratio for the same
category of female patients from control group was 2.17
Our investigation data reveals that at the patients
and for H2 group was 4.8 (almost 2 times) with p<0.001.
with a smaller average age and debut of hypertensive
For a more complex comparison the index of TC/
illness (H1) the measured parameters from above were
HDL-c ratio for the same sex patients was 3.20 in the
slightly different compared with control group but
control group and for the H2 (female patients) was 9.68
statistically significant, and for the other hypertensive
(almost 3 times bigger). By comparison it can be seen
groups modifications were distinctive, taking in
that the atherogenic index of plasma, statistically gives
consideration the length of the disease and the
distinct values than the other atherogenesis formulas.
associated chronic illnesses. Tese data were important
Te AIP value was highest for the H2 group (patients
for the quantification of atherogenic risk and for the
with hypertension grade I/II, impaired glucose tolerance,
future cardiovascular events risk, which we have
central obesity, dyslipidemia and microalbuminuria)
introduced in the formulas of risk calculators.
indicating increased risk of atherogenesis, but with a
Albumin/creatinine ratio revealed us the amount of
lower QRisck score (30.4%±1.95 ♀, 31.8%±2.75 ♂)
microalbuminuria which, according to Boersa et al can be
compared to H4 group (two associated chronic diseases
directly correlated with high blood pressure and kidney
plus hypertension) which has a higher possibility for
function. It has been demonstrated that the level of
cardiovascular events in the next 10 years, more often
microalbuminuria indicates the age of the hypertensive
and at a higher percentage
(42.5%±2.06% ♀ and
illness and the efficiency of treatment, and it can be
44.2%±2.48 ♂). But from atherogenic point of view the
reversible when it has small values, which directs us that
atherogenesis process is more active in patients with
the glomerular apparatus is not yet damaged, so we can
altered lipid profiles with very high lipid fraction values
say it’s not a kidney major problem for its function. In the
(H2) than in patients with associated diseases but with
other hand for the H2, H3 and H4 groups the situation is
altered lipid profile with average values (H3, H4).
different, we can observe high values for microalbuminuria
In conclusion, by comparing each important
even proteinuria, very significant statistically compared
parameter from our, which is involved directly or indirectly
to control group which indicates an obvious renal
in the initiation or maintenance of atherogenesis and
damage, confirmed also by the GFR values for these
cardiovascular disease for each group of hypertensive
groups, similar with literature data [13,15].
patients, we were able to highlight the importance of AIP
Ratios of LDL-c and TC with HDL-c, according to
and QRisck score for the clinician in medical practice and
Grover et al, are good predictors for future cardiovascular
it can be a useful and economical tool for diagnosis,
events, but after Gotto et al who conducted a study of 8
treatment and prevention of chronic cardiovascular disease
years in a predominantly male population, the serum
and major cardiac events (especially MI and stroke).
levels of TG may represent alone an important risk
factor for future cardiovascular events [16,17].
Recent studies have indicates that TG/HDL-c ratio
References
transformed logarithmically can estimate the atherogenic
risk better than all others. TG and HDL-c perfectly reflects
1. Giner V, Poch E, Bragulat E, et al. Renin-angiotensin
the balance between atherogenic lipoproteins and protective
system genetic polymorphisms and salt sensitivity in essential
lipoproteins. Clinical studies revealed that atherogenic
hypertension. Hypertension 2000;35(1 Pt 2):512-7.
Atherogenic Risk Quantification by Using the Atherogenic Index of Plasma (Aip) and Cardiovascular Risk
35
Calculator on Hypertensive Patients
Original articles
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
2.
Gibbons GH. Mechanisms of vascular remodeling in
10.
Njajou O, Kanaya AM, Holvoet P, Connelly S, Harris
hypertension: role of autocrine-paracrine vasoactive
T. Association between oxidized LDL-C, obesity and type
factors. Curr Opin Nephrol Hypertens 1995;4(2):189-
2 diabetes. Diabetes Metab Res rev 2009;25(8):733-9.
96.
11.
Libby P. Inflammation in atherosclerosis. Nature
3.
Dzau VJ, Gibbons GH. Endothelium and growth
2002;420:868-74.
factors in vascular remodeling of hypertension.
12.
European guidelines on cardiovascular disease prevention
Hypertension 1991;18(5 Suppl):III115-21.
in clinical practice. European Society of Cardiology
4.
Barton M, Dubey RK, Traupe T. Oral contraceptives
(2012).
and the risk of thrombosis and atherosclerosis. Expert
13.
Boersma C, Maarten J, Visser ST, et al. Baseline
Opin Investig Drugs 2002;11(3):329-32.
albuminuria predicts the efficacy of blood pressure-
5.
Fruchart JC, Kastelein JP, Duriez P. Atherosclerosis:
lowering drugs in preventing cardiovascular events. Br J
Evolving Vascular Biology and Clinical Implications
Clin Pharmacol 2008;65(5):723-32.
New Risk Factors for Atherosclerosis and Patient Risk
14.
Hippisley-Cox J, Coupland C, Vinogradova Y,
Assessment. Circulation 2004;109:III-15-III-19.
Robson J, Minhas R, Sheikh A. Predicting
6.
Grundy S, Brewer B, Cleema J, Smith S, Lenfant C.
cardiovascular risk in England and Wales: prospective
Definition of Metabolic Syndrome NHLBI/AHA.
derivation and validation of QRISK2. BMJ
Conference Proceedings Report of the National Heart,
2008;336:a332.
Lung, and Blood Institute/American Heart Association.
15.
Rodicio J, Campo C, Ruilope L. Microalbuminuria in
Circulation 2004;109:433-438.
essential
hypertension.
Kidney
International
7.
MacMahon S, Robson R, Johnsona R. Use of the
1998;54,S51-S54.
Friedewald Formula to Estimate LDL-Cholesterol in
16.
Grover S, Dorais M, Coupal L. Improving the
Patients with Chronic Renal Failure on Dialysis.
prediction of cardiovascular risk: interaction between
Clinical Chemistry 1997;43(11):2183-4.
LDL and HDL cholesterol. Epidemiology
8.
Ahmadi SA, Boroumand MA, Gohari-Moghaddam
2003;14(3):315-20.
K, Tajik P, Dibaj SM. Te impact of low serum
17.
Gotto AM. Triglyceride; the forgotten risk factor.
triglyceride on LDL-cholesterol estimation. Arch Iran
Circulation 1998;97:1027-8.
Med 2008;11(3):318-21.
18.
Dobiasova M, Frohlich J. Te plasma parameter log
9.
Turen T. Hepatic lipase and HDL metabolism. Curr
(TG/HDL-C- C) as an atherogenic index. Clin
Opin Lipidol 2000;11(3):277-83.
Biochem 2001;34:583-8.
36
Popa et al
Original articles
CHANGES OF SERUM PENTOSIDINE LEVELS IN PATIENTS WITH
RHEUMATOID ARTHRITIS STAGE I-II BEFORE TREATMENT
Cojocaru Manole1, Ghinescu Minerva Claudia1, Rusu Elena1, Bălăeţ Constantin1, Cojocaru Inimioara Mihaela2
1Titu Maiorescu University, Faculty of Medicine,Bucharest, 2Carol Davila University of Medicine and Pharmacy,
Bucharest
Address for correspondence:
Cojocaru Manole MD, PhD, EurClinChem
5 Tomas Masaryk St., Sector 2, Postal Code 020983
Bucharest, Romania
E-mail: mancojocaru@yahoo.com
Received: 15.01.2013
Accepted: 20.02.2013
Med Con March 2013, Vol 8, No 1, 37-40
Abstract
(ranges from 41.45-55.76 nmol/L, mean value 51.3±4.7
nmol/L; p<0.0001). Sixteen (39%) patients with signs
Background: Pentosidine, an advanced glycation
of inflammation (CRP>40 mg/L) had a significantly
end product (AGE), has recently been observed to be
(p<0.001) higher plasma pentosidine content. Tis was
elevated in rheumatoid arthritis (RA).
mainly due to the increased oxidative stress and to the
Objectives: To evaluate serum pentosidine in blood
extinction of the inflammatory process.
samples from patients with RA stage I-II before
Conclusion: In RA, there were significant
treatment and to investigate the relationship to clinical
correlations between pentosidine in serum and
outcome
C-reactive protein, and erythrocyte sedimentation rate.
Materials and methods: Te study was carried out
Pentosidine in serum is associated with the systemic
before therapy, in a group of 41 patients with RA stage
inflammatory activity of RA. Serum pentosidine was the
I-II ranging in age between 28-65 years. Te serum
superior indicator for RA disease status.
values of pentosidine were evaluated in a group of 24
Keywords: rheumatoid arthritis before treatment,
normal controls of the same age range and presenting
pentosidine, oxygen radicals
no signs of rheumatic disease. Te serum pentosidine
levels were measured by a direct HPLC method with
Pentosidine is one of a number of advanced
column switching. Data were reported as means±SD
glycation end products (AGEs). Pentosidine is formed
with 95% confidence limits. Te statistical significance
by sequential glycosylation and oxidation reactions.
of difference was determined with Student’s t-test.
Terefore, it is hypothesized that pentosidine formation
Prevalences were compared by the χ2 test. Fisher’s exact
is accelerated in diseases related to oxidative stress [1].
test and linear regression were used. Correlation analyses
Rheumatoid arthritis is a chronic systemic disease,
were performed by means of Pearson test.
although its major clinical consequence is inflammation
Results: Pentosidine in serum was significantly
of the joints and contiguous structures. Tere is now
higher in RA. In patients with RA stage I-II, before
considerable evidence for the involvement of oxygen-
treatment, the increase of serum pentosidine levels were
centred free radicals in acute and chronic inflammatory
significant (ranges from 57.14 nmol/L-145.17 nmol/L,
arthritis. Te role of free radicals in the autoxidation of
mean value 129.4±10.5 nmol/L vs. normal controls’
biological lipids is well established. Patients with RA
Changes of Serum Pentosidine Levels in Patients with Rheumatoid Arthritis Stage I-II Before Treatment
37
Original articles
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
have depressed serum levels of the antioxidant, and a low
compared by the χ2 test. Fisher’s exact test and linear
antioxidant level is a risk factor for RA. Because oxidative
regression were used. Correlation analyses were
stress and oxygen free radicals play a significant role in
performed by means of Pearson test. Statistical
tissue damage and inflammation in RA, pentosidine is
significance was defined as p<0.05.
supposed to be implicated in this disease [2]
Several years ago, pentosidine was reported to be
Results
elevated in the articular cartilage of RA. However, its
significant relationship to RA has not been investigated
Concentrations of pentosidine increase with age.
until recently. Now, there have been several studies
However, serum pentosidine did not show a statistically
which provide evidence that pentosidine is elevated in
significant correlation with age in the RA group.
patients with RA. Pentosidine in serum reflects the
Pentosidine levels in serum were significantly higher in
disease activity of RA. Although all pentosidine levels in
RA patients than in control subjects. Values were
body fluids have been associated with RA disease
129.4±10.5 nmol/L vs. 51.3±4.7 nmol/L (p<0.0001).
activity, it has not been clear which pentosidine levels,
Pentosidine levels in serum of RA were significantly
i.e. in serum, synovial fluid or urine, are a superior
correlated with CRP, ESR. Pentosidine levels in serum
indicator. Given the intrinsec importance of oxidative
were significantly higher in the high-activity group than in
reactions for the formation of pentosidine, we
the low-activity group (p<0.05). Sixteen (39%) patients
hypothesized an increased glycoxidation as a
with signs of inflammation
(CRP>40 mg/L) had a
consequence of conditions associated with increased
significantly (p<0.001) higher plasma pentosidine content.
oxidative stress in RA [3].
A significant positive correlation was found between
plasma pentosidine and CRP (r=0.78; p<0.0001).
Materials and Methods
We classified the patients into two groups on the
basis of CRP levels. In the inflamed (CRP>40 mg/L)
Te study included 41 patients with RA stage I-II,
patients, the plasma pentosidine was significantly higher
before treatment and 24 normal controls of the same
than in the noninflamed patients, and CRP levels were
age range and presenting no signs of rheumatic disease.
significantly correlated with plasma pentosidine
RA was diagnosed according to the criteria of the
contents. Te higher plasma pentosidine content was
American College of Rheumatology (ACR). Te RA
linked to inflammation. Tus, accumulation of plasma
group consisted of 35 female and 6 male patients aged
pentosidine in RA is unlikely to be an appropriate
28-65 years (mean age 61.0±13.0 years). Patients who
marker to predict severe course. Tese results prove that
had diabetes mellitus and those with abnormal levels of
pentosidine may accumulate in the absence of
serum blood urea nitrogen or creatinine were excluded
hyperglycemia or impaired kidney function.
from the study. Te control group consisted of 13
female and 11 male patients aged 46-79 years (mean age
Discussion
62.7±10.6 years). Tere was no significant difference in
age between RA and controls. After collection, blood
We measured levels of pentosidine in serum in RA
samples were centrifuged at 3000 r.p.m. for 15 min.
patients stage I-II before treatment, and examined the
Sera samples were kept at
-20°C until used for
pentosidine analysis. Informed consent was obtained
from all participants. Te procedures followed were in
accordance with the principles of the Declaration of
Helsinki in 1975, as revised in 1983. Serum C-reactive
protein
(CRP) and erythrocyte sedimentation rate
(ESR) were measured by routine laboratory methods.
Pentosidine was measured by a direct HPLC method
with column switching. Te concentrations of
pentosidine in serum were expressed as nmol/L. Urea,
creatinine, glucose, total serum proteins, and albumin
were measured immediately in serum by conventional
methods with a Hitachi 917 autoanalyzer.
Te statistical significance of difference was
Figure 1. Mean value of the serum pentosidine concentrations
determined with Student’s t-test. Prevalences were
in patients with rheumatoid arthritis as compared to controls
38
Cojocaru et al
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
Original articles
relationship between pentosidine and RA disease
RA stimulates Maillard reactions, then increases the
activity. Pentosidine has been described as a glycoxidation
formation of pentosidine in synovial fluid in RA [3].
product. Concentrations of tissue pentosidine increase
Terefore, the elevated pentosidine levels in serum of
with age. Concentrations of pentosidine are increased in
RA are not derived from the synovial fluid, but from an
diabetes, a consequence of hyperglycemia
[1]. Free
increase in the formation of pentosidine in the whole
radicals are implicated in tissue damage and
body in RA. Te general increase in free radicals is likely
inflammation in RA, and the formation of pentosidine
to accelerate the formation of pentosidine in RA [5].
is associated with oxidation. However, there have so far
Accordingly, pentosidine may not be a biochemical
been a few reports studying pentosidine in RA. Te
marker for joint degradation, but may be a marker for the
mechanisms of these phenomena remain unclear. It is
disease activity of RA. However, further research is needed
known that chronic hyperglycaemia leads to the
to verify this. Te results in the present study showed that
accumulation
of
non-enzymatically
derived
pentosidine levels in serum were significantly correlated
glycosylation products of proteins, such as pentosidine
with each other. However, serum pentosidine was a
in diabetes mellitus [2].
superior indicator for RA disease activity. Although the
In RA, the increased pentosidine concentrations are
substances in synovial fluid can directly reflect the local
present in serum; however, glucose levels are normal.
joint status, such as the inflammation and degradation of
Interest in recent years has focused on the potential of
the joint tissues, pentosidine may be carried into synovial
glycated proteins as a source of free radicals [3]. Exposure
fluid from the blood circulation. Terefore, among these
of IgG and other proteins to oxygen radicals, generated
body fluids, serum pentosidine is the best indicator for
by photolysis or by a mixture of iron or copper salts and
the disease status of RA. Te presence of increased
hydrogen peroxide, induces fluorescence in the protein
concentrations of serum pentosidine in RA confirms the
which is essentially indistinguishable from that
complexity of AGE accumulation. All RA patients in this
attributed to Schiff base formation. Because pentosidine
study were normoglycemic and had intact kidney
formation requires aerobic conditions, we propose that
function, as documented by their clinical records and
such free radicals could explain possible pathways for
confirmed by their serum creatinine and urea value. A
the elevation of pentosidine in RA. Tus, protein-linked
lokely explanation for the formation of pentosidine in RA
fluorescence such as that of pentosidine may therefore
patients involves increased oxidative stress. RA is a
not be the result of cumulative glycaemia over many
autoimmune disease associated with increased oxidative
years, but could be the result of successive exposure to
stress [6].
free radical-induced oxidation, and this may be of
importance in disease activity in RA [4].
Conclusion
We observed the elevated levels of serum pentosidine
in RA and its significant relationship to disease activity,
Te presence of increased concentrations of serum
we supposed that the elevated pentosidine in the blood
pentosidine in RA patients indicates that this compound
circulation was derived from the inflammatory joints in
is not a simple marker of glycosidation in diabetes, but
RA. Te increased concentrations of pentosidine would
can be used as a more general marker of oxidative stress
also be found in pathological conditions associated with
in RA. Pentosidine measurement in RA is clinically
increased oxidative stress. In that study, we proposed
useful. Measurement of serum pentosidine may provide
two possible pathways for the elevation of pentosidine
valuable information for active periods of RA.
in RA. One possibility is that because pentosidine is
abundant in cartilage compared with the other tissues,
Conflict of interest: Te authors who have taken part
inflammation of the joints may induce the breakdown
in this study declared that they do not have anything to
of cartilage, releasing cartilaginous pentosidine into
disclose regarding funding or conflict of interest with respect
synovial fluid; the other is an increase in the formation
to this manuscript.
of pentosidine in synovial fluid. It is known that total
proteins increase in synovial fluid in severely inflamed
joints, especially in those of RA. It is also known that
References
free radical oxidation products of synovial fluid were
higher in inflammatory than in degenerative joint
1. Sell DR, Monnier VM. End-stage renal disease and
disease, and in patients with RA than in normal controls.
diabetes catalyze the formation of a pentose-derived
A combination of elevated proteins (and amino acids)
crosslink from aging human collagen. J Clin Invest
and the acceleration of free radicals in synovial fluid of
1990;85:380-4.
Changes of Serum Pentosidine Levels in Patients with Rheumatoid Arthritis Stage I-II Before Treatment
39
Original articles
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
2. Takahashi M, Suzuki M, Kushida K, Miyamoto S,
5. Chen JR, Takahashi M, Suyuki M, Kushida K,
Inoue T. Relationship between pentosidine levels in
Mizamoto S, Inoue T. Measurement of pentosidine in
serum and urine and activity in rheumatoid arthritis.
synovial fluid in patients with osteoarthritis and
Br J Rheumatol 1997;36:637-42.
rheumatoid arthritis: relationship with disease activity
3. Rodriguez-Garcia J, Requena JR, Rodriguez-Segade
in rheumatoid arthritis. J Rheumatol 1998;25:2440-
S. Increased concentrations of serum pentosidine in
4.
rheumatoid arthritis. Clin Chem 1998;44(2):250-5.
6. Miyata T, Ishiguro N, Yasuda Y, et al. Increased
4. Chen JR, Takahashi M, Suzuki M, Kushida K, Miyamoto
pentosidine, an advanced glycation end product, in
S, Inoue T. Comparison of the concentrations of pentosidine
plasma and synovial fluid from patients with rheumatoid
in the synovial fluid, serum and urine of patients with
arthritis and its relation with inflammatory markers.
rheumatoid arthritis and osteoarthritis. Oxford Journals
Biochem Biophys Res Commun 1998;244:45-9.
Medicine Rheumatology 1999;38:1275-8.
40
Cojocaru et al
Original articles
THE SANOGENIC ROLE OF THERAPEUTIC INTERVENTION FOR
FIREFIGHTERS
Popa Gabriela Sorina, Podea Delia, Puşchiţă Maria
Vasile Goldiş West Univesity, Arad
Address for correspondence:
Psychologist Popa Gabriela Sorina
Tel. 0400752444227
Email: vancugabriela@yahoo.com
Received: 14.01.2013
Accepted: 25.02.2013
Med Con March 2013, Vol 8, No 1, 41-45
Abstract
Conclusions: Te short intervention we proposed
had positive outcomes in most cases, 79% of participants
Goal: Te present study investigates the efficiency
showed significant decrease in symptoms. In the cases
of a psychological intervention for firefighters who show
were the intervention showed no improvements we
symptoms of depression and anxiety. What motivates
intend to continue it with the consent of participants.
this study is the fact that the psychologist within the
Keywords: firefighter, critical incident, depression,
inspectorates for emergency situations must not only
anxiety,
psychological
intervention,
Hamilton
evaluate and monitor firefighters’ psychological
Depression Scale, Hamilton Anxiety Scale
evolution, but also to intervene in a preventive or
therapeutic way.
Introduction
Materials and Methods: Out of the firefighters we
evaluated periodically, we selected 19 individuals who
Te firefighters who work within the inspectorates
showed higher level of depression and anxiety symptoms,
for emergency situations are frequently and constantly
in order to include them in a psychological intervention
exposed due to the nature of their activities to high
program. Te intervention targeted cognitive aspects:
stressing situations also known as critical incidents. A
positive reformulation of experiences, emotional aspects:
critical incident represents a highly stressing event which
awareness and acceptance of intense emotions and a
can significantly disturb the physical and psychological
behavioral aspect: development of new or improved
function and wellbeing. Te critical incident is a
coping strategies. Te intervention comprised of six
stimulus which can trigger a physical and psychological
meeting. Pre-intervention and post-intervention
crisis [1].
psychological assessment was done with Hamilton
Te response to critical incidents and to any other
Depression Scale and Hamilton Anxiety Scale.
stressful situation is determined by objective features of
Results: Te scores for depression and anxiety
the situation, by individual’s subjective perception and
symptoms, for the entire lot, were significantly lower
interpretation of the situation, by the state of physical
post-intervention than those pre-intervention, showing
health and psychological wellbeing, by the coping
a decrease in the intensity of symptoms. Yet, 4 of the 19
mechanisms, by a series of psycho-individual factors
subjects showed stagnation or an increase of scores,
such as emotional stability and responsiveness, self
indicating no improvement of symptoms.
esteem, perceived self-efficacy, sense of coherence, locus
The Sanogenic Role of Therapeutic Intervention for Firefighters
41
Original articles
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
of control, but also by several psycho-social factors
scores that could be consider of clinical significance at
which include the socio-economical context in which
least at one of the two scales used.
rescue activities are performed, the institutional response
Te 19 subjects’ lot has undergone a psychological
to the certain event, mass-media representation of the
intervention which aimed to reduce the intensity of
event, etc. [2,3,4].
anxiety and depression symptoms. Te intervention
Te stress generated by critical incidents induces
focused on following aspect: a) awareness of one’s own
changes both at a physiological and somatic level, as
intense emotions and feelings experienced after a critical
well as at a psychological and behavioral level. At
incident; b) emotional unblocking and confronting with
physiological level, one can show cardiac dysfunctions,
the intense experiences triggered by the critical incident;
neurological and endocrine dysfunctions, myalgia and
c) investigating and acknowledging the negative
somatovisceral dysfunctions [3]. At psychological level
consequences of one’s own inadequate response and
one can show sensorial and perceptive dysfunctions,
coping strategy to stressful events in the professional and
cognitive, emotional and affective dysfunctions and, in
personal life
(marital, family, social relationships); d)
some severe cases, even psychotic decompensations.
positive reformulation of highly stressful experiences; e)
Tese dysfunctions can be reversible or irreversible. A
replacing the less functional coping strategies, focused on
common disorder among individuals frequently and
emotion relief, with more functional ones, focused on
constantly exposed to critical incidents is post-traumatic
problems and solutions. Te intervention comprised of
stress disorder [4].
six meetings with each of the 19 subjects, respecting each
Physical symptoms include: shivers, thirst, fatigue,
subject’s privacy. Five of the six meetings focused on one
nausea, feint or tendency to feint, vertigo, vomiting,
of the five aspects mentioned above and the sixth one
headaches, myalgia, spurts of high blood pressure, chest
consisted of a summarization, a feedback and a chance to
pains, accelerated heartbeat rhythm, muscular tremor.
re-evaluate the subject’s depression and anxiety symptoms.
Generally they can be described as high physiological
Te Hamilton Depression Scale is comprised of 17
responsiveness. At cognitive level one can show:
items of which, 10 items score on a five steps scale, from
confusion, uncertainty, denial,
hyper-vigilance,
0 to 4, while the rest of 7 items score on a three steps
concentration problems, time and space disorientation,
scale, from 0 to 2. Minimum score is 0 and maximum
decrease in decision making. At an emotional and
score is 52. Total scores lower than 7 indicate absence of
affective level, the most frequent symptoms refer to:
clinical depression. Scores between 7 and 17 indicated a
anxiety, self blaming, panic, agitation, irritability,
mild depression. Scores ranged between
18 and 24
impulsivity, depression, anger, fear, suicidal thoughts,
indicate a moderate depression while scores equal or
inadequate emotional responses (either regarding the
above 25 point to a severe depression.
intensity or the nature of expressed emotions), hyper or
Te Hamilton Anxiety Scale consists of 14 items,
hypo-emotionality. And at behavioral level one can find:
scored on a five steps scale, from 0 to 4. Maximum score
social withdrawal, antisocial behaviors, abuse of alcohol
is
56. Scores above 20 show the presence of clinical
and substances, psychogenic flight, impairment in
intensity anxiety.
family and marital relationship [4].
Data were centralized and processed with SPSS for
Windows 10. In order to investigate the differences
Materials and Methods
between pre-intervention and post-intervention anxiety
and depression scores, we used the paired sample t test
Te study was run on a lot of 19 firefighters that
due to the fact that the research design is a two factor
showed some anxiety and depression symptoms. All
within group. All 19 subjects assessed pre-intervention
subjects are males, aged between 27 and 42. Te age
were subjects to the final assessment.
average is 29 years while the standard deviation is 3.77
years. Experience as a firefighter ranges between 6 and
Results
10 years, with a average of 6.42 years and a standard
deviation of 0.96 years. Subjects were selected from the
Initial assessment
entire firefighter personnel periodically assessed
Te scores on the depression scale, at the pre-
according to specific work safety and health norms that
intervention assessment, ranged between 7 and 9, with an
apply within the inspectorates for emergency situations
average of 7.84 and a standard deviation of 0.69. On the
from Romania, on the basis of higher scores on
anxiety rating scale, pre-intervention, subject scored
Hamilton Depression Scale and Hamilton Anxiety
between 9 and 17 with an average score of 11 and a
Scale. Te selection of subjects took in account the
standard deviation of
2. Tus, subjects show a mild
42
Popa et al
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
Original articles
depression and precisely this was the reason to select them
Discussions
into the intervention lot. Te intensity of the anxiety
symptoms is not of clinical level, but as they are associated
We notice that the t values, for anxiety as well as for
with the mild depression symptoms, taken together it
depression are statistically significant at p values lower
could represent a risk factor for developing more severe
than 0.05 thus allowing us to state that anxiety and
emotional, cognitive and behavioral dysfunctions later.
depression levels dropped significantly as a result of the
Post-intervention assessment
psychological intervention. Terefore we can say that
At the end of the intervention another psychological
our intervention achieved its goals, that of improving
assessment of depressive and anxiety symptoms was done.
the firefighters’ emotional wellbeing as shown by the
Results on the anxiety scale show an average score of 9.26
decrease of anxiety and depression symptoms. In the
with a standard deviation of 1.97 and individual scores
case of anxiety, the intervention explains 64% of the
ranging between 6 and 13. On the depression scale, scores
score variance from pre-intervention to post-
range between 4 and 9, with an average score of 6.42 and
intervention, while in the case of depression the
a standard deviation of 1.39. We notice a drop in the
percentage of variance explained by the intervention is
average scores both for anxiety as well as for depression.
as high as
79. Tus, the five step intervention we
Comparing scores at pre-intervention and post-
proposed seems to yield positive outcomes at an
interventions, with the paired sample t test, turned the
emotional and psychological wellbeing.
following results. We must mention that for both rating
Analyzing the post-interventions scores, for each of
scales as well as for both assessments, the distribution was
the 19 subjects we notice that 16 subjects show lower
a normal one. For the anxiety scale, we obtained
scores for depression; 2 subjects show the same score
t(18)=3.511 at p=0.002, and for depression we obtained
while the remaining subject shows an increase form 8 to
t(18)=5.524 at p<0.001. Te magnitude of the differences
9, thus not a dramatic increase. As for anxiety,
15
in scores revealed by the r coefficient shows the following
subjects show lower scores post-intervention, 1 subject
figures: 0.637 for anxiety and 0.793 for depression.
scored identically post and pre-intervention while
3
subjects show an increase in scores post-intervention.
In the case of the subjects were scores increased or
stayed level as well as for anxiety and depression, we
intend to continue the intervention as to improve
subjects emotional and psychological wellbeing as to
identify probable causes which hindered the success of
the intervention. We mention that during the
intervention the 19 firefighters continued to take part in
interventions if needed.
Also, in order to identify new strategies of
intervention we consider necessary to investigate some
other psychological variables which could influence
firefighters’ responses to stress as a consequence of
frequent and constant exposure to critical incidents.
Figure 1. Average scores at the anxiety scale
Such variables are: self-esteem, perceived stress, post-
traumatic stress growth, perceived self-efficacy,
robustness, optimism, sense of coherence, tendency
towards developing somatic symptoms as well as rational
versus irrational beliefs [2].
In this study we start from an actual situation that
we are used to encounter in the daily work as a
psychologist within the firefighter department. Te
firefighters are frequently and constantly exposed to
critical incidents. Events perceived as critical incident by
the firefighters include: self injury, risk of loosing one’s
own life, injury or death of a fellow firefighter,
intervention upon victims in death agony, mostly if
Figure 2. Average scores on the depression scale
these victims are children, taking part in interventions
The Sanogenic Role of Therapeutic Intervention for Firefighters
43
Original articles
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
in which the victims are firefighters’ relatives or
stress, while males tend to isolate themselves, to reduce
acquaintances. Tese all have a major impact on
social interactions and to focus on solutions. Te
firefighters’ physical health and psychological wellbeing.
authors of the research state that these differences in
Although, due to their basic technical training, the
stress response have to do with cumulative action of
negative response to such events can be lowered in
oxytocin, female reproductive hormones and
comparison with common population, it can not be
endogenous opioid mechanisms, thus favoring females’
eliminated. Tus, the psychologist’s role in this context
pro-social behaviors, while in males’ case, testosterone
is to monitor periodically the psychological state of the
seems to block oxytocin’s effects and activate the
firefighters but also to intervene precisely through
adrenergic system, thus favoring a flight or fight
defusing and debriefing or more largely through a
response.
psychological intervention with more profound
It is highly probable that in certain cases in which
therapeutic valence.
the emotional blockage of firefighters is related with the
Te defusing represents a volunteer, short,
belief that conceiving the existence of distress due to
individual meeting, in complete privacy that aims
frequent and constant exposure to critical incidents
mainly to defuse the psychological and physical tension
might lead to negative responses from the superiors and
of the firefighters. It has to take place short time after
fellow firefighters, our approach focused on awareness
the incident, recommended at 4 hours but not later
and acceptance of one’s own experiences might not
than 12 hours and does not have to be too formal;
work to well. Tus, we consider changing the focus of
actually it is recommended to be as least formal as
the intervention towards functional coping strategies or
possible [4]. Te defusing is focused on the awareness
alternative activities through which firefighters might
and acceptance of one’s own feeling as normal and on
experience positive emotions and feelings, such as
the adaptive or non-adaptive role of action taken post-
hobbies [9].
event.
Te debriefing is a more formal meeting, run within
Conclusions
the group that took part in the incident, at an interval of
about 24-72 hours and it focuses on different coping
Our study shows that a short-term psychological
ways [4].
intervention, centered on explicit goals, on problems
Research in the field of clinical and health
and solutions, on positive reformulation of experiences
psychology show that most recommended types of
without neglecting awareness and acceptance of the
psychological interventions regarding the firefighters are
client’s intense emotional responses in highly stressing
the short-term ones, focused on problems and solutions
situations and also these reactions’ consequences on
[4,5].
individual’s, his family and peers’ physical and
Te firefighter activity is characterized by a strong
psychological wellbeing can lead to a significantly
male stereotype
[6] which significantly cumbers the
improvement of anxiety and depression symptoms. Yet,
psychological counselor’s activity due to the fact that a
there are individuals for which our intervention does
direct approach towards emotional and affective
not work. Terefore we must strive to improve our
experiences could be perceived like imposing an alien
approach by looking for the causes of the intervention
model thus triggering resistance or avoidance of the
failure as well as trying to find other psychological
counseling process. An approach focused on behavioral
variables that could enable us to improve the
aspects, on more practical features like actions, decisions
psychological intervention process. Te diversity of
is far more recommended.
therapeutic approaches and that of therapeutic methods
Male individuals have greater difficulties in speaking
available at the present allow us to develop improved
open about feelings, emotions and affective states.
therapeutic interventions.
Avoiding emotions and feelings is explainable but does
not represent a functional coping mechanism. Such a
confrontation process requires conscious effort and
References
involvement on the side of the client. McFarlane [7]
shows that avoidance is a weak coping mechanism and
1. Burns, C., Rosenberg, L. Redifining critical incidents:
is a factor which makes more probable the development
a preliminary report. International Journal of
of post-traumatic stress. A research on stress response in
Emergency Menthal Health, 2001;3 (1),17-24.
females in comparison with that of the males [8] points
2. Băban, A. Stres şi personalitate. Editura Presa
that females tend to initiate social interactions under
Universitară Clujeană, Cluj-Napoca, 1998.
44
Popa et al
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
Original articles
3. Iamandescu, I.-B. Stresul psihic din perspectivă
Interdisciplinary Journal of Applied Family Studies
psihologică şi psihosomatică. Editura Info Medica,
2005;54(3),423-35.
Bucureşti, 2002.
7. McFarlane, A. Avoidance and intrusion in posttraumatic
4. Maier, R. Stres, stres, stres. Editura Gutenberg Univers,
stress disorder.
Journal of Nervous and Mental
Arad, 2011.
Diseases 1992;180,439-45.
5. Holdevici, I. Psihoterapia anxietăţii. Abordări cognitiv-
8. Taylor, S.E., Klein, L.C., Lewis, B.P., Gruenenwald,
comportamentale. Editura Dual Tech, Bucureşti,
T.L., Gurung, R.A.R., Updegraff, J.A. Biobehavioral
2002.
responses to stress in females: tend-and-befriend not fight-
6. Regehr, C., Dimitropoulos, G., Bright, E., George,
or-flight. Psychological Review 2000;107(3),411-29.
S., and Henderson, J. Behind the brotherhood: Rewards
9. Holdevici, I. Psihologia succesului. Autosugestie şi
and challenges for wives of firefighters. Family Relations:
relaxare. Editura Universitară, Bucureşti, 2010.
The Sanogenic Role of Therapeutic Intervention for Firefighters
45
Medical Connections/Conexiuni Medicale
Conflict-of-Interest Statement
Medical Connections/Conexiuni Medicale (Med Con) requires all authors and reviewers to declare any
conflicts of interest that may be inherent in their submissions.
Conflict of interest for a given manuscript exists when a participant in the peer review and publication
process-author, reviewer, or editor - has ties to activities that could inappropriately influence his or her
judgment, whether or not judgment is in fact affected.
Financial relationships with industry, for example, through employment, consultancies, stock
ownership, honoraria, expert testimony, either directly or through immediate family, are usually considered
to be the most important conflicts of interest. However, conflicts can occur for other reasons, such as
personal relationships, academic competition, and intellectual passion.
Public trust in the peer review process and the credibility of published articles depend in part on how
well conflict of interest is handled during writing, peer review, and editorial decision making. Bias can
often be identified and eliminated by careful attention to the scientific methods and conclusions of the
work. Financial relationships and their effects are less easily detected than other conflicts of interest.
Participants in peer review and publication should disclose their conflicting interests, and the information
should be made available so that others can judge their effects for themselves.
Authors: When they submit a manuscript, whether an article or a letter, authors are responsible for
recognizing and disclosing financial and other conflicts of interest that might bias their work. Tey should
acknowledge in the manuscript all financial support for the work and other financial or personal
connections to the work.
Reviewers: External peer reviewers should disclose to editors any conflicts of interest that could bias
their opinions of the manuscript, and they should disqualify themselves from reviewing specific
manuscripts if they believe it appropriate. Te editors must be made aware of reviewers’ conflicts of interest
to interpret the reviews and judge for themselves whether the reviewer should be disqualified. Reviewers
should not use knowledge of the work, before its publication, to further their own interests.
Manuscript Title: _ __________________________________________________________
I declare no conflict of interest
I declare the following potential conflict of interest:
_ _________________________________________________________________________
_ _________________________________________________________________________
_ _________________________________________________________________________
_ _________________________________________________________________________
_ _________________________________
_ _________________________________
Name
Signature/Date
Please fax or mail this signed form to the Med Con Editorial Office.
Fax: +40-261-710456
Mail: colmedsm@gmail.com
GENERAL REVIEW
RELATIONSHIP BETWEEN TP53 AND FGFR3 MUTATIONS IN SUPERFICIAL
BLADDER CANCER
Prunduş Paul¹, Stanca Vasile Dan², Nicolescu Sergiu¹, Coman Ioan²
¹Department of Urology, Clinical Municipal Hospital Cluj-Napoca, Romania, ²University of Medicine and Farmacy
“Iuliu Haţieganu” Cluj-Napoca, Romania
Address for correspondence:
Paul Prunduş
Department of Urology, Clinical Municipal Hospital Cluj-Napoca, Romania
Email: prunduspaul@yahoo.com
Received: 02.12.2012
Accepted: 15.02.2013
Med Con March 2013, Vol 8, No 1, 47-52
Abstract
men and the 17th most prevalent cancer in women, with
an incidence of 30 cases per 100.000 inhabitants in
Bladder cancer is one of the most common cancers
Europe.
worldwide, being a disease of the elderly with a peak
According to SEER estimations
(Surveillance
incidence in the sixth decade of life.
Epidemiology and End Results) of NCI
(National
Tumors that are invasive have a high risk of
Cancer Institute), in 2007 were 67.160 pacients with
progression despite radical cystectomy and other
bladder cancer (50.040 men and 17.120 women) in
treatments. Tere are efforts made to identify markers
SUA. Te number of deceased in 2007 it is approximately
that predict recurrence and progression of the disease,
13.750.
response to treatment, and survival.
Between 2000-2004, the median age for bladder
Bladder tumors develop through different molecular
cancer diagnosis was 73 years old. Approximately 0.1%
pathways. Recent reports suggest that activating
of the pacients were diagnosed under the age of 20 years
mutations of the fibroblast growth factor receptor 3
old, 0.6% between 20 and 34 years, 2.1% between 35-
(FGFR3) gene as marker for the “papillary” pathway
44 years, 7.8% between 45-54 years, 17.2% between
with good prognosis, in contrast to the more malignant
55-64 years,
28.5% between
65-74 years,
31.9%
“carcinoma in situ” (CIS) pathway. Over expression of
between 75-84 years, and 11.8% over 85 years. Te age
P53 in the nucleus, detected by use of
incidence rate per year was 21.1 per 100.000 cases in
immunohistochemical techniques, is commonly
men and women [1,2,3].
regarded as a surrogate marker for P53 mutation, and
More than 90% of bladder cancers are carcinomas,
has been the most widely investigated molecular marker
which are presenting at different stages. Te current
in bladder cancer in the past decade.
bladder cancer staging is performed considering the
Keywords: bladder cancer, FGFR3 gene, protein
histopatological examination and is based on the 2002
p53, genetic mutations, disease progression
revison of UICC classification
(International Union
Against Cancer).
Introduction
Superficial bladder tumors are representing by: Ta
tumors (papillary, generally low-grade tumors, which do
Bladder cancer is one of the most common cancers
not invade beyond the basement membrane), carcinoma
worldwide. It is the seventh most prevalent cancer in
in situ (CIS - is a flat tumor with a high grade, which
Relationship Between TP53 and FGFR3 Mutations in Superficial Bladder Cancer
47
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
generally does not invade de basement membrane) and
such as embryogenesis, development, and wound
T1 tumors (invade the subepithelial connective tissue but
healing, and a range of pathological conditions. Te
up to muscularis propria). On the other hand, infiltrative
effects of FGFs are mediated by a family of four
bladder cancer defines tumors that have invaded at least
fibroblast growth factor receptors (FGFR1-4). FGFRs
the detrusor muscle (pT2, pT3, pT4) [4].
are transmembrane glycoproteins with a conserved
In what concerns the superficial bladder tumors,
structure comprising an extracellular portion with two
30% of the pacient will not present reccurence, however
to three immunoglobulin-like domains
(IgI-III), a
70% will develop at least one recurrence; 10-20% of the
transmembrane domain, and an intracellular split
cases will develop progressive infiltrative disease. On
tyrosine-kinase domain [12].
presentation, 70-80% of bladder tumors are superficial
Te gene that codifies the fibroblast growth factor
(70% pTa and 30% pT1) [5].
receptor 3 belongs to tyrosine kinases receptors. Te
Te pTa and pT1 bladder tumors have substantial
FGFR family includes more members participating at
differences concerning the risk of progression to muscle
the regulation of cell proliferation, cell migration and
invasion. Te progression appears in only 3% of pTa
differentiation during embryogenesis and in tissue
tumors, while the percentage reaches
30% for pT1
regeneration process. Te inadequate gene expression
tumors [6]. Te risk of progression is highly corelated
for fibroblast growth factor can contribute to bladder
with mortality: less than 1% for pTa tumors, while 24%
cancer pathogenesis by altering the angiogenesis or by
for pT1 tumors [7,8,9].
direct effect on stimulation of tumor cells. Te fibroblast
Genetics in bladder cancer
growth factors exercise their functionality by 4 receptors
Te assessment of the genetic substrate of bladder
(FGFR1-4). More evidence claims that the activation of
tumors offers a whole now and promising perspective.
FGFR3 mutation is responsible for its oncogenic role in
Although the „superficial bladder tumors” term includes
urothelial tumors development. Te FGFR3 mutations
pTa, pT1 and CIS, in the light of current genetic data,
are specific for urothelial cancer, occurring in over 40%
this subdivision is totally inappropriate because their
of the tumors [13,14].
genetic substrate is different; this fact determinates
Te FGFR3 protein overexpression has been more
different behaviors regarding invasion and metastasis
frequently present in cases of well differentiated urothelial
capacity. Te tumors that have penetrated the basement
tumors, in comparison to poorly differentiated,
membrane (pT1) and CIS are considered high risk
respectivly in low tumoral stage in comparison to
lesions in opposition with pTa tumors which tend to
advanced tumoral stage. Tis observations confirms the
recur, but not progres.
hypothesis that FGFR3 expression has a role in the early
Tere are clinical and molecular evidence for the
development of urothelial neoplasia [15].
existence of two pathways of bladder tumor progression
Subsequent larger studies established that FGFR3
and development: the CIS and Ta pathways. CIS
mutations occur in around 50% of both lower and
progress in about 50% of cases to T1 stage and after that
upper urinary tract tumours and these cluster in three
to muscle-invasive tumors [10,11].
distinct hotspots in exons 7, 10, and 15 [27-32] (Figure
FGFR3 mutations in superficial bladder tumours
1). Te most common mutations in exon 7 and 10 are
Lower grade pTa tumors
(G1-G2) have few
S249C (~61%), Y375C (~19%), R248C (~8%), and
molecular altereations. Despite the efforts of many
G372C (~6%), with others occurring at very low
laboratories that have tested hundreds of tumors , only
frequencies (<2%) [16].
two alterations have been described: deletions of part or
Literature studies have demonstrated the FGFR3
of the entire chromosome 9 and FGFR3 mutations
overexpression
through
immunohistochemistry
(fibroblast growth factor receptor 3).
techniques in 83% of pTa tumors, 100% in pT1 tumors
In addition, lower grade pTa tumors are highly stable
and 50% of pT2 tumors. At the same time, the FGFR3
genetically. Te study of synchronous or metachronous
mutation was present in 64-74% of pTa tumor cases,
tumors from the same pacient revealed the same genetic
0-21% of pT1 tumors, and 0-16% of pT2 tumor cases.
alterations. Te loss of chromosome 9 heterozygozity is
Tese findings indicate that the FGFR3 expression
less divergent in time event, while the FGFR3 mutation
is more frequent than the activating mutation of the
is significantly identified in bladder tumors only.
gene. Tis difference between the protein overexpression
In humans, fibroblast growth factors are a family
and the activating mutation of the gene, especially in
comprising
18 growth factors
(FGFs) and 4 FGF-
case of pT1 tumors, raise the suspicion of a new protein
homologous factors (FHFs), many of which play a
overexpression mechanism, other than gene activation
crucial role during both normal physiological processes,
[17,18].
48
Prunduş et al
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
GENERAL REVIEW
Te frequency of FGFR3 mutations decreased with
differences between minimally invasive tumors (pT1)
increasing stage and grade: 65% in pTa, 30.2% in pT1,
and profound tumors (pT2-4) are minimum, sugesting
11.5% in pT2-4 and 69.8% in G1, a very similar rate in
that the tumors which have the abillity to invade and
G2 (68%) and 18.6% in G3. Tese trends, for both
pass the basement membrane are aggressive lesions [23.]
stage and grade, were highly significant (p<0.0001 and
TP53 is a tumor suppressor gene, located on the
p<0.0001, respectively). For pTa tumors, the most
short arm of chromosome 17. Tis gene mutation is
common of the four possible groups (wild-type FGFR3
relatively frequent in human tumor pathology, being
plus wild-type TP53, wild-type FGFR3 plus mutated
present in approximately
50% of malignancies. Te
TP53, mutated FGFR3 plus wild-type TP53, mutated
TP53 function in very complex - it is considered “the
FGFR3 plus mutated TP53) was tumors with mutated
guardian of the genome” with an important role in cell
FGFR3 and wild-type TP53 (61.9% of cases), followed
cycle regulation, DNA repair - and cell apoptosis. TP53
by tumors wild-type for both FGFR3 and TP53 (31.5%
overexpression is associated with tumor grade and stage,
of cases) [19].
having an independent predictive value for tumor
FGFR3 mutation status has been investigated as a
recurrence. Despite of the multiple studies, the TP53
prognostic marker for survival, recurrence and bladder
role in the bladder tumor patient’s management is still
tumors progression. A small study including a number of
poorly known, that is why the current use of this gene
53 pTaG1-2 bladder tumors showed that wild-type
mutation in practice is somewhat limited.
FGFR3 is predictive of disease recurrence [20]. In contrast,
TP53 mutation in bladder cancer is detected by
in a subsequent larger study of 764 superficial bladder
polymerase
chain
reaction
(PCR)
and
tumors FGFR3 mutation was predictive of a higher rate of
imunohystochimical analysis. Sidransky et al. detected
recurrence in TaG1 but not TaG3 or T1 tumors [21].
the p53 mutation in 11 cases of 18 patients with bladder
After a study, Fauceglia et al. concludes that FGFR3
cancer, Fujimoto et al. detected mutations in 7 of 23
gene mutation is a strong indicator for a low rate of
cases of bladder tumors, and Spruck et al detected the
recurrence in case of pTa urothelial tumors. At the same
gene mutation in 29 of 80 patients [14,24].
time, no prognostic value of the protein FGFR3
Furthermore, no differences were observed between
overexpression in the recurrence prediction or bladder
genetical alterations in pT1 tumors and the metastasis
tumor progression was found - due to the relatively low
of these tumors [22]. FGFR3 mutation seems to define
patient follow up (12 months) [14].
superficial tumors, while TP53 mutation is characteristic
In his study which included 100 patients diagnosed
in tumors exceeding the basement membrane; these
with bladder tumor, Junker et al. found the FGFR3
alterations however seem to be mutually exclusive.
mutation in
48.9% of patients. Te frequency of
Hernandez et al. in a study of a large series of tumors
FGFR3 mutations according to the tumor stage T was:
suggests that FGFR3 and TP53 mutations were
pTa - 61%, pT1 - 40%, pT2/3 - 0%. Te FGFR3
independent events in pT1G3 tumors and also in pTa,
mutation is significantly associated with the degree of
pT1G2 and muscle-invasive tumors (pT≥2). By contrast,
tumor differentiation: G1 - 70%, G2 - 46%, G3 - 4%.
FGFR3 mutations and TP53 mutations were not
In case of pTaG1 tumors, the mutation has been
independent events if we considered all tumors together,
found in 72% of cases. Tese results confirm the fact
without accounting for stage and grade , or all pT1
that the FGFR3 mutation characterizes low grade non-
tumors together (pT1G2 and pT1G3 tumors) [24].
invasive bladder tumors, representing an important
Tere is no proven association between the FGFR3
prognostic marker for bladder tumors with low
expression and TP53. Te overexpression of FGFR3/
potential, and may represent a surrogate maker for the
TP53K represents a favorable path in bladder
detection of genetically stable bladder tumors, with
carcinogenesis and singular FGFR3 overexpression is
good clinical and oncological results [22].
unlikely to have predictive value for bladder tumors
FGFR3 expression is significantly associated with
[13,25,26].
two important prognostic factors: stage and grade and
Te multifocal bladder tumor existence, a volume
the protein expression is not an independent predictive
exceeding 3 cm, the CIS coexistence, the response to
factor for pTa/pT1 tumour recurrence and progression.
intravesically chemotherapy, the existence of early
TP53 mutation in superficial bladder cancer
recurrence and the histological grade of bladder tumor
PT1 tumors have a much more diverse genetically
are variables which taken individually or collectively
substrate. Tere have been identified mutations of gene
provide us information on the prognosis of bladder
p53, ERBB2, PTEN, deletions of chromosomes 8p,
tumors, especialy in T1 tumors (25-30% of T1 bladder
11p, 18q,4q, etc. Significant is the fact that the genetic
tumors present progression with the invasion of the
Relationship Between TP53 and FGFR3 Mutations in Superficial Bladder Cancer
49
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
muscularis after 2 years, and this percentage rises up to
method which allowed doctors to determine the most
40% in case of T1G3 bladder tumors) [27].
useful adjudvant therapy for patients after endoscopic
In early tumoral stages - pTaG1 and pTaG2, the
resection. Data from 2596 patients with pTa, pT1 or
frequency of FGFR3 mutation was high in the Ta low-
Tis was used to develop a prognostic index.
grade pathway, whereas that of TP53 mutation was very
Te variables representing prior recurrence rate,
low. If those tumours progress to muscle-invasive
number of tumors, the tumor size, the T stage, and the
tumours, they will carry TP53 mutations at a frequency
carcinoma in situ presence were included in the final
similar to that in tumours of the CIS pathway. For
multivariable model to determine the time of the first
tumours of the Ta pathway, the frequency of TP53
recurrence and time of progression [30].
mutations seems to increase gradually with stage, from
A meta-analysis regardind the relationship between
pTa (5% of tumours) to pT1 ( TP53 mutations in 27%
FGFR3 and TP53 mutations in bladder cancer has
of tumours) and pT2-4 tumours (TP53 mutations in
found that FGFR3 and TP53 mutations occurred
42% of tumours).
independently when stage and grade were taken into
Tumoral grade also seems to be important, the
account. Te frequency of TP53 mutation was high in
frequency of TP53 mutation was
17% in pT1G2
pT1G3 and pT2-4 tumours, regardless of the presence
tumours and 37% in pT1G3 tumours.
or absence of FGFR3 mutations in these tumours. TP53
FGFR3 mutation frequency was found to be very
mutations can occur in Ta pathway tumours, when
similar in pTa G1/G2 and pT1G2 tumours, suggesting
these tumours progress.
that most of pT1G2 tumours are derived from the Ta
Bladder tumors of different degrees and at different
pathway rather than the CIS pathway. Te variability of
stages have specific phenotype and genotype. Although
FGFR3 and TP53 mutations when all pT1 tumours are
the recognition of molecular changes by analyzing tumor
considered together, reflect the two different pathways
tissue, urine and blood samples is possible, few of these
of bladder cancer development, Figure 1 [21].
molecular markers are used in clinical practice. Studies
A high proportion of bladder cancers present a
are needed to determine the accuracy of these genetic
wild-type phenotype (no FGFR3 or TP53 mutations):
markers and their use widespread, in order to improve
32% of Ta tumors, 40% of T1 tumors and 43% of T2-4
treatment of bladder cancer. Clinical utility of molecular
tumors). Tese tumors probably have mutations in
markers already discovered cannot be deteremined until
genes other than FGFR3 or TP53, but with a similar
several multicenter prospective studies will establish the
effect (activation of the FGFR3 signaling pathway in Ta
efficacy, the safety and their predictive value in
tumors of low grade and mutations of genes causing
monitoring patients with bladder cancer.
genetic instability in high-grade or high-stage tumors).
In the last time, FGFR3 and TP53 play a key role in
RAS mutations, which are observed in about 10% of
the development of bladder cancer and promise as
bladder cancers and are never found with FGFR3
therapeutic targets, screening tools, and diagnostic, and
mutations, are thought to affect the FGFR3 signaling
prognostic biomarkers. Future challenges include
pathway [28,29].
refining FGFR-based screening and prognostic tests,
In 2006, Sylvester et al. published a method for
identification of markers to select patients most likely to
predicting recurrence and progression for every patient,
benefit from FGFR-targeted therapies and development
of strategies to overcome recurrence after treatment
withdrawal or development of resistance.
Te results of research on the role of FGFR3 and
TP53 in bladder cancer will be translated into the
clinical management for bladder tumours.
References
1. Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer
statistics, 2002. CA Cancer J Clin 2005;55:74-108.
2. Murta-Nascimento C, Schmitz-Dräger BJ, Zeegers
MP, et al. Epidemiology of urinary bladder cancer: from
tumour development to patient’s death. World J Urol
Figure 1. FGFR3 activation and TP53 mutation: the two-
pathway model of different types of bladder cancer development
2007;25:285-95.
50
Prunduş et al
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
GENERAL REVIEW
3.
Jemal A, Tiwari RC, Murray T, et al. Cancer statistics,
urothelial papilloma. Te Journal of Pathology
2004. CA Cancer J Clin 2004;54(1):8-29.
2002;198(2):245-51.
4.
Burger M, van der A MNM, van Oers JMM,
17.
Gomez-Roman JJ, Saenz P, Cuevas Gonzalez J,
Brinkmann A, van der Kwast TH et al. Prediction of
Escuredo K, Santa Cruz S, Junquera C, et al.
Progression of Non-Muscle-Invasive Bladder Cancer by
Fibroblast growth factor receptor 3 is overexpressed in
WHO 1973 and 2004 Grading and by FGFR3
urinary tract carcinomas and modulates the neoplastic
Mutation Status: A Prospective Study. European
cell growth. Clin Cancer Res 2005;11:459-65.
Urology 2008;54,835-44.
18.
Matsumoto M, Ohtsuki Y, Ochi K, Seike Y, Iseda N,
5.
Donat SM. Evaluation and follow-up strategies for
Sasaki T, et al. Fibrosblast growth factor receptor
3
superficial bladder cancer. Urol Clin North Am
protein expression in urothelial carcinoma of the urinary
2003;30(4):765-76
bladder, exhibiting no association with low-grade and/or
6.
Heney NM, Ahmed S, Flanagan MJ, et al. Superficial
non-invasive lesions. Oncol Rep 2004;12:967-71.
bladder cancer: progression and recurrence. J Urol
19.
Yann N et al. A Meta-Analysis of the Relationship
1983;130(6):1083-6.
between FGFR3 and TP53 Mutations in Bladder
7.
Abel PD. Follow-up of patients with
“superficial”
Cancer. PLoS One 2012;7(12):e48993
transitional cell carcinoma of the bladder: the case for a
20.
vanRhijn BWG, Lurkin I, Radvanyi F, Kirkels WJ,
change in policy. Br J Urol 1993;72(2):135-42.
van der Kwast TH, Zwarthoff EC. Te fibroblast
8.
Herr HW, Wartinger DD, Fair WR, Oettgen HF.
growth factor receptor 3 (FGFR3) mutation is a strong
Bacillus Calmette-Guerin therapy for superficial
indicator of superficial bladder cancer with low
bladder cancer: a
10-year followup. J Urol
recurrence rate. Cancer Research 2001;61(4):1265-8.
1992;147(4):1020-3.
21.
Hernández S, López-Knowles E, Lloreta J, et al.
9.
Jeremy L, Abe PD. Treatment Options in Superficial
Prospective study of FGFR3 mutations as a prognostic
(pTa/pT1/CIS) Bladder Cancer. In: Urological cancers
factor in nonmuscle invasive urothelial bladder
in clinical practice, Springer-Verlag, London Limited,
carcinomas.
Journal
of
Clinical
Oncology
2007,75-102.
2006;24(22):3664-71.
10.
Spruck CH 3rd, Ohneseit PF, Gonzalez-Zulueta M,
22.
Junker K, Zwarthoff E, Van Oers J, Kania I, Schubert
Esrig D, Miyao N, et al. Two molecular pathways to
J. Low Frequency of chromosomal alterations in CGH
transitional cell carcinoma of the bladder. Cancer Res
analysis in low-risk papillary bladder tumours with
1994;54:784-8.
FGFR3 mutations. European Urology Suppliment
11.
4. Billerey C, Chopin D, Aubriot-Lorton MH, Ricol
2006;5(2):77.
D, Gil Diez de Medina S, et al. Frequent FGFR3
23.
Knowles MA. Molecular Biology of Bladder Cancer. in J
mutations in papillary non-invasive bladder
(pTa)
Waxman. Urological Cancers, Springer, 2005;115-30.
tumors. Am J Pathol 2001;158:1955-9
24.Hernández S, López-Knowles E, Lloreta J, Kogevinas
12.
di Martino E, Darren C, Tomlinson M, Knowles A. A
M, Jaramillo R, et al. FGFR3 and Tp53 mutations in
Decade of FGF Receptor Research in Bladder Cancer:
T1G3 transitional bladder carcinomas: independent
Past, Present, and Future Challenges. Adv Urol
distribution and lack of association with prognosis. Clin
2012;2012:429213.
Cancer Res 2005;11:5444-50.
13.
Mhawech-Faucegliaa P, Cheneya RT, Fischerb G,
25. Kawasaki T, Tomitaa Y, Watanabea R, Tanikawaa T,
Becka A, Herrmannb FR. FGFR3 and p53 protein
Kumanishi T, Satoa S. mRNA and protein expression of
expressions in patients with and pT1 urothelial bladder
~53 mutations in human bladder cancer cell lines.
cancer. EJSO 2006;(32),231-7.
Cancer Letters 1994;(82)113-21
14.
Takahashi T, Habuchi T, Kakehi Y, et al. Clonal and
26.Hovey RM, Chu L, Balasz M et al. Genetic alterations in
chronological genetic analysis of multifocal cancers of the
primary bladder cancers and their metastases. Cancer
bladder and upper urinary tract. Cancer Res
Res 1998;58(16):3555-60
1998;58(24):5835-41.
27. Alonso AR, Fernandez SP, Carrero JG. p53 and ki67
15.
Kimura T, Suzuki H, Ohashi T, Asano K, Kiyota H,
expression as prognostic factors for cancer
- related
Eto Y. Te incidence of thanatophoric dysplasia
survival in stage T1 transitional cell bladder carcinoma.
mutations in FGFR3 gene is higher in low-grade or
European Urology 2002;(41)182-9.
superficial bladder carcinomas. Cancer 2001;92:2555-
28. Wu XR. Urothelialtumorigenesis: a tale of divergent
61.
pathways. Nat Rev Cancer 2005;5:713-25.
16.
vanRhijn BWG, Montironi R, Zwarthoff EC, Jöbsis
29. Jebar AH, Hurst CD, Tomlinson DC, Johnston C,
AC, van der Kwast TH. Frequent FGFR3 mutations in
Taylor CF, et al. FGFR3 and Ras gene mutations are
Relationship Between TP53 and FGFR3 Mutations in Superficial Bladder Cancer
51
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
mutually exclusive genetic events in urothelial cell
patients with stage Ta T1 bladder cancer using EORTC
carcinoma. Oncogene 2005;24:5218-25.
risk tables: a combined analysis of 2596 patients from
30. Sylvester RJ, van der Meijden AP, Oosterlinck W, et
seven EORTC trials. EurUrol
2006;49:466-77
al. Predicting recurrence and progression in individual
(discussion 475-7).
52
Prunduş et al
GENERAL REVIEW
ETIOLOGY OF POSTOPERATIVE ASTIGMATISM AFTER CATARACT
SURGERY
Pop Rodica1, Pop Radu2
1Integrated Ambulatory of the Clinic of Infectious Diseases Cluj-Napoca, 2Ophthalmology Clinic Cluj-Napoca
Address for correspondence:
Pop Rodica;MD
3 Mestecenilor St, Bloc 9L, Sc. II, Et. 4, Ap. 19, Cod 400348, Cluj-Napoca, Jud. Cluj
Tel: 0723147278
E-mail: pop_rodica_1957@yahoo.com
Received: 10.12.2012
Accepted: 20.02.2013
Med Con March 2013, Vol 8, No 1, 53-58
Abstract
numerous studies were made concerning postoperative
astigmatism after cataract surgery, at first related to the
Postoperative astigmatism after cataract surgery
intra capsular extraction and later on to the extra
depends mainly on it’s preexisting, on factors that are
capsular extraction. Since 1982, in the cataract surgery
related to the surgical act and also on the characteristics
has been the practice of extra capsular extraction with
of the intraocular lens. Over time there have been
implantation of intraocular artificial lens. Te progresses
numerous studies concerning mainly the effects of
made in this surgical technique further allowed the
corneal healing on its curvature and on its refractive
introduction and utilization on a larger scale of the
stability. An important role in the apparition of this
extraction of cataract through phacoemulsification and
astigmatism has the type of the surgical incision: sutured
of foldable artificial lens implantation.
or not sutured, size, depth and the incision’s location.
Surgical induced astigmatism is the astigmatism
Nowadays, the not sutured incision, in clear cornea, is
larger than 1 diopter, with-the-rule or against-the-rule,
the most frequent technique used in the extraction of
which is present at 6-8 weeks postoperatively [2]. Tis
the
cataract
with
phacoemulsification.
Te
form of astigmatism may compromise the postoperative
improvements brought lately to cataract surgery follow
functional results, after the cataract surgery, increasing
a good healing and remodeling of the wound, which
postoperative astigmatism.
ensures the refractive stability of the cornea.
Te etiologic factors that can be associated with
Keywords: Postoperative astigmatism, clear corneal
postoperative astigmatism are: preoperative astigmatism
incision, refractive stability
and factors that are related to the surgical procedure.
Introduction
Preoperative astigmatism
Te major objective of cataract surgery is a good
Larger preoperative astigmatism can be associated
functional result, with an optimal visual acuity, without
with increased values of postoperative astigmatism after
optic correction.
cataract surgery [3]. Studies showed that nearly 15-29% of
Donders (1864) was the first who showed that the
the patients who undergo cataract surgery have a
alteration of the corneal curvature is an unpleasant
preexistent astigmatism larger than
1.5 diopters
[4].
consequence of cataract surgery
[1]. Over time,
Reducing this type of astigmatism during cataract surgery
Etiology of Postoperative Astigmatism after Cataract Surgery
53
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
may improve the postoperative visual results, especially
sutures with absorbable sutures and wound compression
when a multifocal artificial lens is implanted. So, the
which appears in cases with sutures with non-absorbable
correct value of the astigmatism, during cataract surgery
sutures. Comparative studies were performed on eyes
must be equal with the sum of the vectors of the preexistent
operated of cataract with monofilament sutures and
astigmatism and the surgically induced astigmatism [5].
with sutures with natural silk threads, taking into
Te correction of preexistent astigmatism can be
consideration the importance of the relations between
made during cataract surgery through incision
changes in the corneal curvature after the removal of the
techniques, like handling these for the flattening of the
monofilament and after the biodegradability of the silk
most refractive corneal meridian or by implantation of
thread [14]. Tus, in cases of monofilament sutures, the
an artificial toric intraocular lens. Both methods can
power and the cylinder axis were constant as long as the
reduce a small to moderate astigmatism [6]. According
sutures remained in place. After their removal,
to other authors, preoperative astigmatism can be
postoperative astigmatism was significantly reduced due
corrected during cataract surgery, using different
to the decreasing of tension produced by monofilament
methods that include relaxing peripheral incisions,
sutures, in the wound. In case of absorbable sutures, the
choosing the incision’s location or implantation of an
value of the cylinder axis varied, and the healing was
artificial toric intraocular lens [7,8].
associated with a local inflammatory reaction.
Surgical induced astigmatism: can be correlated
Deepness of wound. Te process of corneal wound
with a multitude of factors, such as factors related to the
healing involves epithelial cells and fibroblasts in the
incision and factor related to the intraocular artificial lens.
anterior segment and endothelial cells in the posterior
Factors related to the incision
segment
[15]. Trough studies on humans and
Type of wound, sutured or not sutured. In case of sutured
monkeys, in case of unsutured wounds, it was observed
wound, postoperative astigmatism depends on the length,
that the morphology of the scar tissue differs depending
depth and tightness of the suture [9]. Tus, long sutures,
on wound depth [11]. Tus, in the anterior regions it
placed near each other, create a tissue compression, leading
was found an early restoration, almost anatomical,
to a with-the-rule astigmatism. Widely separated sutures,
pseudolamelar, while in the posterior regions they were
and also less tight sutures, determine an against-the-rule
disorganized. Tese regional differences of healing are
astigmatism. Sutures which are too superficial tend to
supposed to be due to local mechanical factors, such as
eliminate themselves spontaneously, leading to against-
removing the fibrin plug or due to intrinsic properties of
the-rule astigmatism. In sutured wounds, as long as the
different healing between stromal layers.
stitches are in place, the postoperative astigmatism remains
Location of the incision in relation to the limbus. Te
constant, and after their removal this astigmatism induced
incisions in cataract surgery can be: scleral, limbic or
by sutures removes itself [10].
corneal [16].
On the other hand, studies have shown that on the
Te scleral incision it is also called a scleral tunnel.
same cornea, the healing of sutured and suture less
Because it is located posterior, it minimizes the corneal
wounds is different [11]. Tus, sutured wounds initially
deformation which is stabilized by the limbic ring, with
heal more slowly, but over time, obtain a pseudolamellar
a minimum postoperative astigmatism. Another
continuity. In contrast, not sutured wounds are
advantage is that it’s watertight, it’s self-sealing, thus not
characterized by an early healing, almost lamellar, but
requiring suturing, but when is less efficient it determines
may be followed by an inefficient regeneration of the scar.
a postoperative astigmatism. Te more scleral the
Degree of suture tightening. Tis is another factor
incision the lower is the value of the astigmatism.
identified to be responsible for postoperative astigmatism.
Te limbic incision can be done in the anterior part
A large suture allows the cornea to become flat, reducing
of the limbus across the cornea, in the middle or at the
the curvature in the vertical meridian and against-the-
posterior part, along the sclera. Incisions located in the
rule astigmatism. If the suture is too tight, it stretches the
anterior part heal slower, while the incisions situated in
cornea vertically, increasing the curvature in the meridian
the posterior part require sutures, with postoperative
and causing with- the-rule astigmatism [12].
astigmatism.
Suture material used. Changes in corneal curvature
Te corneal incision it is done without involving
after cataract surgery, in case of operated sutured
the conjunctiva or the sclera, and it is also called clear
wounds, differ depending on the suture material used,
cornea incision. Tis causes a minimal inflammatory
resorbable or nonresorbable. According to Jaffe and
reaction, does not require diathermy, thus avoiding the
Clayman [13], the main factors responsible for these
coagulation of collagen fibers. When it is small (about 3
changes are wound dehiscence which occurs in cases of
mm), the postoperative astigmatism is minimal, the
54
Pop et al
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
GENERAL REVIEW
healing and recovery time is short. In this respect, the
having the form of flute’s mouthpiece and has a
literature data show that the incision of 2.8 mm in clear
significant leak. Te wound is small, so postoperative
cornea induces small refractive changes, at least in the
astigmatism is minimal [20].
eyes with small preoperative corneal astigmatism,
Te three planes incision refers to the scleral tunnel.
regardless of the incision’s location [17]. Tis type of
In this approach, first it is made a perpendicular incision
incision is recommended only in case of foldable
in the scleral area, afterwards the intralamelar space is
artificial lens implantation. It is not recommended in
then dissected horizontally, and finally the anterior
cases of rigid intraocular lens implantations, when the
chamber is penetrated by an oblique incision. Tis
surgical wound must be equal to or greater than 5 mm,
incision is usually used in the phacoemulsification
because the postoperative astigmatism is difficult to
technique. Its advantage is a good tightness and self-
prevent. Comparative studies were performed on
sealing, especially in the case of small wounds. Tese
postoperative astigmatism through clear corneal incision
features ensure a better control over postoperative
and posterior limbic incision [18], noticing that for the
astigmatism.
same size incision, 2.2 mm, the posterior limbic location
Dimension of the incision. Lately, reducing the size of
induces astigmatism significantly lower and less variable
the incision has been a major concern for many cataract
(0.25±0.14) compared with the clear corneal incision
surgeons.
However,
larger
scale
use
of
(0.69±0.49). A more corneal incision determines a more
phacoemulsification and foldable intraocular lens
important with-the-rule astigmatism and a scleral
development allowed smaller and smaller incisions in
incision determines a smaller against-the-rule
cataract surgery. Nowadays, the standard technique for
astigmatism [19]. Although studies have shown that
cataract surgery, in the industrialized countries, is made
limbic incisions and scleral incisions induce less
through an incision of about 3 mm.
astigmatism than the ones in clear cornea, in the case of
Reducing incision size induces a smaller astigmatism
small incisions the effect of the locations is less important
after cataract surgery. On this respect, it was proved that
[17]. Due this fact, nowadays, the most common
a smaller incision can manipulate the cornea softer and
incisions made in cataract surgery through
with minimal stress concerning the adjacent tissue,
phacoemulsification are the ones in clear cornea, thus
providing better optic results [21,22]. Decreasing the
replacing the scleral tunnel and the limbic incision.
incision’s dimension from over 3 mm to less than 2 mm
Type of incision. In terms of plans in which the
determined the reducing of the induced astigmatism
incision is made, this can be of three types [16]: in a
and the corneal aberrations [21,22].
singular plan, in two plans and in three plans.
Referring to the locations of the incisions in relation
Te single plan incision can be a perpendicular
to limbus, the studies show that there are not significant
incision on limbus and is generally made on the anterior
differences in the magnitude of the postoperative
limbus. Tis type of incision is healing slowly and
astigmatism, if they are made in clear cornea or sclera,
requires suturing. Another procedure of it, is the ab-
when it comes to small incisions. Tus, an Italian study
externo oblique limbal incision - was used a lot over the
has compared clear corneal incisions of the same length
past decades for extracapsular cataract extraction. It is
made in the temporal area and the tunnel incisions
generally made in the middle region of the limbus, the
made in the superior area at 12 o’clock. Te degree of
plane of the incision is at 110° from the plane of the
astigmatism was similar, but there were different
cornea. Te disadvantage of these two types of incisions
meridians [23].
is the need for suturing, with the emergence of high
As mentioned before, nowadays, small unsutured
postoperative astigmatism [20].
corneal incision is preferred by most cataract surgeons.
Te two planes incision can be an angled limbic
It is known that the anterior surface of the cornea is the
incision - it can be made at any level of the limbus,
main refractive, element of the eye, contributing to
either corneal or scleral. Te incision is made in two
more than 2/3 of its refractive power [24]. So, it is
planes, one perpendicular and another one at 110° from
important to eliminate the corneal incision’s effect over
the surface of the cornea. Usually, the incision
its optic properties. Lately, the tendency to corneal
perpendicular to the average depth is the first one,
micro-incisions (about 2 mm), which provide a well
followed by the oblique one, which opens the anterior
anatomical restoration and refractive stability of the
chamber. It requires sutures, with the possibility of
cornea, characterized the evolution of cataract surgery.
postoperative astigmatism. Another way for this
Comparatively with standard incisions,
the
procedure is the inverse corneal incision - it is made in
microincision’s advantages are a smaller postoperative
the transparent cornea, 1-2 mm in front of the limbus,
astigmatism and less corneal irregularities, with better
Etiology of Postoperative Astigmatism after Cataract Surgery
55
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
implications over the postoperative functional result
fulfilled by choosing a foldable artificial lens, which can
and earlier rehabilitation. In this respect it has been
be implanted through a corneal micro-incision, with a
shown that the mini-incision of 2.2 mm and micro-
minimum postoperative astigmatism.
incision
1.8 mm used in cataract surgery by
Factors that may induce postoperative astigmatism
phacoemulsification are neutral in terms of astigmatism
and are related to the artificial intraocular lenses are: the
[21]. It seems that the 2 mm clear corneal incision is
position of the posterior chamber artificial intraocular
optimal for the induction of insignificant optical
lens, the materials from which are made the artificial
changes in the human cornea, after surgery [25].
intraocular lenses, the size of the optic segment, the
Location of the incision by meridian. Postoperative
form and size of the haptics and also the design of the
astigmatism in cataract surgery may also vary depending
artificial intraocular lens.
on the meridian on which the incision is placed. Te
Te position of the intraocular lens in the posterior
literature data show that small superior incisions, affect
chamber. Intraocular lens implantation in the capsular
more the corneal curvature than similar incisions, placed
bag is the optimal method in most cases of cataract
in the temporal area [26]. Several explanations have
surgery [32]. Te position of the intraocular lens in the
been given for this purpose. It is known that the human
capsular bag can affect postoperative astigmatism in
cornea is about 1 mm wider than higher [27]. Tus, an
cataract surgery. Te refractive changes induced by the
upper incision can be easily closer to the corneal apex
rotation of the intraocular lens and its longitudinal
than a temporal incision, with more pronounced effects
displacement, are well known
[4]. Posterior
on the curvature of the corneal center. Te temporal
misalignment is the most common one and has multiple
incision is further from the visual axis and any flattening
causes: haptic alteration, zonular dialysis, posterior
due to any wound is less likely to affect corneal curvature
capsule rupture, asymmetric capsulorhexis, asymmetric
and visual axis [28]. On the other hand, in a superior
haptic placing, one in the sulcus and one in the capsular
incision, the gravity factor and the blinking tend to
bag. Late spontaneous dislocation in the bag is associated
create traction on it. Tese forces are neutralized better
with zonular insufficiency, like that of the exfoliated
in temporal locations, because the incisions are parallel
syndrome [34].
with the vectors of the forces.
Examinations performed on cadaver eyes with
Different effects of the incisions, in terms of induced
posterior chamber intraocular lenses showed that
astigmatism, depending on their location, have been
asymmetric setting
(bag-sulcus) is a cause of
reported by many other authors. Kohnen et al. [29]
descentration [35,36]. Te descentration degree was 0.8
reported a statistically significant difference in induced
mm for the case of bag-suculus fixation and only 0.4
astigmatism after unsutured tunnel limbic incision,
mm for bag-bag fixation [37].
temporal and nasal. Guirao et al. [30] showed that
Materials used for artificial intraocular lenses. Before
temporal incision induces fewer aberrations than the
the artificial intraocular lenses era, the most common
nasal one.
used were the ones made of polymethylmethacrylate
From the structural point of view it is known the
(PMMA). In this respect, it is known that PMMA
fact that the incision in the cataract surgery can induce a
implants may be associated with an inflammatory
flattening effect when it is performed near or on the
reaction greater than the ones with hydrophilic acrylic
steepest meridian of the cornea [19]. Tus, placing the
and with a higher rate of posterior capsule opacification
incision on the steepest corneal meridian in the cataract
[38]. It is unclear whether this effect is directly related to
surgery through phacoemulsification, corrects lower
the implant material or to the greater size of the wound
values of the pre-existing astigmatism and it is sufficient
required for rigid implants. Currently, artificial
for most eyes operated of cataract
[8]. A temporal
crystalline lens implants are made of either silicone or
incision of 2.8 mm is recommended for patients with
acrylic polymers. On the other hand, these materials can
negligible preexistent astigmatism, while the upper and
be generally classified after their hydrophilic or
nasal incision should be used also for the correction of
hydrophobic nature. Hydrophilic materials are
low-grade astigmatism when steepest axes are located at
considered generally to have a better uveal
180° and 90° [31].
biocompatibility compared with hydrophobic materials,
Factors which depend on intraocular lenses
but the latter, with their current design may have greater
Te surgeon’s decision to choose a particular type of
performances in the prevention of posterior capsule
artificial lens implant to a specific patient is difficult
opacification
[39,40]. Such a complication requires
nowadays because of the existence on the market of a
YAG capsulotomy, which later can cause a misalignment
wide range of such implants. Tis requirement can be
of the artificial lens [41].
56
Pop et al
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
GENERAL REVIEW
Optical part size. It may be responsible for the
5.
Eydelman MB, Drum B, Holladay J et al. Standardized
occurrence of postoperative astigmatism and it is due to
analyses of correction of astigmatism by laser systems that
more frequent use of small diameter artificial lens,
reshape the cornea. J Refract Surg 2006;22:81-95.
which are more difficult to center. Artificial intraocular
6.
Gills JP. Treating astigmatism at time of cataract surgery.
lenses with larger optical parts
(6 mm), are better,
Curr Opin Ophthalmol 2002;13(1):2-6.
because they are less dependent on centering and have a
7.
Carvahlo MJ, Suzuki SH, Freitas LL, Branco BC,
lower rate of posterior capsule opacification [42]. On
Schor P, Lima AL. Limbal relaxing incisions to correct
the other hand, a larger diameter may require a larger
corneal astigmatism during phacoemulsification. J
incision, thus increasing the risk of postoperative
Refract Surgery 2007;23(5):499-504.
astigmatism.
8.
Amesbury EC, Miller KM. Correction of astigamtism
Shape and size of haptics. Tey have an important
at the time of cataract surgery. Curr Opin Ophthalmol
role in the misalignment of the intraocular lens with the
2009;20:19-24.
possibility of apparition of the postoperative
9.
Basti S, Vasavada A, Tomas R, Padhmanabhan P.
astigmatism. Haptics with the J form come into contact
Extracapsular cataract extraction: surgical tehniques.
with the posterior capsule on a portion with 25% lower
India 1993;41(4):195-210.
than the ones with the C loop [43]. On the other hand,
10.
Luntz MH, Livingston DG. Astigmatism in cataract
a total diameter of 12.0 to 12.5 mm is sufficient for a
surgery. BJO 1977;61:360-5.
better centering of the intraocular lens. A larger diameter
11.
Melles GRJ, Binder PS, Beekhuis WH, Wijdh RHJ,
can stretch the capsule in the direction of the lens,
Moore MNM, Anderson JA, Raj NS. Scar tissue
becoming oval, and the misalignment of the intraocular
orientation in unsutured and sutured corneal wound
lens thus being possible.
healing. BJO 1995;79:760-5.
Te design of the artificial intraocular lens. Te
12.
Van Rij G, Waring GO. Changes in corneal curvature
intraocular lens dislocation has been reported in both of
induced by sutures and incisions. Am J Ophthalmol
the designs, single piece or multi piece
[44]. Tis
1984;98:773-83
complication is more common when the artificial
13.
Jaffe NS, Clayman HM. Te phatophisiology of corneal
implant is not placed symmetrically in the capsular bag.
astigmatism after cataract extraction. Ophthalmology
(Rochester) 1975;79: 615-30.
Conclusions
14.
Wishart MS, Wishart PK, Gregor ZJ. Corneal
astigmatism following cataract extraction. Br J
Postoperative astigmatism of greater value may
Ophthalmol 1986;70:825-30.
compromise functional outcome after cataract surgery.
15.
Maul E, Muga R. Anterior segment surgery early after corneal
Te causes of this type of astigmatism are multiple, but
wound repair. British J of Ophthalmol 1997;61:782-4.
the characteristics of the surgical incision are the most
16.
Buratto L, Maurizio I. Incisions and sutures in cataract
important. Small incision in clear cornea reduces the
suregry. Ed. Fogliaza 1986;32-5,39-40.
risk of corneal damage, providing an early anatomical
17.
Giasanti F, Rapizzi E, Virgili G et al. Clear corneal
and functional rehabilitation after cataract surgery.
incision of 2.75mm for cataract surgery induces little
change of astigmatism in eyes with low preoperative
corneal cylinder. Eur J Ophthalmol 2006;16:385-93.
Bibliography
18.
Ernest P, Hill W, Potvin R. Minimizing surgically
induced astigmatism at time of cataract suregry using a
1. Donders FC. On the anomalities of accomodation and
square posterior limbal incision. Journal of
refraction of the eye. London. New Sydenham Society,
Ophthalmology 2011:2(10):1155/2011/243170.
1864:334-9
19.
Buratto L. Extracapsular cataract microsurgery and
2. Nicula C, Nicula D. Astigmatismul indus operator.
posterior chamber intraocular lenses. Ed. Fogliara,
SRO. Oftalmologia, 2000;43-7.
Milano, 1989:236-43.
3. Cho YK, Kim MS. Preoperative modulating factors on
20.
Biro Z. Bazele facoemulsificarii. Ed.Tudomani, Pecs,
Astigmatism in Sutured Cataract Surgery. Korean J of
2002;Cap 3:39-42.
Ophthalmol 2009;23(4):240-8.
21.
Elkady B, Alio J, Ortiz D, Montalban R. Corneal
4. Kim IT, Park HYL, Kim SH. Postoperative astigmic
aberrations after microincision cataract surgery. J
outcomes based on the haptic axis of intraocular lenses
Catarct Refract Surg 2008;34(1):40-5.
inserted in cataract surgery. Korean J Ophthalmol
22.
Yao K, Tang X, Ye P. Corneal astigamtism, high order
2011;25(1):22-8.
aberrations and optical quality after cataract surgery:
Etiology of Postoperative Astigmatism after Cataract Surgery
57
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
microincision versus small-incision. J Refrac Surg
34.
Masket S, Osher RH. Late complications with
2006;22:1079-82.
intraocular lens dislocation after capsulorexis in
23.
Cillino S et al. Temporal versus superior approach
pseudoexfoliation syndrome. J Cataract Refract Surg
phacoemulsification:
short-term
postoperative
2002;28:1481-4.
astigmatism. J cataract Surg 1997;23:267-71.
35.
Apple DJ et al. Posterior chamber intraocular lenses in a
24.
Bennett AG. Analysis of three meridional keratometric
series of 75 autopsy eyes. Part I. Loop location. J Cataract
measurements of the anterior cornea. Ophthalmic
Refract Surg 1986;12:358-62.
Physiol Opt 1990;10:93-4.
36.
bHansen SO et al. Descentration of flexibile loop
25.
Alio JL, Elkady B, Ortiz D. Corneal quality following
posterior chamber intraocular lenses in a series of 222
sub 1,8 mm micro-incision cataract suregry vs. 2,2 mm
postmortem eyes. Ophthalmology 1988;95:344-9.
mini-incision coaxial phacoemulsification. Middle East
37.
Wassernann D et al. Anterior capsular tears and loop
Afr J ophthalmol 2010;17(1):94-9.
fixation of posterior chamber intraocular lenses.
26.
Merriam JC, Zheng LZ, Urbanowicz J, Zaider M.
Ophthalmology 1991;98:425-31.
Change on the horizontal and vertical meridians of the
38.
Rowe NA, Biswas S, Lloyd IC. Primary IOL
cornea after cataract surgery. Trans Am Ophthalmol
implantation in children: a risk analysis of foldable
Soc 2001(99):187-97.
acrylic versus PMMA lenses. Br J Ophthalmol
27.
Duke-Elder S, Wybar KC. Te ocular tissues. In:
2004;88(4):481-5.
Duke-Elder S. Ed. System of Ophthalmology. Vol II.
39.
Hayashi K, Hayashi H. Posterior capsule opacification
Te anatomy of tha visual system. St Louis, Mo:CV
after implantation of a hydrogel intraocular lens. Br J
Mosby, 1961:92.
Ophthalmol 2004;88(2):182-5.
28.
Gokhale NS, Sawhney S. Reduction in astigmatism in
40.
Hollick EJ, Spalton DJ, Ursell PG, Meacock WR,
manual small incision cataract surgery through change of
Barman SA, Boyce JF. Posterior capsular opacification
incision site. Indian J of Ophthalmol 2005;53(3):201-3.
with hydrogel, polymethylmethacrylate and silicone
29.
Kohnen S, Neuber R, Kohnen T. Effect of temporal
intraocular lenses: two-years results of a randomized
and nasal unsutured limbal tunnel incisions on induced
prospective trial. Am J Ophthalmol 2000;129(5):577-
astigmatism after phacoemulsification. J Catract Rafract
84.
Surg 2002;28(5):821-5.
41.
Steinert RF, Puliafito CA, Kunar SR, et al. Cystoid
30.
Guirao A, Tejedor J, Artal P. Corneal aberrations before
macula edema, retinal detachment and glaucoma after
and after small-incision cataract surgery. Invest
Nd YAG laser posterior capsulotomy. Am. J.
Ophthalmol Vis Sci 2004;45(12):4312-19.
Ophthalmology 1991;112:373-80.
31.
Tejedor J, Perez-Rodriguez A. Astigmatic change
42.
Meacock WR, Spalton DJ, Boyce JF, Jose JR. Effect of
induced by 2.8 mm corneal incisions for cataract surgery.
optic size on posterior capsular opacification with 5.5
Invest Ophthalmol Vis Sci March 2009; 50(3):989-
mm and 6.0 mm optic diameter Acrysof intraocular
94.
lenses. J Cataract Refarct Surg 2001;27:1194-8.
32.
Dick HB, Augustin AJ. Lens implant selection with
43.
Assia EI, Apple DJ. Side-view analysis of the lens. Arc
absence of capsular support. Curr Opin Ophthalmol
Ophthalmol 1992;110:94-7.
2001;12:47-57.
44.
Mamalis N, Brubaker J, Davis D, et al. Complication
33.
Cataract in the adult eye-Complications of intraocular
of foldable intraocular lenses requiring explantation or
lenses. American Academy of Ophyhalmology
secondary intervention. J Catarct Refract Surg
2011;17:29-31.
2008;34:1584-9.
58
Pop et al
GENERAL REVIEW
NEWS IN STUDY OF OPTIC NERVE VASCULARIZATION
Măgureanu Marineta¹, Stănilă Adriana², Stănilă Dan Mircea²
¹Ghencea Medical Center, Bucharest, ²Research Center of Ocular Surface, Lucian Blaga University, Ophthalmology
Clinic - RCOS, Sibiu
Address for correspondence:
Marineta Magureanu, MD
Crinului St, No.43, Sector1, Bucharest
Tel: 0723658133
Email: dr_magureanu@yahoo.com
Received: 30.01.2013
Accepted: 20.02.2013
Med Con March 2013, Vol 8, No 1, 59-65
Abstract
flow, requiring its study to elucidate the hemodynamic
changes in different diseases.
Since many eye diseases are based vascular factor, it
Research carried out in order to understand ocular
is very important to understand both the vascularization
blood flow have increased in recent decades, all over the
of this area as well as their pathogenesis and management.
world. Te
current techniques for noninvasive
Regarding the optic nerve (ON), its vasculature plays a
examination of ocular blood flow have contributed
decisive role in etiopathogenesis of different forms of
significantly to understanding the role of ocular
optic neuropathy (including glaucoma) as well as other
hemodynamic in the etiology of various eye diseases [1].
eye diseases. ON vascularization is complex, particular
In the last years, it was concluded that in
and varies depending its segment.
glaucomatous optic neuropathy, besides intraocular
In the last years new techniques have been
pressure, there are other factors that influence the disease
developed, or some older were perfected, for examination
evolution, including vascular factor would seem to play
of oculo-orbital vessels and blood flow of this level. Te
an important role. A proof of this is the 6th meeting of
current techniques for noninvasive examination of
the World Glaucoma Association
(WGA) of 2009,
ocular blood flow have contributed significantly to
which had as theme “Ocular blood flow in Glaucoma”
understanding the role of ocular hemodynamic in the
[1].
etiology of various eye diseases.
Keywords: arterial circulation, venous circulation,
Optic Nerve Vascularization
blood flow, optic nerve
ON vascularization is complex, particular and varies
Introduction
depending its segment: the optic nerve head, consists of
the following
4 regions from anterior to posterior
Te eye is the organ where the blood vessels can be
aspects: the surface nerve fiber layer, prelaminar region,
examined directly, through noninvasive techniques. Te
lamina cribrosa region and retrolaminar region,
ocular blood flow is influenced by various factors and
intraorbital segment (25-30 mm), canalicular segment
their interaction: metabolic products, perfusion
(9-10 mm), intracranial segment (16 mm) [2,3,4,5],
pressure, blood gases. Effects and interactions of these
being very rich before entry of central retinal artery in
factors influence complex and varied the ocular blood
the glob and much poorer thereafter [6].
News in Study of Optic Nerve Vascularization
59
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
I. Arterial Circulation
peripaplillary choroidal vessels (10% of vascularization
Arterial circulation of ON is achieved through the
of this area) [1,4,10]. Te capillaries of this region are
ophthalmic artery (OA), branch of the internal carotid
complex and are continues with the capillary bed from
artery, with origin at the level of anterior wall of C3
the surface of nerve fibers layers and the level of laminar
regions and with horizontal and anterior direction,
region.
which enters in the orbit through the ophthalmic hole
Circle of Zinn-Haller
along with ON, located lateral and inferior towards it
It was described by Haller in 1754 and Zinn in
[7]. Subsequently, passes over the ON, having in the
1755 as an incomplete anastomotic arterial circle located
front third a parallel trajectory with the medial side of
at the sclera level, and consists from anastomoses of
the orbit and passes medial and superior towards ON
short PCAs around of ON head [1,3,4,10]. At the eyes
[8].OA is divided into ocular and orbital branches [7].
with Zinn-Haller circle well developed, arterial branches
OA ocular branches are [3]: short posterior ciliary artery,
from this supply both the prelaminar, laminar regions
long posterior ciliary artery , central retinal artery (ACR)
[1] as well as retrolaminar region by recurrent branches
which penetrates ON approximately
10-15 mm
[10]. Olver et al., described the circle of Zinn-Haller as
posterior to the globe, and after entering the eye is
a microscopic, intrascleral, elliptical, microvascular
divided into 2 arcade: upper and lower [9].
anastomosis formed by branches of the medial and
Typically, between 2 and 4 posterior ciliary arteries
lateral paraoptic short PCAs [10].
(PCA) has an anterior trajectory and will be divided
3. Te laminar region
into approximately 10-20 short PCA before entering in
Entire vascularisation is provided by branches of
the eye [1]. Often, PCA form the two arterial groups:
short PCAs and Zinn-Haller circle [3,4,10]. Occasionally,
lateral and medial, before branching in short PCA [1].
from peripapillary choroid can leave small arterioles [4].
Short PCA penetrate the perineural sclera for vascularize
At this level, the capillaries are organized as a dense
peripapillary choroid and anterior portion of ON. Some
capillary plexus, forming a highly vascularized structure
of them can cross the sclera until the choroid level
at the ON head [10]. Te capillaries of this region are
without branch
[1]. After Hayreh, PCA along
continues with the capillaries of retrolaminar region.
intraorbital path are divided into numerous branches at
4. Te retrolaminar region
different distances before entering the eyeball: long
Vascularization of this region is double: peripheral,
PCAs in generally in number of 2- one medial and one
centripetal vasculature provided by pial vessels with
lateral- without role in vascularization of ON and short
origins at the Zinn-Haller circle, short PCAs and from
PCAs in number of about 20, which is subdivided into
the choroidal peripapillary region [1,4,10]; may also
2 subgroups - paraoptics arteries (for the ON) and distal
participate pial branches from CRA and other orbital
arteries (for the choroid) [10].
arteries; axial, centrifugal vasculature, present in 75% of
1. Te Surface Nerve Fiber Layer
cases, consisting of branches (from 1 to 8) of CRA.
It is the first area irrigated by centripetal model by
Axial vasculature, when is present, is not as developed as
branches of CRA, which forms at the peripapillary
the peripheral
[4.10]. May also participate capillary
retina [4]. Tese arterioles go to the optical disc and are
from laminar region [4].
called “epipapillary vessels”. Capillary branches of these
In conclusion PCA, directly or via choroidal
vessels are continuous with the retinal capillaries at the
peripapillary branches or short PCAs (or Zinn-Haller
edge of the optic disc, but they have posterior
circle when is present), is the only vascular source for
anastomoses with the prelaminar capillaries of ON
the prelaminar and laminar regions and the main source
[1,3,4,5]. Direct choroidal contribution is not
(if not only) for retrolaminar region [10].
demonstrated at this level
[4,5]. When cilio-retinal
PCA Watershed Zones
artery is present (one or more), precapillary branches
When a tissue is supplied by two or more end-
can contribute to irrigation of temporal sector
arteries, the border between the territories of distribution
[1,3,4,5,10]. Te number of these arteries is correlated
of any two end-arteries is called a “watershed zone”.
with optic disc size [3].
Tese are areas with poor vascularisation, which makes
2. Te prelaminar region
them vulnerable to ischemia. Te important role of
Irrigation is insured mainly by short PCAs through
these zones becomes obvious in cases where the
direct branches or Zinn-Haller circle (when is present).
perfusion pressure from one or more end-arteries
Branches of arterioles and capillaries form a diffuse
belonging to the same area decreases. Te location of
network around and inside nerve fascicles [5]. Tere are
the watershed zones at this level varies according to the
studies that support the existence of branches from
number of the PCAs and their locations [10].
60
Măgureanu et al
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
GENERAL REVIEW
5. Intraorbital part of the ON
Intraorbital region drains mainly into the CRV. Pial
Is subdivided, according to the place of penetration
veins located at the pia mater mostly open at the CRV.
of CRA in ON, in 2 sub-segments: anterior and
CRV is formed at the optic disc level through the union
posterior [10].
a number of different retinal veins, and go posterior
Anterior subsegment disposes of 2 vascular systems:
through the axis of ON, temporal by the CRA. CRV
the peripheral system
(centripetal) and axial system
goes through part of ON before heading out it, in orbit.
(centrifugal). Te peripheral system is always present,
Terefore, venous blood is drained most of the cavernous
arterial vascularization of peripheral fiber of ON being
sinus and to a lesser extent to the orbito-facial and
ensured through the arteries coming from the vascular
orbito-pterygoid network [6].
system of the pia mater, most of them being branches of
Angioarchitecture of the optic nerve
the OA [4], peripapillary choroid, Zinn-Haller circle,
Since
1903 has been described by various
CRA and other orbital arteries [10]. Branches from OA
investigators. Vascularization of ON is identical to the
penetrate the dura at
10-12 mm from the glob to
brain. All arteries of ON provides its vasculature through
participate in the formation pial system [4]. Recurrent
the pial vascular plexus which acts like a “distributing
branches of PCAs and juxta-papillary choroidal are added
centre for the vessels”. Te vessels entering the nerve
to pial vascularization [4]. Te axial (centrifugal) system
from the pia take a covering of the pia and glia with
is present in 75% of ON; central parts of ON are supply
them, which forms the septal system of the nerve. Te
by intraneural arterioles with the pial origin
[6] and
angioarchitecture in the region of the lamina cribrosa
intraneural branches (in number of 1-8) of CRA [6,10].
has been described as comprising numerous, small, very
Posterior subsegment presents a peripheral
close and transversely elongated meshes, a very dense
centripetal vascular system represented by pial vascular
capillary plexus 10-20 mm in diameter which makes
plexus, consisting of multiple small collateral arteries,
this part of the ON head a highly vascular structure.
with origin often at the OA level and rarely in other
Intraorbital segment presents anastomosys between OA
orbital arteries. In 10% of cases there may be an axial
branches to the surface of ON and anastomosys between
centrifugal vascular system consists of intraneural
intraneural branches inside of ON. Longitudinal vessels
branches of the CRA [10].
are connected irregular with transverse vessels that go in
6. Canalicular part of the ON
different directions forming in longitudinal section
Tere are different opinions regarding blood supply
“mesh nets” with irregular forms. Intracanalicular
of this area. After Hayreh, vascularization of this
segment has a similar angioarchitecture with intraorbital
segment is provided by AO by collateral branches,
segment, becoming increasingly complicated as cranial
usually between 1 and 3. Tese branches reach to the
segment approach, losing the difference between
ON traversing the conjunctiva sheath which covers the
longitudinal and transverse vessels. Intracranial segment
nerve at this level. Tere are no axial vascular system at
has a double angioarchitecture: in the distal part,
this level [10].
compared with previous segment, longitudinal vessels
7. Intracranial part of the ON
become prominent, and the transverse vessels become
Tere are many controversies regarding
rare; in the proximal portion, especially lateral side,
vascularization of this segment. In summary, it is
vessels are less dense. At the ON level, capillaries
provided by branches from: internal carotid artery,
extending throughout its length, with anastomosys
anterior cerebral artery, anterior communicating artery,
between them, and above anastomosys with retinal
OA. Pial arterioles become capillary and cross the pial
capillaries [10].
septum until ON axis [4,10].
Vascular wall structure
II. Venous circulation
Vascular wall is made up of 3 concentric layers,
Venous circulation of the ON head is provided
histologically different, from inside to outside: tunica
especially by central retinal vein (CRV) [10], parallel to
intima, media and adventitia.
with homonymous artery inside of ON [1,3]. Small
Tunica intima is made up of endothelial layer,
venules draining from superficial nerve fibers layer to
subendothelial layer and internal elastic lamina.
choroid (optico-ciliary veins) [4].
Endothelial layer has a single row of cells
(simple
Vessels of prelaminar region draining to peripapillary
squamous epithelium), ovoid shape, with the long axis
choroidal veins (VCR, at this level, communicates with
parallel to the long axis of the vessel, placed on the basal
choroidal circulation). Tere is no venous equivalent for
lamina. Teir numbers differ depending on the size of
Zinn-Haller circle. Veins of nerve trunk go one part in
vessel: at vessels with the small caliber one endothelial
CRV and other part in a central posterior vein [6].
cell is sufficient to cover the circumference of the lumen;
News in Study of Optic Nerve Vascularization
61
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
at the greater vessels their number is directly proportional
Pulsatility measurement devices
to their size. In the endothelial cells from arteries level
Ophthalmodynamometry
(ODM): is an indirect
exist Palade corpuscles (ribosomes) who containing von
measurement of the systolic and diastolic blood pressure
Willebrand factor [11], with a role in clot formation.
in the CRA; a contact lens equipped with a pressure
Subendothelial layer is made up of lax conjunctive tissue
sensor measuring increased intraocular pressure (IOP);
and smooth muscle cells disposed longitudinally. Internal
CRA diastolic pressure is considered to be equal to IOP
elastic lamina is made up of elastin, with fenestrated
onset; maximum value of IOP corresponds ACR systolic
aspect (“mesh”), allowing diffusion of the substances. Is
pressure [1].
more developed in the arteries of muscular type.
Ophthalmodynamography
(ODG): measured
Tunica media consists of smooth muscle cells and
pressure in OA; the eye is cover with an elastic membrane
external elastic lamina. Smooth muscle cells are arranged
who exerts pressure on the whole orbit; similar to blood
in the concentric layers, disposed helicoidal, among
pressure measurement with sphygmomanometry,
which finding elastic fibers
(better developed in the
pulsation is transmitted from the orbit through the
arteries of elastic type), type III collagen fibers and
membrane in the device, and recorded on a diagram [1].
proteoglycans. Postcapillary vessels have not medium
Oculo-oscillo-dynamography (OODG): improves the
tunic, which was replaced by pericytes.
previous techniques, determining directly pulsation
Tunica adventitia is made up of fibroblasts, type I
within either retinal or choroidal vascular bed.
collagen fibers and elastic fibers oriented longitudinally.
Pulsatile Ocular Blood Flowmetry (POBF): measures
Depending on the proportion of various elements
IOP in real time, without perturbing it, through a
of the wall structure, arteries are divided into: elastic
modified pneumotonometer connected to the computer.
and muscle [7].
Ocular blood flow varies during the cardiac cycle,
At the microcirculation level, the balance between
influencing IOP value, with a peak during the systole
blood flow and intraluminal pressure is provided by
and a decrease in the diastole. Quantifying IOP
arteriolar tone, precapilare sphincter, pericytes and
pulsation associated cardiac cycle, allows the calculation
capillary tone and smooth muscle fibers from veins.
of pulsatile component of ocular blood flow
(done
Capillary pericytes can substitute role of precapilare
approximately 200 measurements/sec) [1,3,10].
sphincters where they are missing.
Interferometry: highlighted directly the pulsation of
As regards of nature of endothelium, capillaries and
the retinal level, using a laser beam who is divided into
can be fenestrated and nonfenestrated. Fenestrated
two fascicles (one to retina and one for cornea) [1,3].
capillaries
(present in most organs) allow passage of
Laser devices
large molecules, particularly proteins. Nonfenestrated
LDF (Laser Doppler Flowmetry): method was first
capillaries, present at the retinal and ON head level, do
described in 1992 by Riva et al., evaluates blood flow to
not allow diffusion of substances from plasma into
the ON head: the laser beam measuring blood flow at a
surrounding tissue [3,5] and have junctions type tight
depth greater than 520 μm, corresponding to the CPA
between endothelial cells, achieving the blood-ocular
[1,3,10].
barrier [5]. Capillaries of the retina and ON are devoid
SLDF (Scanning Laser Doppler Flowmetry): is the
of precapillary sphincters but have many pericytes.
only device that measures vascular flow in absolute
Tese pericytes act as vascular smooth muscle genuine,
units. By combining the advantages of fundus camera
reacting to the presence of CO2, O2 levels and
and the Doppler effect, may reveal velocity, diameters
adenosine concentration. Tese capillaries are equipped
and vascular tracts [1,10].
to intervene in the control of blood flow to the ON
LSF
(Laser Speckler Flowgraphy): noninvasive
head through the mechanism of
“metabolic
technique first used by Japanese researchers which
autoregulation”. In contrast, choroidal capillary bed
examines the blood flow to the ON head, the laser beam
(coriocapillary) consists of fenestrated capillaries and
reaching depths of 0.5-1 mm. Based on the phenomenon
rare pericytes [3].
of “interference” seen when a light source such as laser
Examination of vascularization and blood flow
scans a reflective surface [1,3,10].
to the ON
Scanning Laser ophthalmoscope
(SLO): technique
In the last years new techniques have been
based on LDF; the devices using a confocal optical
developed, or some older were perfected, for examination
system, which leads to obtaining a high quality image of
of oculo-orbital vessels and blood flow of this level.
the fundus [1,10].
Some remained in the experimental stage, others have
HRF (Heidelberg Retinal Flowmeter): technique
found clinical application.
based on LDF, which has adapted a confocal laser
62
Măgureanu et al
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
GENERAL REVIEW
scanning system which allows a greater depth
contrast agent bound to plasma proteins (indocyanine),
examination. Can provide images of peripapillary retina
injected IV, at the eye vessels level , mainly the choroidal
and neuro-retinal ring [1,3,10].
[3,5,10].
HRT (Retinian Tomography Heidelberg): Evaluates
Magnetic resonance angiography = angio-RM (MRA):
blood flow to the neuro-retinal ring [1].
complete, noninvasive method for examining intra- and
Doppler OCT(Optical Coherence Tomography): New
extracranial circulation; the most used technique is the
generations of OCT: time-domain
(TD-OCT) and
“time of flight”
(TOF), with two possibilities data
spectral-domain (SD-OCT) increased performance of
acquisition for imaging: two-dimensional
(2D-TOF)
the classic OCT. SD-OCT provides three-dimensional
and three-dimensional
(3D-TOF)
[7]. Another
images of the intraretinal microstructure through a
technique used is “phase contrast pulse sequences” [15].
faster scanning and with a higher resolution (18,000
Computed tomography angiography= angio-CT
measurements/sec, with an axial resolution of 5 mm)
(CTA): performed
1mm sections, viewed by MIP
than TD-OCT (400 measurements/sec with an axial
technique (maximum intensity projection) [7.15].
resolution of ~10 mm). Experimental is used High-
“Dynamic ultra-widefield” angiography Optos
speed ultrahigh-resolution OCT (UHR OCT): 25,000
P200MA: offers a very broadly field and high quality
measurements/sec, with an axial resolution of 3.5 mm.
examination [5].
Te new technologies can measure speed and volume of
Oximetry
blood flow to the branches of the retinal vessels and the
Retinal oximetry: noninvasive method that measures
size of these vessels. Te development of these techniques
the oxygen saturation of hemoglobin in retinal structures
attempts to obtain Doppler structural information and
using digital images [1,3].
oximetry during the same scan [1,3,5].
Magnetic Resonance Oximetry: is based on the
Doppler ultrasound: useful in the diagnosis of
paramagnetic properties of oxygen and its ability to
multiple primary or secondary vascular diseases of the
influence the relaxation rate (1/T¹). Posterior vitreous
eye and orbit [12].
oxygenation is used to determine the retinal oxygenation.
Color Doppler imaging (CDI): can examine the OA,
Direct examination
CRA and CRV, short PCAs, superior ophthalmic vein,
Examination of the ON head within fundus
measuring the velocity of vascular flow and resistance
analyzing
by:
direct
ophthalmoscopy,
indirect
vascular index at their level. Te principal parameters
ophthalmoscopy, fundus biomicroscopy with different
measured are: peak systolic velocity (PSV), end diastolic
lenses, fundus camera (is obtained stereoscopic images).
velocity
(EDV), pulsatility index
(PI) and resistivity
Disorders in which it is involving vascularization
index (RI) [1,3,10,12,13].
of ON
Transcranial Doppler ultrasound: non-invasive
Vascular disorders of the ON head
method, used since 1982 by Rune Aaslid, currently has
Central
retinal
vein
occlusion
(RVO):
multiple uses, including examination AO [7.10].
histopathological thrombosis occurs at the lamina
Angiography
cribrosa of the CRV [5,12,13], or at the branch of it.
AFG (Angiofluorography): used in ophthalmology for
Central retinal artery occlusion (RAO): after occlusion
50 years, shows the in vivo vascularization of ON head,
location can be divided into: CRA occlusion, occlusion
retina and choroid (less) [10.14]. Te contrast substance,
of the branch of CRA, cilio-retinal artery occlusion,
fluorescein, is a nontoxic chemical compound, with
occlusion combined CRA and CRV [5,12,13].
bright fluorescing properties, which is injected IV. Blue
Chronic glaucoma
(hypertensive, especially the
excitation light
(λ=465-490 nm), acting on the
normotensive): in the last years have made many
fluorescein, unbound of plasma proteins, resulting in a
prospective studies that have demonstrated retinal,
yellow-blue light (λ=520-530nm). Can be performed an
choroidal and retrobulbar circulation problems. Also,
analysis: sequential - is examined the angiogram frame
glaucomatous optic neuropathy was associated with
by frame highlighting its phases: prearterial, arterial,
abnormal ocular perfusion pressure, nocturnal
arteriovenous and venous; anatomical- are observed
hypotension, disc hemorrhage, migraine and aging of
layers and zones of posterior pole; morphological [5.14].
blood vessels. Chronic ischemia of ON leads to loss of
Scanning Laser AFG: is obtained high quality images
retinal ganglion cells, independent of IOP value.
with a wide field, in which can be examined vascular
Reduction of ocular perfusion pressure may be
diameters and tracks in dynamics (real time) [1,3,10].
secondary to elevated IOP, or may represent the first
Indocyanine green angiography (ICG): is performed
cause of impaired ON in glaucoma. Also, chronic ocular
using a SLO device that will highlight presence of the
ischemia can induce vascular impairment of self-
News in Study of Optic Nerve Vascularization
63
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
regulation and its incapacity to reduce IOP and
Diabetes Mellitus
maintaining adequate ocular perfusion pressure
Arterial hypertension: depending on the degree of
[3,12,13,16].
impairment of vascular bed, hypertension can cause:
Ocular hypertension
hypertensive retinopathy, optic neuropathy and
Retinal detachment
coroidopathy [5].
Optic neuropathies: may be divided into 2 groups:
vascular neuropathies
(anterior ischemic optic
Conclusions
neuropathy
= AION, Horton’s disease, complicated
drusen) and inflammatory neuropathies (demyelinating
Since many eye diseases are based vascular factor, it
diseases, systemic disorders - sarcoidosis) [13]. Hayreh
is very important to understand both the vascularization
divides optic neuropathy according to the arterial source
of this area as well as their pathogenesis and management.
in: anterior ischemic optic neuropathy (AION) which
Regarding the optic nerve (ON), its vasculature plays a
refers to the anterior portion of the ON supplied by the
decisive role in etiopathogenesis of different forms of
PCA circulation and which is subdivided into arteritic
optic neuropathy (including glaucoma) as well as other
and non-arteritic; posterior ischemic optic neuropathy
eye diseases.
(PION) involving the rest of the optic nerve not
For now do not have perfect technique should
supplied by the PCA circulation and which is subdivided
examine blood flow to the ON level. Ophthalmologists
into arteritic, non-arteritic and surgical
(peri- or
need of techniques readily accessible, safe, reliable, non-
postsurgical) [10].
invasive and repetitive in the current practice for
Effect or orbital space-occupying lesions
examination patients with glaucoma, ischemic optic
Cavernous hemangiomas: mostly occur in young
neuropathy or other vascular disorders of the ON. Also,
adults, in the retrobulbar intraconal space [13].
due to the discovery nocturnal hypotension involvement
Capillary hemangioma: usually diagnosed in infants [13].
in the development and progression of non-arteritic
Orbital varices: affected veins change during
AION and glaucoma, is required a method that can
Valsalva’s maneuver (expands and the flow stops), or
monitor blood flow to the ON head continuously/
when the head is leaned [13.17].
frequently over a period of 24 hours (or more) and
Orbital Cellulitis: bacterial infection
(common:
particularly during sleep.
staphylococcus, streptococcus or Haemophilus) of the
Te lack of these technologies make management of
orbital fatty tissue.
ischemic diseases of the ON and, implicitly, to prevent
Orbital lymphoma [13]
blindness a difficult task [10].
Te ON glioma: leads to reduced flow and increased
impedance indices in CRA through the pressure exerted
on the sheath of ON [12].
References
Orbital tumor invasion [10].
Other disorders
1. Harris A, Jonescu-Cuypers CP, Kagemann L, Ciulla
Carotid artery stenosis: causes a decrease in blood
TA, Krieglstein GK. Atlas of Ocular Blood Flow,
flow to the CRA, OA, or both when the degree of
Vascular Anatomy, Pathophysiology and Metabolism,
stenosis is more than 70% and a change of flow in
Second Edition, Ed. Elsevier, 2010,vii:1-9.
occlusions (because of supply OA from external carotid,
2. Basic and Clinical Science Course, American Academy
through activation of anastomoses between periorbital
of Ophthalmology 2012-2013, Section Glaucoma, Te
arteries, with origin in external carotid artery and OA)
Eye M.D. Association, 40-5.
[7,12,13]. When carotid stenosis is over then 90%,
3. Ocular blood flow in glaucoma, the
6th Consensus
perfusion of the OA level decreases by 50%, resulting in
Report of the World Glaucoma Association, Ed.
ocular ischemic syndrome [5].
Kugler, 2009, 5-11.
Carotid-cavernous
fistulas
(posttraumatic
or
4. Duane’s Ophthalmology CD, 2000 edition
spontaneous): shunts between the arterial and venous
5. Arevalo JF. Retinal Angiography and Optical Coherence
system [17]. It is characterized by: CRV is enlarged with
Tomography, Ed. Springer,
2009;10-25,110-5,118-
reverse flow (or bidirectional) and “arterial blood” and
21,155-7,407-17,431-45.
supraorbital vein with reversed flow [12.13]; increase
6. Cernea P. Tratat de Oftalmologie, Ed. Medicală,
the eye pressure [17].
2002,769-70.
Arteriovenous malformations: vein caliber, velocity
7. Tiu C, Antochi F. Neurosonologie, Ed. Semne,
and flow direction changed [12.13].
2006,46-8,52-3,151-3.
64
Măgureanu et al
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
GENERAL REVIEW
8. Gray HL, Bannister LH, Wiliams PL. Gray’s Anatomy,
15. Mansour MA, Labropoulos N. Vascular Diagnosis,
28ed, Ed. Edinburg, Churchill Livingstone 1995.
Ed. Elsevier Saunders, 2005,85-9,105-12.
9. Basic and Clinical Science Course, American Academy
16. Rankin SJA. Color Doppler Imaging of the Retrobulbar
of Ophthalmology
2012-2013, Section
5, Neuro-
Circulation in Glaucoma, Survey of Ophthalmology
Ophtalmology, Te Eye M.D. Association, 12-19.
1999;Supplement 1,43:S176-S181.
10. Hayreh SS. Ischemic Optic Neuropathies, Ed.
17. Schlote T, Rohrbach J, Grueb M, Mielke J. Schlote
Springer,2011,1-78,111-24,153.
Pocket Atlas of Ophthalmology, Ed. Tieme, 2006;5-
11. Gartner LP, Hiatt JL. Color textbook of histology, Ed.
7,41-8.
WB Saunders,1996,213-7.
18. Sinelnikov RD. Atlas of Human Anatomy, Vol II,
12. Dudea SM, Seceleanu A. Aplicaţii ale Ultrasonografiei
Editia a IV-a, 1986,300-304 şi Vol III, 1990
Doppler în Patologia Ochiului şi Orbitei, Revista
19. Balta F, Merticariu A, Panait OB. Practica patologiei
Română de Ultrasonografie, 2002;3-4,181-8.
maculare în imagini, Ed. Medicală Antaeus, 2009;4.
13. Transquart F, Berges O, Koskas P and al. Color
20. Mozaffarieh M, Flamer J. Ocular Blood Flow and
Doppler Imaging of Orbital Vessels: Personal Experience
Glaucomatous Optic Neuropathy 2009;27-8,35-9,79-
and Literature Review, Journal of Clinical Ultrasound
98.
2003;31(5):258-72.
21. Sobotta, Atlas of Human Anatomy, vol.1 Head,
14. Selaru DF, Musat O, Stoenescu D. Ghid de diagnostic
Neck,Upper Limb, Edited by R.Putz and R.Pabst in
în angiofluorografia retiniană, Ed. Morosan,
collaboration with Renate Putz, Editia a 14-a, Ed.
2012,14-8.
Elsevier, 2006,363,368-71.
News in Study of Optic Nerve Vascularization
65
ISSN 1843-9306
Revista
„Medical Connections
/ Conexiuni Medicale” are o vizibilitate naţională şi
2068-8369), prin indexarea în Journals Master List a bazei de date internaţionale Index
Copernicus®, începând cu numerele din anul 2009, precum şi datorită includerii în cadrul
schimburilor cu Universitatea Titu Maiorescu, Bucureşti, Facultatea de Medicină şi Medicină
Dentară, şi Sackler School of Medicine afliată la Universitatea Tel Aviv, Hasharon Hospital,
Centrul Medical Rabin din Israel.
Te journal „Medical Connections / Conexiuni Medicale” has a national and international
(ISSN e-serials 2068-8369), and due to the fact that the journal is included in an exchange
program between national and international universities such as Titu Maiorescu University,
Bucharest, Faculty of Medicine ans Dental Medicine, and Hasharon Hospital, Rabin Medical
Center Affiliated with the Sackler School of Medicine, Tel Aviv University. Te “Medical
Connections / Conexiuni Medicale” is indexed in Journals Master List of Index Copernicus®, isues
since 2009.
CASE PRESENTATION
DESMOID TUMOR MASQUERADING AS FIBROADENOMA. CASE
REPORT AND REVIEW OF LITERATURE
Hermann Naama1, Fridel Ludmila2, Grubstein Ahuva3, Sharon Eran1
1Division of General Surgery, Hasharon Hospital, 2Department of Pathology, Beilinson Hospital and 3Department of
Radiology Beilinson Hospital, Rabin Medical Center, Petah-Tikva, affiliated to Sackler Faculty of Medicine, Tel-Aviv
University, Israel
Address for correspondence:
Naama Herman, MD
Department of Surgery B, Hasharon Hospital,
Petah-Tikva, Israel.
Email: naamahe@clalit.org.il
Received: 25.01.2013
Accepted: 15.02.2013
Med Con March 2013, Vol 8, No 1, 67-70
Abstract
Tis case is unique for the initial misdiagnosis of the
lesion as a benign tumor, which can be attributed to the
We present a case of 19 years old women initially
patient’s young age and unremarkable medical history as
diagnosed with fibroadenoma of the breast. She was
well as lack of awareness to the existence of this rare
referred to us for further evaluation of the growing mass.
lesion. Diagnosis is important due to the invasiveness of
Sonography revealed a non vascular, hypo echoic
the tumor and wide local excision must be performed in
irregular lesion. Biopsy of the lesion revealed the typical
order to try to prevent local recurrence.
histology of a desmoid tumor. She underwent wide local
excision,
with
post-operative
histopathology
Case
confirmation of negative surgical margins.
Keywords: Breast, Desmoid, fibromatosis,
A previously healthy 19 years old woman presented
fibroadenoma
to her local clinic with a newly found solitary, firm and
mobile mass in her left breast. At first she was diagnosed
Introduction
as having a fibroadenoma. After complaining of the
mass growing larger over the course of six months, she
Desmoid tumors of the breast are rare fibroblastic
was referred to our hospital for further evaluation.
tumors that comprise
0.2% of all breast tumors.
Te patient had no prior history of trauma or
Although benign, they are often locally invasive and
surgery to the area. Family history was unremarkable.
have a high rate of local recurrence. Clinical presentation,
On clinical examination a non-tender, superficial,
sonography and mammography often mimic carcinoma.
mobile and well defined
2 cm mass was palpated
Histologically, the lesion, which is composed of spindle
superiorly to the areola, on the upper outer quarter of
cell proliferation and collagen deposition, can help in
the left breast. Axillary lymph nodes were not
making the diagnosis. Management remains
palpated. No signs of inflammation or nipple
controversial and the mainstay of treatment is considered
discharge were found. Te patient was sent for a
to be wide local excision with clear margins.
sonography which revealed a hypo echoic irregular
Desmoid Tumor Masquerading as Fibroadenoma. Case Report and Review of Literature
67
CASE PRESENTATION
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
Figure 1. Sonography shows a hypo echoic, ill
Figure 3. Desmoid tumor composed of fascicles of
defined lesion measuring 2.1 cm
spindle cells with fine collagen deposits (H&E x4)
Figure 2. Doppler sonography of the lesion shows
Figure 4. Desmoid tumor with nuclear Beta-
no significant vascularity
Catenin positive immunostaining (x10)
lesion measuring
2.1 cm, without any significant
Discussion
vascularity, Figure 1 and 2.
Based on these findings, it was decided to perform a
Desmoid tumor, or aggressive fibromatosis, is a
Tru-Cut needle biopsy of the lesion. Biopsy revealed
benign mesenchymal monoclonal proliferations
mild fibroblastic
proliferation
and increased
arising from the connective tissue of the muscle and
collagenization with no atypia or mitoses, a finding
overlying the aponeurosis or fascia. Although it does
consistent with fibromatosis. After consulting the
not metastasize, it is characterized by an infiltrative
oncologists and relaying the information to the patient,
growth pattern and carries a high rate of local
a wide excision of the lesion was performed.
recurrence [1,2]. Tumor-related mortality is rare, and
During the operation a mass measuring about 2X2
morbidity is attributed mostly to disfigurement and
cm was excised with additional 1 cm borders. Te lesion
loss of function from local progression or treatment
was confined to the breast tissue and did not involve the
[3].
underlying fascia. Post-operative histopathology
Desmoid tumors represent
1.5-3.5% of all
revealed foci of spindle cell proliferation with fine
connective tissue tumors [4]. Pathogenesis is unknown,
collagen deposits and some myxoid areas, Figure 3.
but hormonal and genetic factors, as well as local trauma
No nuclear atypia or pleomorphism was seen, and
or surgery have all been suggested. Te majority of
mitotic index was low. Staining for Vimentin and Beta-
desmoid tumors occur sporadically, while the minority
Catenin was positive, Figure 4.
is associated Gardner’s syndrome
[5]. A higher
Removal of the lesion was complete with negative
prevalence among females as well as increase in tumor
surgical margins. Te diagnosis of fibromatosis was
size during pregnancy suggests estrogen may also play a
confirmed.
role in the pathogenesis [1].
68
Hermann et al
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
CASE PRESENTATION
Desmoid tumor of the breast is even extremely rare
recurrence is unclear, as some studies showed positive
and comprise
0.2% of all breast tumors
[1].Tese
resection margin to be predictive of recurrence while
tumors can arise either primarily from the breast
others found no such correlation [1,16-19]. Recurrence
parenchyma, or by secondary infiltration from the
rate for secondary breast lesions, arising from the
musculo-aponeurotic layer of the pectoral muscles [6,7].
musculo-aponeurotic tissue of the pectoral muscle, is
Most cases of breast desmoid tumors occur in women
much higher than that of primary mammary
with only rare reports of affected males [8]. Desmoid
fibromatosis, which is reported to be 21-27% [20].
tumor of the breast is thought to be more prevalent
Radiation therapy can provide good local control of
following surgical intervention to the affected area, but
desmoid tumor as a supplement to surgery or even as
can also arise de novo [1,9]. Some recent case reports
the only treatment. Te current trend is that when wide
described cases following saline or silicone implants,
local excision will result with significant compromise of
implying a possible relationship to the prosthetic’s
function or when surgical margins are positive, adjuvant
capsule [7,8].
radiotherapy should be considered [1,17,18].
On physical examination the lesion is often palpated
Systemic treatment such as hormonal and anti-
as a firm, movable mass. Skin retraction or dimpling
inflammatory agents, chemotherapy and biological
may be present. Typical mammography shows irregularly
treatment have all been used with mixed results and are
shaped, uncalcified, high-density mass with spiculated
generally reserved for cases in which local control is not
margins. By sonography the tumor appears to be a
feasible [3,19,21,22].
poorly marginated, hypo echoic mass. Tus clinical
In conclusion, our case of desmoid tumor of the
presentation and imaging can often mimic carcinoma
breast is unusual as it masqueraded as a different benign
[4,7,10,11].
disease
- fibroadenoma. It was different from most
MRI can be useful in distinguishing desmoid tumor
published cases, in which the lesion was described as
from other malignancies of the breast, as well as revealing
mimicking carcinoma of the breast. Te initial diagnosis
the extent of the tumor and relationship to adjacent
in this case can be attributed to the patient’s young age
structures. Te mass appears ovoid or irregular, crosses
and lack of risk factors, as well as the rarity of desmoid
fascial compartments, is isointense on T1- and
tumors arising in the breast parenchyma.
heterogeneously hyperintense on T2-weighted images
and shows bands of low signal on all sequences. Te
lesions displayed moderate to strong heterogeneous
References
enhancement after IV administration of contrast
material [12,13].
1. Neuman H, Brogi E, Abrhaim A, Brennan M, Van
Histologically the lesion is composed of spindle cell
Zee K. Desmoid Tumors (Fibromatoses) of the Breast: a
proliferation with varying amounts of collagen
25-Year Experience. Ann Surg Oncol 2007;15(1):274-
deposition, sometimes with focal myxoid areas.
80.
Fingerlike extensions into adjacent breast parenchyma
2. McDonald E, Eunhee Y, Wenger D. Extraabdominal
and adipose tissue can be seen. Te tumor cells are often
Desmoid-type
Fibromatosis.
Radio
Graphics
organized in broad sheets, in storiform configuration or
2008;28:901-6.
interlacing bundles with herringbone pattern. Overall
3. Melis M., Zager J, Sondak V. Multimodality
cellularity is low to moderate, and mitotic figures are
Management of Desmoid Tumors: How Important Is a
rare. Immunostaining shows variable reactivity for
Negative Surgical Margin? J Surg Oncol 2008;98:594-
desmin and actin, and nuclear staining for Beta-Catenin
602.
is supportive but not pathognomonic [14,15].
4. Ormandi K, Lazar G, Toszegi A, Palko A. Extra
Management remains controversial, since cases are
Abdominal Desmoid Mimicking Malignant Male Breast
scarce and in the literature there are mostly case reports
Tumor. Eur Radiol 1999;9:1120-2.
with no larger study. Mainstay of treatment is considered
5. Brueckl WM, Ballhausen WG et al. Genetic testing for
to be wide local excision with clear margins. A high
germline mutations of the APC gene in patients with
local recurrence rate after excision is reported by several
apparently sporadic desmoid tumors but a family history
series, ranging from
24% to 77% at 10 years [16].
of colorectal carcinoma. Dis Colon Rectum
Unfavorable risk factors related to recurrence after
2005;48(6):1275-81.
excision are young age, tumor > 3 cm, and arguably a
6. Gump FE, Sternschein MJ, Wolff M. Fibromatosis of
microscopic positive surgical margin. Interestingly the
the breast. Surg Gynecol Obstet 1981;152:57-60.
impact of microscopic margin status in predicting
Desmoid Tumor Masquerading as Fibroadenoma. Case Report and Review of Literature
69
CASE PRESENTATION
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
7.
Chummun S, McLean N, Abraham S, Youseff M.
lesions: analysis of a series and review of the literature.
Desmoid tumor of the breast. J Plast Reconstr Aesthet
Histopathology 2007;51(4):509-14.
Surg 2010;63:339-45.
16.
Gronchi A, Casali PG et al. Quality of Surgery and
8.
Glazebrook K, Reynolds C. Mammary Fibromatosis.
Outcome in Extra-Abdominal Aggressive Fibromatosis:
AJR 2009;193:856-60.
A Series of Patients Surgically Treated at a Single
9.
Yiangou C, Fadl H, Sinnet H, Shousha S. Fibromatosis
Institution. J Clin Oncol 2003;21(7):1390-7.
of the Breast or Carcinoma? J R Soc Med 1996;89:638-
17.
Ballo T, Zagars GK, Pollack A, Pisters PW, Pollack
40.
RA. Desmoid Tumor: Prognostic Factors and Outcome
10.
Okamoto K, Kurihara Y et al. Desmoid Tumor of the
after Surgery, Radiation Terapy, or Combined Surgery
Breast: Te Role of Proton Magnetic Resonance
and Radiation Terapy. J Clin Oncol 1999;17:158-67.
Spectroscopy for a Benign Breast Lesion Mimicking a
18.
Nuyttens J, Rust P, Tomas C, Turrisi A. Surgery
Malignancy. Breast J 2008;14(4):376-8.
versus Radiation Terapy for Patients with Aggressive
11.
Erguvan-Dogan B, Dempsey P, Ayyar G, Gilcrease
Fibromatosis
or
Desmoid Tumors. Cancer
M. Primary Desmoid Tumor
(Extraabdominal
2000;88(7):1517-23.
Fibromatosis) of the Breast. AJR 2005;185:488-9.
19.
Lev D, Kotilingam D et al. Optimizing Treatment of
12.
Nakazona T, Satoh T, Hamamoto T, Kudo S. Dynamic
Desmoid Tumors. JCO 2007;25(13):1785-91.
MRI of fibromatosis of the breast. Am J Roentgenol
20.
Schwarz G, Drotman M et al. Fibromatosis of the
2003;181:1718-9.
Breast: Case Report and Current Concepts in the
13.
Lee J, Tomas J, Phillips S, Fisher C, Moskovic E.
Management of an Uncommon Lesion. Breast J
Aggressive Fibromatosis: MRI Features with Pathologic
2006;12(1):66-71.
Correlation. AJR 2006;186:247-54.
21.
Dufresne A, Bertucci F et al. Identification of biological
14.
In: Rosen P.P. Rosen’s Breast Pathology,
3rd ed.
factors predictive of response to imatinib mesylate in
Philadelphia: Lippincott Williams & Wilkins, Benign
aggressive fibromatosis. B J Cancer 2010;103:482-5.
Mesenchymal Neoplasms 2009;829-37.
22.
Janinis J, Patriki M, Vini L, Aravantinos G, Whelan JS.
15.
Carlson J W, Fletcher CD. Immunohistochemistry for
Te pharmacological treatment of aggressive fibromatosis:
beta-catenin in the differential diagnosis of spindle cell
a systematic review. Ann Oncol 2003;14(2):181-90.
70
Hermann et al
CASE PRESENTATION
METAL STENTS OF THE URETER ARE THEY INNOCENT?
Stein Avi, Freifeld Yuval, Klein Ilan, May Tal, Muhad Yichie, Mecz Yoel, Goldin Dmitri, Faris Gazi,
Kaploun Alexander, Dekel Yoram
Department of Urology, Carmel Medical Centre, Haifa, affiliated to Faculty of Medicine, Teknion University, Haifa,
Israel
Address for correspondence:
Avi Stein, M.D.
Tel: 972 4 8341029, Fax: 972 777577770, Cell: 972 544709767
Email: stein37@netvision.net.il
Received: 10.01.2013
Accepted: 20.02.2013
Med Con March 2013, Vol 8, No 1, 71-72
Abstract
Te objective of this study was to described a case of
endometrial carcinoma of uterus, treated by surgery and
A 69 years old female was diagnosed on 1998 with
adjuvant radiotherapy. She developed severe strictures
endometrial carcinoma requiring surgery and adjuvant
of both distal ureters. A metal stent caused a
radiotherapy. She developed severe strictures of both
complication posing a clinical and surgical challange.
distal ureters, treated by a metal stent inserted in the
distal right ureter.
Case report
Keywords: radiotherapy, ureters, strictures, Metal
ureteral stents
A 69 years old female was diagnosed on 1998 with
endometrial carcinoma requiring surgery and adjuvant
Introduction
radiotherapy. On 2000 she developed severe strictures of
both distal ureters treated with repeated double J ureteral
Metal ureteral stents are a relatively new version of a
stent insertions and bilateral nephrostomy tube
device with a long history of relieving ureteral
placements. A metal stent was inserted in the distal right
obstruction. Metal stents are effective for relieving
ureter. On
2005 end stage renal disease developed
ureteral obstruction but success regarding patient
requiring chronic hemodialysis. Two years later, on 2007,
tolerability has been variable [1].
she underwent renal transplantation and had an
Ureteral stenosis secondary to radiation-induced fibrosis
uneventful recovery and normal kidney function. She
is a well-known, late complication of radiation treatment in
first presented at our institution on 2010 with macroscopic
patients with carcinoma of the uterine cervix. Te incidence
hematuria and recurrent urinary tract infections.
was
15% in patients treated with standard doses of
Computerized tomography detected a large bladder stone
radiotherapy for carcinoma of the uterine cervix [2].
in continuity with a distal ureteral stent (Figure 1).
Patients who were treated with centrally blocked
Cystoscopy revealed a large bladder stone. Laser
external fields or who received more than two
disintegration of the stone was started until the
transvaginal radiation treatments were at increase risk
appearance of a distal part of a metal wall stent which
for developing ureteral stenosis [3].
was obstructed by calcifications. Te calcifications in the
Metal Stents of the Ureter are they Innocent?
71
CASE PRESENTATION
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
disintegration accompanied by stent removal has been
reported to treat such pathology in left over plastic or
silicone stents [5,6]. Te reported case posed an interesting
clinical question if laser disintegration of the bladder
stone and removal of the metal parts of the stent
protruding into the bladder is an adequate solution of the
problem, or whether the stent has to be removed from the
ureter. Tis would not be a question if the discussed
ureter would have been an active ureter. In patients with
difficult ureteric obstructions a metallic stent provides a
safe and effective alternative to an indwelling double-
pigtail catheter or percutaneous nephrostomy [7].
In our case the involved right native kidney was
non-functioning. Retrospectively this was a good
Figure 1. Te computer tomography shoved the
decision as the patient remained asymptomatic on one
stone and stent
year follow-up.
lumen of the stent were lasered and the stent coils were
References
removed by cup biopsy until a flat bladder surface was
obtained at the level of the right ureteral orifice. Te
1.
Benson AD, Taylor ER, Schwartz BF. Metal ureteral
patient had an uneventful recovery. One year after the
stent for benign and malignant ureteral obstruction. J
procedure, urine cultures were negative and no
Urol 2011;185(6):2217-22.
hematuria reappeared. Te ureteral part of the stent was
2.
Buglione M, Toninelli M, Pietta N, et al. Post-
left in place and required no treatment, as the patient
radiation pelvic disease and ureteral stenosis:
remained asymptomatic.
physiopathology and evolution in the patient treated for
cervical carcinoma. Review of the literature and
Discussion
experience of the Radium Institute. Arch Ital Urol
Androl 2002;74(1):6-11.
Radiotherapy to the pelvis has been widely described
3.
McIntyre JF, Eifel PJ, Levenback C, Oswald MJ.
to cause obstruction of distal ureters [4].
Ureteral stricture as a late complication of radiotherapy
Late ureteral fibrosis is a common and distressing
for stage IB carcinoma of the uterine cervix. Cancer
treatment-related complication in patients treated with
1995;75(3):836-43.
radiotherapy for cervix carcinoma. Newer strategies in
4.
Sklaroff DM, Gnaneswaran P, Sklaroff RB.
better defining the target for radiotherapy,
Postirradiation ureteric stricture. Gynecol Oncol
conformational radiotherapy and better understanding
1978;6:538-45.
of biologic factors will contribute to further reducing
5.
Tsai CC, Shen JT, Huang SP, et al. Use of a Holmium
the frequency of such a complication [2].
laser to treat a forgotten double-J stent with whole stent
Silicone or plastic ureteral stents are most commonly
encrustations: a case report. Kaohsiung J Med Sci
used to relieve obstruction, but need to be periodically
2009;25:567-71.
replaced and provide a temporary solution to this
6.
Liatsikos EN, Kagadis GC, Barbalias GA, Siablis D.
problem. To overcome the need for frequent repeated
Cystoscopic holmium lithotripsy of large bladder calculi.
replacements, metal stents have been suggested. Several
J Endourol 2005;19:934-9.
types of metal stents have been used including Resonance®
7.
Wakui M, Takeuchi S, Isioka J, Iwabuchi K,
and Urolume®. Bladder stones may develop around
Morimoto S. Metallic stents for malignant and benign
protruding forgotten synthetic stents and laser stone
ureteric obstruction. BJU Int 2000;85(3):227-32.
72
Stein et al
EDITORIAL APPEARANCE
ENCYCLOPEDIA OF CRISIS MANAGEMENT
Publisher SAGE Publications Inc, March
2013,
ISBN 9781452226125, Editors: K. Bradley Penuel,
Matt Statler - New York University and Ryan Hagen at
Columbia University. SAGE Publications is the largest
independent academic publisher in the world. His
publications in more than 30 areas, most with university
or postgraduate educational aim, include only
encyclopedias in more than 60 different areas. SAGE is
the 5th largest publisher in the world as regarding the
scientific journals (over 700) in the most diverse fields:
social sciences, technology, medicine, and so on.
Encyclopedia of Disaster Management is considered
as a collection of
385 chapters signed by over 150
authors, who are organized alphabetically, in two
volumes with over 1,100 pages.
Authors belong to some of the most prestigious
universities in the world: from USA- Princeton
University, New York University, Columbia University,
from the UK- Oxford University, Coventry University
both in the country (a career of specialist in anesthesia,
and the University of Glasgow, China-Beijing Academy
intensive care and emergency medicine, earthquake of
of Science and Technology, Turkey- Istanbul Technical
1977 ) and abroad (Somalia in 1993, Turkey in 1999,
University and Selcuk University, Italy- University for
the former Yugoslav space, etc.), and the didactic work
Foreigners of Perugia, India- National Institute of
obtained by university or extra-university courses in this
Disaster Management Delhi, Israel- Ben Gurion
area, especially through coordination of Romania first
University of the Negev, to the University of Tasmania
master of Disaster Medicine.
and Hawaii, but also prestigious international executive
Chapter prepared by Professor Dan Mănăstireanu
structures- Global Risk Forum Davos, Taiwan Centers
introduces us in a discipline in which all doctors should
for Disease Control.
be trained today, inevitably confronted with the
In this select company, Titu Maiorescu University
vicissitudes of nature or terrorist attacks. Although we
of Bucharest, through Prof. Dr. Dan Mănăstireanu,
tend to think that we are facing a new medical discipline,
author of the chapter „Triage”, is the only school in
the author demonstrates that its history it sees during
Romania and among the few in Europe, agreed to
Napoleon’s campaigns: „Triage (...) (in a hospital) the
contribute to the prestigious Encyclopedia of Crisis
process of deciding how seriously ill/sick or injured a person
Management.
is, so that the most serious cases can be treated first. Te
Relatively new field, crisis management is presented
term comes from the French verb
„trier” imposed by
thematically in chapters; the book has also a preface
Dominique Jean, Baron Larrey (1766-1842), a military
with mentions linked by large ranges of theoretical fields
surgeon under Napoleon (who also described in his work
(health, agencies and organizations, theories and
things such as the type of hip amputations needed in
techniques, economic crises, etc).
situations of war, the condition known as trench foot, and
Prof. Dan Mănăstireanu’s contribution, the chapter
the term „stretcher-bearer”). British surgeon John Wilson
on „Medical triage in disaster situations” reflects the
proposed in 1846 using different types of treatments to be
experience of the teacher of UTM in specialized work
consistent with the chance of survival, thus inspiring
73
EDITORIAL APPEARANCE
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
categories of treatments on levels of triage. Military
unusual situations and methods. Triage should be dynamic,
medicine over the years had a significant impact on the
continuous, progressive and adaptable to changes both in
development of medical triage. Te difference in doctrine
the needs of victims and the need / use of resources.”
between the two types, civil and military triage, lies in the
Te conclusion chapter draws our attention to: „Te
strategies of the two entities, the war and the need to have
rules of an effective triage are: Anything that can help
as soon as possible fighters in a very short time with the aim
organize and improve the medical answer in disasters is
of assisting as many victims as possible.”
good and should be used. Triage in disaster situations is
Modern definition of triage is presented accurately:
different from that of everyday situations. Te most
„Triage is a formal system used to identify, classify and treat
important factors taken into account in crisis situations are
victims, according to their severity of suffering. Under the
staff and logistics. For the triage to achieve its goal, all
guidance and goal of disaster medicine, offering a chance to
victims should receive the same attention at primary triage.
be saved to as many people as possible”.
No single group of patients can take priority over another;
One by one we are introduced to the methods of
this must be done only in accordance with considerations
triage, triage at disaster place, triage methodology or
regarding their general state. Tis statement includes
severity factor. Author gives us precise instructions
children.”
through the key points of the whole action: „Te lack of
Medical Connections magazine was among the
adequate resources, the high number of victims and
promoters in the publishing space of Disaster Medicine
unexpected aspects are limiting factors in triage. Te
domain, one of Prof. Dr. Dan Mănăstireanu works was
unexpected aspects refer to the disruption of daily life
published in 2011: „What to do in the event of a
patterns and the necessity of adapting existing means to
disaster”, Med Con March 2011; Vol 6, No 1, 87-94.
74
GUIDANCE FOR DRAWING UP
GUIDANCE FOR AUTHORS
Scope
Patient consent forms
Te Medical Connections publishes papers
Te protection of a patient’s right to privacy is
reporting original clinical and scientific research,
essential. Please send copies of patient’s consent forms
which contribute to the advancement of knowledge
on which patients or other subjects of your
in all field of medicine. Te journal also publishes
experiments clearly grant permission for the
reviews, editorials and short communications on
publication of photographs or other material that
specific topics. Case reports will be accepted if of
might identify them. If the consent form for your
great interest and well investigated. Letters to the
research does not specifically include this, please
Editor, especially those mentioning an opinion on an
obtain it or remove the identifying material. A
article previously published, or expressing a new
statement must be included in the ‘Methods’ section
finding are welcome. Te website address of the
of your paper.
Medical
Connections
is
conexiunimedicale.ro. Te journal is published
Ethics Committee approval
quarterly and papers are accepted for publication in
You must state clearly in your submission in the
English language. Papers from contributors living
Methods section that you conducted studies on
abroad and from Romanian authors should be
human participants with the approval of the Hospital,
addressed to the editorial office: dr. Bumbuluţ Călin,
or University Ethics Committee etc. Similarly, you
assitant editor in chief of Medical Connections,
must confirm that experiments involving animals
Eroilor Revoluţiei Pl. no.23-440055 Satu Mare,
adhered to ethical standards.
Romania. Tel./Fax:
+40-261-710456, e-mail:
bumbulutcalin@yahoo.com.
Copyright assignment
Papers are accepted for publication on the
Redundant or duplicate publication
understanding that exclusive copyright in the paper is
We ask you to confirm that your paper has not
assigned to the Publisher. Authors may use material
been published in its current form or a substantially
from their paper in other works published by
similar form, that it has not been accepted for
themselves.
publication by another journal, and that it is not
under consideration by another publication.
Submissions
All manuscripts submitted to the Medical
Conflicts of interest
Connections are made available for online review.
We ask authors to state all possible conflicts of
Te journal introduced the electronic submission of
interest, including financial and other relationships.
manuscripts in Word format, but also accepts
If you are sure that there is no conflict of interest,
manuscripts submitted as attachments to electronic
please state this also. Te sources of funding should
mail (text, figures and tables). Do not send them in
be acknowledged in your paper.
PDF format. Te word count for electronic
submissions is up to 3,500 words for original articles,
Permissions to reproduce previously
2,500 words for case reports,
2,000 for clinical
published material
imaging papers, 500 words for letters, and 4,500
Please send us copies of permission to reproduce
words for review articles. Authors should NOT in
material (such as illustrations) from the copyright
addition post a hard copy submission to the editorial
holder.
office, unless they are supplying artwork, letters or if
75
GUIDANCE FOR DRAWING UP
MEDICAL CONNECTIONS • NUMBER 4 (28) • DECEMBER 2012
les that cannot be submitted electronically, or have
hospital, in the general community etc; Participants
been instructed to do so by the editorial office. For
- indicate the number of study subjects and how they
those authors who have no option but to submit by
were selected, recruited, and assigned to the
mail please send one copy of the article, plus an
intervention; Intervention - report the method of
electronic version on disk or CD-ROM to the
administration and duration of the intervention.
Editorial Office, Conexiuni Medicale/Medical
Results
Connections, Str. Eroilor Revoluţiei Pl. no.23
Provide the main outcomes of the study, including
-440055 Satu Mare, Romania. Double spacing
confidence intervals or p values.
should be used throughout the manuscript, which
Conclusion
should include the following sections, each starting
State only conclusions that are directly supported
on a separate page: title page, abstract and key words,
by the evidence and the implications of the findings.
text, acknowledgements, references, individual tables
Review articles and case reports should include an
and legend for figures. Pages should be numbered
unstructured summary.
consecutively, beginning with the title page, and the
Keywords
Arabic numbers should be placed in the top right
Te abstract should be followed by a list of 3-10
hand corner of each page.
keywords or short phrases which will assist the cross-
indexing of the article and which may be published.
Presentation of papers
When possible, the terms used should be from the
Title page
Medical Subject Headings 262 list of Index Medicus
Te title page should carry the full title of the
paper and a short title to be used as a short ‘running
Text
head’ (and which should be so identified and should
Full papers of an original study may be divided
comprise up to 45 characters). Te first name, middle
into sections headed Introduction, Methods
initial and last name of each author should appear. If
(including ethical and statistical information), Results
the work is to be attributed to a department or
and Discussion (including a conclusion). Tis so-
institution, its full name should be included. Any
called “IMRAD” structure is not simply an arbitrary
disclaimers should appear on the title page, as should
publication format, but rather a direct reflection of
the name and address of the author responsible for
the process of scientific discovery. Long articles may
correspondence concerning the manuscript and the
require subheadings within some sections (especially
name, address and e-mail address of the author to
the Results and Discussion sections) to clarify their
whom requests for reprints should be made (the
content. Other types of articles, such as case reports,
author should mention if he does not want his e-mail
reviews, and editorials, are likely to require other
address to be published). Finally, the title page should
formats. Excessive use of abbreviations is not
include the sources of any support for the work in the
recommended. Outline statistical methods used.
form of grants, equipment, drugs, or any combination
Identify drugs and chemicals used by generic name (if
of these.
trade-marks are mentioned, manufactured name and
Abstracts
city should be given).
Te second page should carry a structured
abstract of no less than
200 words. Do not use
Acknowledgements
abbreviations, footnotes, or references.
Acknowledgements should be made only to those
Background & Aims
who have made a substantial contribution to the
Describe the importance of the study and the
study. Authors are responsible for obtaining written
precise research objective(s) or study question(s).
permission from people acknowledged by name in
Methods
case readers infer their endorsement of data and
Methods should include information on the
conclusions.
following aspects of study design when applicable:
References
Design
- describe the basic study design, e.g.
References should be numbered consecutively in
randomized controlled trial, cross sectional study,
the order in which they first appear in the text. Tey
cohort study, case series, survey etc; Setting - specify
should be assigned Arabic numerals, which should be
whether the study was conducted in a primary or
given in brackets, e.g. [12]. References should include
tertiary care setting, in an ambulatory care clinic or
the names of all authors when six or fewer; when seven
76
MEDICAL CONNECTIONS • NUMBER 4 (28) • DECEMBER 2012
GUIDANCE FOR DRAWING UP
or more, list only the first three names and add et al.
for which an abbreviation stands should precede its
References should also include full title and source
first use in the text unless it is a standard unit of
information. Journal names should be abbreviated as
measurement.
in Index Medicus
serials/terms_cond.html). No more than
90-100
Reprints
references will be accepted for reviews. For Letters to
Ten reprints of the published articles and two
the Editor, 5-6 references. Avoid or keep as low as
copies of the Journal will be supplied free of charge. If
possible the use of abstracts as references. Personal
required in a greater number, they will be available on
communications and unpublished work should not
payment of the necessary cost.
feature in the reference list but should appear in
parentheses in the text. Unpublished work accepted
Editorial policy
for publication but not yet released should be included
We welcome all contributions in the field of
in the reference list with the words “in press” in
medicine. We invite known personalities with
parentheses beside the name of the journal concerned.
expertise and many published papers in a specific
Tables
field to write reviews and editorials in our journal. We
Each table should be assigned a Roman numeral
accept original papers and case reports from all
(e.g. Table III) and a brief title. Explanatory matter
countries.
Te Conexiuni Medicale/Medical
should be placed in footnotes. Explain in footnotes
Connections offers thorough peer review and
all non-standard abbreviations that are used in each
immediate publication on acceptance. Te redactor-
table. Identify statistical measures of variations, such
in-chief or one of the first reads the manuscripts
as standard deviation and standard error of the mean.
received and in about 1-3 weeks decide upon their
Each table should be cited in the text.
priority level: some are immediately sent to the
Illustrations
reviewers, some are rejected without being sent for
All graphs, photographs
(on glossy paper),
review and some are returned to authors with
diagrams will be referred to as figures and should be
suggestions for improvement before submitting them
numbered consecutively in the text in Arabic
to reviewers.
numerals. If a figure has been published before, the
original source must be acknowledged and written
Peer-review procedure
permission from the copyright holder for both print
Te Conexiuni Medicale/Medical Connections
and electronic formats should be submitted with the
promotes evaluation of all the original papers by two
material. Figures may be reduced, cropped or deleted
or three independent reviewers, of whom two are
at the discretion of the Editor.
international personalities. Te peer-review process is
Legends for illustrations
essential for ensuring the quality of the scientific
Captions should have an Arabic numeral
information disseminated. Te reviewers are asked to
corresponding to the illustration to which it refers
evaluate the manuscript by applying the same
with a title above and explanatory notes below it.
standards as for the international journals. Te
Internal scales should be explained and staining
reviewers send their comments to the Editor. Te
methods for photomicrographs should be identified.
Editor will inform the authors about the suggestions
Units of measurement
made by the referee and ask them to answer the
Measurements of length, height, weight, and
questions and make the required corrections. Tis
volume should be reported in metric units (meter,
information is provided up to three months from the
kilogram, or litre) or their decimal multiples.
date they submitted the paper to the journal. Te
Temperatures should be given in degrees Celsius.
revised manuscript should be sent in no more than
Blood pressures should be given in mmHg. All
one month to the Editor. When the Editor receives
hematological and clinical chemistry measurements
the corrected version with all changes marked,
should be reported in the metric system in terms of
accompanied by a letter with a point-by-point reply
the International System of Units (SI).
to the reviewers’ comments, he sends those back to
Abbreviations and symbols
the same reviewer, who makes the final
Use only standard abbreviations. Avoid
recommendation for acceptance or rejection of the
abbreviations in the title and abstract. Te full term
manuscript.
77
GUIDANCE FOR DRAWING UP
MEDICAL CONNECTIONS • NUMBER 4 (28) • DECEMBER 2012
Notice to subscribers
colour page on inside front or inside back cover: Euro
Te annual subscription rates for 2013: 80 RON
350 1 issue, 1400 4 issues. Full colour page ouside
individual,
160 RON institutional. Foreing
back cover: Euro 400 1 issue, 1600 4 issues. Bank
subscribers:
75
$ individual,
150
$ institutional.
account: Colegiul Medicilor Satu Mare, CUI
Additional postage: surface mail 20
$, for overseas air
9839430, Banca Transilvania, branch Agenţia
mail 40
$. Bank account: Colegiul Medicilor Satu
Golescu Satu Mare, IBAN: RO38 BTRL 0310 1202
Mare, CUI 9839430, Banca Transilvania, branch
K392 62XX (RON) IBAN: RO62 BTRL 0310 2202
Agenţia Golescu Satu Mare, IBAN: RO38 BTRL
K392 62XX (USD) Swift: BTRLRO22.
0310 1202 K392 62XX (RON) IBAN: RO62 BTRL
0310 2202 K392 62XX (USD) Swift: BTRLRO22.
© Copyright Conexiuni Medicale/Medical
Orders should be sent to the Editorial Office, Eroilor
Connections, Satu Mare, 2013
Revoluţiei Pl. no.23-440055 Satu Mare, Romania.
No part of this publication may be reproduced,
Tel./Fax:
+40-261-710456 or +40-361-408164, or
stored in a retrieval system or transmitted in any form
by e-mail: colmedsm@gmail.com.
or by any means without prior permission in writing
of Conexiuni Medicale/Medical Connections.
Notice to advertisers
Permission is not however required to copy abstracts
Applications for advertisement space and for rates
of papers or of articles on condition that a full
should be addressed to the Editorial Office of
reference to the source is shown. Correspondence
Conexiuni Medicale/Medical Connections. 2013
regarding permission to reprint all or part of any
advertising rates are Euro 200 full (A4) colour page, 1
article published in this journal should be addressed
issue, and Euro 800 full colour page, 4 issues. Full
to the Editor, e-mail: colmedsm@gmail.com
78
EDITORIAL
Drogaţi cu bucate
„Omul îşi sapă mormântul cu dinţii”
(Proverb hindus)
În anul
1487 Giovanni al II-lea Bentivoglio,
secretă o proteină care trece bariera hemato-encefalică şi
conducătorul Bolognei a organizat un mare banchet cu
ajunge în hipotalamus unde suprimă senzaţia de foame.
ocazia căsătoriei fiului său Hanibal cu Lucreţia d’Este.
El a botezat-o leptină de la grecescul leptos care
Ospăţul a durat şapte ore, de la 8 seara până la
3
înseamnă slab. Şoriceii modificaţi genetic la care nu
dimineaţa, timp în care s-au servit: aperitive şi prăjituri
funcţiona leptina deveneau rapid obezi. O problemă
din aluat moale cu unt şi vin dulce; porumbei fripţi,
majoră de sănătate, obezitatea, părea să ţină de un
ficăţei, sturzi, potârnichi cu măsline marinate şi struguri;
simplu mecanism de feed-back defect. Din păcate
un castel de zahăr cu creneluri şi turnuri plin de păsări
lucrurile au început să se complice în clipa când s-a
vii ce şi-au luat zborul în momentul servirii, un căprior
descoperit că leptina joacă un rol esenţial în
şi un struţ fript înconjuraţi de felurite aluaturi; căpăţâni
comportamentul adictiv. Animalele de laborator
de viţel, claponi rasol; piepturi şi pulpe de viţel; iezi;
dependente de heroină suferă mult mai greu în perioada
cârnaţi; porumbei cu sosuri; păuni fripţi împodobiţi cu
de sevraj dacă sunt şi înfometate. Probabil hormonul
penele lor în chip de roată; mortadela (salam gros copt şi
saţietăţii suprimă nu numai dorinţa de hrană, ci şi de
aromat cu mărar); iepuri şi căpriori serviţi în rântaş şi
anumite droguri. Oricine a ţinut o cură de slăbire ştie ce
reîmbrăcaţi în pielea lor încât păreau vii; turturele şi
greu este să renunţi la vechile obiceiuri. Să fie oare şi
fazani din al căror cioc ieşeau flăcări; sucuri de citrice şi
obezitatea o formă de dependenţă? La prima vedere, nu!
diverse sosuri. Au urmat apoi torturi de zahăr cu migdale
O persoană care mănâncă prea mult nu dezvoltă
în formă de palate din care au ieşit iepuri vii, brânzeturi
toleranţă la mâncare, iar cei puşi la regim nu fac
şi biscuiţi. Au continuat cu purcei de lapte rumeniţi
simptome de sevraj. La o privire mai atentă, observăm
întregi şi friptură de raţă sălbatică. În încheiere s-au adus
că obezii au unele semne de dependenţă: o dorinţă
dulciuri din lapte şi gelatină, pere, paste, zaharicale,
puternică de a mânca şi pierderea autocontrolului până
marţipan şi alte delicatese. Toate au fost însoţite de
la a-şi neglija alte nevoi. Din punct de vedere
vinuri de preţ. După cum relatează cronicarul Cherubino
neurobiologic cele două afecţiuni sunt similare. Fibre
Ghirardacci „înainte să fie puse dinaintea mesenilor,
nervoase care merg de la trunchi la nucleul accumbens
bucatele erau purtate cu foarte mare onoare în jurul
secretă din abundenţă dopamină ori de câte ori trăim o
pieţei palatului…pentru a fi arătate poporului, ca să
surpriză sau o plăcere, cum ar fi o masă excelentă.
vadă atâta măreţie”.
Similar, cocaina şi amfetamina cresc nivelul de dopamină
Prima întrebare pe care ţi-o pui, citind această
din nucleul accumbens de 10 ori declanşând un val de
relatare, este cine poate mânca atâta? Portretele
plăcere. Acest sistem de recompensă controlează
Renaşterii italiene ne arata nişte nobili supli care,
hipotalamusul, care la rândul lui
reglează
asemeni poporului de rând, probabil mai mult au privit
comportamentul alimentar. Şoriceii modificaţi genetic
decât au mâncat. Chiar şi un obez s-ar declara înfrânt de
care nu mai produc dopamină pur şi simplu nu mai au
un asemenea ospăţ. În ciuda imaginilor ispititoare
dorinţa de a mânca ceva şi mor prin înfometare. Dacă li
organismul are mecanisme de control care pot bloca
se injectează dopamină le revine pofta de mâncare.
comenzile
creierului.
Mecanismele fiziologice
În
2001, Gene-Jack Wang de la Laboratorul
funcţionează la fel de bine şi în sens invers: în ciuda
Naţional Brookhaven şi Nora Volkow de la Laboratorul
hotărârii de a ţine regim, foamea ne poate împinge la
Naţional privind Abuzul de Droguri au confirmat rolul
gesturi nesăbuite.
dopaminei în comportamentul alimentar. Folosind
În anul
1994, Jeffrey M. Friedman de la
tomografia cu emisie de pozitroni ei au măsurat
Universitatea Rockfeller a descoperit că adipocitele
cantitatea de receptori de dopamină din corpul striat al
79
EDITORIAL
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
unor voluntari supraponderali şi au constatat că aceasta
plăcerea şi aversiunea legate de mâncare. Ea a studiat
se corelează strâns cu indicele masei corporale. Ca şi
imaginile tomografice cu emisie de pozitroni ale
dependenţii de droguri, obezii suferă de o lipsă relativă
cortexului orbito-frontal la nouă subiecţi în timp ce
de dopamină, fapt care îi obligă să caute noi satisfacţii în
aceştia mâncau ciocolata lor favorită. Activitatea
mâncare. Dopamina în exces, care apare astfel, duce la
creierului a crescut atât în zona asociată senzaţiilor
reducerea numărului de receptori ca şi în cazul cocainei.
gustative, dar mai ales în regiunea orbito-frontală.
Kevin LaBar de la Universitatea Duke a studiat cu
Subiecţii au continuat să mănânce ciocolată până au
ajutorul rezonanţei magnetice nucleare amigdala, care
ajuns la greaţă. În acel moment activitatea în partea
este implicată în excitaţie şi răspunsul emoţional. Nouă
centrală a zonei orbito-frontale s-a „stins”, reapărând în
subiecţi sănătoşi au fost puşi să privească o serie de
părţile laterale ale aceleiaşi zone.
imagini de alimente, de automobile şi de unelte după o
Toate aceste experimente demonstrează că creierul
înfometare de 8 ore şi respectiv după o masă bună.
procesează stimulii legaţi de alimentaţie în acelaşi fel ca
Amigdala subiecţilor înfometaţi devenea instantaneu
şi ceilalţi stimuli adictivi. Controlul comportamentului
activă când priveau un lucru comestibil. După masă ea
alimentar pare deci să fie considerabil în obezitate. Cum
nu mai răspundea la imaginile cu alimente. Studiile
de voinţă nici nu poate fi vorba, s-a apelat la medicamente
similare făcute pe dependenţii de cocaină la Universitatea
folosite pentru dependenţii de droguri. De exemplu,
Emory au dat rezultate asemănătoare. Se pare că amigdala
naltrexona, un antagonist al opioizilor, a determinat
acţionează ca o sonerie de alarmă care sună ori de câte ori
oprirea creşterii în greutate. Rimonabantul, un blocant
descoperă ceva important pentru supravieţuirea
al receptorilor canabinoizilor endogeni, ajută la slăbit,
organismului: fie un lup periculos, fie o masă bogată.
dar numai în anumite limite. Medicamentele nu sunt
O altă regiune a creierului implicată în
încă o soluţie, mai ales că nu avem nici o idee privind
comportamentul adictiv este cortexul orbito-frontal.
efectul lor pe termen lung. Deocamdată ne limităm la
Pacienţii cu leziuni în această zonă nu se pot controla,
tratamentul consecinţelor obezităţii precum diabetul
acţionează impulsiv şi au un oarecare comportament
zaharat de tip 2, deşi chiar şi aici avem probleme. De
adictiv. La dependenţii de droguri această zonă este mai
aceea cred că cel mai bun mod de a ne înfrâna pofta de
puţin activă. Dana M Small de la Universitatea Yale a
mâncare este să ne amintim că mâncatul este cel mai
demonstrat că regiunea orbito-frontală procesează
primitiv mod de a ne consola.
Dr. Sever-Cristian Oană
80
Original articles
ROLUL PARAMETRILOR BIOUMORALI ÎN STABILIREA CONDUITEI
TERAPEUTICE LA PACIENTUL CU COLICĂ RENALĂ FEBRILĂ LITIAZICĂ
Lăpuşan Carmen, Crişan Nicolae, Cucu Vlad, Coman Ioan
Secţia Clinică de Urologie, Spitalul Clinic Municipal Cluj-Napoca, Universitatea de Medicină şi Farmacie „Iuliu
Haţieganu” Cluj-Napoca
Adresa pentru corespondenţă:
Dr. Lăpuşan Carmen
Str Tăbăcarilor 11, cod 400139, Cluj-Napoca, Cluj
Tel: 0745-316717
Email: carmenlapusan@yahoo.com
Primit: 10.12.2012
Acceptat: 15.02.2013
Med Con March 2013, Vol 8, No 1, 81-86
Rezumat
dimensiunea calculului (p<0,0001), gradul hidronefrozei
(p<0,0001) şi severitatea sepsei (p<0,0001).
Introducere: Una dintre cele mai frecvente patologii
Concluzii: Colica febrilă rămâne o urgenţă
urologice o reprezintă colica renală febrilă, cu potenţial
urologică. Remisia fenomenului septic în primele ore de
evolutiv spre sepsă, situaţie în care concomitent cu
la iniţierea terapiei de resuscitare poate fi urmată de
terapia specifică de resuscitare se consideră obligatorie
pasajul spontan al calculului, în special dacă este localizat
dezobstrucţia tractului urinar
distal şi are dimensiuni mici.
Obiectiv: de a evalua în mod independent şi în
Cuvinte cheie: litiază uretrală infectată, colică
asociere parametrii clinici şi bioumorali în vederea
renală febrilă, dezobstrucţie urinară
stabilirii eventualei valori predictive pentru necesitatea
dezobstrucţiei urinare la pacienţii cu colică renală febrilă
Introducere
de natura litiazică.
Materiale şi metode: Studiul este de tip prospectiv
Sepsa cu punct de plecare urinar are incidenţă
şi include toţi pacienţii cu litiază renoureterală şi colică
crescută atât în secţiile cu profil urologic cât şi în cele de
febrilă
(peste
38°C) care s-au prezentat la
terapie intensivă, fiind cunoscut faptul că evoluţia şi
Compartimentul de Primire Urgenţe din cadrul
prognosticul pacientului septic depind de diagnosticul
Spitalului Clinic Municipal Cluj în perioada 1 aprilie
precoce şi instituirea rapidă a tratamentului
[1-3].
2010-31 decembrie 2012. Protocoalele de diagnostic şi
Diagnosticul pacientului cu urosepsis se face pe criterii
tratament sunt standardizate. Parametrii clinici evaluaţi
clinice, imagistice şi de laborator, iar oportunitatea şi
sunt: vârsta, sexul, stadiul urosepsei la internare, diabet
momentul optim pentru intervenţia urologică sunt în
zaharat, neoplazii active, dimensiunile şi localizarea
continuare doar relativ definite [1,2,4]. Una dintre cele
calculului, gradul hidronefrozei, manevre urologice
mai frecvente patologii urologice o reprezintă colica
asupra tractului urinar.
renală febrilă, cu potenţial evolutiv spre sepsă, situaţie în
Rezultate: Au fost internaţi 142 pacienţi pentru
care concomitent cu terapia specifică de resuscitare se
colică renală febrilă (peste 38°C) prin obstacol litiazic
consideră obligatorie dezobstrucţia tractului urinar
între 2010 şi 2012. Decizia de a efectua drenajul urinar
[1,4,5]. Studii recente au evidenţiat o creştere continuă
s-a asociat semnificativ statistic cu localizarea şi
a incidenţei urolitiazei infectate, aceasta dublându-se
The Therapeutic Approach in Febrile Lithiasic Renal Colic-Single Center Experience
81
Original articles
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
practic în ultimii zece ani. Acelaşi trend ascendent a fost
dar şi tipul de germeni implicaţi în declanşarea stării
observat şi în asocierea urolitiazei cu sepsa, rata
septice precum şi sensibilitatea acestora la antibiotice.
mortalităţii ramânând însă nemodificată (0,2-0,25%)
Decizia de dezobstrucţie urinară a fost luată
[6]. La ora actuală există o serie de criterii nespecifice
conform recomandărilor din ghidurile EAU în vigoare:
prin care se stabileşte indicaţia de drenaj urinar la
febra peste 38°C, leucocitoza cu neutrofilie şi persistenţa
pacientul cu colică renală: febră peste 38°C, leucocitoză
durerii peste 24 de ore în contextul utilizării analgosedării
cu neutrofilie şi persistenţa durerii în pofida analgeziei
corespunzătoare. De asemenea, antibioterapia şi terapia
adecvate. Există însă anumite situaţii în care a fost
complementară au fost aplicate standard conform
demonstrată evoluţia favorabilă a pacientului cu colică
ghidurilor în vigoare în funcţie de stadiul sepsei, de tipul
litiazică febrilă şi în absenţa manevrelor invazive de
de infecţie suspicionat (comunitară sau nozocomială) şi
dezobstrucţie a tractului urinar superior [2,7,8].
de tratamentele antibiotice anterioare. Modalitatea de
drenaj urinar de primă intenţie în litiaza renoureterală
Obiective
infectată utilizată în clinica noastră este drenajul ureteral
intern în analgosedare, iar în caz de eşec, nefrostomia
Obiectivul acestui studiu este de a evalua în mod
percutanată ecoghidată în anestezie locală.
independent şi în asociere parametrii clinici şi
Din studiu au fost excluşi pacienţii la care din
bioumorali în vederea stabilirii eventualei valori
diverse motive nu s-a respectat protocolul standard de
predictive pentru necesitatea dezobstrucţiei urinare la
diagnostic şi tratament, dar şi pacienţii la care nu a fost
pacienţii cu colică renală febrilă de natura litiazică. De
obiectivată natura litiazică a suferinţei.
asemenea ne propunem evaluarea comparativă a
Datele numerice sunt fie continue, fie discrete.
agenţilor patogeni izolaţi şi a susceptibilităţii acestora la
Variabilele discrete au fost caracterizate prin frecvenţă
antibiotice.
(număr şi procent). Valorile continue au fost prezentate
ca şi medii +/- derivaţia standard (SD). Comparaţia
Material şi metodă
între două grupuri a fost efectuată utilizând testul
Student pentru variabile continue cu distribuiţie
Studiul este de tip prospectiv şi include toţi pacienţii
normală şi testul pentru variabile categoriale. Diferenţa
cu litiază renoureterală şi colică febrilă (peste 38°C) care
între categorii, în caz de mai mult de două categorii, a
s-au prezentat la Compartimentul de Primire Urgenţe
fost testată folosind metoda Kruskal-Wallis sau ANOVA.
din cadrul Spitalului Clinic Municipal Cluj în perioada
Valorile p<0,05 au fost considerate statistic semnificative.
1 aprilie
2010-31 decembrie
2012. Protocolul de
Am folosit pentru analiza statistică programul MedCalc®
diagnostic este standard şi cuprinde: anamneza,
9.3.9.0.
antecedentele personale patologice, examenul obiectiv,
ecografia, radiografia renovezicală simplă şi/sau
Rezultate
computer tomografia, analize de laborator (glicemie,
funcţie
renală,
hepatică,
hemoleucogramă,
În perioada
2010-2012 au fost internaţi
142
coagulogramă, sumar de urină, urocultură). Probele
pacienţi pentru colică renală febrilă (peste 38°C) prin
biologice au fost recoltate de personal calificat şi
obstacol litiazic, dintre aceştia 99 (66,9%) au fost femei
prelucrate în laboratorul acreditat al spitalului.
şi
47 bărbaţi (33,1%). Vârsta medie a fost de 51 ani.
Parametrii clinici care urmează a fi evaluaţi sunt:
Caracteristicile pacienţilor la internare sunt sumarizate
vârsta, sexul, stadiul urosepsei la internare, diabet
în Tabelul I.
zaharat, neoplazii active, dimensiunile şi localizarea
Un număr de 56 de pacienți (40%) au prezentat
calculului, gradul hidronefrozei, manevre urologice
litiază sub 4 mm iar 84 de pacienți (60%) peste 4 mm.
asupra tractului urinar.
Aproximativ o treime dintre pacienţi
(32,4%) au
Parametrii clinici şi bioumorali care au fost analizaţi
eliminat spontan fragmentul litiazic, pentru restul fiind
în dinamică (la prezentare, la 12h, 24h şi 48h), dar şi
necesară o manevră de dezobstrucţie urinară astfel: în 82
corelat cu momentul dezobstrucţiei dacă aceasta a
de cazuri (57,7%) s-a montat endoscopic stent ureteral,
existat, sunt: temperatura, pulsul, tensiunea arterială, nr.
iar în
14 cazuri
(9,9%) s-a montat nefrostomie
de leucocite şi procentul neutrofilelor, examenul sumar
percutană.
de urină şi urocultura şi funcţia renală precum şi stadiul
Drenajul urinar s-a asociat semnificativ statistic cu
sepsei.
localizarea şi dimensiunea calculului (p<0,0001), gradul
De asemenea au fost notate modalitatea de drenaj
hidronefrozei (p<0,0001), severitatea sepsei (p<0,0001),
urinar (pasaj spontan, stent ureteral JJ sau nefrostomă)
valoarea creatininei serice (p=0,0037) şi cu urocultura
82
Lăpuşan et al
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
Original articles
Tabel I. Caracteristicile pacienţilor la internare
Medie, DS,
Variabila
%
Vârsta
51,16±16,17
Sex:
F (nr, %)
95 (66,9)
M (nr, %)
47 (33,1)
Creatinina:
<1,4 (nr, %)
106 (74,6)
>1,4 (nr, %)
36 (25,1)
Stadiul sepsei:
SIRS
111 (78,1)
Sepsis
29 (20,4)
Sepsis sever
2 (1,4)
Leucociturie:
Absent
43 (30,3)
Prezent
99 (69,7)
Nitriți:
Absent
106 (74,7)
Prezent
36 (25,3)
Hematurie:
Absent
34 (23,9)
Figura 1. Localizarea calculilor şi procedura
Prezent
108 (76,1)
Urocultură:
negativă
78 (54,9)
germeni simpli
41 (28,9)
germeni multirezistenți
13 (9,1)
ESBL
10 (7,1)
Ph urinar
5,59±1,17
Leucocite:
<4000
5 (3,5)
4000-10000
51 (35,9)
10000-20000
69 (48,5)
20000
17 (12,1)
Trombocite:
<100000
9 (6,5)
100000-400000
118 (83,0)
>400000
15 (10,5)
Localizare calcul:
Bazinetal
30 (21,4)
Lombar
45 (32,1)
Iliac
34 (23,3)
Juxtavezical
31 (22,1)
Dimensiune calcul:
<0,4mm
56 (40)
Figura 2. Locaţia calculilor şi gradul hidronefrozei
>0,4mm
84 (60)
Procedură efectuată:
Pasaj spontan
46 (32,4)
Stent
82 (57,7)
Nefrostomă
14 (9,9)
de la internare au constituit criteriile de dezobstrucţie
Zile spitalizare
4,13±2,7
urinară de urgenţă în majoritatea cazurilor. La pacienţii
Diabet asociat:
Nu
98 (69)
internaţi cu semne clinice de sepsis şi sepsis sever,
Da
44 (31)
dezobstrucţia s-a efectuat în primele
6 ore de la
Neoplazie asociată:
Nu
130 (91,5)
prezentare. La pacienţii cu SIRS drenajul urinar s-a
Da
12 (8,5)
efectuat în medie la 24 ore (12-48 ore) de la internare.
Nu am înregistrat niciun deces.
Două cazuri au necesitat intervenţii chirurgicale
(p=0,0087). Au fost înregistrate 46 de cazuri de pasaj
deschise, ureterolitotomie şi respectiv pielolitotomie,
spontan al calculului, majoritatea lor de mici dimensiuni
efectuate în urgenţă din cauza complicaţiilor apărute
(41 de cazuri - 89,13%) şi cu localizare pelvină (40
după tentativa eşuată de stentare ureterală. La cele 94 de
cazuri - 86,95%), Figura 1.
cazuri la care s-a efectuat dezobstrucţia ureterală cu stent
Din punct de vedere al stadiului sepsei, majoritatea
sau nefrostomă, intervenţia curativă s-a efectuat
pacienţilor s-au prezentat cu SIRS, doar 31 pacienţi
programat la 14-21 zile după remisia procesului septic.
(21,83%) au fost cu sepsis, din care 2 cu sepsis sever.
Localizarea calculilor s-a asociat semnificativ statistic
Persistenţa febrei, leucocitozei şi hidronefrozei la 12 ore
cu gradul hidronefrozei (p=0,0001), gradul de dilatare
The Therapeutic Approach in Febrile Lithiasic Renal Colic-Single Center Experience
83
Original articles
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
Tabel 2. Rezultate bacteriologice la urocultură
An/germene
2010 (37 pac/16 inf)
2011 (44 pac/17 inf)
2012 (61 pac/31 inf)
Gram negativi total
11
15
23
G- multirezistent
-
2
6
G- ESBL
1
4
5
Gram pozitivi total
5
2
8
G+ multirezistent
1
-
4
pielocaliceală cel mai important fiind pentru calculii
obstructivă la care s-a efectuat drenaj urinar, indică o
lombari, apoi pentru cei iliaci, pelvini şi bazinetali,
medie de 3 zile (0-38) de la debutul afecţiunii până în
Figura 2.
momentul intervenţiei urologice [10]. Tipul drenajului
Dimensiunea calculilor de peste 4 mm s-a asociat
urinar: stent sau nefrostomă este încă controversat; în
semnificativ statistic cu prezenţa de leucocite în urină
SUA şi de către Asociaţia Europeană de Urologie este
(p=0,02) şi urocultură pozitivă
(p=0,04), dar şi cu
preferat drenajul ureteral [9,11], în timp ce în Marea
prezenţa hidronefrozei de grad II (p=0,001).
Britanie este agreată nefrostomia percutanată în
Deşi la internare, în baza examenului sumar de
obstrucţia ureterală însoţită de sepsis [12].
urină, infecţia a fost suspectată la
99 de pacienţi
Sammon şi colab. evidenţiază recent că litiaza
(69,7%), obiectivarea prin urocultură a germenilor
urinară are incidenţă mai mare la bărbaţi, dar asocierea
implicaţi în apariţia procesului septic s-a făcut în 64 de
litiazei cu infecţia este mai frecventă la femei, la acestea
cazuri
(45,07%). Dintre aceştia, majoritatea au fost
dublându-se practic incidenţa litiazei infectate între
germeni Gram negativi, 49 de cazuri(76,56%), cel mai
1999-2009. Acelaşi studiu indică faptul că dezobstrucţia
frecvent implicat fiind E. Coli 35 cazuri (71,42%). Pe
de urgenţă este mai frecventă la femei care sunt mai
lotul studiat am înregistrat
10 cazuri cu germeni
predispuse în a dezvolta sepsă comparativ cu bărbaţii,
producători de ESBL şi
13 cazuri de germeni
mortalitatea fiind însă similară [6].
multirezistenţi. Se remarcă trendul ascendent al acestor
În ceea ce privesc modalităţile de tratament ale
infecţii pe parcursul celor
3 ani. În Tabelul II sunt
calculilor ureterali în funcţie de localizare şi dimensiuni,
prezentate rezultatele bacteriologice obţinute.
mai multe studii arată o rată crescută (până la 80%) a
Pe lotul studiat nu s-a obținut o corelație
pasajului spontan pentru calculii sub 4 mm situaţi la
semnificativă statistic între procedură și sex sau vârstă.
nivelul ureterului distal, în timp ce la aceleaşi
În ceea ce priveşte durata spitalizării, aceasta s-a
dimensiuni, eliminarea spontană a calculilor ureterali
corelat semnificativ statistic cu dimensiunea calculului
proximali se produce în maxim 50% din cazuri, fără
(p<0,001), cu localizarea calculului (p=0,001), dar şi cu
însă a preciza intervalul de timp pâna la expulzie. Aceste
gradul hidronefrozei (p<0,001) şi cu tipul de procedură
procente scad însă odată cu creşterea dimensiunilor
(p<0,0001).
calculilor ureterali [11-15]. În situaţia asocierii sepsei,
de cele mai multe ori nu se poate aştepta pasajul spontan
Discuţii
al calculului, chiar dacă acesta este de mici dimensiuni,
fiind necesare manevre invazive de deblocare a căilor
În absenţa unui marker real, diagnosticul sepsei se
urinare, cu toate riscurile pe care acestea le presupun. Pe
face în continuare doar pe criterii clinice nespecifice,
lotul studiat au fost 14 cazuri la care s-a montat stent
unele dintre acestea putând fi determinate atât de sepsă
pentru calculi sub 4 mm.
cât şi de durerea acută din colica renală. Colica febrilă
Angulo şi colab. au concluzionat, în urma unui
este o urgenţă urologică, însă momentul optim şi tipul
studiu prospectiv pe 110 pacienţi cu colică renală prin
dezobstrucţiei nu sunt încă statuate
[4,11].
litiază reno-ureterală, că proteina C reactivă este un
Dezobstrucţia urinară la pacientul septic trebuie facută
parametru valoros în stabilirea deciziei de dezobstrucţie
în cel mai puţin invaziv mod [1,2,4]. Recent, la pacienţii
urinară la pacienţii cu colică litiazică, mai important
cu litiază reno-ureterală şi infecţie, Sammon şi colab. au
decât leucocitoza, sau nivelul seric al creatininei [16].
evaluat la 28,5% pacienţii care necesită dezobstrucţie
Din punct de vedere al rezultatelor bacteriologice,
urinară în prima zi de internare şi faptul că dintre aceştia
evidenţierea agentului patogen în urocultură a fost
70,1% erau femei [6]. Rezultatele recent publicate de
posibilă doar în 45,07% din cazuri, procent mai mic
Yamamoto şi colab., pe un lot de 98 de pacienţi cu PNA
decât cel pentru sepsă în general
[1,3], una dintre
84
Lăpuşan et al
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
Original articles
explicaţii fiind existenţa unui obstacol urinar complet
3.
Calandra T, Cohen J. International Sepsis Forum
cu stază purulentă suprajacentă, care nu a putut fi
Definition of Infection in the ICU Consensus Conference.
obiectivată nici după dezobstrucţie întrucât pacientul
Te international sepsis forum consensus conference
era deja cu tratament antibiotic [4].
on definitions of infection in the intensive care unit.
Schmudermaier şi colab., într-un studiu pe 6 ani au
Crit Care Med 2005;33:1538-48.
evidenţiat o creştere semnificativă a rezistenţei la
4.
Coman I, Secasan I, Feciche B, et al. Infectiile tractului
antibioticele standard în infecţiile urinare cu E. Coli, în
urinar în Sinescu I, Gluck G, et al. Tratat de Urologie,
schimb nu relevă creşterea rezistenţei tulpinilor
ediţia I, Editura Medicală, Bucureşti, 2008:875-932.
producătoare de ESBL [17]. În 2010, Hoban şi colab.
5.
Naber KG, Schaeffer AJ, Heyns CF, Matsumoto T,
constată o creştere a rezistenţei bacililor Gram negativi
Shoskes DA, Bjerklund Johansen TE. International
izolaţi la cazurile cu infecţii nosocomiale, fapt care
Consultation on Urogenital Infections. Stockholm,
complică selecţia empirică a antibioticelor pentru
Sweden, March 2009 Urogenital Infections, EAU,
cazurile la care se suspectează acest tip de infecţie
edition 2010.
[18,19]. În 2008, Souli şi colab. evidenţiază o creştere a
6.
Sammon JD, Ghani KR, Karakiewicz PI. Temporal
incidenţei Enterobacteriaceelor cu rezistenţă combinată
Trends, Practice Patterns, and Treatment Outcomes for
la asocierea beta-lactamine/inhibitori de beta-lactamaze,
Infected Upper Urinary Tract Stones in the United
cât şi la carbapenemi [19,20].
States. Eur Urol 2012;25. Available from URL: http://
Limitele acestui studiu sunt date de stabilirea valorii
limită de 4 mm pentru calculii la care se aşteaptă pasajul
S0302283812011037.
spontan, deşi în literatură se citează eliminări spontane
7.
Angulo JC, Gaspar MJ, Rodríguez N, García-Tello A,
şi la calculi de 5-7mm, până la 1cm. Pe lotul studiat am
Torres G, Núñez C. Te value of C-reactive protein
avut 6 pacienţi cu calculi peste 4 mm eliminaţi spontan.
determination in patients with renal colic to decide
O altă limitare a studiului este aceea că nu sunt
urgent urinary diversion. Urology 2010;76:301-6.
comparate datele obţinute la pacienţii cu colică febrilă,
8.
Matlaga BR. How Do We Manage Infected, Obstructed
cu cele ale pacienţilor cu colică renală şi infecţie, dar
Hydronephrosis? Eur Urol 2012;16. Available from
care nu asociază semnele clinice de sepsă.
pii/S0302283812012316.
Concluzii
9.
Ghani KR, Sammon JD, Trinh QD. Reply from
Authors re: Brian R. Matlaga. How Do We Manage
În absenţa unui marker real al sepsei, colica febrilă
Infected, Obstructed Hydronephrosis? Eur Urol. 2012 In
ramâne o urgenţă urologică în care alături de măsurile
de resuscitare este necesară dezobstrucţia tractului
com/science/article/pii/S0302283812013309.
urinar. Remisia fenomenelor septice în primele ore de la
10.
Yamamoto Y, Fujita K, Nakazawa S. Clinical
iniţierea terapiei de resuscitare poate fi urmată de pasajul
characteristics and risk factors for septic shock in patients
spontan al calculului mai ales dacă acesta este cu
receiving emergency drainage for acute pyelonephritis with
localizare joasă şi de mici dimensiuni. Aceste situaţii însă
upper urinary tract calculi. BMC Urol 2012;13:12:4.
necesită o monitorizare atentă şi drenaj urinar dacă
11.
Türk C, Knoll T, Petrik A, Sarica K, Straub M, Seitz
parametrii clinici şi bioumorali o impun. Incidenţa în
C. Guidelines on urolithiasis. European Association of
creştere a germenilor multirezistenţi impune reanalizarea
protocoalelor locale de antibioterapie în concordanţă cu
org/gls/pdf/20_Urolithiasis_LR%20March%20
susceptibilitatea germenilor izolaţi.
13%202012.pdf.
12.
Lynch M, Anson K, Patel U. Percutaneous nephrostomy
and ureteric stent insertion for acute renal deobstruction.
Referinţe
Consensus based guidelines. Br J Med Surg Urol
2008;1:120-5.
1. European Association of Urology, Sepsis Syndrome in
13.
Preminger GM, Tiselius HG, Assimos DG,et al.
Urology
(Urosepsis), Guidelines edition
2012.
EAU/AUA Nephrolithiasis Guideline Panel.
2007
guideline for the management of ureteral calculi. J Urol
pdf/17_Urological%20infections_LR%20II.pdf
2007;178:2418-34.
2. Wagenlehner FM, Pilatz A, Weidner W. Urosepsis-
14.
Tseng TY, Stoller ML. Medical and medical/urologic
from the view of the urologist. Int J Antimicrob Agents
approaches in acute and chronic urologic stone disease.
2011;38 Suppl:51-7.
Med Clin North Am 2011;95:169-77.
The Therapeutic Approach in Febrile Lithiasic Renal Colic-Single Center Experience
85
Original articles
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
15. Graham A, Luber S, Wolfson AB. Urolithiasis in the
imipenem, and other antimicrobial agents: data from
emergency department. Emerg Med Clin North Am
the Study for Monitoring Antimicrobial Resistance
2011;29:519-38.
Trends 2002 to 2007. Diagn Microbiol Infect Dis
16. Angulo JC, Gaspar MJ, Rodríguez N, García-Tello A,
2010;66:78-86.
Torres G, Núñez C. Te value of C-reactive protein
19. Hoban DJ, Nicolle LE, Hawser S, Bouchillon S,
determination in patients with renal colic to decide
Badal R. Antimicrobial susceptibility of global inpatient
urgent urinary diversion. Urology 2010;76:301-6.
urinary tract isolates of Escherichia coli: results from the
17. Schmudermaier M, Lunacek A, Koenig U, et al.
Study for Monitoring Antimicrobial Resistance Trends
Trends of Increasing Resistance of E. Coli and Non-
(SMART) program:
2009-2010. Diagn Microbiol
Significant Changes in Extended Spectrum Beta-
Infect Dis 2011;70:507-11.
Lactamase (ESBL) E. Coli in Urinary Tract Infections.
20. Souli M, Galani I, Giamarellou H. Emergence of
Urology 2011:S225.
extensively drug-resistant and pandrug-resistant Gram-
18. Hoban DJ, Bouchillon SK, Hawser SP, Badal RE.
negative bacilli in Europe. Euro Surveill
2008;13.
Trends in the frequency of multiple drug-resistant
Enterobacteriaceae and their susceptibility to ertapenem,
org/ViewArticle.aspx?ArticleId=19045.
86
Lăpuşan et al
Original articles
ATITUDINEA PĂRINŢILOR FAŢĂ DE EFICACITATEA EDUCAŢIEI
SEXUALE ÎN ŞCOLI, ÎN SOCIETATEA ARABĂ DIN ISRAEL
Joubran Samia1, Marcus Ohad2, Iancu Iulian3,8,Tova Hartman4, Abraham Weizman5,8, Rath-Wolfson Lea6,8,
Ram Edward7,8
1Facultatea de Medicină Bruce Rappaport, Institutul TehnologicTechnion şi Centrul Medical Emek, 2Departamentul de
Psihologie, Colegiul Valea Yezreel, 3,8Clinica de Sănătate Mentală Yavne, 4Departamentul de Educaţie şi al Genului Bar-
Ilan, Universitatea Israel, 5,8Centrul de Sănătate Mentală Geha, Petah Tikva, Israel, 6,8Departamentul de Patologie,
Spitalul Hasharon, Centrul Medical Rabin, 7,8Divizia de Chirurgie Generală, Spitalul Hasharon, Centrul Medical
Rabin, 8Facultatea de Medicină Sackler, Universitatea Tel Aviv
Adresa pentru corespondenţă:
Edward Ram
Division of General Surgery, Rabin Medical Center- Campus Golda
Petach Tiqva Keren Kaiemet St.7
Tel: 972-3-9372323, Fax: 972-3-9372401
E-mail: edwardrm@netvision.net.il
Primit: 13.12.2012
Acceptat: 15.02.2013
Med Con March 2013, Vol 8, No 1, 87-94
Rezumat
musulmani) şi că majoritatea părinţilor cred că astăzi
educaţia sexuală este mai bună decât în trecut (în special
Educaţia sexuală în Israel, în general şi în sectorul
în rândul părinţilor creştini).
arab în special, nu a beneficiat de aproape niciun studiu.
Credem că o mare influenţă asupra părinţilor o au
Studiul nostru a avut ca şi scop de a determina ce cred
comunitatea arabă şi cultura mediteraneană, în care
parinţii israeliano-arabi despre educaţia sexuală pe care
actul sexual şi educaţia sexuală nu sunt probleme triviale,
copii lor o primesc la şcoală, în general şi separat între
deşi ele vor deveni mai moderne. De asemenea am ajuns
părinţii musulmani şi creştini.
la concluzia că, arabii creştini înclină mai mult spre
Pentru a aborda această problemă, celor 797 de
modernizare şi spre sfârşitul individualist al
participanţi le-au fost adresate cinci întrebări dintr-un
continuumului decât arabii musulmani, care în general
sondaj utilizat anterior de către Blendon şi colab.
sunt mai strict colectivişti.
Rezultatele noastre au aratat ca majoritatea părinţilor
Cuvinte cheie: atitudini parentale, act sexual,
(de ambele confesiuni, dar mai ales creştină) cred că
sectorul arab în Israel, musulmani şi creştini
educaţia sexuală este foarte importantă şi că influenţează
în mare măsură evitarea bolilor cu transmitere sexuală,
Introducere
evitarea sarcinilor nedorite, amânarea relaţiilor sexuale
până la căsătorie şi luarea deciziei privind actul sexual,
Cu toţii suntem fiinţe sexuale umane. De la naştere,
având o influenţă doar parţială asupra iniţierii actului
dar în special în timpul adolescenţei, sentimentele
sexual. În plus, am constatat că majoritatea părinţilor
sexuale se schimbă şi se intensifică. Aceste sentimente
cred că profesorii de educaţie sexuală nu au o pregătire
sexuale pot adăuga o dimensiune vitală vieţii
suficientă, că educaţia sexuală este doar parţial
adolescenţilor, dimensiune care ar putea avea elemente
compatibilă cu valorile lor (în special în rândul părinţilor
pozitive. Ar putea fi acel sentiment minunat şi intens de
Parent’s Attitude Toward the Effectiveness of Sexual Education in Schools in the Arab Society in Israel
87
Original articles
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
a fi atras de altcineva, precum şi oportunitatea de
interpersonală, pot influenţa în sala de clasă atât
împlinire care vine dintr-o relaţie intimă cu o altă
curriculum-ul explicit, cât şi cel ascuns [15].
persoană. Aceste elemente pozitive nu ar trebui să fie
Cadrele didactice din New Brunswick au identificat
uitate sau ignorate [1].
reacţiile anticipate ale părinţilor cu privire la includerea
Educaţia pentru sănătate sexuală este un subiect
unor teme specifice, ca fiind cel mai mare obstacol în
controversat, care probabil scoate
„scântei” într-o
calea dorinţei lor de a preda educaţia pentru sănătate
dezbatere ca niciun alt subiect. Administratorii şcolilor
sexuală [16].
au identificat teama părinţilor sau opoziţia comunităţii
Israelul este o resursă valoroasă pentru a furniza o
ca fiind bariere majore în furnizarea educaţiei pentru
abordare multireligioasă la diverse probleme. El
sănătate sexuală [2,3].
reprezintă o varietate de religii, grupuri etnice, culturi şi
Şcoala este singura instituţie în contact regulat cu o
tradiţii. Statul Israel are aproximativ 7,4 milioane de
proporţie considerabilă a populaţei de adolescenţi [4],
locuitori. Caracteristica cea mai importantă a populaţiei
cu participarea a aproape tuturor tinerilor înainte de
Israelului este diversitatea sa ridicată. Pe lângă diviziunea
iniţierea comportamentului sexual riscant [5].
principală a locuitorilor ţării în evrei
(80%) şi arabi
Se pare că există un consens în creştere că şcoala
(20%), există mult mai multe subdiviziuni
(Biroul
poate juca un rol important în furnizarea bazei de
Central de Statistică din Israel, 2009). Sunt de remarcat
cunoştinţe tinerilor, care ar putea să le permită să ia o
statisticile care au în vedere faptul că musulmanii
decizie informată şi să-i ajute să-şi contureze un stil de
reprezintă aproximativ 15% din populaţia israeliană, în
viaţă sănătos [6].
timp ce creştinii cuprind aproximativ
2% [17].
Părinţii pot avea o influenţă importantă asupra
Diferenţele culturale între evreii şi arabii din Israel
comportamentelor sexuale ale copiilor. Studiile indică
conduc la valorile de bază ale fiecărui sector, datorită
faptul că relaţiile de susţinere părinte-copil precum şi
apartenenţei culturale derivate de la cele patru origini:
monitorizarea şi supravegherea părintească sunt asociate
etnie, limbă, religie, naţionalitate; populaţia israeliană
cu întârzierea activităţii sexuale în rândul copiilor [7]; în
creştină şi cea musulmană se caracterizează prin diferenţe
fapt, părinţii nu sunt prea mult implicaţi în discuţia
substanţiale de valori, credinţe, alcătuirea familiei şi
problemelor legate de sex, adolescenţii exprimându-şi
modele de comportament sexual (Biroul Central de
ferm dorinţa ca părinţii lor să le poată fi ghid în
Statistică din Israel, 2009).
cunoştinţele despre sex [8,9]. Ei înţeleg această situaţie
Diferenţele subculturale există în cultura arabă între
şi sunt conştienţi de limitele lor, astfel încât speră să
arabii creştini şi cei musulmani. Arabii creştini înclină
obţină asistenţă din partea profesioniştilor, pentru a
spre modernizare şi spre sfârşitul individualist al
dobândi abilităţi de a se angaja în educaţia parentală
continuumului mai mult decât musulmanii arabi, care
privind sexualitatea [10].
sunt, în general, mult mai strict colectivişti. În formarea
Discuţia despre sexualitate în casă este o componentă
generală au realizări academice superioare faţă de omologii
importantă a educaţiei elevilor în general, sănătatea
lor arabi musulmani; mai multe femei creştine studiază în
sexuală şi educaţia pentru sănătate sexuală în şcoală
învăţământul superior decât femeile musulmane, iar
putând uşura discuţia despre sexualitate a părinţilor cu
şcolile creştine sunt considerate a fi printre cele mai bune
copii lor [11,12].
[18]. Diferenţele apar de asemenea şi în populaţia arabă în
Cei mai mulţi părinţi cred că părinţii şi şcolile ar
sine, în conformitate cu diferenţele de gen şi de variaţie
trebui să împartă responsabilitatea pentru educaţia
subculturală. Educaţia fiicelor este mai strictă decât cea a
pentru sănătate sexuală. De exemplu, McKay şi colab.
fiilor, care au o expunere mai mare la influenţele de
[13] au constatat că majoritatea părinţilor au identificat
modernizare în afara casei părinteşti şi care primesc mai
părinţii
(88%), profesioniştii din domeniul sănătăţii
multă autonomie din partea părinţilor [19].
(88%) şi profesorii (77%), ca oamenii adecvaţi pentru a
Cultura arabă în Israel se distinge prin orientarea sa
furniza educaţie pentru sănătate sexuală în şcoală şi
tradiţională, omogenitate şi orientare colectivistă, în
comunitate.
ciuda trecerii ei printrun proces de modernizare
Multe autorităţi de mult timp au fost de acord că
[20,21,22].
cel mai important factor de succes în implementarea
Oamenii dintr-o societate colectivistă tind să se
programelor de învăţământ privind sexualitatea este un
comporte în conformitate cu obiectivele colective
profesor la clasă, bine calificat şi cu dorinţă de a o face
comune preferate. Ei tind să-şi expună relaţiile intime
[14].
între ei şi să le ţină la distanţă faţă de străini şi outsideri.
Caracteristicile cadrelor didactice, atitudinea,
Armonia colectivă este valorizată mai presus de toate
concepţia de sine şi dispoziţia intelectuală şi
[23].
88
Joubran et al
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
Original articles
Această normă determină în educarea copiilor
definit ca laici sau tradiţionalişti, iar 252 s-au definit ca
dezvoltarea unui
„locus” de control exterior şi
religioşi sau foarte religioşi.
conformitatea cu o imagine acceptată, minimalizând în
Chestionare
acelaşi timp autocritica (Barakat, 1993). De exemplu,
Studiul s-a bazat pe un chestionar elaborat de Blendon
statusul familial şi onoarea au dus studenţii arabi
(2004), care a constat din 42 de întrebări cu răspunsuri
americani la ignorarea consilierului lor şcolar
multiple, examinând atitudinea părintelui faţă de educaţia
(Courtland, 1997).
sexuală. Chestionarul a fost tradus în arabă
(dublă
Societatea arabă este încă considerată colectivistă,
traducere) şi a fost verificat de un specialist în limba arabă.
iar adolescenţii săi continuă să dea importanţă mai mare
Din acest chestionar au fost utilizate 3 întrebări.
apartenenţei la un colectiv mai mare, în dauna
Întrebările care au ghidat această cercetare sunt:
planificării viitorului lor individual [6,24].
(1) Este important ca educaţia sexuală să facă parte
Mediul educaţional israelian conţine două culturi
din programa şcolară?
diferite, cu sisteme separate de învăţământ; profesorul
(2) Cum influenţează educaţia sexuală din şcoli
arab primeşte educaţia primară prin învăţământul
abilitatea copiilor de a ...
secundar, în contextul colectivist al sectorului
A. iniţia un act sexual?
educaţional arab, care include musulmani şi creştini. El
B. evita bolile cu transmitere sexuală?
studiază în limba maternă, câştigând unele experienţe
C. evita sarcini nedorite?
anterioare prin cultura occidentală israeliană [25].
D. amâna contactul sexual până la căsătorie?
Ministerul Educaţiei din Israel este responsabil
E. lua o decizie bună despre actul sexual?
pentru educaţia sexuală în şcoli, astfel încât ministerul
(3) Profesorii de educaţie sexuală au suficientă pregătire?
are numeroase programe de educaţie sexuală pentru
(4) Cât de mult educaţia sexuală în şcoală este
fiecare sector populaţional din Israel.
compatibilă cu valorile tale?
În 1996 Ministerul Educaţiei a publicat primul
(5) Cât de bună este astăzi educaţia sexuală în
program de educaţie sexuală pentru cetăţenii arabi.
şcoală, comparativ cu cea din trecut?
Acest program prezintă educaţia vieţii de familie şi
Procedura
educaţia sexuală vizând împărtăşirea cunoştinţelor,
Chestionarele au fost puse la dispoziţia
aptitudinilor, precum şi înţelegerea modului de abordare
administratorilor şcolilor din întreaga ţară, care le-au
a subiectul despre sex. Programul are 12 capitole de
trimis aleatoriu părinţilor din şcolile lor. Chestionarele
subiecte teoretice şi activităţi care includ aceste subiecte:
completate anonim au fost trimise înapoi la anchetatori
educaţia sexuală şi educaţia pentru o viaţă bună de
prin e-mail. Din 1000 chestionare au fost returnate 797,
familie, adolescenţă, relaţia dintre părinţi şi adolescenţi,
rata de răspuns de 79,7% reprezintând o rată de răspuns
propriul corp, luarea deciziilor, prietenie, prejudecăţi,
ridicată pentru comunitatea arabă.
educaţie şi încredere în sine, presiunea celor din aceeaşi
generaţie, tradiţie şi obiceiuri, SIDA şi bolile cu
Rezultate
transmitere sexuală [26].
Programul de mai sus este conceput să înceapă în
În primul rând am vrut să ştim dacă este important
grădiniţă şi se termină în liceu, dar în realitate elevii
ca educaţia sexuală să facă parte din programa şcolară.
învaţă doar 45 de minute la nivelul şcolii elementare.
Am constatat că 81,1% dintre părinţi cred că este
Scopul acestui studiu este de a determina ce cred
foarte important ca educaţia sexuală să fie parte din
părinţii israeliano-arabi despre educaţia sexuală pe care o
programa şcolară, 16,6% cred că nu este important ca
primesc copii în şcoală, în general şi separat în rândul
educaţia sexuală să fie o parte a curriculum-ului şcolar şi
părinţilor musulmani şi creştini.
doar 2,3% cred că nu are deloc importanţă ca educaţia
sexuală să fie o parte din programa şcolară.
Metodologia de cercetare
A fost, de asemenea, o diferenţă semnificativă între
părinţii musulmani şi creştini în privinţa importanţei
Participanţii
educaţiei sexuale ca parte a programei şcolare
Participanţii au fost 797 părinţi israeliano-arabi din
[U(787)=71311,5, p<0,01], astfel, părinţii musulmani
întregul Israel, al căror interval de vârstă a fost între 20 şi
cred că educaţia sexuală care face parte din curriculum-
66 de ani (M=39). Printre ei au fost 371 creştini şi 426
ul şcolar (M=380,10) este mai puţin importantă decât
musulmani, 208 bărbaţi şi 589 femei, 533 locuind în
cred părinţii creştini (M=409,74).
oraşe şi 264 în zonele rurale sau sate; 483 cu studii
Am vrut să ştim cum educaţia sexuală în şcoală
academice şi 314 fără. În plus, 545 participanţi s-au
influenţează abilitatea copiilor de a iniţia relaţii sexuale,
Parent’s Attitude Toward the Effectiveness of Sexual Education in Schools in the Arab Society in Israel
89
Original articles
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
Tabel I. Procentul părinţilor care cred că este important ca
şcoală este foarte eficientă asupra abilităţii copiilor de a
educaţia sexuală să facă parte din programa şcolară, în
lua decizii bune privind actul sexual, 35,1% cred că este
general şi în funcţie de religie
parţial eficientă, 3,7% cred că nu este eficientă, iar 1,9%
sunt de părere că nu este deloc eficientă.
Procente generale
Nu a fost nicio diferenţă între părinţii musulmani şi
Creştin
Musulman
creştini în aprecierea eficacităţii educaţiei sexuale din
Foarte important - 81,1%
şcoală asupra abilităţii copiilor de a se angaja în relaţii
Nu este important - 16,6%
Deloc important - 2,3%
sexuale
[U(593)=43652,5, ns], de a evita bolile cu
Foarte important - 84,8%
Foarte important - 77,8%
Nu este important - 14,6%
Nu este important - 18,4%
Deloc important - 0,5%
Deloc important - 3,8%
Tabel II. Procentul părinţilor care cred că educaţia sexuală
***U(787)=71311,5
influenţează abilitatea copiilor de a angaja relaţii sexuale,
de a evita bolile cu transmitere sexuală, de a evita sarcinile
****p<0.05
***p<0.01
**p<0.005
*p<0.001
nedorite, de a amâna actul sexual până la căsătorie şi să ia
o decizie bună privind actul sexual
Educaţia sexuală în şcoală
influenţează abilitatea
copiilor de a …
iniţia actul sexual
foarte eficientă - 31,0%
eficientă parţial - 57,3%
neeficientă - 7,4%
deloc eficientă - 4,2%
evita bolile cu transmitere
foarte eficientă - 69,2%
sexuală
eficientă parţial - 27,7%
neeficientă - 2,6%
Figura 1. Procentul părinţilor care cred că este important ca
deloc eficientă - 0,5%
educaţia sexuală să facă parte din programa şcolară, în
evita o sarcină nedorită
foarte eficientă - 66,1%
general şi în funcţie de religie
eficientă parţial - 29,7%
neeficientă - 3,8%
deloc eficientă - 0,4%
amâna actul sexual până la
foarte eficientă - 51,7%
de a evita bolile cu transmitere sexuală şi sarcinile
căsătorie
eficientă parţial - 37,5%
nedorite, de a amâna actul sexual până la căsătorie şi să
neeficientă - 8,1%
ia o decizie adecvată despre actul sexual.
deloc eficientă - 2,7%
Am constatat că 31% dintre părinţi cred că educaţia
lua o decizie bună privind
foarte eficientă - 59,4%
sexuală în şcoală este foarte eficientă asupra iniţierii unui
actul sexual
eficientă parţial - 35,1%
contact sexual, 57% cred că este parţial eficientă, 7,4%
neeficientă - 3,7%
cred că nu este eficientă, iar 4,3% cred că nu este eficientă
deloc eficientă - 1,9%
deloc; 69,2 % dintre părinţi cred că educaţia sexuală în
şcoală este foarte eficientă asupra abilităţii copiilor de a
evita bolile cu transmitere sexuală, 27,7% cred că este
parţial eficientă, 2,6% cred că nu este eficientă, iar 0,5%
sunt de părere că nu este eficientă deloc; 66,1% din
părinţi cred că educaţia sexuală în şcoală este foarte
eficientă asupra abilităţii copiilor de a evita sarcini
nedorite, 29,7% cred că este parţial eficientă, 3,8% cred
că nu este eficientă, iar 0,4% sunt de părere că nu este
eficientă deloc;
51,7% dintre părinţi cred că educaţia
sexuală în şcoală este foarte eficientă asupra abilităţii
Figura 2. Procentul părinţilor care cred că educaţia sexuală
copiilor de a amâna actul sexual până la căsătorie, 37,5%
influenţează abilitatea copiilor de a iniţia relaţii sexuale, de
cred că este parţial eficientă, 8,1% cred că nu este eficientă,
a evita bolile cu transmitere sexuală, de a evita sarcinile
iar 2,7% sunt de părere că nu este eficientă deloc şi în
nedorite, de a amâna actul sexual până la căsătorie şi de a
sfârşit 59,4% dintre părinţi cred că educaţia sexuală în
lua decizia bună privind actul sexual
90
Joubran et al
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
Original articles
transmitere sexuală [U(773)=71,308, ns], de a evita sarcinile
A existat, de asemenea, o diferenţă semnificativă
nedorite [U(758)=70,864, ns], de a amâna actul sexual
între părinţii musulmani şi creştini în compatibilitatea
până la căsătorie
[U(766)=68,142, ns] şi pentru a lua
educaţiei sexuale din şcoală cu valorile lor
decizia bună asupra actului sexual [U(753)=68042,5, ns].
[U(635)=44650,5, p<0,01], astfel încât părinţii
Tabelul II şi Figura 2 rezumă rezultatele de mai sus.
musulmani cred că educaţia sexuală în şcoală este mai
Am întrebat părinţii, dacă cadrele didactice au
puţin compatibilă cu valorile lor (M=302,18) decât cred
suficientă pregătire privind educaţia sexuală?
părinţii creştini (M=336,59).
Am constatat că în timp ce 28,5% dintre părinţi
Tabelul III şi Figura 3 rezumă rezultatele de mai sus.
cred că profesorii de educaţie sexuală au suficientă
În cele din urmă, am întrebat: cât de bună este
pregătire, 71,5% dintre ei cred că profesorii de educaţie
astăzi educaţia sexuală în şcoală, comparativ cu educaţia
sexuală nu au suficientă pregătire.
sexuală din trecut?
Nu a fost nicio corelaţie semnificativă între religia
Am constatat că
70,9% dintre părinţi cred că
părinţilor şi credinţa lor cu privire la pregătirea suficientă
educaţia sexuală este astăzi mai bună decât în trecut,
a cadrelor didactice în educţia sexuală [2χ(1)=1.45, n.s.].
18,7% dintre părinţi cred că astăzi educaţia sexuală este
Am întrebat părinţii: cât de compatibilă este
aceeaşi ca şi în trecut şi doar 10,4% dintre părinţi cred
educaţia sexuală din şcoală cu valorile lor?
că educaţia sexuală astăzi este mai rea decât în trecut.
Am constatat că
28,2% dintre părinţi cred că
A fost, de asemenea, o diferenţă semnificativă între
educaţia sexuală în şcoală este foarte compatibilă cu
părinţii
musulmani şi creştini în evaluarea
valorile lor,
58,7% cred că este parţial compatibilă,
compatibilităţii educaţiei sexuale în şcoală cu valorile lor
9,6% cred că nu este compatibilă, iar 3,5% cred că nu
[U(635)=48,928, p<0,05], astfel încât părinţii musulmani
este deloc compatibilă.
cred că astăzi educaţia sexuală este mai bună decât în
Tabelul III. Procentul părinţilor care cred că educaţia
Tabelul IV. Procentul părinţilor despre ce cred că este
sexuală în şcoală este compatibilă cu valorile lor, în
educaţia sexuală în şcoală astăzi în comparaţie cu educaţia
general şi în funcţie de religie
sexuală din trecut, în general şi în funcţie de religie
Procent general
Procent general
Creştin
Musulman
Creştin
Musulman
Foarte compatibilă - 28,2%
Mai bună astăzi decât în trecut - 70,9%
Parţial compatibilă - 58,7%
Aceeaşi - 18,7%
Nu este compatibilă - 9,6%
Astăzi mai rea decât în trecut - 10,4%
Deloc compatibilă - 3,5%
Mai bună astăzi decât în
Mai bună astăzi decât în
Foarte compatibilă - 32,2%
Foarte compatibilă - 24,8%
trecut - 75,9%
trecut - 66,9%
Parţial compatibilă - 57,9%
Parţial compatibilă - 59,5%
Aceeaşi - 12,9%
Aceeaşi - 23,3%
Nu este compatibilă - 8,2%
Nu este compatibilă - 10,8%
Astăzi mai rea decât în
Astăzi mai rea decât în
Deloc compatibilă - 1,7%
Deloc compatibilă - 5,0%
trecut - 11,2%
trecut - 9,7%
*** U(635)=44650,5
****U(635)=48928
****p<0.05
***p<0.01
**p<0.005
*p<0.001
****p<0.05
***p<0.01
**p<0.005
*p<0.001
Figura 3. Procentul părinţilor care cred că educaţia sexuală în
Figura 4. Procentul părinţilor despre credinţa în educaţia
şcoală este compatibilă cu valorile lor, în general şi în funcţie
sexuală în şcoală astăzi, comparativ cu educaţia sexuală din
de religie
trecut, în general şi în funcţie de religie
Parent’s Attitude Toward the Effectiveness of Sexual Education in Schools in the Arab Society in Israel
91
Original articles
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
trecut (M=338,59) mai puţin decât cred părinţii creştini
abilităţilor de comunicare şi negociere, prin joc de rol
(M=313,92).
sau discuţii interactive [32]. Programele care încurajează
Tabelul IV şi Figura 4 sintetizează rezultatele de mai sus.
abstinenţa sunt cea mai bună opţiune pentru adolescenţi,
dar cele care oferă o discuţie privind prevenirea HIV şi
Discuţie
contracepţia pentru adolescenţii activi sexual, s-au
dovedit a întârzia iniţierea activităţii sexuale şi cresc
Educaţia este un proces structurat intenţionat de a
proporţia de adolescenţi activi sexual care au raportat
împărtăşi cunoştinţe şi abilităţi şi de a influenţa cursul
utilizarea de mijloace de control ale sarcinii
[33].
dezvoltării unui individ [27]. Educaţia sexuală permite
Programele care au legat programa de învăţământ de
oamenilor să dobândească cunoştinţe şi să dezvolte
accesul la servicii de sănătate a reproducerii şi intervenţii
abilităţi pe care le pot utiliza pentru a se proteja ei înşişi
cuprinzătoare bazate pe comunitate au înregistrat, de
şi pe alţii [28].
asemenea, reduceri ale ratelor de sarcină [34].
În studiul nostru cei mai mulţi dintre părinţi
Cei mai mulţi dintre părinţii din studiul acesta cred
consideră că este foarte important ca educaţia sexuală să
că educaţia sexuală în şcoală este parţial compatibilă cu
devină o parte a programei şcolare, existând, de
valorile lor, părinţii musulmani crezând că educaţia
asemenea, o diferenţă semnificativă între părinţii
sexuală în şcoală este mai puţin compatibilă cu valorile
musulmani şi creştini, pentru creştini includerea
lor decât cred părinţii creştini.
educaţiei sexuale în planul de învăţământ fiind mult mai
Mulţi arabi musulmani, părinţii şi chiar şi tinerii,
importantă decât pentru musulmani.
sunt foarte preocupaţi atât de metodele actuale de
Multe dintre aspectele psihosociale ale sexualităţii,
educaţie sexuală, cât şi de valorile pe care le poartă, o
cum ar fi atitudinile sexuale, au fost relativ neexplorate
parte din opoziţie bazându-se pe o neînţelegere sau pe o
în diverse grupuri etnice. Există motive să credem că
denaturare a practicilor actuale în domeniul educaţiei
grupurile etnice diferă în valorile sexuale, luând în
sexuale
[18]. Ashraf
[35] a susţinut că baza pentru
considerare factorii disparaţi culturali, politici, istorici,
educaţia sexuală în şcoli în sistemul secular este pur
socio-economici şi care influenţează sexualitatea în
fizică, fără nicio dimensiune spirituală sau morală.
fiecare grup [29]. Dintre cele 69% din şcolile publice
Arabii musulmani înclină mai mult spre modernizare şi
care furnizează la nivel de district educaţie sexuală, 14%
spre sfârşitul individualist al continuumului decât arabii
tratează abstinenţa ca o opţiune pentru adolescenţi,
musulmani, care sunt în general colectivişti mult mai
51% predau abstinenţa ca opţiunea preferată pentru
stricţi [18].
adolescenţi, dar permit discuţia despre contracepţie ca
Aproximativ 71% dintre părinţi în studiul nostru
un mijloc eficient de protecţie împotriva sarcinilor
cred că educaţia sexuală este astăzi mult mai bună decât
nedorite şi a bolilor cu transmitere sexuală şi mai mult
în trecut, musulmanii cred că educaţia sexuală astăzi este
de una din trei (35%) predau numai abstinenţa, cu
mai puţin bună decât în trecut, în contrast părinţii
interzicerea discuţiei despre contracepţie, sau limitarea
creştini cred că astăzi este mult mai bună.
la discutarea lipsei ei de eficacitate [30].
Profesorul arab primeşte educaţia primară prin
Religia joacă un rol important în socializare prin
învăţământul secundar, în contextul colectivist al
inocularea normelor la copii, a valorilor societăţii şi
sectorului educaţional arab, care include musulmani şi
furnizează ghiduri despre ceea ce este bine şi ce este
creştini. Ei studiază în limba maternă, câştigând unele
greşit în societate [31].
experienţe anterioare prin cultura occidentală israeliană
Toţi părinţii care au participat la acest studiu, de
[25]. Din cauză că profesorii în comunitatea arabă îşi
ambele religii, cred că educaţia sexuală în şcoală afectează
dobândesc educaţia în context colectivist, majoritatea
parţial capacitatea copiilor de a se angaja în relaţii
părinţilor care au participat la studiul nostru cred că
sexuale, cei mai mulţi dintre părinţi cred că educaţia
profesorii de educaţie sexuală nu au pregătirea adecvată.
sexuală în şcoală afectează mult abilitatea copiilor de a
evita bolile cu transmitere sexuală, sarcina nedorită,
Concluzie
luare unei decizii bune despre actul sexual şi să amâne
actul sexual până la căsătorie.
Scopul acestui studiu a fost de a determina ce cred
Programele doar despre abstinenţă nu au demonstrat
parinţii israeliano-arabi despre educaţia sexuală pe care o
rezultate de succes în ceea ce priveşte întârzierea iniţierii
primesc în şcoală copii, în general şi separat în rândul
activităţii sexuale, sau utilizarea de practici sexuale mai
părinţilor musulmani şi creştini.
sigure. Programele eficiente tind să ofere abilităţi
Am constatat că majoritatea părinţilor (de ambele
practice, cum ar fi exercitarea controlului şi creşterea
credinţe, dar mai ales creştinii) cred că educaţia sexuală
92
Joubran et al
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
Original articles
este foarte importantă şi că în mare măsură influenţează
Services Review, 1997;19,415-39. 24. Al-Haj M. Te
evitarea bolilor cu transmitere sexuală, evitarea sarcinii
Arab Teacher in Israel: Status, Questions, Expectations.
nedorite, amânarea actului sexual până la căsătorie şi în
Haifa, Israel: University of Haifa, Center for
luarea unei decizii bune despre actul sexual, având doar
Multiculturalism and Educational Research 1995.
parţial influenţă asupra iniţierii actului sexual. În plus,
6.
Seginer R. Adolescents facing the future: Cultural and
am constatat că majoritatea părinţilor cred că profesorii
socio-political perspectives. Youth and Society,
de educaţie sexuală nu au pregătire suficientă, că
1988;19:314-33.
educaţia sexuală este doar parţială compatibilă cu
7.
Miller BC, Benson B, Galbraith D. Family
valorile lor (în special în rândul părinţilor musulmani) şi
relationships and adolescent pregnancy risk: A research
că majoritatea părinţilor cred că educaţia sexuală de
synthesis. Developmental Review, 2001;21:1-38.
astăzi este mai bună decât în trecut (în special în rândul
8.
Fisher TD. Parent-child communication about sex and
părinţilor creştini).
young adolescents sexual knowledge and attitudes.
Noi credem că atât comunitatea arabă cât şi cultura
Adolescence 1986;2(83):517-28.
mediteraneană, în care actul sexual şi educaţia sexuală
9.
Warren C, Neer M. Family sex communication
nu sunt probleme triviale, au o mare influenţă asupra
orientation. Journal of Applied Communication
părinţilor, în pofida faptului că vor deveni mai moderne.
Research, 1986;14:86-107.
De asemenea, am ajuns la concluzia că arabii creştini
10.
Alter JS, Baxter S, Cook AT, Kirby D., Wilson P.
înclină mai mult spre modernizare şi spre sfârşitul
Teaching Parents to be the Primary Sex Educators of
individualist al continuumului decât arabii musulmani,
Teir Children. Bethesda, Md: Mathtech, 1982.
care sunt, în general, mult mai strict colectivişti.
11.
Berne LA, Patton W, Milton J, Hunt LYA, Wright S,
Cercetarea noastră este printre puţinele studii
Peppard J, Dodd J. A qualitative essessment of
efectuate în domeniul educaţiei sexuale în general şi în
Australian parents’ perceptions of sexuality education
societatea arabă în special. Aceasta este printre primele
and communication. Journal of Sex Education and
studii care examinează diferenţele dintre creştini şi
Terapy, 2000;25:161-8.
musulmani, precum şi printre primele care examinează
12.
Parcel GS, Coreil J. Parental evaluations of a sex
în profunzime subiectul educaţiei sexuale în societatea
education course for young adults. Journal of School
israeliano-arabă. Studiul nostru contribuie în mod
Health, 1985;55:9-12.
semnificativ la educaţia sexuală în societatea arabă în
13.
McKay A, Pietrusiak M, Holowaty P. Parents’opinions
general şi evidenţiază în special asemănările care există
and attitudes toward sexuality education in the schools.
în această societate.
Te Canadian Journal of Human Sexuality,
Mulţumiri: Societăţii pentru Dezvoltarea Cercetării
1998;7:139-45.
Academice Abhath pentru sprijinul şi ajutorul în
14.
Ryan IJ, Dunn PC. Sex education from prospective
desfăşurarea acestui studiu.
teachers’ view poses a dilemma. Journal of School
Health,
1979;49(10),573-5.20. Al-Haj M. Te
changing Arab kinship structure: Te effect of
Referinţe
modernization in an urban community. Economic
Developmental Cultural Change, 1988;36(2):237-58.
1. Kirby D, Short L, Collins J, Rugg D, Kolbe L, Howard
15.
Wenzlaff TL. Dispositions and portfolio development: Is
M, Miller B, Sonenstein F, Zabin L. School-based
there a connection? Education, 1998;118(4):564-9.
programs to reduce sexual risk behaviors: a review of
16.
Cohen JN, Byers ES, Sears HA, Weaver AD. New
effectiveness. Public Health Rep, 1994;109(3):339-60.
Brunswick Teachers’ Ideas About Sexual Health
2. Reis J, Seidl A. School administrators, parents, and sex
Education.
2001, Fredericton, New Brunswick:
education: A resolvable paradox? Adolescence,
University of New Brunswick, Department of
1989;24:639-45.
Psychology.
3. Scales P, Kirby D. Perceived barriers to sex education: A
17.
Trumbull CP. (Ed.) Britannica Book of the Year.
survey of professionals. Journal of Sex Research,
Chicago, 2001, Encyclopaedia Britanica.
1983:19:309-26.
18.
Swirski S. Education in Israel: Schooling for Inequality.
4. Zabin L, Hirsch M.
(). Evaluation of Pregnancy
1990,Tel-Aviv, Israel: Breirot.
Prevention Programs in the School Context.
1988,
19.
Jarrous-Absawy G. Relationships Between Parents and
Lexington, MA: Lexington Books.
Adolescents as a Function of Culture and Values.
5. Kirby D, Coyle K. School-based programs to reduce
Unpublished master’s thesis, University of Haifa,
sexual risk-taking behavior. Children and Youth
Israel, 1999.
Parent’s Attitude Toward the Effectiveness of Sexual Education in Schools in the Arab Society in Israel
93
Original articles
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
20.
Lehrer EL. Religion as a Determinant of Economic and
J. Maggs & K. Hurrelmann (eds.), Health Risks and
Demographic Behavior in the USA. Population
Developmental Transition During Adolescence,
Development Review, 2004;30(4):707-26.
Cambridge: University press, 1997,pp 110-35.
21.
Al-Haj M. Social research on family life styles among
29.
Amaro H, Navarro A, Conron K, Raj A, On C.
Arabs in Israel. Journal of Comparative Family
Cultural influences on women’s sexual health, in R. J.
Studies, 1989;20(2):175-95.
DiClemente & G. M. Wingood (Eds.), Women’s
22.
Florian V, Mikulincer M, Weller A. Does culture affect
Sexual and Reproductive Health, New York: Plenum,
perceived family dynamics? A comparison between Arab
2002,pp. 71-92.
and Jewish adolescents in Israel. Journal of Comparative
30.
Landry DJ, Kaeser L, Richards CL. Abstinence
Family Studies, 1993;24(2):189-201.
promotion and the provision of information about
23.
Triandis HC, McCusker C, Hui CH. Multimethod
contraception in public school district sexuality education
probes of individualism and collectivism. Journal of
policies. Family Plann Perspect, 1999;31:280-6.
Personality and Social Psychology, 1990;59:1006-20.
31.
Tornton A, Camburn D. Religious Commitment and
24.
St Leger L. Te opportunities and effectiveness of the
Adolescent Sexual Behavior and Attitudes. Journal of
health promoting primary school in improving child
Marriege Family, 1994;51(3):641-53.
health - a review of the claims and evidence. Health
32.
Frost JJ, Forrest JD. Understanding the impact of
Education Research, 1999:14,51-69.
effective teenage pregnancy prevention programs. Family
25.
Eilam B. Passing Trough a Western-Democratic
Plann Perspect, 1995;27:188-95.
Teacher Education: Te Case of Israeli Arab Teachers.
33.
Zabin LS, Hirsch MB, Streett R, et al. Te Baltimore
Teachers College Record, 2002;104:1656-701.
pregnancy prevention program for urban teenagers. How
26.
Israel Ministry of Education, 1996.
did it work? Family Plann Perspect, 1988;20,182-
27.
Schneewind KA, Socialization and Education:
7.35. Ashraf SA. Editorial: the Islamic concept of sex as
Teoretical perspective, in: Smelser NJ, Baltes PB (eds.),
the basis of sex education, Muslim Education Quarterly,
International Encyclopedia of Social and Behavioral
1996;13:1-3.
Sciences, Amsterdam: Elsvier 2001,pp 14507-13.
34.
Vincent ML, Clearie AF, Schluchter MD. Reducing
28.
Beyth-Marom R, Fischhoff B. Adolescents’ Decisions
adolescent pregnancy through school and community-
about Risks: A cognitive perspective, in: T. Schulenberg,
based education. JAMA, 1987;257:3382-6.
Traducere: dr Bumbuluţ Călin
94
Joubran et al
Original articles
SIMPTOMELE DEPRESIVE ŞI TULBURĂRILE MEMORIEI PACIENŢILOR
VÂRSTNICI
Popescu Cristina Maria1, Ghiuru Rodica2, Spiru Luiza3, Stroe Felicia4
1C.M.I. Mănăstirea Tudor Vladimirescu, judeţul Galaţi, 2Clinica a V-a Medicală de Geriatrie şi Gerontologie, Spitalul
C.F.R., Iaşi, Facultatea de Medicină şi Farmacie „Gr. T. Popa”, Iaşi, România, 3Facultatea de Medicină şi Farmacie
„Carol Davila”, Bucureşti, România, 4Institutul Naţional de Sănătate Publică, Bucureşti, România
Adresa pentru corespondenţă:
Dr. Cristina Maria Popescu,
1300, C.M.I. Mănăstirea Tudor Vladimirescu, 807295, judeţul Galaţi, România
Telefon: 0040766774026
E-mail: popescucristinamaria@yahoo.com
Primit: 05.01.2013
Acceptat: 15.02.2013
Med Con March 2013, Vol 8, No 1, 95-100
Rezumat
Concluzii: Rezultatele sugerează că persoanele
vârstnice cu distimie sau depresie severă, mai ales cu
Context: Din ce în ce mai multe dovezi sugerează
debut precoce, trebuie monitorizate cu atenţie pentru
depresia ca factor de risc important pentru dezvoltarea
apariţia demenţei şi agravarea simptomatologiei. Studiile
bolii degenerative de memorie.
viitoare ar trebui să stabilească dacă tratamentul
Obiectiv: Corelarea simptomelor depresive
tulburărilor din spectrul depresiv poate reduce riscul de
netratate cu riscul de a dezvolta demenţă într-un studiu
apariţie a acestor rezultate.
retrospectiv şi un grup de paciente vârstnice.
Cuvinte cheie: simptome depresive, tulburare de
Metode: Din fişele personale ale unui număr de 73
memorie legată de vârstă, demenţa de tip Alzheimer,
femei cu vârste cuprinse între 70 şi 90 ani, dispensarizate
paciente vârstnice
în cabinetul de medicină de familie, s-au extras date
despre antecedente de episoade depresive. Simptomele
Introducere
depresive prezente au fost evaluate cu Scala de depresie
geriatrică. Diagnosticul de Boală Alzheimer
(BA) şi
Depresia se întâlneşte în 30% [1] până la 50% sau
deficit cognitiv lejer s-a făcut în conformitate cu criteriile
mai mult [2] din pacienţii cu boală Alzheimer (BA), şi
Manualului de diagnostic şi statistică a tulburărilor
este frecvent raportată la persoanele cu deficit cognitiv
psihice.
lejer
(DCL), ca stadiu iniţial, dar anormal, de declin
Rezultate: Un număr de 17 femei au avut un istoric
cognitiv [3]. Persoanele care au experimentat episoade
de depresie
(9 cu un debut<60 ani şi
8 cu debut
depresive la o vârstă precoce ar fi mai susceptibile de a
tardiv>60 ani). Incidenţa depresiei de orice tip a fost
dezvolta BA decât cele care nu s-au confruntat niciodată
semnificativ mai mare la pacientele cu BA decât la cele
cu acestea
[4]. Depresia este asociată cu reducerea
fără
(85,71% faţă la
16,67%, p=0,0001,
95%CI:
activităţii fizice, a interacţiunii sociale şi este un factor de
3,1336-9,5204, RR=5,462). Incidenţa demenţei a fost
risc pentru afectarea sănătăţii, a calităţii vieţii şi pentru
de: 23,53% la persoanele cu depresie severă, 14,29% la
deces. Nu se cunoaşte cu certitudine dacă depresia este
cele cu depresie mai puţin severă (distimie) şi 5,36% la
un simptom al BA sau o cauză a acesteia [5,6]. Mai multe
cele fără depresie;
12,33% la cele cu debut<60 ani,
studii au subliniat faptul că un istoric de depresie majoră
10,96% la cele cu debut>60 ani.
ar dubla riscul de a dezvolta o demenţă mai târziu [5,6] şi
Depressive Symptoms and Memory Disorder in Elderly
95
Original articles
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
că persoanele cu mai multe simptome depresive la
Toate au fost testate prin examen medical complet
momentul iniţial au o incidență crescută de DCL şi BA
în anul 2011.
cu trecerea timpului. Încă nu se cunoaşte dacă depresia
Măsurători
este un semn precoce de demenţă, care s-ar fi explicat
Simptome depresive
printr-o creştere a incidenţei depresiei înainte de
Istoricul de simptome depresive a fost extras din
diagnosticul BA, sau prin modificarea simptomelor
fişele personale ale persoanelor participante şi a fost
depresive pe parcursul progresiei bolii. Rezultatele
investigată prezenţa simptomelor depresive existente la
studiilor desfăşurate până în prezent sunt nesemnificative
evaluare. Simptomele depresive au fost evaluate cu
[5,6]. Cu toate acestea, depresia nu trebuie să fie privită
ajutorul celor
30 de întrebări ale Scalei Depresiei
ca o parte inevitabilă a BA, simptomele depresive pot fi
Geriatrice Yesavage
[8], la momentul iniţial.
asociate cu modificări cerebrale specifice, care pot reduce
Respondenţii au indicat dacă au avut sau nu simptome
rezerva neuronală, astfel încât depresia ar trebui să fie
depresive specifice
(de exemplu: scăderea activităţii/
atent tratată [5,6]. Tratamentul antidepresiv ameliorează
interesului, lipsa de speranţă) sau stări care sugerează
simptomele şi calitatea vieţii pacienţilor, dar nu
absenţa depresiei
(de exemplu: un plus de energie,
încetineşte progresia BA în cazul în care ambele afecţiuni
gândul că viaţa este minunată), prin răspunsuri de tip
sunt prezente. În pseudodemenţă (declin cognitiv ca
DA/NU. Răspunsurile care sugerează depresia au fost
expresie clinică a depresiei) dacă tulburările de memorie
însumate, scorul≥11 pledând pentru o depresie
sunt cauzate de depresie, tratamentul antidepresiv poate
probabilă. Depresia severă a fost considerată începând
aduce îmbunătăţiri în funcţia cognitivă [7]. De aceea,
cu un scor de 21, între 11 şi 21, pacientele au fost
medicul trebuie să caute întotdeauna prezenţa depresiei,
considerate a avea o depresie mai degrabă uşoară sau
atunci când tratează vârstnicii cu tulburări cognitive, atât
distimie.
deficitele apărute într-o perioadă scurtă de timp, cât şi
Depresia şi distimia au fost identificate cu ajutorul
deficitul cognitiv uşor. O mai bună înţelegere a depresiei
Clasificării Internaţionale a Maladiilor, după a zecea
ar putea descoperi noi căi în prevenirea bolii Alzheimer
revizie (ICD-10) [9]. De la aceste coduri ICD-10 a fost
[5,6].
creată o variabilă pe trei niveluri pentru categoriile:
Obiectivul studiului a fost de a determina dacă
distimie, depresie şi fără diagnostic de distimie/depresie.
distimia şi depresia severă sunt asociate cu un risc crescut
În cazul în care o persoană a avut atât un diagnostic de
de demenţă şi deficit cognitiv lejer, la persoanele cu un
depresie cât şi de distimie pe parcursul perioadei de
debut precoce al simptomelor depresive, faţă de cele cu
referinţă, au fost considerate a fi îndeplinite criteriile
debut tardiv. Am investigat impactul simptomelor
pentru depresie [10].
depresive cu debut precoce (<60 ani), în timpul vârstei
Cogniţia şi capacitatea funcţională
mijlocii şi cele cu debut tardiv
(>60 ani), asupra
Participantele au completat mai multe teste
debutului tulburărilor de memorie legate de vârstă. La
cognitive incluzând: Examenul Minim al Stării Mentale
acest studiu au participat persoane cu vârste cuprinse
(MMSE) al lui Folstein [11], care măsoară orientarea,
între 70 şi 90 ani, care erau sub supravegherea unui
înregistrarea de informaţii, atenţia, calculul, redarea
medic de familie. Acest studiu urmăreşte să sublinieze
informaţiilor şi vorbirea; testul de desen al ceasului
importanţa evaluării simptomelor depresive şi a depresiei
Brodaty [12], în care pacientul a fost invitat să deseneze
în general şi la pacienţii vârstnici în special, având în
cadranul unui ceas rotund cu toate numerele şi cu
vedere riscurile majore ale acestor afecţiuni şi asocierile
limbile care arată ora 2:45; testul SIB pentru insuficienţa
morbide care caracterizează pacientul vârstnic şi care
severă, a fost utilizat pentru MMSE<9 şi testul de
influenţează evoluţia clinică.
fluenţă verbală.
Activităţile vieţii zilnice şi capacitatea funcţională
Metode
de a trăi independent a fost măsurată cu: (a) Scala
activităţilor de bază ale vieţii zilnice
(BADL), care
Participanţi
analizează: mersul pe jos, hrănirea, spălatul, îmbrăcatul,
Datele pentru acest studiu retrospectiv de cohortă
toaleta şi continenţa; (b) Scala de activităţi ale vieţii
au fost obținute din fişele personale dispensarizate
zilnice (ADL), cu 17 elemente legate de: mersul pe jos,
într-un cabinet de medicină de familie din regiunea
îmbrăcatul, spălatul la maşina, toaleta, continenţa,
Moldova, din România. Au fost incluse în studiu 73
îngrijirea personală, pregătirea meselor, folosirea
femei în vârstă de peste
70 ani, care au acceptat
obiectelor, hrănirea;
(c) Scala pentru activităţile
participarea. Media de vârstă a fost de 78,5±4,83 ani, iar
instrumentale ale vieţii zilnice (IADL), care explorează
nivelul mediu de educație şcolară a fost clasa a 6-a.
opt activităţi instrumentale: folosirea telefonului,
96
Popescu et al
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
Original articles
gestionarea banilor/mersul la cumpărături, pregătirea
procent din cazuri, din lotul global de la începutul
unui ceai/unei mese, grija de propria casă, spălatul
studiului. Probabilitatea specifică grupei de vârstă de a
rufelor, utilizarea vehiculelor/vizitarea casei prietenilor şi
dezvolta boala a fost calculată prin împărţirea
luarea medicamentelor.
evenimentelor din grupa de vârstă respectivă la numărul
Decizia pentru starea clinică cognitivă
de persoane în grupa respectivă.
Decizia clinică cognitivă a fost efectuată în funcţie
de performanţa participantelor cu privire la testele
Rezultate
cognitive, istoricul medical, medicamente şi starea
funcţională, înregistrate la momentul iniţial şi la un an
În lotul global prevalenţa distimiei a fost de 19,18%
de urmărire, când s-a putut înregistra declinul progresiv
şi a depresiei severe 4,11%. 23,29% au fost considerate ca
al memoriei. Potrivit criteriilor Manualului de
având depresie. În raport cu vârsta, cea mai mare
Diagnostic şi Statistică a Tulburărilor Mentale, ediţia a
prevalenţă a depresiei a fost găsită în intervalul 85-89 ani,
patra [13], a criteriilor Institutului Naţional de Tulburări
7,14% pentru depresie severă şi 42,57% pentru distimie
Neurologice şi Comunicative şi Accident Vascular
(Figura
1). După stabilirea diagnosticului conform
Cerebral şi Asociaţiei pentru Boala Alzheimer şi Bolile
criteriilor DSM IV, a fost calculată prevalenţa specifică pe
Înrudite [14], a Clasificării Internaţionale a Maladiilor,
grupe de vârstă pentru BA şi DCL, restul participantelor
după a zecea revizie
[9], s-a determinat dacă
dovedindu-se a fi normale pentru vârstă sau cu „uitare
participantele au fost normale cognitiv, au avut DCL
benignă”. Au fost diagnosticate 9,59% cu BA, 34,25% cu
sau demenţă. După
12 luni, s-a apreciat progresia
DCL, 56,16% fiind considerate normale pentru vârstă
declinului cognitiv prin compararea rezultatelor
(Figura 2). Se observă că prevalenţa creşte cu vârsta pentru
testărilor făcute la 1 lună, 3 luni, 6 luni.
BA şi DCL, pe măsură ce „uitarea benignă” scade.
A fost utilizată scala GDS Reisberg [15] pentru a evalua
stadiul de depreciere, cu un prag pentru demenţă la stadiul
patru Reisberg. Doar pacientele dependente funcţional la
cel puţin una dintre scalele care evaluează activităţile vieţii
zilnice şi cu declin cognitiv la testele neuropsihologice au
fost considerate cu screening-ul pozitiv pentru diagnosticul
posibil sau probabil de demenţă.
Alte măsurători
Datele demografice ale participantelor au cuprins:
vârsta, nivelul de şcolarizare, prezenţa depresiei şi a altor
comorbidităţi. Au fost efectuate: probe serologice de
rutină, electrocardiograma în stare de repaus şi
tomografia computerizată (TC).
Procedură
Figura 1. Prevalenţa specifică fiecărei grupe de vârstă pentru
Consimţământul voluntar al pacientelor a fost
tulburările din spectrul depresiv (fără depresie, distimie,
înregistrat după ce au primit informații cu privire la
depresie severă)
obiectivul şi protocolul studiului. În cazul în care
pacienta nu îşi putea exprima propria decizie, a fost
contactată şi informată cea mai apropiată rudă a
pacientei pentru a-şi da acordul scris pentru studiu.
Analiza statistică
Toate procedurile statistice au fost efectuate cu
ajutorul EpiInfo
(TM) software
(CDC Atlanta),
versiunea 3.5.3. Rezultatele au fost exprimate ca medie
± DS pentru variabilele numerice. Pentru variabile
calitative au fost utilizate frecvenţa totală şi procentele.
Evaluarea diferenţelor dintre grupuri a fost efectuată cu
ajutorul testului „t Student” pentru variabilele continue
şi χ2 pentru variabilele categoriale. Semnificaţia statistică
Figura 2. Prevalenţa specifică fiecărei grupe de vârstă pentru
a fost definită ca p<0,05, pentru un interval de încredere
demenţă, deficit cognitiv lejer şi uitare benignă (normal
(CI) de 95%. Rata de prevalenţă a fost calculată ca
pentru vârstă)
Depressive Symptoms and Memory Disorder in Elderly
97
Original articles
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
de a dezvolta BA (RR=2,00), fără ca diferenţa să arate
semnificaţie statistică, p=0,42 (>0,05), pentru 95% CI
0,43-7,24.
În funcție de prezenţa DTA a fost definită o variabilă
cu două niveluri. Caracteristicile demografice ale
pacientelor investigate sunt ilustrate în funcţie de acastă
variabilă în tabelul I. Se poate observa că depresia de
orice tip, severă şi distimia, sunt semnificative statistic în
lotul cu DTA cu p=0,0001 (<0,05), 95% CI: 3,1336-
9,5204, cu un risc relativ de 5 ori mai mare de a avea
depresie pentru persoanele diagnosticate cu BA, RR
(riscul relativ)=5,4620. Corelaţia a fost pozitvă atât
pentru depresia severă, cât mai ales pentru distimie.
Astfel la depresia severă: p=0,0112 (<0,05), 95% CI:
1,94-182,62 şi RR:18; iar la distimie: p=0,0020 (<0,05),
Figura 3. Distribuţia de frecvenţă a MMSE
95% CI: 1,62-8,86, RR: 3,8.
Scorul de depresie geriatrică Yesavage a avut o medie
de 12,94 pentru persoanele cu BA şi 8,68 pentru cele
fără BA, interpretându-se un scor între 0-10 ca fără
depresie, 11-20 ca depresie uşoară şi 21-30 ca depresie
severă.
Tabelul I. Caracteristicile participantelor
la momentul inițial în funcție de prezența DTA
(demenţei de tip Alzheimer)
n=73
BAa
fără BA
n=7b
n=66
Vârsta (ani), media ± SD
82,14±2,32
78,5±4,75
Figura 4. Variația MMSE pe grupe de vârstă
Sex (femei), n (%)
7 (9,59)
66 (90,41)
Educaţie (ani), media ± SD
6,1±1,45
6,03±2,03
Scorul de depresie Yesavage,
12,94±2,8
8,68±5,33
Distribuţia de frecvenţă a MMSE mediu se înscrie
media ± SD
într-o curbă gaussiană cu un punctaj între 15 şi 30 pentru
GDSc, media ± SD
4,0±0***
2,35±0,55
MMSE (Figura 3 şi 4). Din grafice se observă că media
Depresie+Distimie (prezenţa),
6 (85,71)***
11 (16,67)
ambelor valori arată prezenţa unui deficit cognitiv
n (%)
moderat, care corespunde pe scala Reisberg stadiului 4,
Depresie severă (prezenţa), n
2 (28,57)*
1 (1,52)
sau unui stadiu incipient de demenţă de tip Alzheimer
(%)
(DTA), conform DSM IV. Aceste paciente au avut un
Distimie (prezenţa), n (%)
4 (57,14)**
10 (15,15)
deficit cognitiv moderat (MMSE=10-20), asociat de un
Debut Depresie sub 60 ani, n
deficit funcţional uşor, evaluat prin ADL, IADL,
4 (57,14)***
5 (7,58)
(%)
obiectivat doar de persoanele apropiate. Doar 8% din
Debut Depresie peste 60 ani,
paciente au avut valori ale MMSE între 10 şi 15 puncte.
2 (28,57)
6 (9,09)
n (%)
La acestea aspectul tomografic a arătat diferite grade de
atrofie corticală şi lărgire ventriculară. Distribuţia pe
a Diagnosticul de boală Alzheimer (BA) şi fără BA, s-a făcut în
conformitate cu criteriile DSM IV.
grupe de vârstă a DCL şi BA este reprezentată în Figura 4.
b testul χ2 pentru variabilele categoriale şi testul t pentru variabilele
În funcţie de momentul de debut al depresiei, s-a
continue a arătat diferențe în caracteristicile de bază în funcţie de
calculat riscul de apariţie a BA pentru categoriile: debut
criteriul cu BA/fără BA la *p<0,05, **p<0,01 şi ***p<0,001.
sub 60 ani şi debut peste 60 ani, constatându-se că în
c GDS (Scala de deteriorare globală Reisberg) a evaluat gradul
primul caz se însoţeşte cu un risc de două ori mai mare
global de depreciere.
98
Popescu et al
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
Original articles
Discuții
Alzheimer, depresia cu debut tardiv ar putea fi un semn
precoce de boală.
În acest studiu s-a examinat relaţia longitudinală
Prezenţa simptomelor depresive în special cu debut
dintre prevalenţa tulburărilor de memorie legate de vârstă
precoce, trebuie să fie monitorizată cu atenţie pentru
şi prezenţa simptomelor depresive în funcţie de momentul
efecte adverse, precum boala degenerativă de memorie
de apariţie înainte sau după 60 ani. De asemenea, s-a
sau deces.
arătat faptul că depresia severă şi distimia, sunt corelate
Studiile viitoare ar trebui să stabilească dacă
pozitiv cu prezenţa demenţei de tip Alzheimer.
tratamentul tulburărilor din spectrul depresiei ar putea
În absenţa tratamentului antidepresiv, depresia ar
reduce riscul acestor rezultate. Un stil de viaţă sănătos, o
trebui să fie monitorizată pentru rezultatele negative, de
viaţă în comunitate şi gândirea pozitivă ar putea fi, de
apariţie a BA sau de deces.
asemenea, luate în considerare atunci când se tratează
Rezultatele lucrării sunt similare cu cele ale studiilor
tulburările de memorie.
anterioare, care arată o relaţie pozitivă între depresie şi
Toţi autorii declară lipsa conflictelor de interese.
simptomele depresive din perioada vieţii de mijloc şi
Cercetarea de faţă nu a avut alt sprijin extern.
tulburările de memorie legate de vârstă.
După lungi dezbateri în jurul rezultatelor diferitelor
studii, relația de cauzalitate dintre depresie şi demenţă
Referinţe
este departe de a fi clarificată [16]. Cele două afecţiuni
au în comun disfuncţii motorii, cognitive şi
1.
Alexopoulos G S, Abrams R C. Depression in
comportamentale. O lucrare recentă care raportează
Alzheimer’s disease. Psychiatric Clinics of Nord
rezultatele a 17 ani de urmărire [17], subliniază faptul că
America 1991;14(2):327-40.
21,6% dintre persoanele cu depresie la momentul iniţial
2.
Tune L E, Depression and Alzheimer’s disese. Depress.
au dezvoltat demenţă, faţă de 16,6% dintre cele fără
Anxiety 1998;8(Suppl.1):91-5.
această boală la debut. Ge Li şi colab. [16] au studiat
3.
Devanand D P, Sano M, Tang Ming-Xin, et al.
asocierea temporală între depresie şi demenţă şi au tras
Depressed Mood and the Incidence of Alzheimer’s disease
concluzia că depresia vârstelor târzii ar putea fi mai
in Elderly Living in the Community. Arch Gen
degrabă o primă manifestare a demenţei.
Psychiatry 1996;53(2):175-82.
Depresia severă a fost prezentă la 28,57% dintre
4.
Geerlings M I, den Heijer T, Koudstaal P J, Hofman
cele cu DTA şi numai la 1,52% din cele fără DTA.
A, Breteler M M B. History of depression, depressive
Se poate estima că riscul de a dezvolta depresie
symptoms, and medial temporal lobe atrophy and the
pentru persoanele care suferă de tulburări de memorie
risk of Alzheimer disease, Neurology 2008;70:1258.
este de aproximativ 5 ori mai mare decât pentru cele
5.
Wilson RS, Hoganson G M, Rajan KB, Barnes LL,
care nu suferă de aceste tulburări: 2,77<(RR=5,46)<9,54.
Mendes de Leon CF, Evans DA. Temporal course of
Referitor la influenţa depresiei asupra tulburărilor
depressive symptoms during the development of
de memorie legate de vârstă, DCL şi DTA, 50% dintre
Alzheimer disease: Blowing hot and cold over depression
pacientele care au fost mai deprimate, mai în vârstă şi cu
and cognitive impairment. American Academy of
scoruri mai mici MMSE, au dezvoltat boala de memorie.
Neurology 2011;76:1531-2.
6.
Wilson RS, Arnold SE, Todd L, Beck MS, Bienias JL,
Concluzii
Bennett DA. Changes in Depressive Symptoms During
the Prodromal Phase of Alzheimer’s Disease. Arch Gen
Depresia de orice tip este frecvent asociată cu
Psychiatry 2008;65(4):439-46.
afectarea memoriei legate de vârstă. Asocierea este
7.
Lantz MS, Buchalter EN. Pseudodementia. Cognitive
semnificativă statistic pentru depresia severă şi distimie,
decline caused by untreated depression may be reversed
p=0,0001 (<0,05), 95% CI: 3,13-9,52. Riscul de a avea
with treatment. Geriatrics 2001;56(10):42-3.
depresie pentru o persoană cu BA este de aproximativ 5
8.
Yesavage JA, Brink TL, Rose TL, et al. Development and
ori mai mare (RR=5,46), iar riscul unei persoane cu
Validation of a Geriatric Depression Screening Scale: A
depresie de a dezvolta BA este de
2 ori mai mare
Preliminary Report. J Psych Research 1983;17(1):37-49.
(RR=2,00). Riscul este mai mare pentru depresia severă,
9.
World Health Organisation, Tenth revision of the
RR=18, p=0,0112 (<0,05) şi mai mic, dar prezent,
international classification of the disease. Geneva:
pentru distimie, RR=3,8, p=0,0020 (<0,05).
World Health Organisation, 1993;46-7.
În timp ce depresia apărută sub vârsta de 60 ani
10.
Castilla-Puentes RC, Habeych ME. Subtypes of
poate fi un factor de risc pentru demenţa de tip
Depression among Patients with Alzheimer’s Disease and
Depressive Symptoms and Memory Disorder in Elderly
99
Original articles
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
Other Dementias. Alzheimer’s & Dementia
Alzheimer’disease:report of the NINCDS-ADRDA Work
2010;6(1):63-9.
Group under the auspices of the Department of Health
11. Folstein MF, Folstein SE, McHugh PR. „Mini-mental
and Human Services Task Force on Alzheimer’s disease.
state”. A practical method for granding the cognitive
Neurol 1984,34:939-44.
state of oatients for the clinician. Journal of Psychiatric
15. Reisberg B, Ferris SH, de Leon MJ, Crook T. Te Global
Resourses 1975;12(3):189-98.
Deterioration Scale for assessment of primary degenerative
12. Brodaty H, Moore C M. Te Clock Drawing Test for
dementia. Am J Psychiatry 1982;139(9):1136-9.
dementia of the Alzheimer type: a comparison of three
16. Li G, Wang LY, Shofer GB, et al. Temporal Relationship
scoring methods in a memory disorders clinic. Int J of
Between Depression and Dementia. Findings From a
Geriatric Psychiatr 1997;12:619-27.
Large Community-Based
15-Year Follow-up Study.
13.
***, Diagnostic and Statistical Manual of Mental
Arch Gen Psychiatry 2011;68(9):970-7.
Disorders, 4th edn., American Psychiatric Association,
17. Saczynski JS, Beiser A, Seshadri S, Auerbach S, Wolf
Washington, 1994;21-5.
PA, Au R. Depressive symptoms and risk of dementia.
14. McKhann G, Drachman D, Folstein M, Katzman R,
Te Framingham Heart Study. Neurology
Price D, Stadian E. Clinical diagnosis of
2010;75(1):35-41.
100
Popescu et al
Original articles
CUANTIFICAREA RISCULUI ATEROGENIC FOLOSIND INDEXUL
ATEROGENIC AL PLASMEI (AIP) ŞI AL RISCULUI DE BOLI
CARDIOVASCULARE A PACIENŢILOR HIPERTENSIVI
Popa Călin1, Puşchiţă Maria2
1Catedra de Histologie, Facultatea de Medicină, Farmacie şi Medicină Dentară, Univesitatea de Vest „Vasile Goldiş”
Arad, Spitalul Clinic Judeţean de Urgenţă Timişoara, 2Catedra de Medicină Internă, Facultatea de Medicină, Farmacie
şi Medicină Dentară, Univesitatea de Vest „Vasile Goldiş” Arad, Spitalul Clinic Judeţean de Urgenţă Arad
Adresa pentru corespondenţă:
Dr. Călin Popa
Univesitatea de Vest „Vasile Goldiş” Arad
Facultatea de Medicină, Farmacie şi Medicină Dentară
Arad, Strada Feleacului Nr. 1
Email: calinpopa@msn.com.
Primit: 10.01.2013
Acceptat: 20.02.2013
Med Con March 2013, Vol 8, No 1, 101-108
Rezumat
tutun, alcool. Metoda utilizată a fost cea a comparaţiei
mai multor formule de aterogeneză şi a scorurilor de
Scopul a fost să găsim un protocol de cuantificare a
boli cardiovasculare.
riscului de aterogeneză precum şi a riscului de
Rezultate: Din studiu am obţinut valori ridicate ale
evenimente cardiovasculare majore la pacienţii
fracţiunilor lipidice şi o semnificativă scădere a valorii
hipertensivi, cu sau fără boli cronice asociate.
HDLc în toate grupurile de studiu faţă de cel de control.
Material şi metodă: Studiul a cuprins
80 de
În grupurile H1-H4 am observat o diferenţă
pacienţi hipertensivi grupaţi astfel: primul grup (H1) a
semnificativă a riscului de evenimente cardiovasculare
inclus 20 de pacienţi hipertensivi nou-descoperiţi gradul
posibile la pacienţii de sex masculin faţă de pacienţii de
I (conform clasificării Societăţii Europene de Cardiologie
sex feminin. De asemnea s-a observat o creştere
şi a ultimelor ghiduri europene de hipertensiune) fără
semnificativă a LDLc în grupul H2 faţă de grupul H1 şi
tratament antihipertensiv, grupul al doilea (H2) cu 20
valorile indexului aterogenic al plasmei
(AIP) de
de pacienţi cu sindrom X metabolic, al treilea grup (H3)
0,604±0,23 faţă de 0,136±0,19 cu un p<0,0001 (foarte
cu 20 de pacienţi hipertensivi gradul II având asociat
semnificativ statistic); pentru grupul H1 riscul
diabet zaharat tip 2, grupul al patrulea (H4) cu 20
aterogenic şi de evenimente cardiovasculare fost unul
pacienţi hipertensivi gradul
2 având asociat diabet
moderat, iar pentru grupurile H2, H3 şi H4 a fost foarte
zaharat tip 2 şi boală cronică renală şi un grup control
ridicat comparat cu grupul control p<0,001.
(C) cu 20 de subiecţi sănătoşi. Criteriile de includere au
Concluzii: Corelând datele obţinute cu studiile
fost vârstă peste 35 de ani şi sub 60 de ani (media de
recente din literatura de specialitate, am concluzionat că
vârstă pentru pacienţii de sex feminin a fost 44,5±3,9 şi
indicele aterogenic al plasmei (AIP) şi scorul de risc
pentru pacienţii de sex masculin a fost 45,5±3,2), fără
cardiovascular estimativ (QRISK) sunt net superioare
boli cardiovasculare asociate
(antecedente de bypass,
din punct de vedere statistic şi al diagnosticării
stentare sau alte boli cardiovasculare), fără consum de
aterogenezei şi a riscului de evenimente CV majore.
Atherogenic Risk Quantification by Using the Atherogenic Index of Plasma (Aip) and Cardiovascular Risk
101
Calculator on Hypertensive Patients
Original articles
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
Cuvinte cheie: hipertensiune, riscul aterogenic,
[7,8]. Riscul de a dezvolta boli cardiace coronariene este
riscul cardiovascular, LDL, HDL, colesterol total
crescut la pacienţii cu niveluri ridicate ale TG şi mutaţii ale
genei HL ce influenţează structura şi sinteza HDLc
Introducere
precum şi creşterea TG [9]. Hipertrigliceridemia va creşte
activitatea lipazei hepatice HL şi consecutiv va denatura
Hipertensiunea arterială şi ateroscleroza sunt două
HDLc, cu fiecare degradare a 1mg de HDLc va determina
cauze principale ale morbidităţii şi mortalităţii
o creştere cu 2% a riscului de boală coronariană [10,11].
cardiovasculare la nivel global. Ele adesea pot coexista la
Obiectivul principal al acestui studiu a fost să găsim
pacient şi ambele se pot provoca şi/sau exacerba. Noile
un protocol de cuantificare a riscului de aterogeneză
studii ştiinţifice din domeniul biologiei moleculare au
precum și a riscului de evenimente cardiovasculare
dus la identificarea de polimorfisme genetice asociate cu
majore la pacienții hipertensivi cu sau fără boli cronice
hipertensiune arterială şi cu evenimentele cardiovasculare,
asociate.
iar studiile clinice recente au pus în evidenţă diversitatea
fiziologică la hipertensivi şi caracterul heterogenetic al
Material şi metodă
bolilor cardiovasculare [1]. S-a dovedit, deasemenea, că o
serie de factori de creştere peptidică au fost identificaţi
Au fost evaluaţi 80 de pacienţi (45 de sex masculin,
prin mecanisme paracrine şi autocrine ce pot fi implicate
feminin 35) suferind de hipertensiune arteriala şi au fost
în remodelarea vasculară şi aterogeneză la nivelul
grupaţi astfel: primul grup (H1) a inclus 20 de pacienţi
endoteliului vascular la pacienţii hipertensivi
[2].
(9 sex masculin, feminin 11) hipertensivi gradul I fără
Datorită locaţiei sale strategice, endoteliul vascular
tratament, grupul al doilea (H2) cu 20 de pacienţi (12
funcţionează ca un senzor al tensiunii arteriale care
sex masculin, feminin
8) cu sindrom X metabolic
mediază modificări hemodinamice şi umorale [3].
(hipertensiune gradul I/II, scăderea toleranţei la glucoză,
Studiile epidemiologice au arătat că mai mulţi factori
obezitate, sedentarism), al treilea grup (H3 - 11 de sex
contribuie la debutul şi progresia aterosclerozei, dintre
masculin, feminin 9) a inclus 20 de pacienţi hipertensivi
aceștia vârsta, sexul şi predispoziţia genetică fiind
gradul II având asociat diabet zaharat tip 2, grupul al
parametri nemodificabili. Deşi sexul masculin este un
patrulea (H4 - 13 de sex masculin, feminin 7) a cuprins
important factor de risc, ateroscleroza devine o problemă
20 pacienţi hipertensivi gradul 2 având asociat diabet
majoră şi pentru femeile care iau contraceptivele orale
zaharat tip 2 şi boală cronică renală. Al cincilea grup,
crescându-le riscul şi mai mult atunci când sunt utilizate
grupul control a cuprins 20 de persoane sănătoase (10
şi după menopauză, de obicei simptomele aparând cu
de sex masculin, feminin 10).
aproximativ 10 ani mai târziu [4]. Nivelurile crescute ale
Criteriile de includere pentru grupurile de studiu au
colesterolului seric sunt principalul factor de risc pentru
fost vârsta peste 35 de ani şi sub 60 de ani (media de
ateroscleroză, mai ales fracţia LDLc, amintind şi de alţi
vârstă pentru pacienţii de sex feminin a fost 44,5±3,9 şi
factori de risc pentru ateroscleroză: fumatul, scăderea
pentru pacienţii de sex masculin a fost 45,5±3,2), fără
toleranţei la glucoză, obezitatea şi sedentarismul
[5].
boli cardiovasculare asociate
(antecedente de bypass,
Prevalenţa sindromului metabolic în rândul ţărilor
stentare sau alte boli cardiovasculare), fără consum de
dezvoltate este în creştere datorită creşterii incidenţei
tutun, alcool, medicaţie hipolipemiantă.
obezităţii. Obezitatea centrală joacă un rol cheie în
Datele clinice ale pacienţilor hipertensivi şi a
patogeneza sindromului metabolic: promovează
grupului de control au fost colectate din examenul
inflamaţia, hipertensiunea arterială şi dislipidemia şi duce
anamnestic, clinic şi paraclinic realizat fiecărui pacient
la dezvoltarea diabetului zaharat de tip 2 şi aterosclerozei.
în momentul includerii în grupul de studiu. Măsurătorile
Corectarea şi controlarea acestora înseamnă un risc mai
tensiunii arteriale au fost efectuate conform ghidurilor
mic de dezvoltare sau progresie a aterosclerozei [6].
Societăţii Europene de Hipertensiune Arterială (ESH),
Pentru estimarea riscului aterogen există mai multe
în unele cazuri, pacienţii din grupul H3 şi H4
(5
metode la ora actuală, în funcţie de studiul pe care se
pacienţi) au necesitat aparat de monitorizare a tensiunii
bazează, ca de exemplu compararea colesterolul total,
arteriale Holter pentru 24 de ore, pentru a stabili corect
raportul HDLc/LDLc, calculatoare ce utilizează fie
gradul de hipertensiune arterială (clasa 2/3) deoarece au
formula Friedewald sau formula Iraniană, raportul
avut hipertensiune arterială fluctuantă [12].
colesterol total/HDLc şi multe altele. Indicele aterogenic
Consecutiv anamnezei şi examenului clinic,
plasmatic (AIP) este un instrument de evaluare a riscului
examenul paraclinic a inclus dozarea din sângele venos a
aterogenetic, acesta se bazează pe o formulă care utilizează
colesterolului total (CT), trigliceridelor (TGR), LDL-
nivelul TG şi a HDLc exprimat fie în mmol/L fie în mg/dl
colesterol, HDL-colesterol, a creatininei (în mod special
102
Popa et al
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
Original articles
pentru calcularea estimativă a ratei filtrării glomerulare
raportul de LDLc/HDLc şi valorile AIP
(indexul
- RFG). S-a investigat şi raportul albumină/creatinină,
aterogenic al plasmei) între fiecare grup de pacienţi
utilizând dipstick-uri urinare
(pentru evaluarea
hipertensivi şi grupul de control. Pentru comparaţia
albuminuriei ca marker al afectării renale consecutive
eficienţei acestora am utilizat un soft medical licenţiat şi
hipertensiunii sau diabetului zaharat) [13].
autorizat QRiskR2-2012 pentru estimarea riscului de
Deoarece stresul este un factor de risc important,
evenimente cardiace majore pentru următorii 5 sau 10
am inclus un chestionar psihologic de evaluare a
ani (un program ce utilizează o multitudine de date
stresului. Testul a cuprins
25 de întrebări, fiecare
anamnestice, clinice şi paraclinice în special cele din
întrebare putând fi punctată cu
1 punct pentru un
profilul lipidic), util de asemenea şi pentru diagnosticarea
răspuns pozitiv şi cu
0 pentru un răspuns negativ.
pacienţilor care nu au fost încă diagnosticaţi [14].
Rezultatele obţinute au fost încadrate într-una din cele
Toate rezultatele au fost exprimate ca medie±deviaţia
3 categorii de rezultate posibile ale testului astfel: sub 4
standard
(DS). Datele au fost analizate pentru
puncte - stres minim, 5-13 puncte a indicat faptul că
semnificaţie statistică folosind programul informatic
subiectul a întâmpinat experienţe de stres date de
Statistica
7. Pentru valorile lui p<0,05 s-a considerat
probleme de sănătate, fie mentale, fie fizice sau ambele şi
semnificativ, pentru valori ale lui p<0,01 s-a considerat
peste 14 puncte a indicat un nivel critic de stres.
deosebit de semnificativ statistic, pentru valori ale lui
Pentru cuatificarea riscului aterogen şi cel al riscului
p<0,001 s-a considerat foarte semnificativ, iar pentru
bolilor cardiovasculare ne-am propus realizarea unui
valori p>0,05 au fost considerate nesemnificative.
protocol pentru cea mai corectă metodă estimativă a
celor două probleme importante la ora actuală:
Rezultate
aterogeneza şi evenimentele cardiovasculare majore
(infarct miocardic şi accident vascular cerebral). Astfel
În Tabelul I (date selectate din anamneză şi examen
am inclus determinarea raportului dintre TC/HDLc,
clinic obiectiv) se poate observa că vârsta subiecţilor în
Tabelul 1. Date clinice ale pacienţilor hipertensivi şi a grupului de control
Parametri*
Grup
Vârstă1
IMC1
TA1
CS1
♂
♀
♂
♀
♂
♀
♂
♀
Control
38,5±2,3
37±4,2
24,3±3,2
20,4±1,6
124±2,1
118±1,2
4,75±1,2
6±2,3
/78±1,7
/74±1,7
H1
42±5,7
39±4,5
25,9±2,3
25,1±1,2
148±1,7
146±1,9
10,75±3,4
10,89±4,2
/96±1,8
/94±2,4
p (H1 cu C)2
0,00026
0,01492
0,26054
0,00155
0,00355
0,00213
0,00086
0,00897
***
**
***
**
***
**
H2
46,5±3,6
44,5±4,8
31,5±4,6
29,5±5,3
150±3,2
148±2,8
13±1,9
12±1,6
/92±2,4
/98±2,3
p (H2 cu C)2
0,00012
0,00123
0,01801
0,00256 **
0,00082
0,00188
0,00048
0,00064
***
**
***
**
***
***
H3
47±5,1
46±7,2
25,8±1,7
24,9±1,4
168±2,2
156±2,6
12±2,8
11±2,4
/106±2,4
/104±2,8
p (H3 cu C)2
0,00018
0,00025
0,01901
0,00158 **
0,00142
0,00186
0,00036
0,00054
***
***
**
**
***
***
H4
49±4,2
52±3,1
25,3±3,8
25,5±4,7
176±2,8
172±3,5
14±1,89
13±1,67
/104±2,9
/108±4,1
p (H4 cu C)2
0,00102
0,01811
0,03902
0,00118
0,00024
0,00048
0,00022
0,00028
**
**
***
***
***
***
Legendă: 1=media şi deviaţia standard; IMC=indicele de masă corporală, TA=tensiunea arterială; CS=chestionar stres; 2=valorile lui p
rezultat prin în comparaţia fiecărui grup de hipertensivi cu grupul control, p<0,05* semnificativ statistic, p<0,01** foarte semnificativ
statistic şi p<0,001*** extrem de semnificativ statistic.
Atherogenic Risk Quantification by Using the Atherogenic Index of Plasma (Aip) and Cardiovascular Risk
103
Calculator on Hypertensive Patients
Original articles
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
grupurile studiate este apropiată, de asemenea IMC
creatinină spre microalbuminurie în special la pacienţii
(indicele de masă corporală) nu prezintă diferenţe foarte
de sex masculin, ceea ce indică un început de afectare
mari între grupurile hipertensive H1-H4 (valoarea lui
glomerulară datorită hipertensiunii şi nivelului glicemiei
p=0,26054 pentru grupul H1 faţă de grupul control),
aflată la limita superioară la aceşti pacienţi. Diferenţele
numai nivelul hipertensiunii în aceleaşi grupuri este
mari semnificativ statistic au fost mai importante la
semnificativ diferit faţă de cel de control cu valori ale lui
valorile CT, TG şi HDL-c, în special la pacienţii de sex
p<0,05 (p=0,0082 pentru subiecţii de sex masculin şi
masculin, restul fiind la limita superioară, dar în limite
p=0,0018 pentru subiecţii de sex feminin din grupul H2).
normale (Tabel II).
În ceea ce priveşte distribuţia pe sexe, pacienţii de
În grupul H2 (Tabel III) parametrii biochimici au
sex feminin au avut valori mai reduse ale parametrilor
fost semnificativ modificaţi la aceşti pacienţi având
măsuraţi faţă de cei de sex masculin, iar indexul de stres
valori foarte mari. Din datele anamnestice reiese că
ne arată că în grupurile cu boli asociate stresul este mult
pacienţii acestui grup sunt obezi cu profil lipidic foarte
mai mare faţă de cei din grupul control, de exemplu
modificat, hipertensivi de mai mult de 1 an, cu un stil
valoarea lui p=0,00028 din grupul H4 pentru pacienţii
de viaţă sedentar şi vicios, cu toleranţă scăzută la glucoză,
de sex feminin şi p=0,00022 pentru cei de sex masculin.
cu microalbuminurie şi RFG care indică afectare a
Pentru pacienţii din grupul H1
(pacienţi
funcţiei renale, în acest sens şi valorile p sunt
hipertensivi
nou-descoperiţi
fără
tratament
semnificative comparativ cu grupul control.
antihipertensiv) se observă o modificare a profilului
Pentru pacienţii grupurilor H3 şi H4 datele
lipidic şi o uşoară deviaţie a valorii raportului albumină/
rezultate ne indică un ecart semnificativ în comparaţie
Tabelul II. Date biochimice a grupului de studiu H1, comparativ cu grupul de control
Grupul de control
H1
p
Parametri
♀
♂
♀
♂
♀
♂
CT (mg/dl)*
186,1±11,2
188,1±10,2
202,2±25,8
206,5±26,8
0,0125
0,0118
TG (mg/dl)*
122,8±9,8
138,3±9,6
144,3±22,4
182,6±18,6
0,0228
0,0214
LDL colesterol (mg/dl)*
126,4±7,5
124,2±8,4
154,2±26,8
158,5±24,5
0,0345
0,0278
HDL colesterol (mg/dl)*
58,1±2,8
52,1±4,4
46,7±32,3
44,8±12,26
0,0159
0,0147
Glicemie (mg/dl)*
88,3±1,68
92,3±2,4
98,7±17,6
98,7±18,45
0,0445
0,0356
Creatinină serică (mg/dl)
0,84±0,18
0,92±0,12
1±0,68
1,2±0,88
0,0562
0,0511
Raport albumină/creatinină (mg/g)
18±1,5-N
20±2,4-N
22±2,8-N
24±3,2-M
0,0126
0,0118
RFG(ml/min/1,73m2)
118±2,2
120±3,4
102±7,5
108±5,7
0,0044
0,0024
Legendă: *= media+DS, Valoarea lui p<0,05 considerat semnificativă (S), p>0,05 considerat nesemnificativ (NS); Raportul albumină-
creatinină: N-valori normale, M-prezenţa microalbuminuriei, A-proteinurie clinică
Tabelul III. Date biochimice a grupului de studiu H2, comparativ cu grupul de control
Grupul de control
H2
p
Parametri
♀
♂
♀
♂
♀
♂
CT (mg/dl)*
186,1±11,2
188,1±10,2
386,1±54,6
424,3±58,5
0,0036
0,0028
TG (mg/dl)*
122,8±9,8
138,3±9,6
368,1±25,7
452,4±56,2
0,0068
0,0015
LDL colesterol (mg/dl)*
126,4±7,5
124,2±8,4
192,3±25,5
202,4±44,3
0,0145
0,0122
HDL colesterol (mg/dl)*
58,1±2,8
52,1±4,4
40,5±34,5
38,8±38,5
0,0224
0,0189
Glicemie (mg/dl)*
88,3±1,68
92,3±2,4
102,2±23,6
110,7±46,8
0,0388
0,0259
Creatinină serică (mg/dl)*
0,84±0,18
0,92±0,12
1,4±0,89
1,6±0,46
0,0148
0,0125
Raport albumină/creatinină (mg/g)
18±1,5-N
20±2,4-N
44±12,5-M
68±8,9-M
0,0065
0,0089
RFG (ml/min/1,73m2)
118±2,2
120±3,4
96±12,5
92±7,8
0,0188
0,0145
Legendă: *= media+DS, Valoarea lui p<0,05 considerat semnificativă (S), p>0,05 considerat nesemnificativ (NS; Raportul albumină-
creatinină: N-valori normale, M-prezenţa microalbuminuriei, A-proteinurie clinică
104
Popa et al
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
Original articles
cu grupul de control şi grupul H1 a valorilor parametrilor
de a grupului control şi în limite normale
(media
biochimici având în vedere ca la aceşti pacienţi patologia
statistică 1,2±0,88).
este mai diversificată, precum şi media de vârstă mai
Pentru calcularea estimativă a ratei filtrării
mare. Diferenţele dintre grupul de control şi fiecare alt
glomerulare
(RFG) am utilizat un calculator online
grup sunt evidente, astfel grupul H2
(cu sindrom
gratuit utilizând formula MDRD (Modification of Diet
metabolic) are cele mai mari valori ale fracţiunilor
in Renal Disease) dezvoltat de Societatea Internaţională
lipidice, iar pentru acelaşi grup H2 şi pentru grupul H3
de Nefrologie
(ISN
- International Society of
şi H4 (pacienţi cu diabet zaharat de tip 2) s-au evidenţiat
Nephrology). Cu date anamnestice şi nivelul creatininei
cele mai ridicate valori ale glicemiei. Corelat cu valorile
serice am reuşit să determinăm valoarea estimativă a
glicemice şi cu cele ale hipertensiunii am determinat
RFG (ml/min/1,73m2) şi să clasificăm stadiul funcţional
microalbuminurie uşoară încă din grupul H1 la pacienţii
al rinichilor pentru grupurile noastre de studiu conform
de sex masculin (valori ale mediei peste 20 mg/g), iar în
stadializării ISN (Tabelul VI). Grupurile H2 şi H3 s-au
grupul H2 şi H3 microalbuminurie marcată (valori ale
aflat
în stadiul I de boală cronică renală
mediilor între 44-180 mg/g), iar în grupul H4 (Tabelul
(microalbuminurie prezentă), grupul H4 s-a aflat în
V) s-a găsit proteinurie clinică (valori ale mediei statistice
stadiul II de boală cronică renală (raportul albumină/
>240 mg/g). Valorile lui p au indicat diferenţe
creatinină indicând proteinurie clinică) cu disfuncţie
semnificative între control şi grupul H1 la toţi parametrii
renală prezentă.
masuraţi, doar valoarea creatininei serice a fost
În Tabelul VII s-au prezentat datele rezultate prin
nesemnificativă la acest grup (p>0,05), fiind apropiată calcularea raportului LDL-c/HDL-c şi raportului CT/
Tabelul IV. Date biochimice a grupului de studiu H3, comparativ cu grupul de control
Grupul de control
H3
p
Parametri
♀
♂
♀
♂
♀
♂
CT (mg/dl)*
186,1±11,2
188,1±10,2
212,2±34,5
234,7±25,8
0,0098
0,0122
TG (mg/dl)*
122,8±9,8
138,3±9,6
256,1±38,4
260,7±33,7
0,0144
0,0147
LDL colesterol (mg/dl)*
126,4±7,5
124,2±8,4
166,2±42,1
168,5±34,6
0,0159
0,0135
HDL colesterol (mg/dl)
58,1±2,8
52,1±4,4
46,3±44,8
38,4±27,4
0,0115
0,0215
Glicemie (mg/dl)*
88,3±1,68
92,3±2,4
262,2±31,3
324,3±28,4
0,0025
0,0012
Creatinină serică (mg/dl)*
0,84±0,18
0,92±0,12
2,2±0,25
2,4±0,26
0,0059
0,0156
Raport albumină/creatinină (mg/g)
18±1,5-N
20±2,4-N
162±11,5-M 180±12,5-M
0,0012
0,0256
RFG (ml/min/1,73m2)
118±2,2
120±3,4
88±4,8
86±11,8
0,0278
0,0125
Legendă: *= media+DS, Valoarea lui p<0,05 considerat semnificativă (S), p>0,05 considerat nesemnificativ (NS; Raportul albumină-
creatinină: N-valori normale, M-prezenţa microalbuminuriei, A-proteinurie clinică
Tabelul V. Date biochimice a grupului de studiu H4, comparativ cu grupul de control
Grupul de control
H4
p
Parameters
♀
♂
♀
♂
♀
♂
CT (mg/dl)*
186,1±11,2
188,1±10,2
244,8±46,2
252,9±51,1
0,0147
0,0125
TG (mg/dl)*
122,8±9,8
138,3±9,6
262,2±31,7
281,5±46,5
0,0255
0,0261
LDL colesterol (mg/dl)*
126,4±7,5
124,2±8,4
172,1±28,5
174,2±11,8
0,0169
0,0256
HDL colesterol (mg/dl)
58,1±2,8
52,1±4,4
42,4±48,2
36,3±12,3
0,0259
0,0169
Glicemie (mg/dl)*
88,3±1,68
92,3±2,4
298,6±22,1
286,1±28,4
0,0048
0,0158
Creatinină serică (mg/dl)*
0,84±0,18
0,92±0,12
5,2±0,73
5,8±0,86
0,0011
0,0098
Raport albumină/creatinină (mg/g)
18±1,5-N
20±2,4-N
242±11,7-A
260±10,2-A
0,0059
0,0185
RFG (ml/min/1,73m2)
118±2,2
120±3,4
66±4,8
58±8,2
0,0198
0,0194
Legendă: *= media+DS, Valoarea lui p<0,05 considerat semnificativă (S), p>0,05 considerat nesemnificativ (NS); Raportul albumină-
creatinină: N-valori normale, M-prezenţa microalbuminuriei, A-proteinurie clinică
Atherogenic Risk Quantification by Using the Atherogenic Index of Plasma (Aip) and Cardiovascular Risk
105
Calculator on Hypertensive Patients
Original articles
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
Tabelul VI. Stadializarea disfuncţiei renale în funcţie de RFG
Stadiul** GFR*
Description
I
90+ Funcţie renală normală (analiza de urină, malformaţiile structurale saufactorii genetici indică
afecţiune renală)
II
60-89
Disfuncţie renală uşoară (se corelează RFG cu analiza de urină, malformaţiile structurale sau factorii
genetici pentru indicarea stadiului II).
III a
45-59
Disfuncţie renală moderată (cu sau fără alte dovezi de afectare renală)
III b
30-44
Disfuncţie renală moderată
IV
15-29
Disfuncţie renală severă
V
<15
Insuficienţă renală severă
Legendă: *RFG=rata filtrării glomerulare calculată în ml/min/1.73m2, valori estimative obţinute prin formula MDRD a calculatorului
GFR; **stadializare ISN (International Society of Nephrology) privind clasificarea disfuncţiilor renale.
Tabelul VII. Formulele aterogenezei (valori şi deviaţia standard)
C
H1
p(H1-C)
H2
p(H2-C)
I*
♀
♂
♀
♂
♀
♂
♀
♂
♀
♂
AIP
0,046±
0,064±0,23
0,136±
0,257±
***
***
0,604±
0,688±
***
***
0,8
1,2
1,45
1,87
1,75
LDLc/
2,17±
2,38±0,27
3,34±1,1
3,59±
**
**
4,8±2,32
5,31±
**
**
HDLc
1,2
1,67
1,98
TC/
3,20±
3,61±0,56
4,39±1,12
4,68±
**
**
9,68±2,31
11,15±
**
**
HDLc
0,75
1,24
2,06
II*
C
H3
p(H3-C)
H4
p(H4-C)
♀
♂
♀
♂
♀
♂
♀
♂
♀
♂
AIP
0,046±
0,064±0,67
0,385±1,98
0,475±
***
***
0,435±
0,532±
***
***
0,97
2,11
2,31
2,33
LDLc/
2,17±
2,38±1,11
3,60±1,55
4,42±
**
**
4,09±
4,83±
**
**
HDLc
0,67
1,67
1,99
3,11
TC/
3,20±
3,61±1,76
4,60±1,65
6,15±
**
**
5,80±
7,02±
**
**
HDLc
0,12
1,98
1,75
2,34
Legendă: * media+DS; ***valoarea lui p<0,0001 (extrem de semnificativ statistic), ** valoarea lui p<0,001 (foarte semnificativ statistic).
Tabelul VIII. Scorurile de risc cardiovascular (media calculelor)
Parametri1
AIP
Scorul QRISK
Grupuri
♀
♂
♀
♂
Control
0,046±0,8
0,064±0,23
0,4%±1,71
0,5%±1,52
H1
0,136±1,2
0,257±1,45
4,2%±2,52
4,6%±2,45
p (H1 cu C)2
***
***
***
***
H2
0,604±1,87
0,688±1,75
30,4%±1,95
31,8%±2,75
p (H2 cu C)2
***
***
***
***
H3
0,385±1,98
0,475±2,11
20,2%±2,14
21,3%±3,24
p (H3 cu C)2
***
***
***
***
H4
0,435±2,31
0,532±2,33
42,5%±2,06
44,2%±2,48
p (H4 cu C)2
***
***
***
***
Legendă: 1-media şi deviaţia standard; AIP (indicele aterogenic al plasmei), scorul QRisck (scor ce indică estimativ riscul
de a dezvolta boli cardiovasculare în următorii 10 ani) obţinut cu software-ul licenţiat QRISCKR2012; 2-valorile lui p
rezultat prin în comparaţia fiecărui grup de hipertensivi cu grupul control, p<0.0001*** (extrem de semnificativ).
106
Popa et al
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
Original articles
HDL-c, acestea au fost raportate la valorile AIP
reflectă perfect balanţa dintre lipoproteinele aterogene şi
(indexului aterogen al plasmei).
cele protectoare. Studiile clinice au arătat că indexul
În Tabelul VIII a fost comparat AIP
(indexul
aterogenic al plasmei
(AIP) poate estima şi riscul
aterogenic plasmatic) pentru fiecare grup în funcţie de
cardiovascular, de asemenea acest index este sensibil şi la
sex, cu scorul QRISCK utilizând un program
tratamentul farmacologic, fiind un barometrul al reuşitei
QRISKR2-2012 (licenţiat de către ClinRisk Ltd UK).
terapeutice. În ceea ce priveşte AIP, valorile normale
Acesta utilizează date anamnestice (vârstă, sex, IMC,
trebuie să fie mai mici decât 0,11, riscul de evenimente
stilul de viață, boli asociate şi altele), valorile tensionale
cardiovasculare fiind redus; intervalul 0,11-0,21 indică
şi raportul CT/HDL-c pentru estimarea riscului de a
un risc intermediar de boli CV iar valori >0,24 un risc
dezvolta boli cardiovasculare majore (infarct miocardic
cardiovascular ridicat [18].
sau accident vascular cerebral) în următorii 10 ani.
În studiul nostru, diferenţe semnificative în
Se poate observa că valorile lui p sunt foarte mici
grupurile de pacienţi hipertensivi au fost şi între subiecţii
(<0,0001) ceea ce ne indică o semnificaţie statistică foarte
de sex feminin şi masculin. AIP pentru pacienţii de sex
importantă, decât valorile lui p comparativ cu indicii
feminin din grupul de control este 0,046 şi în grupul
aterogenezei ai raporturilor CT/HDL-c şi LDL-c/LDL-c.
H2 pentru pacienţii de sex feminin este de
0,604
(aproape de 13 de ori mai mare), cu valori ale lui
Discuţii
p<0,0001 (extrem de semnificativ statistic), pe când
indicele aterogenic al raportului LDLc/HDLc din lotul
Datele studiului nostru releva faptul ca la pacienţii
de control este 2,17 pentru pacienţii de sex feminin, iar
cu media de vârstă mai mică şi debut de boală
pentru grupul H2 (sex feminin) este de 4,8 (aproape de
hipertensivă (H1) parametrii amintiţi au fost modificaţi
2 ori mai mult) cu un p<0,001.
uşor dar semnificativ statistic faţă de grupul control iar
Pentru o comparaţie şi mai complexă indicele
la celelalte grupuri de studiu modificările au fost marcate
raportului CT/HDLc pentru grupul de control la
având în vedere vechimea bolii precum şi bolile cronice
pacienţii de acelaşi sex este 3,20 la grupul control şi la
asociate. Aceste date au fost importante pentru
grupul H2 este de 9,68 (aproape de 3 ori mai mult).
cuantificarea riscului aterogenic şi cel al evenimentelor
Prin comparaţie se poate observa că indexul aterogenic
cardiovasculare pe care ulterior le-am introdus în
al plasmei, statistic, ne dă valori deosebit de semnificative
formulele de calcul al riscurilor.
faţă de celelalte formule de aterogeneză.
Raportul albumină/creatinină ne-a indicat valoarea
Valoarea AIP a fost cea mai mare pentru grupul H2
microalbuminuriei care, conform lui Boersa şi colab. se
(pacienţi cu hipertensiune gradul I/II, scăderea toleranţei
poate corela direct cu hipertensiunea arterială şi funcţia
la
glucoză, obezitate centrală, dislipidemie şi
renală. S-a dovedit că nivelul microalbuminuriei ne
microalbuminurie) indicând un risc de aterogeneză
indică vechimea hipertensiunii până în momentul
crescut, dar un scor QRisck mai mic (30,4%±1,95 ♀,
determinării precum şi eficienţa tratamentului
31,8%±2,75 ♂) faţă de grupul H4 unde sunt două boli
antihipertensiv, fiind reversibilă pentru pacienţii cu
cronice asociate pe langă hipertensiunea arterială, semn
valori mici ale microalbuminuriei semn că aparatul
că acest grup
(H4) poate dezvolta evenimente
glomerular nu este încă distrus, deci nu există o afectare
cardiovasculare în următorii
10 ani mai frecvent şi
renală marcată, pe când la pacienţii din grupurile H2,
într-un procent mai mare (42,5%±2,06 ♀ şi 44,2%±2,48
H3 si H4 valorile au fost mari, foarte semnificativ
♂). Însă procesul aterogenezei este mai activ la pacienţii
statistic faţă de grupul C indicând şi afectare renală, fapt
cu profilul lipidic foarte modificat cu valori foarte mari
dovedit şi de valorile estimative ale RFG, date
(H2) decât la pacienţii cu boli asociate, dar cu un profil
asemanatoare celor din literatură [13,15].
lipidic modificat cu valorii medii (H3, H4).
Rapoartele LDLc/HDLc şi CT/HDLc, potrivit lui
În concluzie, prin compararea fiecărui parametru
Grover şi colab. sunt bune predictoare pentru
important din studiul nostru, implicat în mod direct
evenimentele cardiovasculare viitoare, însă după Gotto
sau indirect în iniţierea sau întreţinerea aterogenezei
şi colab. care au realizat un studiu de 8 ani pe o populaţie
precum şi a bolilor cardiovasculare, pentru fiecare grup
predominat masculină, nivelul seric al TG poate
de pacienţi hipertensivi am reuşit să punem în evidenţă
reprezenta singur un factor de risc important pentru
importanţa AIP şi a scorului QRisck în practica medicală
evenimentele cardiovasculare viitoare [16,17].
a clinicianului, putând fi un instrument util şi economic
Studiile recente au indicat faptul că raportul dintre
pentru diagnosticarea, tratamentul şi prevenţia bolilor
TG/HDLc transformat logaritmic poate estima riscul
cardiovasculare cronice şi a evenimentelor cardiace
aterogenic mai bine decât toate celelalte. TG şi HDLc
majore (în special IM şi AVC).
Atherogenic Risk Quantification by Using the Atherogenic Index of Plasma (Aip) and Cardiovascular Risk
107
Calculator on Hypertensive Patients
Original articles
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
Referinţe
9.
Turen T. Hepatic lipase and HDL metabolism. Curr
Opin Lipidol 2000;11(3):277-83.
1.
Giner V, Poch E, Bragulat E, et al. Renin-angiotensin
10.
Njajou O, Kanaya AM, Holvoet P, Connelly S, Harris
system genetic polymorphisms and salt sensitivity in
T. Association between oxidized LDL-C, obesity and
essential hypertension. Hypertension
2000;35(1 Pt
type
2 diabetes. Diabetes Metab Res rev
2):512-7.
2009;25(8):733-9.
2.
Gibbons GH. Mechanisms of vascular remodeling in
11.
Libby P. Inflammation in atherosclerosis. Nature
hypertension: role of autocrine-paracrine vasoactive factors.
2002;420:868-74.
Curr Opin Nephrol Hypertens 1995;4(2):189-96.
12.
European guidelines on cardiovascular disease prevention
3.
Dzau VJ, Gibbons GH. Endothelium and growth
in clinical practice. European Society of Cardiology
factors in vascular remodeling of hypertension.
(2012).
Hypertension 1991;18(5 Suppl):III115-21.
13.
Boersma C, Maarten J, Visser ST, et al. Baseline
4.
Barton M, Dubey RK, Traupe T. Oral contraceptives
albuminuria predicts the efficacy of blood pressure-
and the risk of thrombosis and atherosclerosis. Expert
lowering drugs in preventing cardiovascular events. Br J
Opin Investig Drugs 2002;11(3):329-32.
Clin Pharmacol 2008;65(5):723-32.
5.
Fruchart JC, Kastelein JP, Duriez P. Atherosclerosis:
14.
Hippisley-Cox J, Coupland C, Vinogradova Y,
Evolving Vascular Biology and Clinical Implications
Robson J, Minhas R, Sheikh A. Predicting
New Risk Factors for Atherosclerosis and Patient Risk
cardiovascular risk in England and Wales: prospective
Assessment. Circulation 2004;109:III-15-III-19.
derivation and validation of QRISK2. BMJ
6.
Grundy S, Brewer B, Cleema J, Smith S, Lenfant C.
2008;336:a332.
Definition of Metabolic Syndrome NHLBI/AHA.
15.
Rodicio J, Campo C, Ruilope L. Microalbuminuria in
Conference Proceedings Report of the National Heart,
essential
hypertension.
Kidney
International
Lung, and Blood Institute/American Heart Association.
1998;54,S51-S54.
Circulation 2004;109:433-438.
16.
Grover S, Dorais M, Coupal L. Improving the
7.
MacMahon S, Robson R, Johnsona R. Use of the
prediction of cardiovascular risk: interaction between
Friedewald Formula to Estimate LDL-Cholesterol in
LDL and HDL cholesterol. Epidemiology
Patients with Chronic Renal Failure on Dialysis.
2003;14(3):315-20.
Clinical Chemistry 1997;43(11):2183-4.
17.
Gotto AM. Triglyceride; the forgotten risk factor.
8.
Ahmadi SA, Boroumand MA, Gohari-Moghaddam
Circulation 1998;97:1027-8.
K, Tajik P, Dibaj SM. Te impact of low serum
18.
Dobiasova M, Frohlich J. Te plasma parameter log
triglyceride on LDL-cholesterol estimation. Arch Iran
(TG/HDL-C- C) as an atherogenic index. Clin
Med 2008;11(3):318-21.
Biochem 2001;34:583-8.
108
Popa et al
Original articles
VARIAŢII ALE NIVELURILOR DE PENTOZIDINĂ LA PACIENŢI CU
POLIARTRITĂ REUMATOIDĂ ÎN STADIUL I-II ÎNAINTEA TRATAMENTULUI
Cojocaru Manole1, Ghinescu Minerva Claudia1, Rusu Elena1, Bălăeţ Constantin1, Cojocaru Inimioara Mihaela2
1Facultatea de Medicină, Universitatea Titu Maiorescu, Bucureşti, 2Universitatea de Medicină şi Farmacie Carol Davila,
Bucureşti
Adresa pentru corespondenţă:
Dr. Cojocaru Manole, EurClinChem
Strada Tomas Masaryk nr 5, Sector 2, Cod Poştal 020983
Bucureşti, România
E-mail: mancojocaru@yahoo.com
Primit: 15.01.2013
Acceptat: 20.02.2013
Med Con March 2013, Vol 8, No 1, 109-112
Rezumat
au fost semnificative
(limitele între
57,14-135,17
nmol/L, valoarea medie 129,4±10,5 nmol/L faţă de
Introducere: Recent, pentozidina, produs final al
subiecţii normali (limitele între 41,45-55,76 nmol/L,
glicării avansate
(AGE), a fost semnalat crescut în
valoarea medie
51,3±4,7 nmol/L; p<0,0001).
poliartrita reumatoidă (PR).
Şasesprezece
(39%) dintre pacienţii cu semne
Obiective: Să evaluăm pentozidina în serul
inflamatorii (CRP>40 mg/l) au prezentat concentraţia
pacienţilor cu PR stadiul I-II înaintea treatmentului şi
de pentozidină plasmatică mai crescută
(p<0,001).
să investigăm relaţia cu evoluţia clinică.
Aceasta s-a datorat în principal stresului oxidativ crescut
Materiale şi metode: S-au măsurat nivelurile de
şi întinderii procesului inflamator.
pentozidină în ser la pacienţi cu PR şi s-a examinat
Concluzii: În PR, există corelaţii semnificative între
relaţia dintre pentosidină şi evoluţia PR. Cercetarea s-a
pentozidină în ser şi proteina C reactivă şi viteza de
efectuat înaintea tratamentului la un grup de 41 pacienţi
sedimentare a eritrocitelor. Pentozidina în ser se asociază
cu PR în stadiul I-II cu vârsta între 28-65 ani. Nivelurile
cu activitatea inflamatorie sistemică din PR. Concentraţii
serice de pentozidină s-au evaluat la un grup de 24
mai crescute sau similare de pentozidină în ser
subiecţi normali între aceleaşi limite de vârstă şi care nu
comparativ cu lichidul sinovial indică că nivelurile
au prezentat semne de afecţiune reumatică. Nivelurile
crescute de pentozidină în ser în PR nu provin din
de pentozidină în ser au fost măsurate prin metoda
lichidul sinovial, ci există creşterea producerii de
HPLC directă cu membrane schimbătoare de ioni.
pentozidină în organism în PR. Pentozidina în ser este
Rezultatele au fost raportate ca media±DS cu
95%
un indicator superior pentru starea de PR.
limitele de încredere. Semnificaţia statistică s-a
Cuvinte cheie: Poliartrita reumatoidă înainte de
determinat cu testul Student t. Prevalenţele au fost
tratament, pentozidina, stres oxidativ
comparate folosind testul χ2. S-a folosit testul Fisher şi
regresia lineară. Pentru corelaţie s-au obţinut date
Pentozidina este unul dintre produşii finali de
folosind testul Pearson.
glicare avansată (AGEs). Pentozidina se formează prin
Rezultate: Pentozidina în ser a fost semnificativ mai
glicozilare secvenţială şi reacţii de oxidare. Prin urmare,
crescută în PR. La pacienţii cu PR stadiul I-II, înainte
există ipoteza că formarea pentozidinei este accelerată în
de tratament, creşterea nivelurilor de pentozidină în ser
boli determinate de stres oxidativ [1].
Changes of Serum Pentosidine Levels in Patients with Rheumatoid Arthritis Stage I-II Before Treatment
109
Original articles
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
Poliartrita reumatoidă
(PR) este o afecţiune
pentozidină în ser s-au exprimat în nmol/l. Ureea,
sistemică cronică, cu inflamaţia articulaţiilor şi
creatinina, glucoza, proteinele serice totale şi albumina
structurilor învecinate. În prezent există numeroase
s-au măsurat în ser imediat după recoltare prin metodele
dovezi pentru implicarea radicalilor liberi ai oxigenului
convenţionale cu autoanalizorul Hitachi 917.
în PR. Rolul radicalilor liberi în autooxidarea lipidelor
Semnificaţia statistică s-a determinat cu testul
biologice este cunoscut. Pacienţii cu PR prezintă niveluri
Student t. Prevalenţele au fost comparate folosind testul
serice scăzute de antioxidanţi, iar nivelul de antioxidanţi
χ2. S-a folosit testul Fisher şi regresia lineară. Pentru
scăzut este un factor de risc pentru PR. Din cauză că
corelaţie s-au obţinut date folosind testul Pearson.
stresul oxidativ şi radicalii liberi ai oxigenului joacă un
Semnificaţia statistică a fost pentru p<0,05.
rol semnificativ în distrugerea ţesuturilor şi inflamaţie în
PR, se consideră că pentozidina este implicată în această
Rezultate
afecţiune [2].
De mulţi ani, pentozidina s-a raportat ca fiind
Concentraţiile de pentozidină cresc paralel cu
crescută în cartilajul articular în PR. Totuşi, semnificaţia
vârsta. Totuşi, pentozidina serică nu prezintă corelaţie
acesteia în PR nu a fost investigată decât recent. În
semnificativă statistic cu vârsta în PR. Nivelurile de
prezent există numeroase studii care demonstrează că
pentozidină în ser au fost semnificativ crescute la
pentozidina este crescută la pacienţi cu PR. Pentozidina
pacienţii cu PR comparativ cu lotul martor (129,4±10,5
serică reflectă evoluţia clinică în PR. Cu toate că
nmol/l comparativ cu 51,3±4,7 nmol/l; p<0,0001).
nivelurile de pentozidină în lichidele oranismului s-au
Concentraţiile de pentozidină în serul pacienţilor
asociat cu activitatea bolii, nu este clar care niveluri de
cu PR s-au corelat semnificativ cu CRP, VSH. Nivelurile
pentozidină, ex. ser, lichidul sinovial sau urină reprezintă
de pentozidină în ser au fost semnificativ mai crescute la
un indicator superior. Dat fiind importanţa mare a
grupul cu evoluţie clinică mai gravă decât la grupul cu
reacţiilor de oxidare pentru formarea de pentozidină,
evoluţie clinică moderată (p<0,05). Şasesprezece (39%)
ipoteza studiului a fost glicooxidarea crescută, consecinţă
dintre pacienţii cu semne inflamatorii (CRP>40 mg/l)
a condiţiilor asociate cu stres oxidativ crescut în PR [3].
au prezentat concentraţia de pentozidină plasmatică mai
crescută
(p<0,001). A existat o corelaţie pozitivă
Materiale şi metode
semnificativă între pentozidina plasmatică şi CRP
(r=0,78; p<0,0001).
Studiul a cuprins 41 pacienţi cu PR în stadiul I-II,
Autorii au clasificat pacienţii în două grupe pe baza
înaintea tratamentului şi
24 martori sănătoşi între
nivelurilor de CRP. La pacienţii în puseu (CRP>40 mg/l),
aceleaşi limite de vârstă care nu au prezentat semne de
pentozidina plasmatică a fost semnificativ mai crescută
boală reumatismală. PR a fost diagnosticată conform
decât la pacienţii care nu erau în puseu, nivelurile de CRP
criteriilor Colegiului American de Reumatologie (ACR).
au fost corelate semnificativ cu nivelurile de pentozidină
Grupul cu PR a cuprins 35 femei şi 6 bărbaţi cu vârsta
plasmatică. Concentraţii de pentozidină plasmatică mai
între 28-65 ani (vârsta medie 61,0±13,0 ani). Pacienţii
crescute au fost în legătură cu inflamaţia. Astfel, creşterea
care au prezentat diabet zaharat şi cei cu niveluri
pentozidinei plasmatice în PR este probabil un marker
anormale ale ureei sau creatininei serice au fost excluşi
din lotul studiat. Grupul de martori a constat din 13
femei şi 11 bărbaţi cu vârste între 46-79 ani (vârsta
medie
62,7±10,6 ani). Nu a existat o diferenţă
semnificativă de vârste între pacienţii cu PR şi martori.
După recoltare, probele de sânge au fost centrifugate la
3000 turaţii/min, 15 min. Probele de ser au fost păstrate
la −20°C până la măsurarea pentozidinei. S-a obţinut
consimţământul informat de la toţi pacienţii.
Procedurile efectuate au fost în concordanţă cu
principiile Declaraţiei de la Helsinki din 1975, revizuite
în
1983. Proteina C-reactivă
(CRP) şi viteza de
sedimentare a hematiilor (VSH) au fost determinate
folosind metodele de rutină ale laboratorului.
Pentozidina s-a determinat prin metoda HPLC directă
Figura 1. Valoarea medie a concentraţiei de pentozidină serică
cu membrane schimbătoare ioni. Concentraţiile de
la pacienţi cu poliartrită reumatoidă comparativ cu lotul martor
110
Cojocaru et al
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
Original articles
util care prevede evoluţia severă. Rezultatele obţinute
cunoscut că produşii de oxidare în lichidul sinovial sunt
demonstrează că pentozidina poate să crească în absenţa
crescuţi în inflamaţie comparativ cu procesele
hiperglicemiei sau afectării funcţiei rinichiului.
degenerative ale articulaţiilor, la pacienţii cu PR
comparativ cu martorii. Proteinele
(şi aminoacizii)
Discuţii
crescute asociate cu accelerarea radicalilor liberi în
lichidul sinovial în PR stimulează reacţiile Maillard,
Autorii au măsurat nivelurile de pentozidină în serul
apoi cresc formarea de pentozidină în lichidul sinovial
pacienţilor cu PR în stadiul I-II înaintea tratamentului şi
în PR [3]. Nivelurile crescute de pentozidină în ser în
au analizat legătura dintre pentozidină şi evoluţia bolii.
PR nu derivă din lichidul sinovial, ci este crescută
Pentozidina este un produs al glicoxidării. Concentraţia de
producerea de pentozidină în sânge în PR. Creşterea de
pentozidină tisulară creşte paralel cu vârsta. Concentraţiile
radicali liberi în general este posibil să accelereze
de pentozidină cresc în diabetul zaharat, consecinţă a
formarea de pentozidină în PR [5].
hiperglicemiei [1]. Radicalii liberi sunt implicaţi în lezarea
În concluzie, pentozidina nu este un marker biochimic
ţesuturilor şi inflamaţie în PR, iar formarea pentozidinei se
al distrugerii articulaţiilor, însă este un marker al evoluţiei
asociază cu oxidarea. Totuşi, există puţine studii referitoare
PR. Sunt necesare studii care să demonstreze această
la pentozidină în PR. Mecanismele acestor fenomene sunt
observaţie. Rezultatele acestui studiu au arătat că nivelurile
încă neelucidate. Se cunoaşte că hiperglicemia cronică
de pentozidină în ser s-au corelat semnificativ cu ceilalţi
conduce la acumularea de produşi de glicozilare a
parametrii ai inflamaţiei. Totuşi pentozidina serică a fost
proteinelor derivaţi neenzimatic, cum este pentozidina în
un indicator superior pentru evoluţia PR. Substanţele din
diabetul zaharat [2].
lichidul sinovial pot direct să reflecte starea locală a
În PR, concentraţiile de pentozidină în ser sunt
articulaţiilor, precum inflamaţia şi degradarea articulaţiilor,
crescute; deşi nivelurile de glucoză sunt normale.
pentozidina este posibil să ajungă în lichidul sinovial din
Recent, interesul a fost concentrat pe potenţialul
circulaţia sanguină. Ca urmare, pentozidina serică este cel
proteinelor glicate ca sursă de radicali liberi
[3].
mai bun indicator al evoluţiei PR. Prezenţa concentaţiilor
Expunerea IgG şi altor proteine la radicalii de oxigen,
crescute de pentozidină în ser confirmă complexitatea
generaţi de fotoliză sau de un amestec de săruri de fier
acumulării de AGE. Toţi pacienţii cu PR incluşi în studiu
sau cupru şi peroxid de hidrogen, induce fluorescenţă
au fost normoglicemici şi au avut funcţia rinichiului
proteinei care nu se deosebeşte de formarea de bază
normală, dovedită de examenele clinice şi confirmată de
Schiff. Din cauză că formarea sa necesită condiţii de
nivelurile de creatinină şi uree sanguină. Explicaţia pentru
aerobioză, autorii sugerează că radicalii liberi ar putea să
formarea de pentozidină în PR este stresul oxidativ crescut.
explice căile posibile pentru evaluarea de pentozidină în
PR este o afecţiune autoimună care se asociază cu creşterea
PR. Fluorescenţa asociată proteinei, ex. pentozidina ar
stresului oxidativ [6].
putea să nu fie rezultatul glicemiei crescute, ci rezultatul
expunerii succesive la oxidarea indusă de radicalii liberi,
Concluzii
aceasta ar putea să fie importantă în evoluţia PR [4].
Autorii au semnalat observaţia că nivelurile de
Prezenţa unor concentraţii crescute de petozidină
pentozidină în ser sunt crescute în PR, precum şi
serică la pacienţii cu PR indică că acest compus nu este
importanţa în evaluarea evoluţiei clinice a PR, de
un marker simplu al glicozilării în diabet, dar poate fi
asemenea, autorii consideră că pentozidina crescută în
folosit ca marker general al stresului oxidativ în PR.
circulaţia sanguină provine de la nivelul articulaţiilor
Determinarea pentozidinei în PR este importantă în
inflamate în PR. Concentraţiile crescute de pentozidină
clinică. Pentozidina serică poate să ofere informaţii
ar putea fi observate, de asemenea, în condiţii patologice
despre perioadele active ale PR.
asociate cu stres oxidativ crescut. În acest studiu autorii
propun două căi posibile pentru creşterea de pentozidină
Conflict de interese: autorii care au luat parte la acest
în PR. O cale posibilă este că pentozidina este abundentă
studiu nu au nimic de declarat referitor la fonduri sau
în cartilaj comparativ cu alte ţesuturi, inflamaţia la
conflictul de interese privind manuscrisul.
nivelul articulaţiilor ar putea să inducă distrugerea
cartilajului, eliberarea de pentozidină în lichidul
sinovial; cealaltă cale este creşterea producerii de
Referinţe
pentozidină în lichidul sinovial. Se cunoaşte că
proteinele cresc în lichidul sinovial în articulaţiile
1. Sell DR, Monnier VM. End-stage renal disease and
inflamate sever, în special în PR. Este, de asemenea,
diabetes catalyze the formation of a pentose-derived
Changes of Serum Pentosidine Levels in Patients with Rheumatoid Arthritis Stage I-II Before Treatment
111
Original articles
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
crosslink from aging human collagen. J Clin Invest
with rheumatoid arthritis and osteoarthritis. Oxford
1990;85:380-4.
Journals Medicine Rheumatology 1999;38:1275-8.
2. Takahashi M, Suzuki M, Kushida K, Miyamoto S,
5. Chen JR, Takahashi M, Suyuki M, Kushida K,
Inoue T. Relationship between pentosidine levels in
Mizamoto S, Inoue T. Measurement of pentosidine in
serum and urine and activity in rheumatoid arthritis.
synovial fluid in patients with osteoarthritis and
Br J Rheumatol 1997;36:637-42.
rheumatoid arthritis: relationship with disease activity in
3. Rodriguez-Garcia J, Requena JR, Rodriguez-Segade
rheumatoid arthritis. J Rheumatol 1998;25:2440-4.
S. Increased concentrations of serum pentosidine in
6. Miyata T, Ishiguro N, Yasuda Y, et al. Increased
rheumatoid arthritis. Clin Chem 1998;44(2):250-5.
pentosidine, an advanced glycation end product, in
4. Chen JR, Takahashi M, Suzuki M, Kushida K,
plasma and synovial fluid from patients with rheumatoid
Miyamoto S, Inoue T. Comparison of the concentrations of
arthritis and its relation with inflammatory markers.
pentosidine in the synovial fluid, serum and urine of patients
Biochem Biophys Res Commun 1998;244:45-9.
112
Cojocaru et al
Original articles
ROLUL SANOGENETIC AL INTERVENŢIEI TERAPEUTICE ÎN CAZUL
POMPIERILOR SALVATORI
Popa Gabriela Sorina, Podea Delia, Puşchiţă Maria
Universitatea de Vest „Vasile Goldiş” Arad
Adresa pentru corespondenţă:
Psiholog Popa Gabriela Sorina
Telefon 0400752444227
Email: vancugabriela@yahoo.com
Primit: 14.01.2013
Acceptat: 25.02.2013
Med Con March 2013, Vol 8, No 1, 113-117
Rezumat
acestea 4 din cei 19 subiecţi au prezentat fie o stagnare,
fie o creştere a scorurilor, indicând absenţa unei
Obiectiv: Studiul prezent investighează eficienţa
ameliorări, sau chiar prezenţa unei creşteri a intensităţii
unui demers de intervenţie psihologică în cazul
simptomelor anxios-depresive.
pompierilor salvatori care prezintă simptome anxios-
Concluzii: Intervenţia de scurtă durată propusă de
depresive. Motivaţia studiului derivă din faptul că
noi a avut efecte pozitive în cele mai multe cazuri, 79%
activitatea psihologului din cadrul inspectoratelor
din totalul participanţilor. În cazurile în care intervenţia
pentru situaţii de urgenţă nu vizează doar monitorizarea
nu s-a dovedit eficientă urmează să continuăm demersul
modificărilor psihologice pe care le experientează
psihologic, cu acordul participanţilor.
pompierii, ci şi intervenţia psihologică preventivă sau
Cuvinte cheie: pompier salvator, incident critic,
terapeutică.
simptome anxios-depresive, intervenţie psihologică,
Material şi metode: Din totalul pompierilor
Scala de depresie Hamilton, Scala de anxietate Hamilton
salvatori evaluaţi periodic, am selectat un lot de
19
subiecţi care prezentau un nivel mai ridicat al
Introducere
simptomelor anxios-depresive, în vederea includerii lor
în cadrul unei intervenţii psihologice. Intervenţia a vizat
Prin natura activităţilor la care participă, personalul
aspecte cognitive: reformularea pozitivă a experienţelor,
de intervenţie din cadrul Inspectoratelor de Urgenţă,
aspecte emoţional-afective: conştientizarea şi acceptarea
personal numit în continuare, generic, pompieri
emoţiilor intense experientate şi un aspect
salvatori, este expus frecvent şi în mod constant la
comportamental: dezvoltarea de noi strategii de coping.
situaţii înalt stresogene cunoscute şi sub denumirea de
Intervenţia a constat din şase şedinţe. Evaluarea pre-
incidente critice. Un incident critic reprezintă un
intervenţie şi cea post-intervenţie a simptomelor anxios-
eveniment intens stresogen, care are capacitatea de a
depresive a fost efectuată cu Scala de depresie Hamilton
perturba semnificativ funcţionarea şi bunăstarea fizică şi
şi Scala de anxietate Hamilton.
psihică a celui care este expus evenimentului respectiv.
Rezultate: Per ansamblul lotului, scorurile la cele
Incidentul critic este stimulul care poate declanşa o stare
două scale au fost semnificativ mai scăzute la evaluarea
de criză şi disfuncţionalitate fizică şi psihică [1].
post-intervenţie, indicând o descreştere semnificativă a
Răspunsul la incidentele critice şi în definitiv la orice
intensităţii simptomelor anxios-depresive. Cu toate
situaţie stresogenă este determinat de caracteristicile
The Sanogenic Role of Therapeutic Intervention for Firefighters
113
Original articles
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
obiective ale situaţiei, de percepţia şi interpretarea
specifice inspectoratelor pentru situaţii de urgenţă din
subiectivă pe care fiecare individ o dă situaţiei, de starea
România, în baza scorurilor mai ridicate la Scala de
de sănătate fizică şi bunăstare psihică, de mecanismele de
depresie Hamilton şi Scala de anxietate Hamilton.
coping de care dispune, de o serie de factori psiho-
Selecţia subiecţilor supuşi intervenţiei din totalul
individuali, precum stabilitatea şi reactivitatea emoţională,
pompierilor salvatori evaluaţi periodic s-a efectuat pe
stima de sine, autoeficacitatea percepută, sentimentul de
criteriul obţinerii unui scor semnificativ clinic la cel
coerenţă, locusul controlului, dar şi de o serie de factori
puţin una din cele două scale.
psiho-sociali, unde putem include: contextul socio-
Lotul de 19 subiecţi a fost supus unei intervenţii
economic în care persoana derulează activitatea sa de
psihologice care a avut ca scop reducerea intensităţii
pompier salvator, răspunsul instituţional la situaţia
simptomelor anxioase şi depresive. Demersul a vizat
particulară, reprezentarea în mass-media, etc. [2,3,4].
următoarele aspecte: a) conştientizarea de către
Stresul generat de incidentele critice induce
participanţi a propriilor trăiri emoţional-afective şi a
modificări atât la nivel fiziologic, somatic, cât şi la nivel
răspunsului inadecvat la situaţiile stresante; b) deblocarea
psihologic, comportamental. La nivel fiziologic pot apare
emoţională şi confruntarea cu trăirile emoţionale
tulburări funcţionale precum tulburări cardiace,
intense; c) investigarea şi conştientizarea prezenţei unor
respiratorii, tulburări neuro-endocrine, mialgii, tulburări
repercursiuni negative ale răspunsului inadecvat la stres
somatoviscerale
[3]. La nivel psihologic pot apare
în viaţa personală a subiecţilor
(relaţiile de cuplu,
tulburări senzorio-perceptive, cognitive, afective, iar în
relaţiile familiale, relaţiile sociale); d) reformularea
cazuri severe chiar decompensări psihotice. Aceste
pozitivă a experienţelor intens stresogene; e) înlocuirea
tulburări pot fi reversibile sau ireversibile. O tulburare
strategiilor de coping mai puţin funcţionale, centrate pe
frecvent întâlnită la persoanele expuse frecvent la incidente
emoţii, cu strategii centrate pe soluţii şi probleme
critice este tulburarea de stres post-traumatic [4].
(strategii cu un grad mai ridicat de funcţionalitate).
Simptomele fizice includ: frisoane, sete, oboseală,
Intervenţia a avut loc pe durata a şase întâlniri
stări de leşin, vertij, greaţă, vărsături, cefalee, mialgii,
individuale cu fiecare din cei 19 subiecţi, respectând
puseuri hipertensive, dureri toracice, ritm cardiac
confidenţialitatea participanţilor. Cinci din cele şase
accelerat, tremor muscular. În general ele pot fi cuprinse
şedinţe au vizat câte unul din aspectele menţionate mai
în sintagma: reactivitate fiziologică ridicată. La nivel
sus, iar cea de a şasea şedinţă a constituit o sumarizare a
cognitiv sunt înregistrate confuzie, incertitudine, negare,
intervenţiei cu rol de feedback, în care am efectuat o
hipervigilenţă, dificultăţi de concentrare, dezorientări de
nouă reevaluare a simptomelor anxioase şi depresive cu
timp şi de loc, scăderea capacităţii decizionale. Sub aspect
cele două instrumente menţionate anterior.
emoţional-afectiv, simptomele cele mai frecvente se
Scala de depresie Hamilton este alcătuită din 17
referă la: stări anxioase, autoculpabilizare, panică,
itemi. Pentru 10 itemi, scorarea se face pe o scală în
agitaţie, iritabilitate, impulsivitate, depresie, furie,
cinci paşi, de la 0 la 4, iar pentru restul de 7 itemi,
angoasă, gânduri suicidare, răspunsuri emoţionale
scorarea se face pe o scală în trei paşi, de la 0 la 2. Scorul
inadecvate ca intensitate sau orientare, blocaj emoţional,
minim posibil este 0, iar scorul maxim 52. Scorurile
hiper sau hipoemotivitate. Iar la nivel comportamental
totale sub 7 indică absenţa depresiei. Scorurile cuprinse
semnalăm: retragerea socială, comportamente antisociale,
între 7 şi 17 indică o depresie uşoară. Scorurile cuprinse
consum de alcool şi alte substanţe, fuga psihogenă,
între 18 şi 24 indică o depresie moderată, iar scorurile
deteriorarea relaţiilor maritale şi familiale [4].
mai mari sau egale cu
25 indică un nivel sever al
depresiei.
Material şi metode
Scala de anxietate Hamilton este alcătuită din 14
itemi, cu scorare de pe o scală în 5 paşi, de la 0 la 4.
Studiul a fost efectuat pe un lot de 19 pompieri
Scorul maxim posibil este de 56. Un scor peste 20 indică
salvatori care prezintă anumite simptome depresive şi
prezenţa unei anxietăţi de intensitate clinică.
anxioase. Subiecţii sunt de gen masculin, cu vârste
Analiza statistică: datele au fost centralizate şi
cuprinse între 27 şi 42 de ani, vârsta medie fiind de 29
prelucrate cu programul statistic SPSS for Windows 10.
de ani, cu o abatere standard de 3,77 ani. Vechimea în
Pentru a investiga diferenţele apărute la nivelul scorurilor
activitatea de pompier salvator a participanţilor este
la anxietate şi depresie între cele două momente ale
cuprinsă între 6 şi 10 ani, cu o medie de 6,42 ani şi o
evaluării, am utilizat testul statistic t Student pentru
abatere standard de 0,96 ani. Subiecţii au fost selectaţi
eşantioane perechi, designul statistic al cercetării fiind
din lotul total al pompierilor salvatori evaluaţi periodic,
unul bifactorial intrasubiecţi. Toţi cei
19 subiecţi
conform normelor sănătăţii şi securităţii în muncă
evaluaţi iniţial au fost supuşi evaluării finale.
114
Popa et al
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
Original articles
Rezultate
efectuat cu testul t Student pentru eşantioane perechi,
scorurile având o distribuţie normală, pentru ambele
Evaluarea iniţială
scale şi ambele momente ale evaluării. Rezultatele la
Scorurile la scala de depresie, la evaluarea iniţială, pe
anxietate indică un t(18)=3,511 la p=0,002, iar la
lotul de subiecţi supuşi intervenţiei, variază între 7 şi 9,
depresie, t(18)=5,524 la p<0,001. Indicele de
cu o medie de 7,84 şi abaterea standard de 0,69. La scala
magnitudine r ia valorile 0,637 pentru anxietate şi 0,793
de evaluare a anxietăţii, pre-intervenţie, subiecţii au
pentru depresie.
obţinut scoruri cuprinse între 9 şi 17, cu media de 11 şi
abaterea standard de 2. Subiecţii prezintă un nivel scăzut
Discuţii
al depresiei, dar nu absent, motiv pentru care au fost
selectaţi în lotul supus intervenţiei. Intensitatea
Observăm că valorile lui t, atât pentru anxietate cât
simptomelor de anxietate nu este de nivel clinic, dar ele
şi pentru depresie, sunt semnificative statistic la un prag
sunt asociate cu simptomele depresive de intensitate
inferior lui
0,05 ceea ce ne permite să afirmăm că
scăzută, cele două împreună constituind factor de risc.
intensitatea simptomelor depresive, cât şi a celor
Evaluarea la finalizarea intervenţiei
anxioase, scade semnificativ în urma intervenţiei. Astfel,
La finalizarea intervenţiei s-a efectuat o nouă
intervenţia noastră şi-a atins scopul, acela de a ameliora
evaluare a simptomelor depresive şi anxioase. Rezultatele
disfuncţiile emoţional-afective prezentate iniţial de către
obţinute la scala de anxietate indică un scor mediu de
subiecţi. În cazul anxietăţii, intervenţia explică circa
9,26 şi o abatere standard de 1,97, scorurile variind
64% din varianţa scorurilor pre-intervenţia comparativ
între 6 şi 13. La scala de depresie, scorurile obţinute
cu cele post-intervenţie, iar în cazul depresiei, procentul
variază între
4 şi 9, valoarea medie fiind de 6,42 şi
explicat de intervenţie se ridică la 79. Aşadar, intervenţia
abaterea standard de 1,39. Constatăm o scădere a mediei
în cinci paşi pe care am propus-o pare a da rezultate
scorurilor atât la anxietate, cât şi la depresie.
semnificative în ameliorarea simptomatologiei anxios-
Comparaţia scorurilor pre-intervenţie cu a celor
depresive a pompierilor salvatori.
post-intervenţie, atât la anxietate cât şi la depresie, s-a
Analizând scorurile post-intervenţie, pentru fiecare
subiect în parte, constatăm că în cazul a 16 subiecţi din
totalul de 19, scorurile la depresie au scăzut comparativ
cu cele pre-intervenţie. În cazul a doi subiecţi scorurile
au stagnat, iar în cazul unui singur subiect scorul a
crescut de la 8 la 9, nefiind aşadar vorba de o creştere
dramatică. La scala de anxietate,
15 subiecţi au
înregistrat scoruri mai scăzute post-intervenţie, un
subiect a obţinut un scor identic, iar
3 subiecţi au
înregistrat scoruri mai ridicate post-intervenţie
comparativ cu cele pre-intervenţie.
În cazurile în care scorurile la scalele de anxietate sau
depresie au stagnat sau chiar crescut, intenţionăm a
continua intervenţia atât pentru a ameliora simptomele
Figura 1. Mediile scorurilor la scala de anxietate
anxios-depresive ale pompierilor, cât şi pentru a identifica
posibilele cauze care au favorizat lipsa de succes a
intervenţiei. Menţionăm că pe durata intervenţiei
pompierii au continuat să participe la intervenţii.
De asemenea, pentru a identifica posibile noi
strategii de intervenţie apare ca necesară investigarea şi a
altor variabile psiho-individuale care influenţează
răspunsul pompierilor la stresul generat de expunerea
frecventă şi constantă la incidente critice, variabile
precum stima de sine, percepţia stresului, potenţialul de
dezvoltare pozitivă post-traumatică, autoeficacitatea
percepută, robusteţea, optimismul, sentimentul de
coerenţă, tendinţa spre somatizare, tendinţa spre
Figura 2. Mediile scorurilor la scala de depresie
dezvoltarea de cogniţii raţionale versus iraţionale [2].
The Sanogenic Role of Therapeutic Intervention for Firefighters
115
Original articles
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
În studiul prezent pornim de la o situaţie concretă
mecanism de coping care face foarte probabilă dezvoltarea
întâlnită în activitatea curentă cu pompierii salvatori.
sindromului de stres post-traumatic. Un studiu asupra
Aceştia sunt frecvent expuşi la incidente critice.
răspunsului diferenţiat la stres al femeilor comparativ cu
Evenimentele care sunt percepute de pompierii salvatori
bărbaţii [8] a arătat că femeile tind să iniţieze interacţiuni
ca incidente critice includ: accidentarea propriei
sociale când sunt stresate, în timp ce bărbaţii, în situaţii
persoane, riscul pierderii propriei vieţi, accidentarea sau
intens stresante, tind să se izoleze, să reducă nivelul
moarte unui coleg, intervenţia asupra victimelor aflate
interacţiunilor sociale. Autorii cerectării consideră că
în agonie, mai ales dacă acestea sunt copii, participarea
aceste diferenţe s-ar datora unui efect neuro-endocrin
la intervenţii în care victimele sunt persoane cunoscute
cumulat prin asocierea pozitivă a acţiunii oxitocinei,
ale salvatorului. Toate acestea au un impact major asupra
hormonilor reproducători femini şi a mecanismelor
bunăstării psihice şi fizice a salvatorului. Cu toate că
opioide endogene, potenţând, în cazul femeilor,
pregătirea lor tehnică de bază reduce intensitatea
comportamentele pro-sociale, în timp ce la bărbaţi
răspunsului negativ, ea nu-l poate elimina. Astfel, rolul
testosteronul tinde să blocheze sau să reducă acţiunea
psihologului în acest context este de a monitoriza
oxitocinei, potenţând acţiunea sistemului adrenergic şi
periodic bunăstarea psihică a pompierilor salvatori, de a
implicit pe cea a unui răspuns specific de fugă sau luptă.
interveni punctual prin defusing, debriefing, sau chiar
E foarte probabil ca în anumite cazuri în care blocajele
printr-o intervenţie de mai mare amploare, intervenţie
emoţionale ale pompierilor salvatori sunt conectate cu
cu valenţe terapeutice prestabilite.
convingerea că recunoaşterea distresului generat de
Defusingul presupune o întâlnire individuală,
expunerea frecventă la incidente critice ar putea genera
scurtă, pe bază de voluntariat şi în condiţii de
reacţii negative din partea colegilor sau superiorilor,
confidenţialitate, care are ca prim scop detensionarea
abordarea noastră centrată şi pe acceptarea şi conştienizarea
psihică şi fizică a salvatorului. Ea trebuie să aibă loc
propriilor experienţe să nu fie foarte eficientă. Considerăm
foarte aproape de momentul incidentului, recomandat
că în aceste cazuri am putea să ne axăm mai mult pe
ar fi la un interval de 4 ore, dar nu mai mult de 12 ore
dezvoltarea de strategii de coping funcţionale, pe orientarea
de la incident şi nu trebuie să fie excesiv de formală, ba
clientului spre activităţi alternative generatoare de emoţii
chiar se recomandă a fi mai degrabă informală [4].
şi dispoziţii afective pozitive [9].
Defusingul este axat pe conştientizarea şi acceptarea
propriilor trăiri ca fiind normale şi pe rolul adaptativ sau
Concluzii
inadaptativ al acţiunilor intreprinse post-eveniment.
Debriefingul este o întâlnire mai formală, realizată în
Studiul nostru arată că o intervenţie psihologică de
cadrul grupului celor care au luat parte la incidentul
scurtă durată, axată pe obiective concrete, pe probleme
respectiv, la un interval de 24-72 de ore de la eveniment şi
şi soluţiile acestora, pe reformularea pozitivă a
se centrează pe diferitele modalităţi de reacţie la stres [4].
experienţelor, fără a neglija conştientizarea şi acceptarea
Cercetările din domeniul psihologiei clinice şi a
din partea clientului a răspunsurilor emoţionale intense
sănătăţii arată că cele mai indicate tipuri de intervenţii
în situaţiile puternic stresogene specifice incidentelor
în cazul pompierilor salvatori sunt cele de scurtă durată,
critice, cât şi a consecinţelor acestor reacţii asupra
centrate pe problemă şi pe soluţii [4,5].
propriei persoane, dar şi a celor din jur (familie, colegi,
Actvitatea de pompier salvator este caracterizată de
prieteni), poate duce la o ameliorare semnificativă a
prezenţa unui puternic stereotip masculin [6], ceea ce
simptomelor anxios-depresive. Cu toate acestea, există şi
îngreunează semnificativ activitatea psihologului consilier
cazuri în care acest demers nu reuşeşte, iar cauzele
prin aceea că abordarea directă a laturii emoţional-afective
acestor nereuşite trebuie căutate atât în particularităţile
a răspunsului individual la incidentele critice poate fi
psihologice ale clientului, cât şi în natura demersului
percepută ca impunerea un model străin lui, rezultând o
psihologic. Diversitatea abordărilor psihoterapeutice şi a
reacţie de rezistenţă faţă de consilier, de evitare a solicitării
tehnicilor şi strategiilor psiho-educative fac posibilă o
consilierii. Este mult mai indicată o abordare centrată pe
mare varietate de strategii de intervenţie.
aspecte comportamentale, practice, concrete.
Subiecţii de gen masculin au dificultăţi în a vorbi
deschis despre sentimente, emoţii şi stări dispoziţionale.
Referinţe
Evitarea propriilor emoţii şi trăiri afective este firească,
dar nu reprezintă un bun mecanism de coping. Această
1. Burns, C., Rosenberg, L. Redifining critical incidents:
confruntare necesită efort conştient, implicare din partea
a preliminary report. International Journal of
clientului. McFarlane [7] arată că evitarea este un slab
Emergency Menthal Health, 2001;3 (1),17-24.
116
Popa et al
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
Original articles
2. Băban, A. Stres şi personalitate. Editura Presa
and challenges for wives of firefighters. Family Relations:
Universitară Clujeană, Cluj-Napoca, 1998.
Interdisciplinary Journal of Applied Family Studies
3. Iamandescu, I.-B. Stresul psihic din perspectivă
2005;54(3),423-35.
psihologică şi psihosomatică. Editura Info Medica,
7. McFarlane, A. Avoidance and intrusion in posttraumatic
Bucureşti, 2002.
stress disorder.
Journal of Nervous and Mental
4. Maier, R. Stres, stres, stres. Editura Gutenberg Univers,
Diseases 1992;180,439-45.
Arad, 2011.
8. Taylor, S.E., Klein, L.C., Lewis, B.P., Gruenenwald,
5. Holdevici, I. Psihoterapia anxietăţii. Abordări cognitiv-
T.L., Gurung, R.A.R., Updegraff, J.A. Biobehavioral
comportamentale. Editura Dual Tech, Bucureşti,
responses to stress in females: tend-and-befriend not fight-
2002.
or-flight. Psychological Review 2000;107(3),411-29.
6. Regehr, C., Dimitropoulos, G., Bright, E., George,
9. Holdevici, I. Psihologia succesului. Autosugestie şi
S., and Henderson, J. Behind the brotherhood: Rewards
relaxare. Editura Universitară, Bucureşti, 2010.
The Sanogenic Role of Therapeutic Intervention for Firefighters
117
Medical Connections/Conexiuni Medicale
Declaraţia de conflict de interese
Medical Connections/Conexiuni Medicale (Med Con) solicită tuturor autorilor şi recenzorilor să declare
orice conflict de interese care ar putea interveni în contribuţiile lor.
Conflictul de interese pentru un anumit manuscris există atunci când un participant în procesul de
recenzie inter pares (peer review) şi de publicare -autor, referent, sau editor- are legături cu activităţi care
l-ar putea influenţa necorespunzător pe el sau judecata lui, indiferent dacă aceasta este sau nu afectată.
Relaţiile financiare cu industria medicală, de exemplu prin muncă salarială, consultanţă, deţinere de
acţiuni, onorarii, testimoniale ca şi expert, fie direct, fie prin intermediul familiei, sunt de obicei considerate
a fi cele mai importante conflicte de interese. Cu toate acestea, pot apărea conflicte din alte motive, cum ar
fi relaţiile personale, concurenţa academică şi implicarea intelectuală.
Încrederea publicului în procesul de revizuire inter pares şi credibilitatea articolelor publicate depinde
în parte de cât de bine este administrat posibilul conflict de interese în timpul redactării, recenziei inter
pares şi a luării deciziilor editoriale. Părtinirea poate fi de multe ori identificată şi eliminată prin atenţia
crescută asupra metodelor ştiinţifice şi concluziilor lucrării. Relaţiile financiare şi efectele lor sunt mai uşor
de identificat decât alte conflicte de interese. Participanţii la peer review şi în procesul de publicare trebuie
să-şi dezvăluie posibilele conflictele de interese, iar informaţiile trebuie să fie puse la dispoziţie, astfel încât
şi alţii să poată aprecia aceste efecte pentru ei înşişi.
Autori: atunci când trimit un manuscris sau o scrisoare, autorii sunt responsabili pentru recunoaşterea
şi divulgarea conflictelor financiare şi altor conflicte de interese care ar putea să le influenţeze activitatea. Ei
trebuie să recunoască în manuscris orice sprijin financiar pentru activitate, precum şi orice alte legături
financiare sau personale în munca lor.
Recenzorii: evaluatorii externi inter pares trebuie să dezvăluie editorilor orice conflicte de interese care
le-ar putea părtini opiniile asupra manuscrisului şi ar trebui să se recuze de la recenzia anumitor manuscrise
în cazul în care cred că este oportun. Editorii trebuie să fie conştienţi de posibilele conflicte de interese ale
recenzorilor în interpretarea recenziilor şi trebuie să judece pentru ei dacă recenzorul ar trebui să fie recuzat.
Recenzorii nu trebuie să utilizeze informaţiile în munca lor, înainte de publicare, pentru a-şi promova
propriile interese.
Titlul manuscrisului: _ _______________________________________________________
Declar că nu există conflict de intereseI declare no conflict of interest
Declar că există următoarele conflicte de interese potenţiale:
_ _________________________________________________________________________
_ _________________________________________________________________________
_ _________________________________________________________________________
_ _________________________________________________________________________
_ _________________________________
_ _________________________________
Nume
Semnătura/Data
Vă rugăm trimiteţi acest formular semnat pe fax sau mail la sediul editorului Med Con.
Fax: +40-261-710456
Email: colmedsm@gmail.com
GENERAL REVIEW
RELAŢIA DINTRE MUTAŢIILE TP53 ŞI FGFR3 ÎN CANCERUL VEZICAL
SUPERFICIAL
Prunduş Paul¹, Stanca Vasile Dan², Nicolescu Sergiu¹, Coman Ioan²
¹Departamentul de Urologie al Spitalului Clinical Municipal Cluj Napoca, România, ²Universitatea de Medicină şi
Farmacie „Iuliu Haţieganu” Cluj-Napoca
Adresa pentru corespondenţă:
Paul Prunduş
Departamentul de Urologie al Spitalului Clinical Municipal Cluj-Napoca, Romania
Email: prunduspaul@yahoo.com
Primit: 02.12.2012
Acceptat: 15.02.2013
Med Con March 2013, Vol 8, No 1, 119-124
Rezumat
ocupă locul şapte în cazul bărbaţilor şi locul 17 în rândul
femeilor, cu o incidenţă de 30 cazuri/100.000 în Europa.
Cancerul vezical reprezintă una dintre cele mai frecvente
Potrivit estimărilor SEER (Surveillance Epidemiology
malignităţi la nivel mondial, fiind o patologie a vârstnicilor,
and End Results) din cadrul NCI (National Cancer
cu un maxim al incidenţei în decada a şasea de viaţă.
Institute), în 2007 au fost diagnosticaţi 67.160 pacienţi
Tumorile care sunt invazive prezintă un risc crescut de
cu cancer vezical (50.040 bărbaţi şi 17.120 femei) în
progresie în ciuda cistectomiei radicale sau a altor
SUA. Numărul deceselor în 2007 a fost de aproximativ
tratamente. Se fac eforturi pentru identificarea markerilor
13.750.
cu rol în prevederea recurenţei şi progresiei tumorale, a
În perioada 2000-2004 vârsta medie la diagnosticul
răspunsului la tratament şi în ceea ce priveşte supravieţuirea.
cancerului de vezică urinară a fost de
73 de ani.
Tumorile vezicale se dezvoltă pe căi moleculare
Aproximativ 0,1% din pacienţi au fost diagnosticaţi sub
patogenetice diferite. Rezultatele recente sugerează faptul
vârsta de 20 de ani, 0,6% între 20 şi 34 de ani, 2,1%
că activarea mutaţiei genei receptorului 3 al factorului de
între 35 şi 44 de ani, 7,8% între 45 şi 54 de ani, 17,2%
creştere al fibroblaştilor (FGFR3) poate fi considerată ca
între 55 şi 64 de ani, 28,5% între 65 şi 74 de ani, 31,9%
şi marker pentru calea patogenică „papilară” cu prognostic
între 75 şi 84 de ani, 11,8% peste 85 de ani. Incidenţa
bun, în opoziţie cu calea patogenică a „carcinomului in
adaptată la vârstă a fost de 21,1 cazuri la 100.000 de
situ” (CIS), mult mai agresivă. Supraexpresia P53 la nivel
bărbaţi şi femei/an [1,2,3].
nuclear, detectată cu ajutorul tehnicilor de
Mai mult de 90% dintre cancerele de vezică sunt
imunohistochimie, este privită ca şi un marker surogat
carcinoame care se prezintă în diverse stadii evolutive.
pentru mutaţia P53, acesta fiind cel mai studiat marker
Sistemul curent de stadializare a tumorilor vezicale are la
molecular în cancerul vezical în ultima decadă.
bază examenul histopatologic şi este bazat pe revizia din
Cuvinte cheie: cancer vezical, gena FGFR3,
2002 a clasificării UICC (International Union Against
proteina p53, mutaţii genetice, progresie tumorală
Cancer).
Tumorile vezicale superficiale sunt reprezentate de:
Introducere
tumorile Ta (papilare, în general de grad tumoral redus,
care nu invadează structurile situate dincolo de
Cancerul vezical reprezintă una dintre cele mai
membrana bazală), carcinomul in situ (CIS- tumoră
frecvente malignităţi la nivel mondial. Ca prevalenţă
plană, de grad înalt, care în general nu invadează
Relationship Between TP53 and FGFR3 Mutations in Superficial Bladder Cancer
119
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
membrana bazală) şi tumorile T1 (care invadează ţesutul
La om, familia factorilor de creştere a fibroblaştilor
conjunctiv subepitelial, dar care respectă musculara
cuprinde 18 membri (FGFs) şi 4 factori omologi ai FGFR
proprie). În opoziţie, cancerul vezical infiltrativ defineşte
(FHFs), mulţi dintre aceştia având un rol crucial în cadrul
tumorile care au invadat cel puţin detrusorul vezical
proceselor fiziologice, cum ar fi embriogeneza, dezvoltarea,
(pT2, pT3, pT4) [4].
vindecarea plăgilor şi o serie de condiţii patologice. Efectele
În cazul tumorilor vezicale superficiale 30% dintre
FGF sunt mediate de o familie de patru receptori de
pacienţi nu vor prezenta recurenţe tumorale, însă 70%
creştere a fibroblaştilor
(FGFR1-4). FGFRs sunt
vor avea cel puţin o recidivă tumorală; 10-20% dintre
glicoproteine transmembranare cu o structură având o
cazuri vor prezenta progresie la boala infiltrativă. La
porţiune
extracelulară
cu două-trei
domenii
prezentare, între 70% şi 80% dintre tumorile vezicale
imunoglobulină-like IgI-III, un domeniu transmembranar
sunt superficiale (70% pTa şi 30% pT1) [5].
şi un altul tyrosine-kinazic intracelular [12].
Tumorile vezicale pTa şi pT1 demonstrează diferenţe
Gena care codifică receptorul 3 al factorului de
substanţiale în ceea ce priveşte potenţialul lor de progresie
creştere a fibroblaştilor aparţine receptorilor tirozin-
la invazie musculară. Progresia apare în doar 3% dintre
kinazici. Familia FGFR cuprinde mai mulţi membri,
tumorile pTa, în timp ce procentul ajunge la 30% pentru
aceştia participând la reglarea proliferării celulare,
pT1 [6]. Riscul de progresie este strâns corelat cu
migrarea şi diferenţierea celulelor în timpul
mortalitatea: sub 1% pentru tumorile pTa, în timp ce
embriogenezei şi cu rol în repararea tisulară. Expresia
pentru tumorile pT1 este de 24% [7,8,9].
inadecvată a genelor factorilor de creştere fibroblastici
Genetica în cancerul vezical
poate contribui la patogenia cancerului vezical fie prin
O perspectivă cu totul nouă şi promiţătoare este
alterarea angiogenezei, fie prin efect de stimulare directă
oferită de evaluarea substratului genetic al tumorilor
a celulelor tumorale. Factorii de creştere fibroblastici îşi
vezicale. Deşi termenul de „tumori vezicale superficiale”
exercită funcţionalitatea prin patru receptori (FGFR1-
include pTa, pT1 şi CIS, în lumina datelor genetice
4). Mai multe dovezi susţin că activarea mutaţiei FGFR3
curente, această subdiviziune este total nepotrivită
este responsabilă pentru rolul ei oncogen în apariţia
întrucât substratul lor genetic este diferit; acest lucru le
cancerului urotelial. Mutaţiile FGFR3 sunt specifice
dictează şi comportamentul diferit în ceea ce priveşte
cancerului urotelial, unde pot să apară în peste 40%
capacitatea de invazie şi metastazare. Tumorile care au
dintre tumori [13,14].
penetrat membrana bazală (pT1) şi CIS sunt leziuni de
Supraexpresia proteinei FGFR3 a fost mai frecvent
risc înalt, în opoziţie cu pTa, care tind să recidiveze, dar
prezentă în cazul tumorilor uroteliale bine diferenţiate
nu progresează. La baza acestui comportament diferit se
comparativ cu cele prost diferenţiate, respectiv în stadiu
pare că stau diferenţele în ceea ce priveşte mutaţiile
tumoral scăzut comparativ cu stadiile avansate tumorale.
genetice cauzatoare.
Aceste observaţii confirmă ipoteza potrivit căreia extresia
Există dovezi clinice şi moleculare pentru existenţa a
FGFR3 are rol în dezvoltarea precoce a neoplaziei
două căi de progresie şi dezvoltare a cancerului vezical:
uroteliale [15].
calea CIS şi calea Ta. CIS progresează în aproximativ
Studii clinice ample au stabilit faptul că mutaţiile
50% dintre cazurile de tumori în stadiul T1 şi apoi
FGFR3 apar la aproximativ 50% dintre tumorile de
devin tumori musculo-infiltrative [10,11].
tract urinar superior şi inferior, în special la nivelul a trei
Mutaţiile FGFR3 în tumorile vezicale superficiale
puncte distincte la nivelul exonilor 7, 10 şi 15. Cele mai
Tumorile pTa de grad redus (G1-G2) au puţine
frecvente mutaţii la nivelul exonului 7 şi 10 sunt S249C
alteraţii moleculare. În ciuda eforturilor multor
(~61%), Y375C (~19%), R248C (~8%) şi G372C
laboratoare care au testat sute de tumori, au fost descrise
(~6%), alte modificări apărând cu o frecvenţă mult mai
doar 2 alteraţii: deleţii ale cromozomului 9 şi mutaţii ale
redusă (<2%) [16].
FGFR3 (receptorul
3 al factorului de creştere a
Studiile din literatură au demonstrat supraexpresia
fibroblaştilor).
proteinei FGFR3 prin metoda imunohistochimică la
În plus, tumorile pTa de grad redus sunt foarte
83% dintre tumorile pTa, 100% în cazul tumorilor pT1
stabile genetic. Studierea unor tumori sincrone sau
şi
50% în cazul tumorilor pT2. Totodată, mutaţia
metacrone de la acelaşi pacient a pus în evidenţă faptul
FGFR3 a fost prezentă la 64-74% din cazurile de tumori
că prezentau aceleaşi alterări genetice. Pierderea
pTa, 0-21% în cazul tumorilor pT1 şi 0-16% în cazul
heterozigoticităţii cromozomului 9 este evenimentul cel
tumorilor pT2.
mai puţin divergent în timp, pe când mutaţia FGFR3
Aceste date indică faptul că expresia FGFR3 este mai
este identificată cu frecvenţă semnificativă doar în
frecventă decât mutaţia activatoare a genei. Această
tumorile vezicale.
diferenţă dintre supraexpresia proteinei şi mutaţia
120
Prunduş et al
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
GENERAL REVIEW
activatoare a genei, în special în cazul tumorilor pT1,
Expresia FGFR3 este semnificativ asociată cu doi
naşte bănuiala existenţei unui alt mecanism de
factori prognostici importanţi: stadiul şi gradul, expresia
supraexpresie proteică, altul decât activarea genei [17,18].
proteinei nu reprezintă un factor predictiv independent
Frecvenţa mutaţiilor FGFR3 scade odată cu
pentru recurenţă şi progresia tumorilor pTa/pT1.
creşterea stadiului şi gradului tumoral: 65% în cazul
Mutaţiile TP53 în cancerul vezical superficial
pTa, 30,2% în cazul pT1, 11,5% în cazul pT2-4 şi
Tumorile pT1 au un substrat genetic mult mai
69,8% în cazul gradului G1, o rată similară pentru
variat. Au fost identificate mutaţii ale genelor p53,
gradul G2 (68%) şi 18,6% în cazul gradului G3. Aceste
ERBB2, PTEN, deleţii ale cromozomilor 8p, 11p, 3p,
evidenţe pentru stadiu şi grad tumoral sunt înalt
18q, 4q, etc. Semnificativ este însă faptul că diferenţele
semnificative (p<0,0001 şi respectiv p<0,0001). Pentru
genetice dintre tumorile minim invazive (pT1) şi cele
tumorile pTa, cea mai comună dintre cele patru posibile
mai profunde (pT2-4) sunt minime, sugerând faptul că
grupe
(FGFR3 tip sălbatic plus TP53 tip sălbatic,
tumorile care au abilitatea de a trece prin membrana
FGFR3 tip sălbatic plus mutaţia TP53, mutaţia FGFR3
bazală a epiteliului sunt leziuni agresive [23].
plus TP53 tip sălbatic, mutaţia FGFR3 plus mutaţia
Gena p53 este o genă supresoare tumorală, localizată
TP53) au fost tumorile cu mutaţia FGFR3 şi TP53 tip
pe braţul scurt al cromozomului 17. Mutaţia aceastei
sălbatic (61,9% dintre cazuri), urmate de tumorile cu
gene este relativ frecventă în patologia tumorală umană,
ambele mutaţii FGFR3 şi TP53 tip sălbatic (31,5%
fiind prezentă la aproximativ
50% din totalul
dintre cazuri) [19].
malignităţilor. Funcţia p53 este una foarte complexă -
Statusul mutaţiilor FGFR3 a fost investigat ca şi
este considerată „gardianul genomului” cu rol în reglarea
marker prognostic pentru supravieţuire, recurenţă şi
ciclului celular, repararea ADN-ului şi apoptoza celulară.
progresie tumorală. Un studiu de talie mică, care a
Supraexpresia genei p53 este asociată cu gradul şi stadiul
inclus un număr de 53 de cazuri de tumori vezicale în
tumoral, aceasta având o valoare predictivă independentă
stadiul pTaG1-2, a arătat faptul că tipul sălbatic al
în cazul recurenţelor tumorale. În ciuda multiplelor
mutaţiei FGFR3 este predictiv pentru recurenţa bolii
studii, rolul p53 în managementul pacienţilor cu cancer
[20]. În opoziţie, un studiu de talie mare care a inclus
vezical este încă insuficient cunoscut şi astfel utilizarea
764 de cazuri de tumori vezicale superficiale, a relevant
curentă a mutaţiei acestei gene în practica curentă este
faptul că mutaţia FGFR3 a fost predictivă pentru
oarecum limitată.
recurenţă în cazul tumorilor TaG1 şi nu în cazul
Mutaţia p53 în cancerul vezical este detectată prin
tumorilor TaG3 sau T1 [21].
reacţia de polimerizare în lanţ
(PCR) şi analiza
Fauceglia şi colab. în urma unui studiu
imunohistochimică. Sidransky şi colab. au detectat
concluzionează faptul că mutaţia genei FGFR3
mutaţia genei p53 în 11 cazuri din 18 pacienţi cu cancer
reprezintă un indicator puternic pentru o rată redusă de
vezical, Fujimoto şi colab. au detectat mutaţii în 7 din
recurenţă în cazul tumorilor uroteliale pTa. Totodată,
23 de cazuri de tumori vezicale, iar Spruck şi colab. au
nu a fost găsită o valoare prognostică a supraexpresiei
detectat mutaţia genei la 29 de pacienţi din totalul de
proteice a FGFR3 în predicţia recurenţei sau progresiei
80 [14,24].
tumorale - asta datorită şi urmăririi relativ reduse a
Mai mult, nu au fost observate diferenţe între
pacienţilor (12 luni) [14].
alteraţiile genetice ale tumorilor pT1 şi ale metastazelor
Junker şi colab. în urma unui studiu care a cuprins
acestor tumori [22]. Mutaţia FGFR3 pare să definească
100 de pacienţi diagnosticaţi cu tumoră vezicală au
tumorile superficiale, în timp ce mutaţia p53 este
regăsit mutaţia FGFR3 la
48,9% dintre aceştia.
caracteristică tumorilor care depăşesc membrana bazală;
Frecvenţa apariţiei mutaţiei în funcţie de stadiul tumoral
aceste alteraţii par însă să se excludă reciproc.
T a fost: pTa- 61%, pT1- 40%, pT2/3- 0%. Mutaţia
Hernandez şi colab. într-un studiu efectuat pe serii
FGFR3 este semnificativ asociată cu gradul de
mari de pacienţi având cancer vezical, sugerează că
diferenţiere tumorală: G1- 70%, G2- 46%, G3- 4%. În
mutaţiile FGFR3 și TP53 au constituit evenimente
cazul tumorilor pTaG1, mutaţia a fost regăsită în 72%
independente în tumorile pT1G3 precum şi în cazul
din cazuri. Aceste rezultate confirmă faptul că mutaţia
tumorilor pTa, pT1G2 şi a celor cu invazie în musculară
FGFR3 caracterizează tumorile non-invazive de grad
(pT≥2). În schimb, mutaţiile FGFR3 şi TP53 nu au
redus, reprezentând un marker prognostic important
constituit evenimente independente dacă se iau în
pentru tumorile vezicale cu potenţial redus, putând
considerare toate tumorile, fără a se ţine cont de stadiu
reprezenta un marker surogat pentru detecţia tumorilor
şi grad (tumorile pT1G2 and pT1G3) [24].
vezicale genetic stabile cu rezultate clinice şi oncologice
Nu există o asociere dovedită între expresia proteinei
bune [22].
FGFR3 şi p53. Supraexpresia proteinei FGFR3C/p53K
Relationship Between TP53 and FGFR3 Mutations in Superficial Bladder Cancer
121
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
reprezintă o cale favorabilă în carcinogeneza vezicală şi
Variabiliatea mutaţiilor FGFR3 şi TP53 atunci când
supraexpresia singulară a FGFR3 este improbabilă în a
toate tumorile pT1 sunt considerate împreună, reflectă
avea valoare predictică în cazul tumorilor vezicale
cele două căi patogenetice de dezvoltare a cancerului
[13,25,26].
vezical, Figura 1 [21].
Existenţa multifocalităţii tumorale vezicale, volumul
O mare proporţie dintre cancerele vezicale prezintă
tumoral peste
3 cm, coexistenţa CIS, răspunsul la
fenotipul de tip sălbatic (altele decât mutaţiile FGFR3
tratamentul chimioterapic intravezical, existenţa
sau TP53):
32% dintre tumorile Ta,
40% dintre
recurenţelor precoce şi cel mai important, gradul
tumorile T1 şi 43% dintre tumorile T2-4. Aceste tumori
histologic al tumorii vezicale, sunt variabile care luate
probabil au alte mutaţii decât FGFR3 sau TP53, dar cu
individual sau colectiv ne furnizează informaţii privind
un efect similar (activarea semnalizării căii patogenice
prognosticul tumorilor vezicale, în special în stadiul T1
FGFR3 în cazul tumorilor de grad redus Ta şi mutaţiile
(25-30% din tumorile vezicale stadiul T1 prezintă
genelor cauzând instabilitate genetică în cazul tumorilor
progresie cu prinderea muscularei după 2 ani şi acest
de grad înalt sau stadiu crescut). Mutaţiile RAS, care au
procent creşte la 40% în cazul tumorilor vezicale T1G3)
fost observate la aproximativ
10% dintre cancerele
[27].
vezicale şi niciodată găsite asociate cu mutaţia FGFR3,
În stadiile tumorale precoce pTaG1 şi pTaG2,
par să fie implicate în calea patogenică a FGFR3
frecvenţa mutaţiei FGFR3 a fost crescută în cazul
[28,29].
tumorilor de grad redus Ta, mutaţia TP53 fiind redusă.
În 2006, Sylvester şi colab. au publicat o metodă de
Dacă aceste tumori progresează spre invazie musculară,
predicţie a recurenţei şi progresiei în cazul fiecărui
ele vor prezenta mutaţia TP53 cu o frecvenţă similară cu
pacient, care a permis medicilor să determine terapia
cea a tumorilor CIS. Pentru tumorile Ta, frecvenţa
adjuvantă cea mai utilă pentru pacienţi după efectuarea
mutaţiilor TP53 pare să crească gradual odată cu stadiul
rezecţiei endoscopice. Date de la 2596 de pacienţi cu
tumoral, de la pTa (5% dintre tumori) la pT1 (mutaţiile
tumori vezicale stadiul Ta, T1, sau Tis au fost utilizate
TP53 în 27% dintre tumori) şi pT2-4 (mutaţiile TP53
pentru dezvoltarea unui index prognostic.
în 42% dintre tumori).
Variabilele care reprezentau rata de recurenţă
Gradul tumoral pare de asemenea să fie important,
anterioară, numărul de tumori, mărimea tumorii,
frecvenţa mutaţiei TP53 a fost regăsită în 17% dintre
stadiul T, gradul şi prezenţa carcinomului in situ (CIS),
tumorile pT1G2 şi 37% în cazul tumorilor pT1G3.
au fost incluse în modelul multivariabil final pentru
Frecvenţa mutaţiei FGFR3 a fost regăsită ca fiind
stabilirea timpului până la prima recurenţă şi a timpului
similară cu cea în cazul tumorilor pTa G1/G2 şi pT1G2,
de progresie [30].
sugerând faptul că majoritatea tumorilor pT1G2 derivă
O metaanaliză privind relaţia dintre mutaţiile
din calea patogenică Ta mai degrabă decât din cea CIS.
FGFR3 şi TP53 în cancerul vezical a demonstrat faptul
că mutaţiile FGFR3 şi TP53 apar independente atunci
când stadiul şi gradul tumoral sunt luate în considerare.
Frecvenţa mutaţiei TP53 a fost crescută în cazul
tumorilor pT1G3 şi pT2-4, indiferent de prezenţa sau
absenţa mutaţiilor FGFR3 în aceste tumori. Mutaţiile
TP53 pot apărea în cazul tumorilor Ta când aceste
tumori progresează. Tumorile vezicale de diferite grade
şi aflate în diferite stadii, au caracteristici fenotipice şi
genotipice specifice. Deşi recunoaşterea unor modificări
moleculare prin analiza ţesuturilor tumorale, a urinei şi
a probelor de sânge este posibilă, puţini dintre aceşti
markeri moleculari sunt utilizaţi în practica clinică. Sunt
necesare studii în vederea stabilirii acurateţei acestor
markeri genetici şi posibilitatea utilizării lor pe scară
largă, cu scopul de a îmbunătăţi tratamentul cancerului
vezical. Utilitatea clinică a markerilor moleculari deja
descoperiţi nu poate fi determinată până când mai multe
studii prospective multicentrice vor stabili eficacitatea,
siguranţa şi valoarea predictivă a acestora în
Figura 1. Activarea FGFR3 şi mutaţia TP53: cele două căi
monitorizarea pacienţilor cu cancer vezical.
patogenetice ale dezvoltării diferite a cancerului vezical
122
Prunduş et al
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
GENERAL REVIEW
În ultimul timp, mutaţiile FGFR3 şi TP53 joacă un
11.
4. Billerey C, Chopin D, Aubriot-Lorton MH, Ricol
rol important în dezvolatarea cancerului vezical care
D, Gil Diez de Medina S, et al. Frequent FGFR3
promit ca şi ţinte terapeutice, instrumente de screening
mutations in papillary non-invasive bladder
(pTa)
şi diagnostic, precum şi biomarkeri prognostici.
tumors. Am J Pathol 2001;158:1955-9
Viitoarele provocări includ rafinarea testelor de screening
12.
di Martino E, Darren C, Tomlinson M, Knowles A. A
şi prognostic bazate pe mutaţia FGFR, identificarea de
Decade of FGF Receptor Research in Bladder Cancer:
markeri pentru a selecta cel mai probabil pacienţii care
Past, Present, and Future Challenges. Adv Urol
să beneficieze de terapiile ţintite asupra FGFR şi
2012;2012:429213.
dezvoltarea strategiilor pentru depăşirea recurenţelor
13.
Mhawech-Faucegliaa P, Cheneya RT, Fischerb G,
după tratament, sau dezvoltarea de rezistenţă tumorală.
Becka A, Herrmannb FR. FGFR3 and p53 protein
Rezultatele cercetării privind rolul FGFR3 şi TP53 în
expressions in patients with and pT1 urothelial bladder
cancerul vezical trebuie tradus şi aplicat în managementul
cancer. EJSO 2006;(32),231-7.
clinic al pacienţilor diagnosticaţi cu această afecţiune.
14.
Takahashi T, Habuchi T, Kakehi Y, et al. Clonal and
chronological genetic analysis of multifocal cancers of the
bladder and upper urinary tract. Cancer Res
Referinţe
1998;58(24):5835-41.
15.
Kimura T, Suzuki H, Ohashi T, Asano K, Kiyota H,
1.
Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer
Eto Y. Te incidence of thanatophoric dysplasia mutations
statistics, 2002. CA Cancer J Clin 2005;55:74-108.
in FGFR3 gene is higher in low-grade or superficial
2.
Murta-Nascimento C, Schmitz-Dräger BJ, Zeegers
bladder carcinomas. Cancer 2001;92:2555-61.
MP, et al. Epidemiology of urinary bladder cancer: from
16.
vanRhijn BWG, Montironi R, Zwarthoff EC, Jöbsis
tumour development to patient’s death. World J Urol
AC, van der Kwast TH. Frequent FGFR3 mutations in
2007;25:285-95.
urothelial papilloma. Te Journal of Pathology
3.
Jemal A, Tiwari RC, Murray T, et al. Cancer statistics,
2002;198(2):245-51.
2004. CA Cancer J Clin 2004;54(1):8-29.
17.
Gomez-Roman JJ, Saenz P, Cuevas Gonzalez J,
4.
Burger M, van der A MNM, van Oers JMM,
Escuredo K, Santa Cruz S, Junquera C, et al.
Brinkmann A, van der Kwast TH et al. Prediction of
Fibroblast growth factor receptor 3 is overexpressed in
Progression of Non-Muscle-Invasive Bladder Cancer by
urinary tract carcinomas and modulates the neoplastic
WHO 1973 and 2004 Grading and by FGFR3
cell growth. Clin Cancer Res 2005;11:459-65.
Mutation Status: A Prospective Study. European
18.
Matsumoto M, Ohtsuki Y, Ochi K, Seike Y, Iseda N,
Urology 2008;54,835-44.
Sasaki T, et al. Fibrosblast growth factor receptor
3
5.
Donat SM. Evaluation and follow-up strategies for
protein expression in urothelial carcinoma of the urinary
superficial bladder cancer. Urol Clin North Am
bladder, exhibiting no association with low-grade and/or
2003;30(4):765-76
non-invasive lesions. Oncol Rep 2004;12:967-71.
6.
Heney NM, Ahmed S, Flanagan MJ, et al. Superficial
19.
Yann N et al. A Meta-Analysis of the Relationship
bladder cancer: progression and recurrence. J Urol
between FGFR3 and TP53 Mutations in Bladder
1983;130(6):1083-6.
Cancer. PLoS One 2012;7(12):e48993
7.
Abel PD. Follow-up of patients with
„superficial”
20.
vanRhijn BWG, Lurkin I, Radvanyi F, Kirkels WJ,
transitional cell carcinoma of the bladder: the case for a
van der Kwast TH, Zwarthoff EC. Te fibroblast
change in policy. Br J Urol 1993;72(2):135-42.
growth factor receptor 3 (FGFR3) mutation is a strong
8.
Herr HW, Wartinger DD, Fair WR, Oettgen HF.
indicator of superficial bladder cancer with low
Bacillus Calmette-Guerin therapy for superficial
recurrence rate. Cancer Research 2001;61(4):1265-8.
bladder cancer: a
10-year followup. J Urol
21.
Hernández S, López-Knowles E, Lloreta J, et al.
1992;147(4):1020-3.
Prospective study of FGFR3 mutations as a prognostic
9.
Jeremy L, Abe PD. Treatment Options in Superficial
factor in nonmuscle invasive urothelial bladder
(pTa/pT1/CIS) Bladder Cancer. In: Urological cancers
carcinomas.
Journal
of
Clinical
Oncology
in clinical practice, Springer-Verlag, London Limited,
2006;24(22):3664-71.
2007,75-102.
22.
Junker K, Zwarthoff E, Van Oers J, Kania I, Schubert
10.
Spruck CH 3rd, Ohneseit PF, Gonzalez-Zulueta M,
J. Low Frequency of chromosomal alterations in CGH
Esrig D, Miyao N, et al. Two molecular pathways to
analysis in low-risk papillary bladder tumours with
transitional cell carcinoma of the bladder. Cancer Res
FGFR3 mutations. European Urology Suppliment
1994;54:784-8.
2006;5(2):77.
Relationship Between TP53 and FGFR3 Mutations in Superficial Bladder Cancer
123
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
23. Knowles MA. Molecular Biology of Bladder Cancer. in J
expression as prognostic factors for cancer
- related
Waxman. Urological Cancers, Springer, 2005;115-30.
survival in stage T1 transitional cell bladder carcinoma.
24. Hernández S, López-Knowles E, Lloreta J, Kogevinas
European Urology 2002;(41)182-9.
M, Jaramillo R, et al. FGFR3 and Tp53 mutations in
28. Wu XR. Urothelialtumorigenesis: a tale of divergent
T1G3 transitional bladder carcinomas: independent
pathways. Nat Rev Cancer 2005;5:713-25.
distribution and lack of association with prognosis. Clin
29. Jebar AH, Hurst CD, Tomlinson DC, Johnston C,
Cancer Res 2005;11:5444-50.
Taylor CF, et al. FGFR3 and Ras gene mutations are
25. Kawasaki T, Tomitaa Y, Watanabea R, Tanikawaa T,
mutually exclusive genetic events in urothelial cell
Kumanishi T, Satoa S. mRNA and protein expression of
carcinoma. Oncogene 2005;24:5218-25.
~53 mutations in human bladder cancer cell lines.
30. Sylvester RJ, van der Meijden AP, Oosterlinck W, et
Cancer Letters 1994;(82)113-21
al. Predicting recurrence and progression in individual
26. Hovey RM, Chu L, Balasz M et al. Genetic alterations
patients with stage Ta T1 bladder cancer using EORTC
in primary bladder cancers and their metastases. Cancer
risk tables: a combined analysis of 2596 patients from
Res 1998;58(16):3555-60
seven EORTC trials. EurUrol
2006;49:466-77
27. Alonso AR, Fernandez SP, Carrero JG. p53 and ki67
(discussion 475-7).
124
Prunduş et al
GENERAL REVIEW
ETIOLOGIA ASTIGMATISMULUI POSTOPERATOR APĂRUT DUPĂ
CHIRURGIA CATARACTEI
Pop Rodica1, Pop Radu2
1Ambulatorul Integrat al Clinicii de Boli Infecţioase Cluj-Napoca, 2Clinica Oftalmologică Cluj-Napoca
Address for correspondence:
Dr. Pop Rodica
Str. Mestecenilor, Nr. 3, Bloc 9L, Sc. II, Et. 4, Ap. 19, Cod 400348, Cluj-Napoca, Jud. Cluj
Tel: 0723147278
E-mail: pop_rodica_1957@yahoo.com
Primit: 10.12.2012
Acceptat: 20.02.2013
Med Con March 2013, Vol 8, No 1, 125-130
Rezumat
efectuat numeroase studii privind astigmatismul
postoperator după operaţia de cataractă, la început
Astigmatismul postoperator după chirurgia
legate de extracţia intracapsulară şi mai târziu de
cataractei depinde în principal de preexistenţa acestuia,
extracţia extracapsulară. Începând cu 1982, în cadrul
de factori care ţin de actul operator, precum şi de
chirurgiei cataractei s-a trecut la practicarea extracţei
caracteristicele pseudofakului. De-a lungul timpului au
extracapsulare cu implantare de lentilă intraoculară.
existat numeroase studii, legate în principal de efectele
Progresele înregistrate treptat în această tehnică
cicatrizării corneene asupra curburii acesteia precum şi a
chirurgicală au permis apoi introducerea şi utilizarea pe
stabilităţii ei refractive. Un rol important în apariţia
scară tot mai largă a extracţiei cataractei prin metoda
acestui tip de astigmatism îl are tipul inciziei chirurgicale:
facoemulsificării şi implantare de cristalin artificial
suturată sau nesuturată, mărimea, adâncimea şi locaţia
foldabil.
acesteia. În zilele noastre, incizia nesuturată, în cornee
Astigmatismul indus operator este astigmatismul
clară, este cel mai frecvent utilizată în tehnica extracţiei
mai mare de 1 dioptrie, conform sau contrar regulei,
cataractei prin metoda facoemulsificării. Îmbunătăţirile
care este prezent la
6-8 săptămîni postoperator
[2].
aduse în ultimul timp chirurgiei cataractei urmăresc o
Această formă de astigmatism poate compromite
bună vindecare şi remodelare a plăgii, care să asigure
rezultatul funcţional după chirurgia cataractei,
stabilitatea refractivă a corneei.
determinând creşterea astigmatismului postoperator.
Cuvinte cheie: astigmatism postoperator, incizie în
Factorii etiologici care pot fi asociaţi astigmatismului
cornee clară, stabilitate refractivă
postoperator sunt: astigmatismul preoperator şi factori
care ţin de operație.
Introducere
Astigmatismul preoperator
Obiectivul major al chirurgiei cataractei este un
rezultat funcţional bun, cu o acuitate vizuală optimă,
Astigmatismul preoperator de valoare mare se poate
fără corecţie optică.
asocia cu valori crescute ale astigmatismului postoperator
Donders (1864) a fost primul care a arătat faptul că
după chirurgia cataractei [3]. Studiile au arătat faptul că
alterarea curburii corneene este o consecinţă neplăcută a
aproximativ 15-29% din pacienţii care suferă o operaţie
chirurgiei cataractei
[1]. De-a lungul timpului s-au
de cataractă au mai mult de 1,5 dioptrii astigmatism
Etiology of Postoperative Astigmatism after Cataract Surgery
125
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
preexistent [4]. Reducerea acestui tip de astigmatism în
Materialul de sutură folosit. Schimbările în curbura
cursul chirurgiei cataractei poate îmbunătăţi rezultatul
corneană, după chirurgia cataractei, în caz de plăgi
vizual postoperator, mai ales atunci când urmează a fi
operatorii suturate, diferă în funcţie de materialul de
implantat un cristalin artificial multifocal. Astfel,
sutură folosit, rezorbabil sau nerezorbabil. După Jaffe şi
valoarea corectată a astigmatismului în timpul operaţiei
Clayman [13], principalii factori responsabili de aceste
de cataractă trebuie să fie egală cu suma vectorilor
schimbări sunt dehiscenţa plăgii care apare în caz de
astigmatismului preexistent şi a astigmatismului indus
suturi cu fire rezorbabile şi compresia care apare în
operator [5].
suturile cu fire nerezorbabile. S-au efectuat studii
Corectarea astigmatismului preexistent poate fi
comparative pe ochi operaţi de cataractă cu suturi
realizată în timpul chirurgiei cataractei prin tehnici de
monofilament şi cu suturi cu fire de mătase naturală,
incizie, cum ar fi manipularea acestora pentru aplatizarea
considerînd importante relaţiile dintre schimbările în
meridianului cornean mai refringent, sau prin
curbura corneană după îndepărtarea monofilamentului,
implantarea de cristalin artificial toric. Ambele metode
precum şi după biodegrabilitatea firului de mătase [14].
pot reduce un astigmatism mic până la moderat [6].
Astfel, în caz de suturi cu monofilament, puterea şi axul
După alţi autori, astigmatismul preoperator poate fi
cilindrului au fost constante cât timp firele de sutură au
corectat în timpul chirurgiei cataractei, folosind diferite
rămas pe loc. După îndepărtarea acestora, astigmatismul
metode care includ incizii periferice relaxante, alegerea
postoperator s-a redus simţitor, datorită reducerii
locaţiei inciziei, implantare de cristalin artificial toric
tensiunii produsă în plagă prin suturile monofilament.
[7,8].
În caz de suturi rezorbabile, valoarea şi axul cilindrului
Astigmatismul indus de operaţie: poate fi corelat
au variat, vindecarea asociindu-se şi cu o reacţie
cu mai mulţi factori, cum ar fi: factori care ţin de incizie
inflamatorie locală.
şi factori care ţin de pseudofak.
Adâncimea plăgii. Procesul de vindecare a plăgilor
Factori care ţin de incizie
corneene implică celulele epiteliale şi fibroblastele în
Tipul plăgii - suturată sau nesuturată. În cazul plăgii
segmentul anterior şi celulele endoteliale în segmentul
suturate, astigmatismul postoperator este dependent de
posterior [15]. Prin studii efectuate la om şi la maimuţă,
lungimea, etanşeitatea şi adâncimea suturii [9]. Astfel,
în caz de plăgi nesuturate, s-a observat faptul că
suturile lungi, plasate aproape unele faţă de altele,
morfologia cicatricei tisulare diferă în funcţie de
creează o compresiune tisulară, conducând la
adâncimea plăgii [11]. Astfel, în regiunile anterioare s-a
astigmatism conform regulei. Suturile larg separate,
găsit o restaurare precoce, aproape anatomică,
precum şi cele mai puţin etanşe, determină un
pseudolamelară, în timp ce regiunile posterioare au fost
astigmatism contrar regulei. Suturile prea superficiale
dezorganizate. Aceste diferenţe regionale de vindecare
tind să se elimine spontan, conducând la astigmatism
s-ar datora unor factori mecanici locali, cum ar fi
contrar regulei. În plăgile suturate, atât timp cât firele de
eliminarea dopului de fibrină, sau unor proprietăţi
sutură sunt pe loc, valoarea astigmatismului postoperator
intrinseci de vindecare diferite între straturile stromale.
rămâne constantă, iar după îndepărtarea lor acest
Localizarea inciziei în raport cu limbul. Inciziile în
astigmatism indus de suturi se elimină [10].
operaţia de cataractă pot fi: sclerale, limbice sau corneene
Pe de altă parte, studiile au arătat faptul că pe aceeaşi
[16].
cornee, plăgile suturate şi nesuturate reprezintă modele
Incizia sclerală este denumită şi tunel scleral.
de vindecare diferită
[11]. Astfel, plăgile suturate se
Deoarece este situată posterior, minimalizează
vindecă iniţial mai încet, dar obţin o continuitate
deformarea corneană care este stabilizată de inelul
pseudolamelară în timp. În schimb, plăgile nesuturate se
limbic, rezultînd un astigmatism postoperator minim.
caracterizează printr-o vindecare precoce, aproximativ
Un alt avantaj este faptul că este etanşă, se autoînchide,
lamelară, dar poate fi urmată de o regenerare ulterioară
deci nu necesită sutură, dar atunci când este mai puţin
ineficace a cicatricei.
performantă determină astigmatism postoperator.
Gradul de strângere a suturilor. Acesta este un alt
Astigmatismul postoperator este cu atât mai mic cu cât
factor identificat a fi responsabil de astigmatismul
incizia este mai sclerală.
postoperator. O sutură largă permite corneei să se
Incizia limbică se poate efectua în partea anterioară
turtească, cu reducerea curburii în meridianul vertical şi
a limbului, de-a lungul corneei, în partea mijlocie sau în
astigmatism contrar regulei. Dacă sutura este prea
partea posterioară, de-a lungul sclerei. Inciziile localizate
strânsă, ea întinde cornea vertical, crescând curbura în
în partea anterioară se cicatrizează mai lent, în timp ce
acest meridian şi cauzînd astigmatism conform regulei
inciziile situate posterior necesită sutură, cu apariţia
[12].
unui astigmatism postoperator.
126
Pop et al
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
GENERAL REVIEW
Incizia corneană se face fără implicarea conjunctivei
prima, urmată de cea oblică care deschide camera
sau a sclerei, fiind denumită şi incizie în cornee clară.
anterioară. Necesită sutură, cu posibilitatea apariţiei
Aceasta determină o reacţie inflamatorie minimă, nu
astigmatismului postoperator. Un alt procedeu al
necesită diatermie, evitându-se astfel coagularea fibrelor
acesteia este incizia corneană inversă - se efectuează în
de colagen. Atunci când este de dimensiune mică
cornee transparentă, la 1-2 mm în faţa limbului, având
(aproximativ 3 mm) astigmatismul postoperator este
forma unei muşcături de flaut şi o etanşeitate
minim, perioada de vindecare şi recuperare este scurtă.
considerabilă. Plaga este mică, deci astigmatismul
În acest sens, datele din literatură arată faptul că incizia
postoperator este minim [20].
de 2,8 mm în cornee clară induce mici modificări
Incizia în trei planuri se referă la tunelul scleral. În
refractive, cel puţin în ochii cu astigmatism cornean
această abordare se efectuează întâi o incizie
preoperator mic, indiferent de locul inciziei [17]. Acest
perpendiculară în zona sclerală, se disecă apoi spaţiul
tip de incizie se recomandă doar în caz de implantare de
intralamelar în direcţie orizontală, pentru ca în final
cristalin artificial foldabil. Nu este recomandată în caz
camera anterioară să fie penetrată printr-o incizie oblică.
de implantare de cristalin artificial de polymethyl
Această incizie este de obicei utilizată în tehnica
methacrylate (PMMA), când plaga operatorie trebuie să
facoemulsificării. Are ca avantaj o bună etanşeitate şi
fie egală sau mai mare de 5 mm, deoarece astigmatismul
autosigilare, mai ales în cazul plăgilor mici. Aceste
postoperator este greu de prevenit. S-au efectuat studii
caracteristici
asigură un bun control asupra
comparative asupra astigmatismului postoperator prin
astigmatismului postoperator.
incizie în cornee clară şi incizie limbică posterioară [18],
Dimensiunea inciziei. În ultimul timp, reducerea
constatându-se că la aceeaşi mărime a inciziei, 2,2 mm,
dimensiunii inciziei a reprezentat o preocupare
locaţia limbică posterioară induce un astigmatism
importantă pentru mulţi chirurgi de cataractă. Totodată,
semnificativ mai mic şi mai puţin variabil (0,25±0,14)
utilizarea pe scară tot mai largă a facoemulsificării
comparativ cu incizia în cornee clară (0,69±0,49). O
precum şi dezvoltarea implantelor de cristalin foldabil
incizie mai corneană determină un astigmatism mai
au permis incizii tot mai mici în chirurgia cataractei. În
important şi conform regulei, iar o incizie mai sclerală
zilele noastre, tehnica standard pentru chirurgia
determină un astigmatism mai mic şi invers regulei [19].
cataractei în lumea industrializată, este îndeplinită
Deşi studiile au demonstrat că inciziile limbice şi sclerale
printr-o incizie de aproximativ
3 mm. Reducerea
induc mai puţin astigmatism decât cele în corne clară,
mărimii inciziei induce un astigmatism mai mic după
în cazul inciziilor mici efectul locaţiilor este mai puţin
chirurgia cataractei. În acest sens, s-a demonstrat faptul
important [17]. Din acest considerent, în zilele noastre
că o incizie mai mică poate manipula cornea mai blând
cele mai comune incizii efectuate în chirurgia cataractei
şi cu stres minim asupra ţesuturilor adiacente, furnizând
prin facoemulsificare sunt cele în cornee clară, înlocuind
rezultate optice mai bune
[21,22]. Micşorarea
astfel tunelul scleral şi incizia limbică.
dimensiunii inciziei corneene de la peste 3 mm la mai
Tipul inciziei. Din punct de vedere al planurilor în
puţin de 2 mm a dus la reducerea astigmatismului indus
care este efectuată incizia, aceasta poate fi de trei feluri
chirurgical şi a aberaţiilor corneene [21,22].
[16]: într-un singur plan, în două planuri şi în trei
Referitor la locaţiile inciziilor în raport cu limbul,
planuri.
studiile arată faptul că nu există diferenţe semnificative
Incizia întrun singur plan poate fi perpendiculară pe
în magnitudinea astigmatismului postoperator, dacă
limb, se efectuează în general la nivelul limbului anterior.
acestea sunt efectuate în cornee clară sau scleral, atunci
Vindecarea acestui tip de incizie este lentă şi necesită
când este vorba de incizii mici. Astfel, un studiu italian
sutură. Alt procedeu al acesteia este incizia limbică
a comparat inciziile în cornee clară de aceeaşi lungime
oblică ab-externă; a fost mult utilizată în ultimele decade
efectuate temporal şi inciziile tunelizate, efectuate
în cazul extracţiei extracapsulare a cataractei. Se face în
superior, la ora
12. Gradul astigmatismului a fost
general la nivelul regiunii mijlocii a limbului, planul
asemănător, dar meridianele au fost diferite [23].
inciziei fiind de 110° faţă de planul corneei. Dezavantajul
După cum s-a menţionat, în zilele noastre, incizia
acestor două tipuri de incizii este necesitatea suturii, cu
mică corneană, nesuturată, este preferată de majoritatea
apariţia unor astigmatisme postoperatorii mari [20].
chirurgilor de cataractă. Se cunoaşte faptul că suprafaţa
Incizia în două planuri poate fi limbică angulată; se
anterioară a corneei este principalul element refractiv al
poate efectua la orice nivel al limbului, fie cornean, fie
ochiului, contribuind la mai mult de 2/3 din puterea sa
scleral. Incizia se face în două planuri, unul perpendicular
refractivă
[24]. Astfel, este important de a elimina
şi altul la
110° faţă de suprafaţa corneei. De regulă
efectele inciziei corneene asupra calitatii sale optice. În
incizia perpendiculară până la adîncimea medie se face
ultimul timp, tendinţa spre microincizii corneene (de
Etiology of Postoperative Astigmatism after Cataract Surgery
127
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
aproximativ 2 mm), care să asigure o bună restaurare
Factori care ţin de pseudofak
anatomică şi stabilitate refractivă a corneei, a caracterizat
Existenţa pe piaţă a unei game foarte variate de
evoluţia chirurgiei cataractei. Comparativ cu inciziile
implante artificiale de cristalin artificial face dificilă
stadard, avantajele microinciziilor sunt un astigmatism
decizia chirurgului de a alege un anumit tip, la un
postoperator mai mic şi mai puţine iregularităţi
anumit pacient. Această cerinţă poate fi îndeplinită prin
corneene, cu implicaţii favorabile asupra acuităţii vizuale
alegerea unei lentile artificiale foldabile, care să poată fi
şi a reabilitării precoce. În acest sens s-a demonstrat că
implantată printr-o microincizie corneană, cu un
inciziile de
2,2 mm şi 1,8 mm utilizate în chirurgia
astigmatism postoperator minim.
cataractei prin facoemulsificare sunt neutre astigmic
Factorii care pot induce astigmatism postoperator şi
[21]. Se pare că limita de 2 mm incizie în cornee clară
care ţin de pseudofak sunt: poziţia implantului artificial
este optimă pentru inducerea unor schimbări optice
de cristalin de cameră posterioară, materialele din care
nesemnificative în cornea umană, după chirurgie [25].
sunt confecţionate implantele artificiale de cristalin,
Locaţia inciziei în funcţie de meridian. Astigmatismul
mărimea părţii optice, forma şi mărimea hapticelor şi
postoperator în chirurgia cataractei poate varia şi în
designul implantului artificial de cristalin.
funcţie de meridianul pe care este plasată incizia. Datele
Poziţia implantului artificial de cristalin de cameră
din literatură arată faptul că inciziile mici, superioare
posterioară. Implantarea cristalinului artificial de cameră
afectează mai mult curbura corneană decât inciziile
posterioară în sacul capsular este metoda optimă în
similare, temporale [26]. Mai multe explicaţii au fost date
majoritatea cazurilor operate de cataractă [32]. Poziţia
în acest sens. Astfel, se ştie despre corneea umană că este
pseudofakului în sacul capsular poate afecta
cu aproximativ 1 mm mai lată decât mai înaltă [27]. O
astigmatismul postoperator în chirurgia cataractei. Sunt
incizie superioară poate fi deci uşor mai aproape de apexul
bine cunoscute schimbările refractive induse de rotirea
cornean decât o incizie temporală, având un efect mai
pseudofakului şi deplasarea sa longitudinală
[4].
pronunţat asupra curburii centrului corneei. Incizia
Descentrările posterioare sunt cele mai frecvente şi pot
temporală este mai departe de axul vizual şi orice aplatizare
avea cauze multiple [33]: alterarea hapticelor, dializa
datorată plăgii este mai puţin probabil să afecteze curbura
zonulară, rupturi ale capsulei posterioare, capsulorexis
corneană şi axele vizuale [28]. Pe de altă parte, într-o
asimetric, plasarea asimetrică a hapticelor, una în sulcus
incizie localizată superior, factorul gravitaţional şi clipitul
şi una în sacul capsular. Dislocarea tardivă spontană în
tind să creeze o tracţiune asupra acesteia. Aceste forţe sunt
sac se asociază cu insuficienţă zonulară, cum este cea din
neutralizate mai bine în localizările temporale, pentru că
sindromul exfoliativ [34].
inciziile sunt paralele cu vectorii forţelor.
Examinările efectuate pe ochi de cadavru cu
Efecte diferite ale inciziilor, din punct de vedere al
pseudofak de cameră posterioară au arătat că fixarea
astigmatismului indus, în funcţie de locaţia lor, au fost
asimetrică
(bag-sulcus) este o cauză a descentrării
raportate de mulţi alti autori. Kohnen şi colab. [29] au
[35,36]. Gradul descentrării a fost de 0,8 mm în cazul
raportat o diferenţă semnificativă statistic în
fixaţiei bag-sulcus şi de numai 0,4 mm în cazul fixaţiei
astigmatismul cornean indus după incizia tunelară
bag-bag [37].
limbică nesuturată, temporală şi nazală. Guirao şi colab.
Materialele din care sunt confecţionate implantele
[30] au arătat că incizia temporală induce aberaţii mai
artificiale de cristalin. Înainte de era cristalinelor
puţine decât cea nazală.
artificiale foldabile, cel mai frecvent utilizate au fost cele
Din punct de vedere structural este cunoscut faptul
din polymethyl methacrylate (PMMA). În acest sens,
că incizia în chirurgia cataractei poate induce un efect
este cunoscut faptul că implantele PMMA pot fi asociate
de aplatizare atunci când este efectuată aproape sau pe
cu o reacţie inflamatorie mai mare decât cele hidrofilice
meridianul mai refringent al corneei
[19]. Astfel,
acrylice şi cu o rată mai ridicată de opacifiere a capsulei
plasarea inciziei pe meridianul cornean mai refringent în
posterioare [38]. Este neclar dacă acest efect este legat
chirurgia cataractei prin facoemulsificare, corectează
direct de materialul implantului, sau de dimensiunea
valori mici ale astigmatismului preexistent şi este
mai mare a plăgii necesară implantelor rigide. În prezent,
suficientă pentru majoritatea ochilor operaţi de cataractă
implantele artificiale de cristalin sunt confecţionate fie
[8]. O incizie de
2,8 mm localizată temporal este
din silicon, fie din polimeri acrilici. Pe de altă parte,
recomandată pacienţilor cu astigmatism preexitent
aceste materiale pot fi clasificate după natura lor
neglijabil, în timp ce incizia nazală şi superioară ar trebui
hidrofilică sau hidrofobică. Materialele hidrofilice sunt
utilizată tot pentru corectarea astigmatismului de grad
considerate, în general, a avea o biocompatibilitate
mic, atunci cînd axele refringente sunt localizate la 180°
uveală mai bună, în comparaţie cu materialele
şi respectiv 90° [31].
hidrofobice, dar ultimele cu designul lor actual, pot avea
128
Pop et al
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
GENERAL REVIEW
o mai mare performanţă în prevenirea opacifierii
4.
Kim IT, Park HYL, Kim SH. Postoperative astigmic
capsulei posterioare
[39,40]. O astfel de complicaţie
outcomes based on the haptic axis of intraocular lenses
necesită capsulotomie laser YAG, care ulterior poate
inserted in cataract surgery. Korean J Ophthalmol
cauza descentrarea implantului artificial de cistalin [41].
2011;25(1):22-8.
Mărimea părţii optice poate fi responsabilă de
5.
Eydelman MB, Drum B, Holladay J et al. Standardized
apariţia unui astigmatism postoperator şi este datorată
analyses of correction of astigmatism by laser systems that
utilizării tot mai frecvente a cristalinelor artificiale cu
reshape the cornea. J Refract Surg 2006;22:81-95.
diametru mic, care sunt mai dificil de centrat. Implantele
6.
Gills JP. Treating astigmatism at time of cataract surgery.
artificiale de cristalin cu părţi optice mai largi (6 mm),
Curr Opin Ophthalmol 2002;13(1):2-6.
sunt mai bune în acest sens, deoarece sunt mai puţin
7.
Carvahlo MJ, Suzuki SH, Freitas LL, Branco BC,
dependente de centrare şi au o rată mai scăzută de
Schor P, Lima AL. Limbal relaxing incisions to correct
opacifiere a capsulei posterioare [42]. Pe de altă parte un
corneal astigmatism during phacoemulsification. J
diametru mai mare necesită o incizie mai largă, crescând
Refract Surgery 2007;23(5):499-504.
astfel riscul de apariţie a astigmatismului postoperator.
8.
Amesbury EC, Miller KM. Correction of astigamtism
Forma şi mărimea hapticelor au un rol important în
at the time of cataract surgery. Curr Opin Ophthalmol
descentrarea pseudofakului, cu posibilitatea apariţiei
2009;20:19-24.
astigmatismului postoperator. Hapticele cu forma în ,,J”
9.
Basti S, Vasavada A, Tomas R, Padhmanabhan P.
vin în contact cu capsula posterioară pe o porţiune cu
Extracapsular cataract extraction: surgical tehniques.
25% mai mică decât cele cu bucla în ,,C” [43]. Pe de
India 1993;41(4):195-210.
altă parte, un diametru total de 12,0-12,5 mm este
10.
Luntz MH, Livingston DG. Astigmatism in cataract
suficient pentru o centrare mai bună a pseudofakului.
surgery. BJO 1977;61:360-5.
Un diametru mai mare poate întinde capsula în direcţia
11.
Melles GRJ, Binder PS, Beekhuis WH, Wijdh RHJ,
lentilei, devenind ovală, descentrarea pseudofakului
Moore MNM, Anderson JA, Raj NS. Scar tissue
fiind astfel posibilă.
orientation in unsutured and sutured corneal wound
Designul implantului artificial de cristalin. Dislocarea
healing. BJO 1995;79:760-5.
pseudofakului a fost raportată la ambele modele, single
12.
Van Rij G, Waring GO. Changes in corneal curvature
piece sau multi piece [44]. Această complicaţie este mai
induced by sutures and incisions. Am J Ophthalmol
frecventă atunci când implantul artificial nu este plasat
1984;98:773-83
simetric în sacul capsular.
13.
Jaffe NS, Clayman HM. Te phatophisiology of corneal
astigmatism after cataract extraction. Ophthalmology
Concluzii
(Rochester) 1975;79: 615-30.
14.
Wishart MS, Wishart PK, Gregor ZJ. Corneal
Astigmatismul postoperator de valoare mare poate
astigmatism following cataract extraction. Br J
compromite rezultatul funcţional după chirurgia
Ophthalmol 1986;70:825-30.
cataractei. Cauzele acestui tip de astigmatism sunt
15.
Maul E, Muga R. Anterior segment surgery early after
multiple, dar caracteristicele inciziei chirurgicale sunt
corneal wound repair. British J of Ophthalmol
cele mai importante. Incizia mică, în cornee clară,
1997;61:782-4.
reduce riscul deteriorării corneene, asigurând o
16.
Buratto L, Maurizio I. Incisions and sutures in cataract
reabilitare anatomică şi funcţională precoce după
suregry. Ed. Fogliaza 1986;32-5,39-40.
chirurgia cataractei.
17.
Giasanti F, Rapizzi E, Virgili G et al. Clear corneal
incision of 2.75mm for cataract surgery induces little
change of astigmatism in eyes with low preoperative
Bibliografie
corneal cylinder. Eur J Ophthalmol 2006;16:385-93.
18.
Ernest P, Hill W, Potvin R. Minimizing surgically
1. Donders FC. On the anomalities of accomodation and
induced astigmatism at time of cataract suregry using a
refraction of the eye. London. New Sydenham Society,
square posterior limbal incision. Journal of
1864:334-9
Ophthalmology 2011:2(10):1155/2011/243170.
2. Nicula C, Nicula D. Astigmatismul indus operator.
19.
Buratto L. Extracapsular cataract microsurgery and
SRO. Oftalmologia, 2000;43-7.
posterior chamber intraocular lenses. Ed. Fogliara,
3. Cho YK, Kim MS. Preoperative modulating factors on
Milano, 1989:236-43.
Astigmatism in Sutured Cataract Surgery. Korean J of
20.
Biro Z. Bazele facoemulsificarii. Ed.Tudomani, Pecs,
Ophthalmol 2009;23(4):240-8.
2002;Cap 3:39-42.
Etiology of Postoperative Astigmatism after Cataract Surgery
129
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
21.
Elkady B, Alio J, Ortiz D, Montalban R. Corneal
33.
Cataract in the adult eye-Complications of intraocular
aberrations after microincision cataract surgery. J
lenses. American Academy of Ophyhalmology
Catarct Refract Surg 2008;34(1):40-5.
2011;17:29-31.
22.
Yao K, Tang X, Ye P. Corneal astigamtism, high order
34.
Masket S, Osher RH. Late complications with
aberrations and optical quality after cataract surgery:
intraocular lens dislocation after capsulorexis in
microincision versus small-incision. J Refrac Surg
pseudoexfoliation syndrome. J Cataract Refract Surg
2006;22:1079-82.
2002;28:1481-4.
23.
Cillino S et al. Temporal versus superior approach
35.
Apple DJ et al. Posterior chamber intraocular lenses in a
phacoemulsification:
short-term
postoperative
series of 75 autopsy eyes. Part I. Loop location. J Cataract
astigmatism. J cataract Surg 1997;23:267-71.
Refract Surg 1986;12:358-62.
24.
Bennett AG. Analysis of three meridional keratometric
36.
Hansen SO et al. Descentration of flexibile loop
measurements of the anterior cornea. Ophthalmic
posterior chamber intraocular lenses in a series of 222
Physiol Opt 1990;10:93-4.
postmortem eyes. Ophthalmology 1988;95:344-9.
25.
Alio JL, Elkady B, Ortiz D. Corneal quality following
37.
Wassernann D et al. Anterior capsular tears and loop
sub 1,8 mm micro-incision cataract suregry vs. 2,2 mm
fixation of posterior chamber intraocular lenses.
mini-incision coaxial phacoemulsification. Middle East
Ophthalmology 1991;98:425-31.
Afr J ophthalmol 2010;17(1):94-9.
38.
Rowe NA, Biswas S, Lloyd IC. Primary IOL
26.
Merriam JC, Zheng LZ, Urbanowicz J, Zaider M.
implantation in children: a risk analysis of foldable
Change on the horizontal and vertical meridians of the
acrylic versus PMMA lenses. Br J Ophthalmol
cornea after cataract surgery. Trans Am Ophthalmol
2004;88(4):481-5.
Soc 2001(99):187-97.
39.
Hayashi K, Hayashi H. Posterior capsule opacification
27.
Duke-Elder S, Wybar KC. Te ocular tissues. In:
after implantation of a hydrogel intraocular lens. Br J
Duke-Elder S. Ed. System of Ophthalmology. Vol II.
Ophthalmol 2004;88(2):182-5.
Te anatomy of tha visual system. St Louis, Mo:CV
40.
Hollick EJ, Spalton DJ, Ursell PG, Meacock WR,
Mosby, 1961:92.
Barman SA, Boyce JF. Posterior capsular opacification
28.
Gokhale NS, Sawhney S. Reduction in astigmatism in
with hydrogel, polymethylmethacrylate and silicone
manual small incision cataract surgery through change
intraocular lenses: two-years results of a randomized
of
incision site.
Indian J of Ophthalmol
prospective trial. Am J Ophthalmol 2000;129(5):577-
2005;53(3):201-3.
84.
29.
Kohnen S, Neuber R, Kohnen T. Effect of temporal
41.
Steinert RF, Puliafito CA, Kunar SR, et al. Cystoid
and nasal unsutured limbal tunnel incisions on induced
macula edema, retinal detachment and glaucoma after
astigmatism after phacoemulsification. J Catract Rafract
Nd YAG laser posterior capsulotomy. Am. J.
Surg 2002;28(5):821-5.
Ophthalmology 1991;112:373-80.
30.
Guirao A, Tejedor J, Artal P. Corneal aberrations before
42.
Meacock WR, Spalton DJ, Boyce JF, Jose JR. Effect of
and after small-incision cataract surgery. Invest
optic size on posterior capsular opacification with 5.5
Ophthalmol Vis Sci 2004;45(12):4312-19.
mm and 6.0 mm optic diameter Acrysof intraocular
31.
Tejedor J, Perez-Rodriguez A. Astigmatic change
lenses. J Cataract Refarct Surg 2001;27:1194-8.
induced by 2.8 mm corneal incisions for cataract surgery.
43.
Assia EI, Apple DJ. Side-view analysis of the lens. Arc
Invest Ophthalmol Vis Sci March 2009; 50(3):989-
Ophthalmol 1992;110:94-7.
94.
44.
Mamalis N, Brubaker J, Davis D, et al. Complication
32.
Dick HB, Augustin AJ. Lens implant selection with
of foldable intraocular lenses requiring explantation or
absence of capsular support. Curr Opin Ophthalmol
secondary intervention. J Catarct Refract Surg
2001;12:47-57.
2008;34:1584-9.
130
Pop et al
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
GENERAL REVIEW
GENERAL REVIEW
ACTUALITĂŢI ÎN STUDIUL VASCULARIZAŢIEI NERVULUI OPTIC
Măgureanu Marineta¹, Stănilă Adriana², Stănilă Dan Mircea²
¹Centrul Medical Ghencea, Bucureşti, ²Centrul de Cercetare a Suprafeţei Oculare, Universitatea „Lucian Blaga”, Clinica
de Oftalmologie - SCJU, Sibiu
Adresa pentru coresponenţă:
Dr. Marineta Magureanu
Str. Crinului, Nr.43, Sector1, Bucureşti
Tel: 0723658133
Email: dr_magureanu@yahoo.com
Primit: 30.01.2013
Acceptat: 20.02.2013
Med Con March 2013, Vol 8, No 1, 131-137
Rezumat
acestor factori influenţează în mod complex şi variat
fluxul sanguin ocular, necesitând studierea acestuia în
Deoarece multe afecţiuni oculare au factorul
vederea elucidării modificărilor hemodinamice în
vascular la bază, este foarte important să înţelegem atât
diferite afecţiuni.
vascularizaţia acestei zone, cât şi patogenia şi
Cercetările realizate în vederea înţelegerii fluxului
managementul acestora. În ceea ce priveşte nervul optic
sanguin ocular s-au intensificat în ultimele decenii, în
(NO), vascularizaţia acestuia joacă un rol decisiv în
întreaga lume. Tehnicile actuale de examinare
etiopatogenia diferitelor forme de neuropatie optică
noninvazivă a fluxului sanguin ocular au contribuit în
(inclusiv cea glaucomatoasă), precum şi a altor afecţiuni
mod semnificativ la înţelegerea rolului hemodinamicii
oftalmologice. Vascularizaţia NO este complexă,
sanguine oculare în etiologia diferitelor afecţiuni
particulară şi variază în funcţie de segmentul acestuia.
oftalmologice [1].
În ultimii ani au fost dezvoltate noi tehnici, sau au
În ultimii ani, s-a ajuns la concluzia ca în neuropatia
fost perfecţionate altele mai vechi, de examinare a
optică glaucomatoasă, în afara tensiunii intraoculare, ar
vaselor oculo-orbitare şi a fluxului sanguin la acest nivel.
exista şi alţi factori care ar influenţa evoluţia afecţiunii,
Tehnicile actuale de examinare noninvazivă a fluxului
dintre care factorul vascular se pare că ar avea un rol
sanguin ocular au contribuit în mod semnificativ la
important.
înţelegerea rolului hemodinamicii sanguine oculare în
O dovadă în acest sens este a 6-a întâlnire a Asociaţiei
etiologia diferitelor afecţiuni oftalmologice.
Mondiale de Glaucom (WGA) din anul 2009, care a
Cuvinte cheie: circulaţie arterială, circulaţie
avut ca temă ”Fluxul sanguin ocular în Glaucom” [1].
venoasă, flux sanguin, nerv optic
Vascularizaţia nervului optic
Vascularizaţia NO este complexă şi variază în funcţie
Introducere
de segmentul acestuia: capul nervului optic, alcătuit de la
anterior spre posterior din
4 regiuni: stratul fibrelor
Ochiul este organul la nivelul căruia vasele sanguine
nervoase,
prelaminară,
laminară,
retrolaminară,
pot fi examinate în mod direct, prin tehnici neinvazive.
segmentul intraorbital (25-30 mm), segmentul canalicular
Fluxul vascular ocular este influenţat de diverşi factori şi
(9-10 mm), segmentul intracranial (16 mm) [2,3,4,5],
de interacţiunea acestora: produşi metabolici, presiunea
fiind foarte bogată înainte de intrarea arterei centrale a
de perfuzie, gazele sanguine. Efectele şi interacţiunile
retinei în glob şi mult mai saracă după aceea [6].
News in Study of Optic Nerve Vascularization
131
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
I. Circulaţia arterială
din vascularizaţia acestei zone)
[1,4,10]. Capilarele
Circulaţia arteriala a NO se realizează prin artera
acestei regiuni sunt complexe şi se continuă cu patul
oftalmică
(AO), ram al arterei carotide interne, cu
capilar de la nivelul suprafeţei stratului fibrelor nervoase
originea la nivelul peretelui anterior al regiunii C3 şi cu
şi cu cel de la nivelul regiunii laminare.
direcţie orizontală şi anterioară, care intră în orbită prin
Inelul Zinn-Haller
gaura oftalmică împreună cu NO, aşezându-se lateral şi
A fost descris de Haller în 1754 şi de Zinn în 1755
inferior faţă de acesta [7]. Ulterior, trece pe deasupra
ca fiind un cerc arterial anastomotic incomplet, situat la
NO, iar în treimea anterioară are un traiect paralel cu
nivelul sclerei peripapilare şi format din anastomozele
faţa medială a orbitei şi trece medial şi superior de NO
ACP scurte în jurul capului NO [1,3,4,10], Figura 2. La
[8]. AO se împarte în ramuri oculare şi orbitare [7].
ochii cu inel Zinn-Haller bine dezvoltat, ramuri arteriale
Ramurile oculare ale AO sunt
[3]: artere ciliare
din acesta vascularizează atât regiunea prelaminară,
posterioare scurte, artere ciliare posterioare lungi, artera
laminară [1], cât şi regiunea retrolaminară prin ramuri
centrală a retinei
(ACR) care pătrunde în NO la
recurente [10]. Olver şi colab. au descris inelul Zinn-
aproximativ 10-15 mm posterior de glob, iar după ce
Haller ca o anastomoză microvasculară, microscopică,
pătrunde în ochi, se divide în 2 arcade: superioară şi
intrasclerală, eliptică, formată din ramurile laterale şi
inferioară [9].
mediale ale ACP scurte paraoptice.
În mod obisnuit, între 2 şi 4 artere ciliare posterioare
3. Segmentul laminar
(ACP) au un traiect anterior, urmând a se divide în
Întreaga vascularizaţie este asigurată de ramuri ale
aproximativ 10-20 ACP scurte înainte de a pătrunde în
ACP scurte şi de inelul Zinn-Haller [3,4,10]. Ocazional,
globul ocular [1]. Deseori, ACP se grupează în 2 grupuri
din coroida peripapilară pot pleca mici arteriole [4]. La
arteriale: lateral şi medial, înainte de a se ramifica în
acest nivel, capilarele sunt organizate sub forma unui
ACP scurte [1]. ACP scurte penetrează sclera perineurală
plex capilar dens, constituind o structură foarte
pentru a vasculariza coroida peripapilară şi porţiunea
vascularizată la nivelul capului NO
[10]. Capilarele
anterioară a NO. Unele pot străbate sclera până la
acestei regiuni se continuă cu capilarele regiunii
nivelul coroidei, fără a se ramifica [1]. După Hayreh,
retrolaminare.
ACP de-a lungul traiectului intraorbital se împart în
4. Segmentul retrolaminar
numeroase ramuri, la distanţe diferite, înainte de
Vascularizaţia acestei regiuni este dublă (Figura 2):
pătrunderea în globul ocular: ACP lungi în general în
vascularizaţia periferică, centripetă, asigurată de vasele
număr de 2- una medial şi una lateral, fără rol în
piale cu origini la nivelul inelului Zinn-Haller, ACP
vascularizaţia NO şi ACP scurte în număr de aproximativ
scurte şi din zona coroidală peripapilară [1,4,10]; mai
20, care se subîmpart în 2 subgrupe - artere paraoptice
pot participa ramuri piale din ACR şi alte artere orbitale;
(pentru NO) şi artere distale (pentru coroidă) [10].
vascularizaţia axială, centrifugă, prezentă în 75% din
1. Stratul fibrelor nervoase
cazuri, formată din ramuri (de la 1 la 8) ale ACR.
Este prima zona irigată după model centripet, prin
Vascularizatia axială, când este prezentă, nu este la fel de
ramuri ale ACR, care se formează la nivelul retinei
dezvoltată ca şi cea periferică [4,10]. Mai pot participa
peripapilare [4]. Aceste arteriole merg spre discul optic
capilare din regiunea laminară [4].
şi sunt denumite „vase epipapilare”. Ramuri capilare din
În concluzie ACP, în mod direct sau via ramuri
aceste vase se continuă cu capilarele retiniene de la
coroidale peripapilare sau ACP scurte (sau inelul Zinn-
marginea discului optic, dar au şi anastomoze posterioare
Haler când este prezent), reprezintă singura sursă
cu capilarele prelaminare ale NO [1,3,4,5]. Contribuţia
vasculară pentru regiunile laminară şi prelaminară şi
coroidală directă nu este demonstrată la acest nivel
principala sursă
(dacă nu singura) pentru regiunea
[4,5]. Când artera cilio-retiniană este prezentă (una sau
retrolaminară [10].
mai multe), ramurile precapilare pot contribui la irigarea
Zone „watershed” ale arterei ciliare posterioare
sectorului temporal
[1,3,4,5,10]. Numărul acestor
Când un ţesut este irigat de două sau mai multe
artere este corelat cu marimea discului optic [3].
artere terminale, limita de distribuţie între aceste vase se
2. Segmentul prelaminar
numeşte zonă
„watershed”. Acestea sunt zone cu
Irigaţia este asigurată preponderent de ACP scurte
vascularizaţie saracă, ceea ce la face vulnerabile la
prin ramuri directe, sau prin intermediul inelului Zinn-
ischemie. Rolul important al acestor zone se evidenţiază
Haller (când acesta este prezent). Ramuri ale arteriolelor
în cazurile în care presiunea de perfuzie din una sau mai
şi capilarele formează o reţea difuză în jurul şi interiorul
multe artere terminale care aparţin aceleiaşi zone, scade.
fasciculelor nervoase [5]. Sunt studii care susţin existenţa
Localizarea zonelor „watershed” la acest nivel variază în
unor ramuri din vasele coroidiene peripaplilare (10%
funcţie de numărul şi poziţia ACP [10].
132
Măgureanu et al
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
GENERAL REVIEW
5. Segmentul intraorbital
nivelul VCR. VCR se formează la nivelul discului optic
Este subîmpărţit în funcţie de locul de pătrundere a
prin unirea unui număr variat de vene retiniene şi merge
ACR în NO în 2 subsegmente: anterior şi posterior [10].
posterior prin axul NO, situată temporal de ACR. VCR
Subsegmentul anterior dispune de
2 sisteme
străbate o parte a NO înainte de a ieşi din acesta, în
vasculare: sistemul periferic (centripet) şi sistemul axial
orbită. Astfel, sângele venos este drenat în cea mai mare
(centrifug). Sistemul periferic este întotdeauna prezent,
parte către sinusul cavernos şi în mai mică măsură spre
vascularizaţia arterială a fibrelor periferice ale NO fiind
reţeaua orbito-facială şi orbito-pterigoidiana [6].
asigurată prin artere venite din sistemul vascular al piei
Angioarhitectura nervului optic
mater, cele mai multe fiind ramuri din AO [4], coroida
Încă din 1903 a fost descrisă de diverşi investigatori.
peripapilară, inelul Zinn-Haller, ACR şi alte artere
Vascularizaţia NO este identică cu cea a creierului. Toate
orbitale [10]. Ramuri din AO traversează peretele durei
arterele NO asigură vascularizaţia acestuia prin
la
10-12 mm de glob pentru a participa la formarea
intermediul plexului vascular pial, care acţionează ca un
sistemului pial
[4]. Ramuri recurente din ACP şi
„centru de distribuţie a vaselor”. Vasele de sânge care
coroidale juxta-papilare se adaugă vascularizaţiei piale
pătrund în NO străbătând pia sunt acoperite de aceasta
[4]. Sistemul axial (centrifug) este prezent la 75% din
şi de ţesut glial, ceea ce duce la formarea unui sistem
NO; părţile centrale ale NO sunt nutrite de arteriolele
septal la nivelul NO. Angioarhitectura laminei cribrosa
intraneurale de origine pială
[6] şi din ramuri
constă dintr-un plex capilar foarte dens cu diametru de
intraneurale (în număr de 1-8) ale ACR [6,10].
10-20 μm, alcătuit din numeroase
”ochiuri” mici,
Subsegmentul posterior prezintă un sistem vascular
elongate, foarte apropiate, dispuse transversal, ceea ce
periferic centripet reprezentat de plexul vascular pial,
face ca aceasta să fie cea mai vascularizată zonă a capului
format din multiple artere colaterale mici, cu originea
NO. Segmentul intraorbital prezintă anastomoze între
frecvent la nivelul AO şi mai rar la nivelul altor artere
ramurile AO la suprafaţa NO şi anastomoze între
orbitale. În
10% din cazuri, poate exista un sistem
ramurile intraneurale în interiorul NO. Vase
vascular axial centrifug format din ramuri intraneurale
longitudinale sunt conectate neregulat cu vase
ale ACR [10].
transversale care merg în diferite direcţii formând în
6. Segmentul canalicular
secţiune longitudinală „plase cu ochiuri” având forme
Există opinii diferite în ceea ce priveşte vascularizaţia
neregulate.
Segmentul intracanalicular
are
o
acestei zone. După Hayreh, vascularizaţia acestui
angioarhitectură asemănătoare segmentului intraorbital,
segment este asigurată de AO prin ramuri colaterale,
devenind din ce în ce mai complicată pe masură ce se
obişnuit între 1 şi 3. Aceste ramuri ajung la nivelul NO
apropie de segmentul cranial, pierzând-se diferenţa între
traversând teaca conjunctivă care acoperă nervul la acest
vasele longitudinale şi cele transversale. Segmentul
nivel. Nu există sistem vascular axial la acest nivel [10].
intracranial are o dublă angioarhitectură: în partea distală
7. Segmentul intracranial
comparativ cu segmentul anterior, vasele longitudinale
Există multe controverse în ceea ce priveste
devin proeminente, iar cele transversale mai rare; în
vascularizaţia acestui segment. Rezumând, ea este
partea proximală, mai ales în porţiunea laterală, vasele
asigurată de ramuri care provin din: artera carotidă
sunt mai puţin dense. La nivelul NO, capilarele se întind
internă, artera cerebrală anterioară, artera comunicantă
pe toată lungimea acestuia, existând anastomoze între
anterioară, AO. Arteriolele piale devin capilare şi străbat
ele, iar anterior, anastomoze cu capilarele retiniene [10].
septul pial până în axul NO [4,10].
Structura peretelui vascular
II. Circulaţia venoasă
Peretele vascular este alcătuit de
3 straturi
Circulaţia venoasă a capului nervului optic este
concentrice, diferite din punct de vedere histologic, din
asigurată în special de vena centrală a retinei (VCR) [10],
interior spre exterior: tunica intimă, medie şi adventice.
paralelă cu artera omonimă în interiorul NO [1,3]. Mici
Tunica intimă este alcatuită din stratul endotelial,
venule drenează de la stratul fibrelor nervoase superficiale
subendotelial şi lamina elastică internă. Stratul endotelial
către coroidă (vene optico-ciliare) [4]. Vasele regiunii
are un singur strat de celule (epiteliu scuamos simplu)
prelaminare drenează în venele coroidale peripapilare
de formă ovoidală, cu axul lung paralel cu axul lung al
(VCR, la acest nivel, comunică cu circulaţia coroidală).
vasului, aşezate pe lamina bazală. Numărul lor diferă în
Nu există un echivalent venos pentru inelul Zinn-Haller.
funcţie de mărimea vasului: la vasele cu calibru mic este
Venele din trunchiul nervos merg parte în VCR, parte
suficientă o celulă endotelială pentru a acoperi
într-o venă centrală posterioară
[6]. Regiunea
circumferinţa lumenului; la vasele mai mari numărul lor
intraorbitală drenează în principal în VCR. Venele piale
este direct proporţional cu mărimea acestora. În celulele
aflate la nivelul piei mater se deschid preponderent la
endoteliale de la nivelul arterelor exista corpusculi
News in Study of Optic Nerve Vascularization
133
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
Palade (ribozomi) care conţin factor von Willebrand
nivelul ACR; o lentilă de contact prevazută cu un senzor
[11], cu rol în formarea cheagului. Stratul subendotelial
de presiune măsoară creşterea presiunii intraoculare
este format din ţesut conjunctiv lax şi celule musculare
(TIO); presiunea diastolică a ACR este considerată a fi
netede, dispuse longitudinal. Lamina elastică internă
egală cu TIO de debut; valoarea maximă a TIO
este alcatuită din elastină, are aspect fenestrat (“plasă”),
corespunde presiunii sistolice a ACR [1].
permiţând difuziunea substanţelor. Este mai dezvoltată
Oftalmodinamograful (ODG): măsoară presiunea în
la nivelul arterelor de tip muscular.
AO; ochii sunt acoperiţi cu o membrană elastică care
Tunica medie este formată din celule musculare
exercită presiune în orbită; similar măsurării presiunii
netede şi lamina elastică externă. Celulele musculare
sanguine cu ajutorul sfigmomanometrului, pulsaţia se
netede sunt în straturi concentrice, dispuse helicoidal,
transmite de la orbită, prin intermediul membranei,
printre care găsim fibre elastice (mai bine dezvoltate la
dispozitivului care o exprimă într-o diagramă [1].
nivelul arterelor de tip elastic), fibre de colagen tip III şi
Oculo-oscilo-dinamograful (OODG): îmbunătăţeşte
proteoglicani. Vasele postcapilare nu au tunică medie,
tehnica anterioară, determinând în mod direct pulsaţia
aceasta fiind înlocuită de pericite.
la nivelul patului coroidian sau retinian [1].
Tunica adventice este alcatuită din fibroblaşti, fibre
Pulsatile Ocular Blood Flowmetry (POBF): măsoară
de colagen tip I şi fibre elastice, orientate longitudinal.
TIO în timp real, fără a o influenţa, prin intermediul
În funcţie de proporţia diferitelor elemente din
unui pneumotonometru modificat şi conectat la un
structura peretelui, arterele se împart în: elastice şi
computer. Fluxul sanguin ocular variază pe parcursul
musculare [7].
ciclului cardiac, influenţând valoarea TIO, existând un
La nivelul microcirculaţiei, echilibrul dintre fluxul
vârf pe parcursul sistolei şi o scădere în diastolă.
sanguin şi presiunea intraluminală este asigurat de
Cuantificând pulsaţia TIO asociată ciclului cardiac,
tonusul arteriolar, sfincterele precapilare, tonusul
permite calcularea componentei pulsatile a fluxului
pericitelor capilare şi fibrele musculare netede din vene.
vascular ocular
(se realizează aproximativ
200
Pericitele capilare pot substitui rolul sfincterelor
determinări/sec) [1,3,10].
precapilare unde acestea lipsesc.
Interferometrul: evidenţiază în mod direct pulsaţia la
Din punct de vedere al naturii endoteliului, capilarele
nivel retinian, folosind o undă laser care se divide în 2
pot fi fenestrate şi nefenestrate. Capilarele fenestrate
fascicule
(unul pentru retină şi altul pentru cornee)
(prezente în majoritatea organelor) permit trecerea
[1,3].
moleculelor mari, în special proteine. Capilarele
Dispozitive Laser
nefenestrate, prezente la nivel retinian şi la nivelul capului
LDF (Laser Doppler Flowmetry): metodă descrisă
NO, nu permit difuzarea de substanţe din plasmă în ţesutul
pentru prima dată în 1992 de Riva şi colab., evaluează
din jur
[3,5] şi au joncţiuni tip tight între celulele
fluxul sanguin la nivelul capului NO: fasciculul laser
endoteliale, realizând bariera hemato-oculară [5]. Capilarele
măsoară fluxul sanguin la o adâncime mai mare de 520
de la nivelul retinei şi al nervului optic sunt lipsite de
μm, zona corespunzătoare ACP [1,3,10].
sfinctere precapilare, dar au numeroase pericite. Aceste
SLDF (Scanning Laser Doppler Flowmetry): este
pericite acţionează ca nişte veritabili muşchi netezi vasculari,
singurul dispozitiv care măsoară fluxul vascular în
reacţionând la prezenţa CO2, a nivelului O2 şi a
unităţi absolute. Prin combinarea avantajelor oferite de
concentraţiei adenosinei. Aceste capilare sunt echipate
fundus camera şi efectul Doppler, poate evidenţia
pentru a interveni în controlul fluxului sanguin la nivelul
velocitatea, diametre şi traiecte vasculare [1,10].
capului NO prin mecanismul de „metabolic autoregulation”.
LSF (Laser Speckler Flowgraphy): tehnică neinvazivă
În contrast, patul capilar coroidian (coriocapilarele), este
folosită pentru prima dată de cercetători japonezi şi care
constituit din capilare fenestrate şi rare pericite [3].
examinează fluxul sanguin la nivelul capului NO,
Examinarea vascularizaţiei şi a fluxului sangvin
fasciculul laser atingând profunzimi de 0,5-1 mm. Are
la nivelul NO
la bază fenomenul de „interferenţă”, observat când o
În ultimii ani au fost dezvoltate noi tehnici, sau au
sursă de lumină cum ar fi laserul scanează o suprafaţă
fost perfecţionate altele mai vechi, în examinarea vaselor
reflectorizantă [1,3,10].
oculo-orbitare şi a fluxului sanguin la acest nivel. Unele
Scanning Laser ophthalmoscope (SLO): are la bază
au ramas la stadiu experimental, altele şi-au găsit
tehnica LDF; dispozitivele folosesc un sistem optic
aplicabilitate clinică.
confocal, ceea ce duce la obţinerea unor imagini de o
Dispozitive de măsurat pulsatilitatea
calitate deosebită ale fundului de ochi [1,10].
Oftalmodinamometrul (ODM): este un dispozitiv
HRF (Heidelberg Retinal Flowmeter): are la bază
care măsoară indirect presiunea sistolică şi diastolică la
tehnica LDF, la care s-a adaptat un sistem de scanare
134
Măgureanu et al
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
GENERAL REVIEW
laser confocală ceea ce permite examinarea la o
Angiografia cu verde de indocianină
(ICG): se
profunzime mai mare. Poate oferi imagini ale retinei
realizează cu ajutorul unui dispozitiv SLO care va
peripapilare şi inelului neuro-retinian [1,3,10].
evidenţia prezenţa substanţei de contrast legată de
3-HRT (Tomografia retiniana Heidelberg): Evaluază
proteinele plasmatice
(indocianina), injectată IV, la
fluxul sanguin la nivelul inelului neuro-retinian [1].
nivelul vaselor oculare, cu predilecţie cele coroidiene
Doppler OCT (Tomografia în coerenţă optică): Noile
[3,5,10].
generaţii ale OCT: time-domain (TD-OCT) şi spectral-
Angiografia prin rezonanţă magnetică = angio-RM
domain (SD-OCT), au crescut performanţele OCT-ului
(MRA): metodă completă, neinvazivă de examinare a
clasic. SD-OCT oferă imagini tridimensionale de
circulaţiei intra- şi extracraniene; cea mai utilizată
microstructură intraretiniană printr-o scanare mai rapidă şi
tehnică este ”time of flight” (TOF), cu două posibilităţi
cu o rezoluţie superioară (18.000 măsuratori/sec, cu o
de achiziţionare de date pentru imagini: bidimensionale
rezoluţie axială de 5 mm) faţă de TD-OCT (400 măsurători/
(2D-TOF) şi tridimensionale (3D-TOF) [7]. O altă
sec cu o rezoluţie axială de ~10 mm). Experimental se
tehnică folosită este „phase contrast pulse sequences”
foloseşte High-speed ultrahigh-resolution OCT
(UHR
[15].
OCT): 25000 măsurători/sec, cu o rezoluţie axială de 3,5
Angiografia prin tomografie computerizata = angio-
mm. Prin noile tehnologii se pot măsura viteza şi volumul
CT (CTA): realizează secţiuni de 1mm, vizualizate prin
fluxului sanguin la nivelul ramurilor vaselor retiniene ca şi
tehnica MIP (maximum intensity projection) [7,15].
dimensiunile acestor vase. Prin dezvoltarea acestor tehnici
Angiografia „dynamic ultra-widefiel” Optos P200MA:
se încearcă obţinerea de informaţii structurale Doppler şi
oferă un câmp foarte larg de examinare şi o calitate
oximetrice în timpul aceleiaşi scanări [1,3,5].
deosebită [5].
Ultrasonografe Doppler: utile în diagnosticul a
Oximetria
multiple afecţiuni vasculare primare sau secundare ale
Oximetria retiniană: metodă neinvazivă care
ochiului şi orbitei [12].
masoară saturaţia în oxigen a hemoglobinei la nivelul
Ecografia Doppler Color (CDI): poate examina AO,
structurilor retiniene cu ajutorul imaginilor digitale
ACR şi VCR, ACP scurte, vena oftalmică superioară
[1,3].
măsurând velocitatea fluxului vascular şi indexul de
Oximetria prin Rezonanţă Magnetică: se bazează pe
rezistenţă vasculară la nivelul acestora. Principalii
proprietăţile paramagnetice ale oxigenului şi pe capacitatea
parametri măsuraţi sunt: viteza maximă sistolică (PSV),
sa de a influenţa rata de relaxare
(1/T¹). Oxigenarea
vitexa maximă diastolică (EDV), indicele de pulsatilitate
vitrosului posterior este utilizată pentru a determina
(PI) şi indicele de rezistivitate (RI) [1,3,10,12,13].
oxigenarea retiniană. Tehnica poate fi îmbunătăţită
Ultrasonografia Doppler Transcraniană: metodă non-
folosind F19 sau perfluorocarbon (PFC) [1].
invazivă, folosită din
1982 de catre Rune Aaslid, în
Examinarea directă
prezent are multiple utilizări, printre care examinarea
Examinarea papilei NO în cadrul examinării
AO [7,10].
fundului de ochi prin: oftalmoscopie directă, oftalmoscopie
Angiografia
indirectă, biomicroscopia fundului de ochi cu diferite
AFG (Angiofluorografia): folosită în oftalmologie de
lentile de contact, fundus camera (se obţin fotografii
aproximativ 50 de ani, evidenţiază in vivo vascularizaţia
stereoscopice).
capului NO, retinei şi a coroidei (mai puţin) [10,14].
Afecţiuni în care este implicată vascularizaţia NO
Substanţa de contrast, fluoresceina, este un compus
Afecţiuni vasculare ale capului NO
chimic netoxic, cu proprietăţi intens fluorescente, care
Tromboza de VCR: histopatologic se produce
se injectează IV. Lumina de excitaţie albastră (λ=465-
tromboza VCR la nivelul laminei cribrosa [5,12,13], sau
490 nm), acţionează asupra fluoresceinei nelegată de
la nivelul unui ram al acesteia.
proteinele plasmatice rezultând o lumină galben-albastră
Ocluzia de ACR: după localizarea ocluziei se poate
(λ=520-530 nm). Se poate realiza o analiză: secvenţială
împărţi în: ocluzia ACR, ocluzia de ram de ACR, ocluzia
- se examinează angiograma cadru cu cadru
de A cilio-retiniană, ocluzia combinată de ACR si VCR
evidenţiindu-se fazele acesteia prearterială, arterială,
[5,12,13].
arterio-venoasă şi venoasă; anatomică
- se observă
Glaucomul cronic
(hipertensiv, dar mai ales cel
straturile şi zonele polului posterior; morfologică [5,14].
normotensiv): în ultimii ani au fost realizate numeroase
Scanning Laser AFG: se obţin imagini de o calitate
studii prospective care au demonstrat deficienţe în
deosebită pe un câmp larg, în care pot fi examinate
circulaţia retiniană, coroidiană şi retrobulbară. De
traiecte şi diametre vasculare în dinamică (timp real)
asemenea, neuropatia optică glaucomatoasă a fost
[1,3,10].
asociată cu o presiune de perfuzie oculară anormală,
News in Study of Optic Nerve Vascularization
135
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
hipotensiune nocturnă, hemoragii discale, migrene şi
[17]. Se caracterizează prin: VCR este lărgită, cu flux
îmbătrânirea precoce a vaselor sanguine. Ischemia
inversat
(sau bidirecţional) şi arterizat, iar vena
cronică a NO duce la pierderea de celule ganglionare
supraorbitară cu flux inversat [12,13]; creşte presiunea
retiniene, independent de valoarea TIO. Reducerea
oculară [17].
presiunii de perfuzie oculare poate fi secundară unei TIO
Malformaţii arterio-venoase: vene cu calibru, viteză
crescute, sau poate reprezenta prima cauză de afectare a
şi direcţia fluxului modificate [12,13].
NO în glaucom. De asemenea, ischemia oculară cronică,
Diabetul zaharat
poate induce afectări ale autoreglarii vasculare şi
HTA: în funcţie de gradul de afectare al patului
incapacitatea acesteia de a reduce TIO şi menţinerea unei
vascular, HTA poate duce la: retinopatie hipertensivă,
presiuni de perfuzie oculară adecvate [3,12,13,16].
coroidopatie şi neuoropatie optică [5].
Hipertensiunea intraoculară
Dezlipirea de retină
Concluzii
Neuropatiile optice: se pot clasifica în
2 grupuri:
neuropatii vasculare
(neuropatia optica ischemică
Deoarece multe afecţiuni oculare au factorul
anterioară = NOIA, boala Horton, drusenul complicat)
vascular la bază, este foarte important să înţelegem atât
şi neuropatii inflamatorii
(afecţiuni demielinizante,
vascularizaţia acestei zone, cât şi patogenia şi
afectiuni sistemice - sarcoidoza) [13]. Hayreh împarte
managementul acestora. În ceea ce priveşte NO,
neuropatiile optice în funcţie de sursa arterială în:
vascularizaţia acestuia joacă un rol decisiv în
neuropatii optice ischemice anterioare (NOIA) care se
etiopatogenia diferitelor forme de neuropatie optică.
referă la porţiunea anterioară a NO irigată de ACP şi
Deocamdată nu dispunem de tehnica perfectă
care se subîmpart în arteritice şi non-arteritice;
necesară examinării fluxului sanguin la nivelul NO.
neuropatii optice ischemice posterioare (NOIP) care se
Oftalmologii au nevoie de metode uşor accesibile,
referă la restul NO, vascularizat prin alte surse arteriale
sigure, fiabile, non-invazive şi repetitive pentru practica
în afara ACP şi care se subîmpart în arteritice, non-
curentă în vederea examinării pacienţilor cu glaucom,
arteritice şi chirurgicale (peri- sau postchirurgicale) [10].
neuropatii optice ischemice sau alte afecţiuni vasculare
Formaţiuni orbitale
ale NO. De asemenea, datorită descoperirii implicării
Hemangiom cavernos: mai frecvent la adulţii tineri,
hipotensiunii arteriale nocturne în apariţia şi progresia
se dezvoltă la nivelul vârfului orbitei [13].
NOIA non-arteritică şi a glaucomului, este necesară o
Hemangiomul capilar: frecvent la copii [13].
metodă care poate monitoriza fluxul sanguin la nivelul
Varice orbitale: venele afectate se modifică în timpul
capului NO continuu/frecvent pe o perioadă de 24 ore
manevrei Valsava (se dilată şi fluxul se opreşte), sau când
(sau mai mult) şi în particular în timpul somnului.
capul este aplecat [13,17].
Lipsa acestor tehnologii fac din managementul
Celulita orbitală: infecţie bacteriană
(frecvent:
afecţiunilor ischemice ale NO şi implicit al prevenirii
stafilococică, streptococică sau cu Haemophilus) a
orbirii o sarcină dificilă [10].
ţesutului grăsos orbital.
Limfom orbital [13]
Gliom de NO: determină reducerea fluxului şi
Referinţe
creşterea indicilor de impedanţă în ACR prin presiunea
exercitată pe teaca NO [12].
1. Harris A, Jonescu-Cuypers CP, Kagemann L, Ciulla
Tumori de invazie orbitală [10].
TA, Krieglstein GK. Atlas of Ocular Blood Flow,
Alte afecţiuni
Vascular Anatomy, Pathophysiology and Metabolism,
Stenoza arterei carotide: determină o scădere a
Second Edition, Ed. Elsevier, 2010,vii:1-9.
fluxului sanguin la nivelul ACR, AO, sau ambele când
2. Basic and Clinical Science Course, American Academy
gradul stenozei este peste 70% şi o schimbare a fluxului
of Ophthalmology 2012-2013, Section Glaucoma, Te
în ocluzii (datorită alimentării AO din carotida externă,
Eye M.D. Association, 40-5.
prin activarea unor anastomoze între arterele
3. Ocular blood flow in glaucoma, the
6th Consensus
periorbitare, cu origine în artera carotidă externă şi AO)
Report of the World Glaucoma Association, Ed.
[7,12,13]. Când stenoza carotidei este peste
90%,
Kugler, 2009, 5-11.
perfuzia la nivelul ACR scade cu 50%, determinând
4. Duane’s Ophthalmology CD, 2000 edition
sindromul de ischemie oculară [5].
5. Arevalo JF. Retinal Angiography and Optical Coherence
Fistulele carotido-cavernoase
(postraumatice sau
Tomography, Ed. Springer,
2009;10-25,110-5,118-
spontane): şunturi între sistemul arterial şi cel venos
21,155-7,407-17,431-45.
136
Măgureanu et al
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
GENERAL REVIEW
6. Cernea P. Tratat de Oftalmologie, Ed. Medicală,
14. Selaru DF, Musat O, Stoenescu D. Ghid de diagnostic
2002,769-70.
în angiofluorografia retiniană, Ed. Morosan, 2012,14-
7. Tiu C, Antochi F. Neurosonologie, Ed. Semne,
8.
2006,46-8,52-3,151-3.
15. Mansour MA, Labropoulos N. Vascular Diagnosis,
8. Gray HL, Bannister LH, Wiliams PL. Gray’s Anatomy,
Ed. Elsevier Saunders, 2005,85-9,105-12.
28ed, Ed. Edinburg, Churchill Livingstone 1995.
16. Rankin SJA. Color Doppler Imaging of the Retrobulbar
9. Basic and Clinical Science Course, American Academy
Circulation in Glaucoma, Survey of Ophthalmology
of Ophthalmology
2012-2013, Section
5, Neuro-
1999;Supplement 1,43:S176-S181.
Ophtalmology, Te Eye M.D. Association, 12-19.
17. Schlote T, Rohrbach J, Grueb M, Mielke J. Schlote Pocket
10. Hayreh SS. Ischemic Optic Neuropathies, Ed.
Atlas of Ophthalmology, Ed. Tieme, 2006;5-7,41-8.
Springer,2011,1-78,111-24,153.
18. Sinelnikov RD. Atlas of Human Anatomy, Vol II,
11. Gartner LP, Hiatt JL. Color textbook of histology, Ed.
Editia a IV-a, 1986,300-304 şi Vol III, 1990
WB Saunders,1996,213-7.
19. Balta F, Merticariu A, Panait OB. Practica patologiei
12. Dudea SM, Seceleanu A. Aplicaţii ale Ultrasonografiei
maculare în imagini, Ed. Medicală Antaeus, 2009;4.
Doppler în Patologia Ochiului şi Orbitei, Revista
20. Mozaffarieh M, Flamer J. Ocular Blood Flow and
Română de Ultrasonografie, 2002;3-4,181-8.
Glaucomatous Optic Neuropathy 2009;27-8,35-9,79-98.
13. Transquart F, Berges O, Koskas P and al. Color
21. Sobotta, Atlas of Human Anatomy, vol.1 Head,
Doppler Imaging of Orbital Vessels: Personal Experience
Neck,Upper Limb, Edited by R.Putz and R.Pabst in
and Literature Review, Journal of Clinical Ultrasound
collaboration with Renate Putz, Editia a 14-a, Ed.
2003;31(5):258-72.
Elsevier, 2006,363,368-71.
News in Study of Optic Nerve Vascularization
137
Colegiul Medicilor
Satu Mare
Colegiul Medicilor Satu Mare este o persoană juridică autonomă, neguvernamentală,
apolitică şi fără scop patrimonial. Este într-o largă accepţiune o organizaţie profesională
liberală şi reuneşte peste 626 de medici.
Colegiul Medicilor Satu Mare crede că poate reuşi urmând trei principii: să vorbească doar
când are ceva important de spus, să nu critice până când nu are soluţii şi să nu propună decât
soluţii rezultate din sfatul colectiv. Forţa Colegiului Medicilor constă în prezentarea în faţa
societăţii ca o voce autentică, permanent validată, a tuturor membrilor săi.
Satu Mare College of Physicians is an autonomous legal entity, non-governamental, apolitical
and non-profit. In a widley acception it is a liberal professional organization and brings
together over 626 doctors.
Satu Mare College of Physicians believes it can succeed by following three principles: to
speak only when he has something important to say, to make no critics until he has solutions
and to propose only solutions resulted from a of collective advice. Te force of Physicians
College consist in showing in front of the society an authentic voice, always validated, from
all its members.
Eroilor Revoluţiei Pl. no.23, 440055 Satu Mare, Romania.
Tel./Fax: +40-261-710456, +40-361-408164, e-mail: colmedsm@gmail.com
CASE PRESENTATION
TUMORĂ DESMOIDĂ MASCATĂ CA FIBROADENOM. PREZENTARE
DE CAZ ŞI O REVISTĂ A LITERATURII
Hermann Naama1, Fridel Ludmila2, Grubstein Ahuva3, Sharon Eran1
1Divizia de Chirurgie Generală, Spitalul Hasharon, 2Departamentul de Patologie, Spitalul Beilinson, 3Departamentul de
Radiologie, Spitalul Beilinson, Centrul Medical Rabin, Petah-Tikva, afiliat la Facultatea de Medicină Sackler,
Universitatea Tel-Aviv, Israel
Adresa pentru corespondenţă:
Naama Herman, MD
Department of Surgery B, Hasharon Hospital,
Petah-Tikva, Israel.
Email: naamahe@clalit.org.il
Primit: 25.01.2013
Acceptat: 15.02.2013
Med Con March 2013, Vol 8, No 1, 139-142
Rezumat
Acest caz este demonstrativ pentru diagnosticarea
greşită iniţială a leziunii ca o tumoră benignă, care poate
Prezentăm cazul unei femei de 19 ani diagnosticată
fi atribuită vârstei tinere a pacientei şi antecedentelor
iniţial cu fibroadenoam al sânului. Ea a fost trimisă la
fără elemente sugestive, precum şi lipsei de conştientizare
noi pentru o evaluare suplimentară a masei în creştere.
a existenţei acestei leziuni rare. Diagnosticul este
Ecografia a revelat o leziune nonvasculară, hipoechoică,
important din cauza invazivităţii tumorii şi necesităţii
neregulată. Biopsia leziunii a arătat histologia tipică
exciziei locale largi în scopul prevenirii recurenţei locale.
unei tumori desmoide. A fost supusă exciziei largi locale,
având confirmarea histopatologică postoperatorie a
Cazul
marginilor chirurgicale negative.
Cuvinte cheie: sân, desmoid, fibromatoză,
O femeie de 19 ani anterior sănătoasă s-a prezentat la
fibroadenom
clinica ei locală cu o masă nou apărută, solitară, fermă şi
mobilă, în sânul stâng. La început, ea a fost diagnosticată
Introducere
ca având un fibroadenom. După ce s-a plâns de creşterea
progresivă a masei pe parcursul a şase luni, a fost trimisă la
Tumorile desmoide ale sânului sunt tumori rare
spitalul nostru pentru evaluare suplimentară.
fibroblastice, care reprezintă 0,2% din toate tumorile
Pacienta nu a avut antecedente de traumatisme sau
sânului. Deşi benigne, ele sunt de multe ori invazive
intervenţii chirurgicale locale. Istoricul familial nu a fost
local şi au o rată ridicată de recurenţă locală. Prezentarea
semnificativ. La examenul clinic a fost palpată o masă
clinică, ecografia şi mamografia imită adesea carcinomul.
renitentă, superficială, mobilă şi bine definită, de 2 cm,
Histologic, leziunea care este compusă din proliferarea
superioară areolei, în cadranul supero-extern al sânului
celulelor axiale şi depozite de colagen, poate ajuta la
stâng. Nodulii limfatici axilari nu au fost palpaţi. Nu au
diagnostic. Managementul rămâne controversat, iar
fost semne de inflamaţie sau de scurgeri mamelonare.
baza tratamentului este considerată a fi excizia largă
Pacienta a fost trimisă pentru o ecografie, care a revelat o
locală, cu margini clare.
Desmoid Tumor Masquerading as Fibroadenoma. Case Report and Review of Literature
139
CASE PRESENTATION
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
Figura 1. Ecografia prezintă o leziune
Figura 3. Tumoră desmoidă compusă din fascicule
hipoechoică, rău delimitată, măsurând 2,1 cm
de celule axiale cu depozite fine de colagen (H&E x4)
Figura 2. Ecografia Doppler a leziunii nu arată
Figura 4. Tumoră desmoidă cu imunocolorare
nicio vascularizaţie semnificativă
nucleară Beta-catenin pozitivă (x10)
leziune neregulată hipoechoică de
2,1 cm, fără
Discuţie
vascularizaţie semnificativă, Figura 1 şi 2.
Pe baza acestor constatări, s-a decis să se efectueze o
Tumora desmoidă, sau fibromatoza agresivă, este o
biopsie pe ac Tru-Cut a leziunii. Biopsia a revelat o
proliferare benignă mezenchimală care provine din
proliferarea fibroblastică uşoară şi o colagenizare crescută
ţesutul conjunctiv al muşchilor, deasupra aponevrozei
fără atipii sau mitoze, o constatare consistentă cu
sau fasciei. Deşi nu metastazează, este caracterizată de
fibromatoza. După consultarea oncologului şi
un model de creştere infiltrativ şi suportă o rată ridicată
prezentarea informaţiei pacientei, a fost realizată o
de recurenţă locală [1,2]. Mortalitatea legată de tumoră
excizie largă a leziunii.
este rară, morbiditatea este atribuită în cea mai mare
În timpul operaţiei a fost excizată o masă măsurând
parte desfigurarării şi impotenţei funcţionale datorate
2×2 cm, cu o margine suplimentară de 1 cm. Leziunea a
progresiei locale sau tratamentului [3].
fost limitată la ţesutul mamar şi nu a implicat fascia
Tumorile desmoide reprezintă 1,5-3,5% din toate
subjacentă. Histopatologia postoperatorie a evidenţiat
tumorile ţesutului conjunctiv
[4]. Patogeneza este
focare de proliferare a celulelor axiale cu depozite fine de
necunoscută, dar factorii hormonali şi genetici, precum
colagen şi unele zone mixoide, Figura 3.
şi traumatismele locale sau intervenţiile chirurgicale, au
Nu au fost observate atipii nucleare sau pleomorfism,
fost propuse toate. Majoritatea tumorilor desmoide apar
iar indicele mitotic a fost scăzut. Colorarea pentru
sporadic, în timp ce o minoritate este asociată
vimentină şi Beta-catenin a fost pozitivă, Figura 4.
sindromului Gardner [5]. Prevalenţa mai mare la femei,
Eliminarea leziunii a fost completă, cu margini
precum şi creşterea dimensiunii tumorii în timpul
chirurgicale negative. Diagnosticul de fibromatoză a fost
sarcinii, pot sugera că estrogenul joacă, de asemenea, un
confirmat.
rol în patogeneză [1].
140
Hermann et al
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
CASE PRESENTATION
Tumora desmoidă a sânului este extrem de rară şi
chirurgicală microscopică pozitivă. Interesant este că
reprezintă 0,2% din toate tumorile de sân [1]. Aceste
impactul statusului marginii microscopice în estimarea
tumori pot apare fie primar din parenchimul mamar, fie
recurenţei este neclar, deoarece unele studii au aratat că
prin infiltrare secundară din stratul musculo-aponevrotic
marginile de rezecţie pozitive pot fi predictive pentru
al muşchilor pectorali [6,7]. Cele mai multe cazuri de
recurenţă, în timp ce alte studii nu au determinat o
tumori desmoide ale sânului apar la femei, existând
astfel de corelaţie [1,16-19]. Rata de recurenţă pentru
puţine cazuri la bărbaţi [8.]. Tumora desmoidă a sânului
leziunile de sân secundare, care provin din ţesutul
este considerată a fi mai frecventă după intervenţia
musculo-aponevrotic al muşchiului pectoral, este mult
chirurgicală în zona afectată, dar poate apare, de
mai mare decât pentru cele primare mamare
asemenea, de novo [1,9]. Unele rapoarte de caz recente
fibromatoase, care este raportată a fi de 21-27% [20].
au descris cazuri în urma implanturilor de silicon sau
Radioterapia poate oferi un bun control local al
saline, ceea ce presupune o posibilă relaţie cu capsula
tumorii desmoide, ca adjuvantă a intervenţiei
prostetică [7,8].
chirurgicale, sau chiar ca singurul tratament. Tendinţa
La examenul fizic leziunea este deseori palpată ca o
actuală este că, atunci când excizia largă locală are ca
masă fermă, mobilă. Poate fi prezentă retracţia pielii, sau
rezultat o compromitere semnificativă a funcţiei, sau
denivelarea ei. Mamografia tipică prezintă mase de
atunci când marginile chirurgicale sunt pozitive,
formă neregulată, necalcificate, de densitate înaltă, cu
radioterapia adjuvantă ar trebui să fie luată în considerare
margini în spiculi. Ecografic, tumora apare ca o masă
[1,17,18].
rău delimitată, hipoechoică. Astfel, prezentarea clinică şi
Tratamentele sistemice, cum ar fi agenţii hormonali
imagistică poate imita de multe ori carcinomul
şi
anti-inflamatori, chimioterapia şi tratamentul
[4,7,10,11].
biologic, au fost folosite cu rezultate mixte şi sunt în
RMN poate fi util în diferenţierea tumorii desmoide
general rezervate cazurilor în care controlul local nu este
de alte boli maligne ale sânului, precum dezvăluie şi
fezabil [3,19,21,22].
extinderea tumorii şi relaţia cu structurile adiacente.
În concluzie, cazul nostru de tumoră desmoidă de
Masa este ovoidală sau neregulată, traversează
sân este neobişnuit, deoarece se deghizează ca o altă
compartimente fasciale, este izointensă pe T1 şi
boală benignă - fibroadenomul. Este diferit de cele mai
heterogen hipererintensă pe T2-imagini ponderate,
multe cazuri publicate, în care leziunea este descrisă ca
aratând benzi de semnal scăzut în toate secvenţele.
imitând carcinomul sânului. Diagnosticul iniţial în
Leziunile afişează o amplificare de la moderată până la
acest caz poate fi atribuit vârstei tinere a pacientei şi
puternică după administrarea IV de substanţă de
lipsei factorilor de risc, precum şi rarităţii tumorilor
contrast [12,13].
desmoide provenite din parenchimul mamar.
Histologic leziunea este compusă din proliferări de
celule cu depuneri de colagen în cantităţi variabile,
uneori cu zone focale mixoide. Pot fi observate extensii
Referinţe
„în deget” în parenchimul mamar adiacent şi ţesutul
adipos. Celulele tumorale sunt adesea organizate în
1. Neuman H, Brogi E, Abrhaim A, Brennan M, Van
placarde mari, în configuraţie de stocare, sau
Zee K. Desmoid Tumors (Fibromatoses) of the Breast: a
mănunchiuri intercalate cu model „în os de hering”.
25-Year Experience. Ann Surg Oncol 2007;15(1):274-
Celularitatea globală este scăzută până la moderată, iar
80.
indicii mitotici sunt rari. Imunocolorarea indică
2. McDonald E, Eunhee Y, Wenger D. Extraabdominal
reactivitate variabilă pentru desmină şi actină, iar
Desmoid-type
Fibromatosis.
Radio
Graphics
coloraţia nucleară pentru Beta-C atenină susţine
2008;28:901-6.
diagnosticul, dar nu este patognomonică [14,15].
3. Melis M., Zager J, Sondak V. Multimodality
Managementul rămâne controversat deoarece
Management of Desmoid Tumors: How Important Is a
cazurile sunt rare, iar în literatura de specialitate există
Negative Surgical Margin? J Surg Oncol 2008;98:594-
în cea mai mare parte doar rapoarte de caz, fără nici-un
602.
studiu mai mare. Baza tratamentului este considerată
4. Ormandi K, Lazar G, Toszegi A, Palko A. Extra
excizia locală largă, cu margini clare. Este raportată de
Abdominal Desmoid Mimicking Malignant Male Breast
mai multe serii o rată ridicată a recurenţei locale după
Tumor. Eur Radiol 1999;9:1120-2.
excizie, variind de la 24% la 77% la 10 ani [16]. Factorii
5. Brueckl WM, Ballhausen WG et al. Genetic testing for
de risc nefavorabili corelaţi cu recidiva după excizie sunt
germline mutations of the APC gene in patients with
vârsta tânără, tumoră peste 3cm şi discutabil, o margine
apparently sporadic desmoid tumors but a family history
Desmoid Tumor Masquerading as Fibroadenoma. Case Report and Review of Literature
141
CASE PRESENTATION
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
of colorectal carcinoma. Dis Colon Rectum
15.
Carlson J W, Fletcher CD. Immunohistochemistry for
2005;48(6):1275-81.
beta-catenin in the differential diagnosis of spindle cell
6.
Gump FE, Sternschein MJ, Wolff M. Fibromatosis of
lesions: analysis of a series and review of the literature.
the breast. Surg Gynecol Obstet 1981;152:57-60.
Histopathology 2007;51(4):509-14.
7.
Chummun S, McLean N, Abraham S, Youseff M.
16.
Gronchi A, Casali PG et al. Quality of Surgery and
Desmoid tumor of the breast. J Plast Reconstr Aesthet
Outcome in Extra-Abdominal Aggressive Fibromatosis:
Surg 2010;63:339-45.
A Series of Patients Surgically Treated at a Single
8.
Glazebrook K, Reynolds C. Mammary Fibromatosis.
Institution. J Clin Oncol 2003;21(7):1390-7.
AJR 2009;193:856-60.
17.
Ballo T, Zagars GK, Pollack A, Pisters PW, Pollack
9.
Yiangou C, Fadl H, Sinnet H, Shousha S. Fibromatosis
RA. Desmoid Tumor: Prognostic Factors and Outcome
of the Breast or Carcinoma? J R Soc Med 1996;89:638-
after Surgery, Radiation Terapy, or Combined Surgery
40.
and Radiation Terapy. J Clin Oncol 1999;17:158-67.
10.
Okamoto K, Kurihara Y et al. Desmoid Tumor of the
18.
Nuyttens J, Rust P, Tomas C, Turrisi A. Surgery versus
Breast: Te Role of Proton Magnetic Resonance
Radiation Terapy for Patients with Aggressive Fibromatosis
Spectroscopy for a Benign Breast Lesion Mimicking a
or Desmoid Tumors. Cancer 2000;88(7):1517-23.
Malignancy. Breast J 2008;14(4):376-8.
19.
Lev D, Kotilingam D et al. Optimizing Treatment of
11.
Erguvan-Dogan B, Dempsey P, Ayyar G, Gilcrease
Desmoid Tumors. JCO 2007;25(13):1785-91.
M. Primary Desmoid Tumor
(Extraabdominal
20.
Schwarz G, Drotman M et al. Fibromatosis of the
Fibromatosis) of the Breast. AJR 2005;185:488-9.
Breast: Case Report and Current Concepts in the
12.
Nakazona T, Satoh T, Hamamoto T, Kudo S. Dynamic
Management of an Uncommon Lesion. Breast J
MRI of fibromatosis of the breast. Am J Roentgenol
2006;12(1):66-71.
2003;181:1718-9.
21.
Dufresne A, Bertucci F et al. Identification of biological
13.
Lee J, Tomas J, Phillips S, Fisher C, Moskovic E.
factors predictive of response to imatinib mesylate in
Aggressive Fibromatosis: MRI Features with Pathologic
aggressive fibromatosis. B J Cancer 2010;103:482-5.
Correlation. AJR 2006;186:247-54.
22.
Janinis J, Patriki M, Vini L, Aravantinos G, Whelan
14.
In: Rosen P.P. Rosen’s Breast Pathology,
3rd ed.
JS. Te pharmacological treatment of aggressive
Philadelphia: Lippincott Williams & Wilkins, Benign
fibromatosis: a systematic review. Ann Oncol
Mesenchymal Neoplasms 2009;829-37.
2003;14(2):181-90.
Traducere: dr.Bumbuluţ Călin
142
Hermann et al
CASE PRESENTATION
SENTURILE METALICE ALE URETERULUI AU INOCUITATE?
Stein Avi, Freifeld Yuval, Klein Ilan, May Tal, Muhad Yichie, Mecz Yoel, Goldin Dmitri, Faris Gazi,
Kaploun Alexander, Dekel Yoram
Departamentul de Urologie, Centrul Medical Carmel, Haifa, afiliat la Facultatea de Medicină, Universitatea Teknion,
Haifa, Israel
Adresa pentru corespondenţă:
Avi Stein, M.D.
Tel: 972 4 8341029, Fax: 972 777577770, Cell: 972 544709767
Email: stein37@netvision.net.il
Primit: 10.01.2013
Acceptat: 20.02.2013
Med Con March 2013, Vol 8, No 1, 143-144
Rezumat
Obiectivul acestui studiu a fost de a descrie un caz
de carcinom endometrial a uterului, tratat prin chirurgie
O femeie de 69 de ani a fost diagnosticată în 1998
şi radioterapie adjuvantă. Ea a dezvoltat o strictură
cu un carcinom endometrial care a necesitat intervenţii
severă a ambelor uretere distale. Un stent metalic a
chirurgicale şi radioterapie adjuvantă. Ea a dezvoltat
cauzat o complicaţie care a reprezentat o încercare
stricturi severe ale ambelor uretere distale, tratate
clinică şi chirurgicală.
printr-un stent metalic introdus în ureterul distal drept.
Cuvinte cheie: radioterapie, uretere, stricturi,
Prezentare de caz
stenturi metalice ureterale
O femeie de 69 de ani a fost diagnosticată în 1998
Introducere
cu un carcinom endometrial care a necesitat intervenţie
chirurgicală şi radioterapie adjuvantă. În
2000 ea a
Stenturile ureterale metalice sunt o versiune relativ
dezvoltat stricturi severe ale ambelor uretere distale
nouă a unui dispozitiv cu o lungă istorie în dezobstrucţia
tratate cu repetate inserţii de stent J dublu şi amplasarea
ureterală. Stenturile metalice sunt eficiente pentru
de tuburi de nefrostomie bilaterale. Un stent metalic a
dezobstrucţia ureterală, dar în ceea ce priveşte
fost inserat în ureterul distal drept. În
2005 o boală
tolerabilitatea pacientului, au un succes variabil [1].
renală în stadiu terminal a necesitat hemodializă cronică.
Stenoza ureterală secundară fibrozei induse de radiaţii
Doi ani mai târziu, în 2007, ea a fost supusă transplantului
este o complicaţie tardivă binecunoscută a tratamentului cu
renal având o recuperare lipsită de evenimente şi o
radiaţii la pacientele având carcinom de col uterin. Incidenţa
funcţie renală normală. Ea s-a prezentat prima dată la
ei a fost de 15% la pacientele tratate cu doze standard de
instituţia noastră în 2010 cu hematurie macroscopică şi
radioterapie pentru carcinom al colului uterin [2].
infecţii recurente ale tractului urinar. Tomografia
Pacientele care au fost tratate cu câmpuri externe în
computerizată a detectat o piatră mare la vezica urinară
blocuri centrale sau care au primit mai mult de două
în continuarea unui stent ureteral distal (Figura 1).
tratamente transvaginale cu radiatii, au un risc major
Cistoscopia a revelat o piatră mare a vezicii urinare.
pentru dezvoltarea stenozei ureterale [3].
Litotriţia laser a fost iniţiată până la apariţia porţiunii
Metal Stents of the Ureter are they Innocent?
143
CASE PRESENTATION
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
protruzive uitate, iar dezintegrarea pietrelor cu laser
însoţită de înlăturarea stentului a fost raportată ca
tratamentul unei astfel de patologii în cazul resturilor de
stent din plastic sau silicon [5,6]. Cazul prezentat pune
o problemă clinică interesantă: dacă dezintegrarea laser a
piatrelor vezicii urinare şi eliminarea părţilor metalice
ale stentului proeminente în vezica urinară este o soluţie
adecvată a problemei, sau dacă stentul trebuie să fie
eliminat din ureter. Aceasta nu ar fi o întrebare, dacă
ureterul în discuţie ar fi activ. La pacienţii cu obstrucţii
ureterale dificile, un stent metalic reprezintă o alternativă
sigură şi eficientă unui cateter dublu-spiralat a demeure,
sau a nefrostomiei percutane [7].
În cazul nostru, rinichiul drept nativ implicat a fost
Figura 1. Tomografia computerizată a arătat
nefuncţional. Retrospectiv, aceasta a fost o decizie bună
piatra şi stentul
întrucât pacienta a rămas asimptomatică la urmărirea de
distale a peretelui de metal al stentului obstruat de
un an.
calcifieri. Calcificările din lumenul stentului au fost
supuse laserului iar ghidajele stentului au fost scoase
prin biopsie în cupă până când a fost obţinută o
Referinţe
suprafaţă plană a vezicii urinare la nivelul orificiului
ureteral drept. Pacienta a avut o recuperare fără
1.
Benson AD, Taylor ER, Schwartz BF. Metal ureteral
evenimente. La un an de la procedură, uroculturile au
stent for benign and malignant ureteral obstruction. J
fost negative şi hematuria nu a reapărut. Partea
Urol 2011;185(6):2217-22.
ureterală a stentului a fost lăsată la locul ei şi nu a
2.
Buglione M, Toninelli M, Pietta N, et al. Post-
necesitat tratament, întrucât pacienta a rămas
radiation pelvic disease and ureteral stenosis:
asimptomatică.
physiopathology and evolution in the patient treated for
cervical carcinoma. Review of the literature and
Discuţie
experience of the Radium Institute. Arch Ital Urol
Androl 2002;74(1):6-11.
Radioterapia la nivelul bazinului a fost deseori
3.
McIntyre JF, Eifel PJ, Levenback C, Oswald MJ.
descrisă ca şi cauză a obstrucţiei ureterelor distale [4].
Ureteral stricture as a late complication of radiotherapy
Fibroza ureterală tardivă este o complicaţie legată de
for stage IB carcinoma of the uterine cervix. Cancer
tratament comună şi dureroasă la pacientele tratate cu
1995;75(3):836-43.
radioterapie pentru carcinom de col uterin. Strategiile
4.
Sklaroff DM, Gnaneswaran P, Sklaroff RB.
noi în definirea mai bună a ţintei pentru radioterapie,
Postirradiation ureteric stricture. Gynecol Oncol
radioterapia conformaţională şi o mai bună înţelegere a
1978;6:538-45.
factorilor biologici, vor contribui în continuare la
5.
Tsai CC, Shen JT, Huang SP, et al. Use of a Holmium
reducerea frecvenţei unei astfel de complicaţii [2].
laser to treat a forgotten double-J stent with whole stent
Stenturile ureterale de plastic sau silicon sunt cel
encrustations: a case report. Kaohsiung J Med Sci
mai des folosite pentru dezobstrucţie, dar trebuie să fie
2009;25:567-71.
periodic înlocuite şi oferă o soluţie temporară pentru
6.
Liatsikos EN, Kagadis GC, Barbalias GA, Siablis D.
această problemă. Pentru a depăşi nevoia frecventă de
Cystoscopic holmium lithotripsy of large bladder calculi.
înlocuiri repetate, au fost sugerate stenturile de metal.
J Endourol 2005;19:934-9.
Au fost folosite mai multe tipuri de stenturi de metal
7.
Wakui M, Takeuchi S, Isioka J, Iwabuchi K,
incluzând Resonance® şi Urolume®. Litiaza vezicii
Morimoto S. Metallic stents for malignant and benign
urinare se poate dezvolta în jurul stenturilor sintetice
ureteric obstruction. BJU Int 2000;85(3):227-32.
Traducere: dr.Bumbuluţ Călin
144
Stein et al
EDITORIAL APPEARANCE
ENCYCLOPEDIA OF CRISIS MANAGEMENT / ENCICLOPEDIA
MANAGEMENTULUI DE CRIZĂ
Editura SAGE Publications Inc, March 2013, ISBN
9781452226125, editori: K. Bradley Penuel, Matt Statler
- New York University şi Ryan Hagen de la Columbia
University. SAGE Publications este cea mai mare editură
independentă din mediul academic din lume. Publicaţiile
sale din peste 30 de domenii, majoritatea cu caracter
didactic universitar sau postuniversitar, cuprind doar
enciclopedii în peste 60 de diferite domenii. SAGE este a
5-a mare editură din lume în ceea ce privesc jurnalele
ştiinţifice (peste 700) în cele mai diverse domenii: ştiinţe
sociale, tehnologie, medicină, etc.
Enciclopedia de Management al Dezastrelor se
constituie ca o colecţie de 385 de capitole semnate de
peste
150 de autori, care sunt organizate în ordine
alfabetică, în 2 volume cu peste 1100 de pagini.
Autorii aparţin unora dintre cele mai prestigioase
universităţi din lume: din SUA- Princeton University,
New York University, Columbia University, dar şi din
UK- Oxford University, Coventry University şi
de specialitate din ţară (o carieră de medic specialist în
University of Glasgow, China- Beijing Academy of
anestezie, terapie intensivă şi medicină de urgenţă,
Science and Technology, Turcia- Istanbul Technical
cutremurul din 1977) dar şi din străinătate (Somalia
University şi Selcuk University, Italia- University for
1993, Turcia 1999, spaţiul ex-jugoslav, etc), dar şi cea
Foreigners of Perugia, India- National Institut of
didactică obţinută prin cursurile universitare sau extra-
Disaster Management Delhi, Israel- Ben Gurion
universitare în acest domeniu şi mai ales prin
University of the Negev, până la University of Tasmania
coordonarea primului master din Romania de Medicină
şi Hawaii, dar şi structuri executive internaţionale de
de Dezastru.
prestigiu- Global Risk Forum Davos, Taiwan Centers
Capitolul redactat de Profesorul Dan Mănăstireanu
for Disease Control.
ne introduce într-o disciplină în care ar trebuie să fie
În această companie selectă, Universitatea Titu
instruiţi toţi medicii zilelor noastre, inevitabil
Maiorescu din Bucureşti, prin prof. dr. Dan
confruntaţi cu vicisitudinile naturii sau ale atacurilor
Mănăstireanu, autor al capitolului „Triajul”, se înscrie
teroriste. Cu toate că suntem tentaţi a crede că ne aflăm
ca singura unitate de învăţământ din Romania şi printre
în faţa unei discipline medicale noi, autorul ne
puţinele din Europa, agreată să contribuie la prestigioasa
demonstrează ca istoria ei se întrevede din timpul
Enciclopedie de management al crizelor.
campaniilor lui Napoleon: ”Triajul (...) (într-un spital)
Domeniu relativ nou, managementul crizelor este
este procesul de a decide cât de grav bolnavă sau afectată
prezentat tematic în cadrul capitolelor, cartea având şi o
este o persoană, astfel încât cele mai grave cazuri să fie
prefaţă cu menţiuni legate de largi domenii teoretice
tratate primele. Termenul provine din verbul francez
(sănătate, agenţii şi organizaţii, teorii si tehnici, crizele
„trier” impus de Dominique Jean, Baron Larrey (1766-
economice, etc).
1842), un chirurg militar în serviciul lui Napoleon (care a
Contribuţia prof. dr. Dan Mănăstireanu, capitolul
descris în lucrările sale menevre precum amputaţia de şold
privind „Triajul medical în situaţii de dezastru” reflectă
necesară în situaţii de război, condiţia numită piciorul de
experienţa cadrului didactic al UTM atât în activitatea
tranşee şi termenul de brancardier). Chirurgul britanic
145
EDITORIAL APPEARANCE
MEDICAL CONNECTIONS • NUMBER 1 (29) • MARCH 2013
John Wilson propune în 1846 utilizarea diferitelor tipuri
neaşteptate se referă la ruperea rutinei zilnice şi la
de tratamente asociate cu şansa de supravieţuire, acestea
necesitatea adaptării mijloacelor existente la situaţiile
inspirând categorii de tratamente pe niveluri de triaj.
neobişnuite şi metode. Triajul ar trebui să fie dinamic,
Medicina militară, de-a lungul anilor, a avut un impact
continuu, progresiv şi adaptabil la schimbările atât în
semnificativ asupra dezvoltării triajului medical.
nevoile victimelor cât şi ale nevoilor/utilizării resurselor.”
Diferenţele doctrinare între cele două tipuri, triajul civil şi
Concluzia capitolului ne atrage atenţia:
„regulile
militar, stau în strategiile celor două entităţi, războiul şi
unui triaj eficient sunt: Orice poate ajuta la organizare şi
nevoia de a avea cât mai repede disponibili luptători
îmbunătăţirea răspunsului medical în dezastru este bun şi
într-un timp cât mai scurt şi scopul de a asista cât mai
trebuie utilizat. Triajul în situaţiile de dezastru este diferit
multe victime posibil.”
de situaţiile obişnuite. Cei mai importanţi factori luaţi în
Definitia moderna a triajului ne este prezentată cu
considerare în situaţii de criză sunt personalul şi logistica.
acurateţe: „Triajul este un sistem formal, utilizat pentru
Pentru ca triajul să-şi atingă sopul, toate victimele trebuie
identificarea, clasificarea şi tratarea victimelor, în
să beneficieze de aceeaşi atenţie la triajul primar. Nici-un
concordanţă cu severitatea suferinţei lor. Sub ghidajul şi
grup de pacienţi nu poate avea prioritate faţă de altul, acest
prin scopurile medicinei de dezastru, se oferă o şansă de
lucru trebuie făcut doar în concordanţă cu aprecierea
salvare a câtor mai multor oameni posibil”.
statusului lor general. Această afirmaţie include şi copii.”
Rând pe rând suntem iniţiaţi în metodele de triaj,
Revista Conexiuni Medicale a fost printre
triajul la locul dezastrului, metodologia triajului, sau
promotoarele în spaţiul publicistic al domeniului
factorul de severitate. Autorul ne dă indicaţii precise
Medicinei de Dezastru, publicând în 2011 una din
prin punctele cheie ale întregii acţiuni: „Lipsa resurselor
lucrările prof. dr. Dan Mănăstireanu: „Ce avem de făcut
adecvate, numărul mai mare de victime şi aspectele
când se produce un dezastru/What to do in the event of
neaşteptate sunt factori limitatori în triaj. Aspectele
a disaster”, Med Con March 2011; Vol 6, No 1, 87-94.
146
ZILELE MEDICALE SĂTMĂRENE EDIŢIA A X-A, 3-5 octombrie 2013
PRIMUL ANUNŢ
Joi 3 Octombrie 2013
09:00 - 09:30
- Primirea participanţilor. Validarea participării. Înscrieri. Înmânarea documentelor manifestării.
09:30
- Deschiderea oficială
10:00 - 17:00
- Sesiune de comunicări lucrări ştiinţifice cu pauze: pentru cafea şi pentru prânz
Vineri 4 Octombrie 2013
09:00 - 16:00
- Sesiune de comunicări lucrări ştiinţifice cu pauze: pentru cafea şi pentru prânz
Sâmbătă 5 Octombrie 2013
09:00 - 16:00
- Sesiune de comunicări lucrări ştiinţifice cu pauze: pentru cafea şi pentru prânz. Înmânarea
certificatelor de participare. Înmânarea diplomelor de excelenţă pe baza voturilor participanţilor.
Informaţii generale
Conferinţă regională, cu participare internaţională
Locaţie: Restaurant Romantic, str. Careiului nr 63
Organizator: COLEGIUL MEDICILOR SATU MARE
Parteneri: ASOCIAŢIA MEDICILOR DE FAMILIE SATU MARE, CENTRUL MEDICAL RABIN-
UNIVERSITATEA TEL AVIV ISRAEL, UNIVERSITATEA TITU MAIORESCU BUCUREŞTI,
UNIVERSITATEA DE VEST VASILE GOLDIŞ ARAD FILIALA SATU MARE
Preşedinta Comitetului Ştiinţific: Prof. Univ. Dr. Rumelia Koren
Preşedintele de onoare al manifestării: Prof. Univ. Dr. Vasile Astărăstoae
ÎNSCRIERE
Puteţi să vă înscrieţi:
- personal la sediul Colegiului Medicilor Satu Mare
- prin poştă, pe adresa: Colegiul Medicilor Satu Mare, P-ţa Eroilor Revoluţiei nr. 23, cod poştal 440055
- prin fax la numărul: 0361-408164, e-mail: colmedsm@gmail.com
Înregistrarea va fi validată doar după dovada plăţii taxei de participare.
TAXA DE PARTICIPARE
- Medici, specialişti, primari - 60 lei
Până la 31.08.2013
- Medici rezidenţi, studenţi, pensionari - gratuit
- Medici, specialişti, primari - 70 lei
După 31.08. 2013 şi pe loc
- Medici rezidenţi, pensionari - 20 lei
- se poate plăti în contul Colegiului Medicilor Satu Mare: RO21BTRL03101205K39262XX, deschis la Banca
Transilvania Satu Mare, cu menţionarea: taxă participare 03-05.10.2013 şi numele participantului
- se poate achita direct la sediul Colegiului Medicilor Satu Mare
Taxa de participare include: mapa cu documentele manifestării, accesul la sesiunile de lucru, coffee-break-uri,
bufetul suedez pentru fiecare zi.
Pentru rezervări cazare până la data de 30.09.2013: tel 0261-710456, e-mail: colmedsm@gmail.com
LUCRĂRI
Termenul pentru predare a rezumatelor este 1 septembrie 2013.
Comitetul ştiinţific îşi rezervă dreptul de a accepta sau respinge lucrările propuse.
Lucrările participanţilor vor fi sub formă de prezentare în format Power Point şi vor fi susţinute oral timp de 10 minute.
Termenul limită de predare a lucrărilor în format Power Point este 15 septembrie 2013.
lucrări in extenso
Lucrările in extenso vor fi publicate în revista „Conexiuni Medicale” nr. 4/2013, cu condiţia să fie înaintate
la adresa de e-mail bumbulutcalin@yahoo.com.
Se acceptă doar lucrări nepublicate, autorii asumându-şi integral răspunderea conţinutului.
GUIDANCE FOR DRAWING UP
STANDARDE DE REDACTARE
Scop
prin care aceştia permit publicarea fotografiilor sau altor
Revista Conexiuni Medicale publică lucrări de
materiale care ar putea să îi identifice. Dacă formularele
cercetare care contribuie la progresul din toate domeniile
de accept nu prevăd acest lucru vă rugăm să rugăm
medicinei. Revista publică de asemenea reviste generale,
obţineţi acordul, sau îndepărtaţi posibilitatea de
editoriale şi scurte comunicări pe domenii specifice.
identificare. O declaraţie în acest sens trebuie inclusă în
Prezentările de caz sunt acceptate dacă prezintă interes
secţiunea „Metode” a lucrării.
crescut şi sunt bine investigate. Scrisorile către editor, în
special cele care prezintă o opinie privind un articol
Aprobarea Comitetului de Etică
publicat anterior sau care prezintă noi date, sunt de
Precizaţi la secţiunea „Metode” faptul că desfăşuraţi
asemenea binevenite. Adresa web a revistei este http://
studii asupra subiecţilor umani cu aprobarea Spitalului,
Comitetului de Etică al Universităţii, etc. În mod
trimestrial, articolele sunt acceptate în limba engleză sau
similar, confirmaţi dacă experimentele asupra animalelor
română, având cel puţin traducerea în limba engleză a
corespund standardelor etice.
rezumatului şi cuvintelor cheie. Lucrările pot fi trimise
pe adresa: dr. Bumbuluţ Călin, editor şef adjunct,
Asumarea dreptului de copyright
Conexiuni Medicale, P-ţa. Eroilor Revoluţiei nr. 23, cod
Lucrările acceptate pentru publicare au implicit
440055, Satu Mare, Romania. Tel./Fax:
+40-261-
drepturile de copyright cedate către editor. Autorii pot
710456, e-mail: bumbulutcalin@yahoo.com.
utiliza materiale din lucrările lor în alte articole proprii.
Republicarea articolelor
Propunerea pentru publicare
Vă rugăm să confirmaţi că lucrarea dumneavoastră
Toate manuscrisele propuse pentru publicare în
nu a mai fost publicată în forma prezentată sau într-o
Conexiuni Medicale vor fi în format compatibil pentru
formă asemănătoare, sau că nu a fost acceptată pentru
efectuarea recenziei online. Revista acceptă manuscrise
publicare într-o altă revistă.
propuse în formă electronică, în format Word (text,
figuri şi tabele). Nu trimiteţi lucrări în format PDF.
Conflicte de interese
Acceptăm lucrări care nu depăşesc 3.500 de cuvinte
Rugăm autorii să declare posibilele conflicte de
pentru articole originale,
2.500 pentru prezentări de
interese, inclusiv cele de natură financiară. Dacă nu
caz,
2.000 pentru prezentări de imagini clinice, 500
există conflicte de interese, vă rugăm să precizaţi acest
pentru scrisori către editor şi 4.500 de cuvinte pentru
lucru. Sursele de finanţare trebuie precizate în lucrarea
reviste generale. Autorii NU vor trimite prin poştă sub
dumneavoastră.
formă de hârtie propunerea pentru publicare, decât dacă
este vorba de scrisori sau dacă se solicită astfel din partea
Permiterea de a reproduce materiale
redacţiei. Dacă nu există altă opţiune decât trimiterea
publicate anterior
prin poştă, vă rugăm să expediaţi şi versiunea electronică
Vă rugăm să ne trimiteţi o copie a acceptului de
pe disketă sau CD-ROM pe adresa redacţiei: Conexiuni
reproducere (de exemplu al ilustraţiilor) de la deţinătorul
Medicale, P-ţa. Eroilor Revoluţiei nr. 23, cod 440055,
dreptului de copyright.
Satu Mare, România. Utilizaţi text la două rânduri şi
includeţi următoarele secţiuni: pagina de titlu, rezumatul
Formularele de accept ale pacienţilor
şi cuvintele cheie, textul, mulţumiri, referinţe, tabele şi
Protecţia drepturilor pacienţilor este esenţială; vă
figuri. Paginile vor fi numerotate consecutiv, începând
rugăm să ne trimiteţi formularele de accept ale
cu pagina de titlu, numerele arabe fiind plasate în colţul
pacienţilor sau subiecţilor studiului dumneavoastră,
din dreapta sus al fiecărei pagini.
148
MEDICAL CONNECTIONS • NUMBER 4 (28) • DECEMBER 2012
GUIDANCE FOR DRAWING UP
Prezentarea lucrării
a abrevierilor. Folosiţi metode de calcul statistic
Pagina de titlu
standardizate.
Nominalizaţi
medicamentele
şi
Cuprinde titlul întreg şi titlul scurt format din
substanţele chimice utilizând numele generic (dacă sunt
maxim 45 de caractere, numele şi prenumele fiecărui
menţionate mărcile înregistrate, se furnizează numele
autor; dacă lucrarea aparţine unui departament sau unei
producătorului şi oraşul).
instituţii, va fi menţionat numele acestuia în întregime.
Mulţumiri
De asemenea numele, e-mail-ul şi adresa autorului
Vor fi adresate celor care au adus contribuţii
împuternicit pentru corespondenţă, sursele de finanţare
importante la studiu.
sau suport utilizate sub forma burselor, echipamentelor,
Referinţe
medicamentelor, sau orice combinaţie a acestora.
Vor fi numerotate între paranteze drepte cu
Rezumatul
numerale arabe, succesiv în ordinea în care sunt
Pagina a doua va cuprinde rezumatul cu minim 200
menţionate în text. Referinţele vor include numele
de cuvinte; nu utilizaţi abrevieri, note de subsol, sau
autorilor până la al şaselea autor, dacă sunt mai mulţi,
referinţe.
enumeraţi primii trei şi apoi adăugaţi „et al”. Referinţele
Introducere în temă şi scopuri
vor include titlul complet şi sursa informaţiei; numele
Descrieţi importanţa studiului şi obiectivul
revistelor va fi abreviat conform Index Medicus (http://
(obiectivele) precise ale cercetării sau întrebarea
(întrebările) pe care le ridică studiul.
acceptă mai mult de 90-100 referinţe; pentru scrisori
Metode
către redacţie se acceptă 5-6 referinţe. Folosiţi ca şi
Includeţi informaţii privind următoarele aspecte ale
referinţe cât mai puţine rezumate. Comunicările
studiului dacă sunt utilizate: proiectul
- descrieţi
personale şi lucrările nepublicate nu vor fi menţionate la
elementele de bază ale studiului, de exemplu studiu
referinţe şi vor apare în text între paranteze. Lucrările
controlat randomizat, studiu cross-secţional, de cohortă,
nepublicate dar aflate în curs de publicare vor fi incluse
de urmărire, serii de cazuri, etc; procedura - specificaţi
în referinţe cu menţiunea „in press” între paranteze,
dacă a fost desfăşurat în sistem de îngrijire primar sau
lângă numele revistei implicate.
terţiar, în ambulator sau spital, în comunitate, etc;
Tabele
participanţi - indicaţi numărul subiecţilor şi cum au
Fiecare tabel va fi numerotat cu numerale romane,
fost selectaţi, recrutaţi şi desemnaţi pentru intervenţie;
cu un titlu scurt deasupra, la subsolul lor vor fi trecute
intervenţia
- metoda de administrare şi durata
notele
explicative,
menţionându-se abrevierele
intervenţiei.
nestandardizate utilizate; nominalizaţi valorile statistice
Rezultate
care variază precum deviaţia standard şi eroarea standard
Prezentaţi principalele rezultate ale studiului,
a medianei. Fiecare tabel va fi citat în text.
inclusiv intervalurile de confidenţă sau valorile p.
Figuri
Concluzii
Toate graficele, fotografiile, diagramele vor fi
Enunţaţi doar concluziile susţinute direct de dovezi,
considerate ca figuri şi vor fi numerotate succesiv în text
precum şi importanţa descoperirilor. Revistele generale
cu numerale arabe. Dacă o figură a fost publicată
şi prezentările de caz vor include un rezumat
anterior, sursa va fi citată cu mulţumiri, menţionându-
nestructurat.
se permisiunea deţinătorului de copyright. Figurile pot
Cuvinte cheie
fi reduse, grupate sau şterse la dorinţa editorului.
Rezumatul va fi urmat de o listă de 3-10 cuvinte
Legenda figurii va fi plasată la subsolul ei; va fi explicată
cheie sau fraze scurte care vor ajuta la indexare. Dacă este
scala utilizată, respectiv metodele de colorare
posibil, utilizaţi termeni proveniţi din lista Index Medicus
microscopică.
cu 262 subiecte medicale/Medical Subject Headings 262
Unităţi de măsură
Măsurătorile lungimii, înălţimii, greutăţii şi
Textul
volumului vor fi făcute în sistem metric sau multipli
Un studiu original va fi divizat în secţiuni denumite
decimali. Temperaturile vor fi exprimate în grade
Introducere, Metode, Rezultate şi Discuţii
(incluzând
Celsius. Tensiunea va fi măsurată în mmHg. Toate
concluziile), după formula „IMRAD”. Articolele lungi
măsurătorile hematologice vor fi exprimate în Sistemul
pot necesita subsecţiuni
(în special la Rezultate şi
Internaţional de Unităţi (SI).
Discuţii) pentru clarificare. Alte tipuri de articole
Abrevieri şi simboluri
precum prezentări de caz, reviste generale, editoriale,
Utilizaţi doar abrevieri standard. Evitaţi abrevierile
pot urma alt format. Nu recomandăm utilizarea excesivă
în titlu şi rezumat. Cuvântul va preceda abrevierea la
149
GUIDANCE FOR DRAWING UP
MEDICAL CONNECTIONS • NUMBER 4 (28) • DECEMBER 2012
prima utilizare în text, cu excepţia unităţilor de măsură
Abonamente
standard.
Preţul unui abonament anual pentru 2013 este: 80
RON individual, 160 RON pentru instituţii, plătiţi în
Retipăriri
contul Colegiului Medicilor Satu Mare RO38 BTRL
Sunt oferite gratuit zece copii ale articolului publicat
0310
1202 K392
62XX, cod fiscal
9839430, cu
şi două ale revistei. Dacă sunt necesare mai multe copii,
menţiunea
„pentru abonament Conexiuni Medicale”.
sunt disponibile contra cost.
Solicitarea abonării poate fi trimisă prin poştă: P-ţa.
Eroilor Revoluţiei nr.
23, cod
440055, Satu Mare,
Politica editorială
Romania. Tel./Fax: 0261-710456, 0361-408164, sau
Apreciem toate contribuţiile în domeniul medicinei.
prin e-mail: colmedsm@gmail.com.
Invităm personalităţi recunoscute cu expertiză şi articole
din diverse domenii să publice reviste generale şi
Publicitate
editoriale în revista noastră. Acceptăm de asemenea
Cererile pentru spaţiu publicitar vor fi adresate
lucrări originale şi prezentări de caz din toate ţările.
redacţiei Conexiuni Medicale. Preţurile (plătite în lei la
Conexiuni Medicale vă oferă o recenzie atentă şi
cursul BNR) pentru publicitate pe 2013 sunt 200 euro
publicarea imediată după acceptare. Redactorii vor citi
pagina (A4) color, un număr şi 800 euro patru numere;
primii lucrarea, decizând în decurs de 1-3 săptămâni în
coperta interioară faţă sau spate: 350 euro un număr,
funcţie de nivelul de prioritate: unele sunt trimise
1400 euro patru numere; coperta exterioară spate: 400
imediat recenzorilor, unele pot fi respinse, iar unele sunt
euro un număr, 1600 euro patru numere. Cont bancar:
returnate autorilor cu sugestii de îmbunătăţire înainte
Colegiul Medicilor Satu Mare, CUI 9839430, Banca
de expedierea spre recenzori.
Transilvania, agenţia Golescu Satu Mare, IBAN: RO38
BTRL 0310 1202 K392 62XX.
Procedura peer-review
Conexiuni Medicale practică o evaluare a tuturor
© Copyright Conexiuni Medicale/Medical
lucrărilor originale de către doi sau trei recenzori
Connections, Satu Mare, 2013
independenţi, din care doi sunt personalităţi
Nicio parte a acestei publicaţii nu poate fi reprodusă,
internaţionale. Procesul peer-review este esenţial pentru
stocată sau transmisă sub orice formă sau prin orice
asigurarea calităţii informaţiei ştiinţifice. Recenzorii
mijloace, fără permisiunea prealabilă în scris a revistei
sunt rugaţi să evalueze manuscrisul aplicând aceleaşi
Conexiuni Medicale. Permisiunea nu este necesară
standarde ca şi pentru reviste internaţionale; comentariile
pentru a copia rezumate sau articole dacă este indicată
sunt trimise editorului, care va informa autorii asupra
sursa, cu citarea completă a referinţei. Solicitarea
acestor sugestii, rugându-i să răspundă la întrebări şi să
privind permisiunea de a retipări toată revista sau o
facă necesarele corecţii. Aceste informări sunt făcute în
parte a ei, va fi adresată editorului prin e-mail:
cel mult trei luni de la propunerea de publicare.
colmedsm@gmail.com
Manuscrisul revizuit de autori va fi reexpediat editorului
în cel mult o lună. La primirea de către editor a versiunii
Revista Conexiuni Medicale apare trimestrial prin
corectate, însoţită de o scrisoare de răspuns punctuală la
efortul logistic şi financiar al Colegiului Medicilor Satu
comentariile recenzorilor, se retrimite manuscrisul
Mare şi Asociaţiei Medicilor de Familie Satu Mare, în
aceloraşi recenzori, care vor face recomandarea finală
cadrul proiectului comun al Centrului de Documentare
pentru acceptarea sau respingerea acestuia.
şi Educaţie Medicală Continuă Satu Mare.
150